
Abstract
Magnetic seizure therapy (MST) is under development as a means of reducing the side effects of electroconvulsive therapy (ECT) through enhanced control over patterns of seizure induction and spread. We previously reported that chronic treatment with MST resulted in less impairment in cognitive function than electroconvulsive shock (ECS) in a non-human primate model of convulsive therapy. Here we present quantitative analyses of ictal expression and post-ictal suppression following ECS, MST, and anesthesia-alone sham in the same model to test whether differential neurophysiological characteristics of the seizures could be identified. Rhesus monkeys received 4 weeks of daily treatment with ECS, MST, and anesthesia-alone sham in a counterbalanced order separated by a recovery period. Both ECS and MST were given bilaterally at 2.5 × seizure threshold. Neurophysiological characteristics were derived from two scalp EEG electrode recording sites during and immediately following the ictal period, and were compared to sham treatment. EEG power within four frequencies (delta, theta, alpha and beta) was calculated.
Our results support earlier findings from intracerebral electrode recordings demonstrating that MST- and ECS- induced seizures elicit differential patterns of EEG activation. Specifically, we found that ECS shows significantly more marked ictal expression, and more intense post-ictal suppression than MST in the theta, alpha, and beta frequency bands (Ps<.05). However, the ECS and MST were indistinguishable in the delta frequency band during both ictal and post-ictal periods. These results demonstrate that magnetic seizure induction can result in seizures that differ in some neurophysiological respects compared with ECS, but that these modalities share some aspects of seizure expression. The clinical significance of these similarities and differences awaits clinical correlation.
INTRODUCTION
The induction of seizures, as with electroconvulsive therapy (ECT), is a highly effective and rapidly acting treatment for major depression. Given the powerful antidepressant effect of induced seizures, substantial research has focused on the relations among the neurophysiological characteristics of seizures and clinical outcome. Developing a means of seizure induction that provide enhanced control over aspects of seizure expression would provide tools for studying and exploiting the relations among neurophysiological characteristics, efficacy, and cognitive side effects. For example, manipulations of electrode placement and electrical parameters of stimulation result in significant differences in seizure expression, efficacy and amnestic side effects of ECT 1 Magnetic seizure therapy (MST) is under development as another means of achieving enhanced control over seizure expression, taking advantage of the focality of magnetic fields. 2 –4 Unlike the transcanial application electricity in ECT, magnetic fields are not impeded by scalp and skull and thus can be more precisely targeted 5
Studies of scalp electroencephalographic (EEG) characteristics during (ictal) and immediately following (post-ictal) the seizure have revealed correlations with treatment outcomes with ECT. For example, EEG characteristics of patients during and following ECT treatments linked clinical efficacy to a change in EEG delta power in pre-frontal regions. 6,7 However, the relationship between EEG characteristics and cognitive side effects appears to be complex and may depend upon treatment parameters. For example, one study reported an association between retrograde amnesia following ECT treatment and increase in EEG theta power in left fronto-temporal region, 8 while a study by Perera and colleagues 9 using similar stimulus parameters did not find strong associations between the EEG measures and cognitive outcome. It has been suggested that both clinical efficacy and side effects in ECT depend upon (among other variables) the site of seizure initiation and the pattern of activation, factors that are hard to control in ECT. MST offers better control over these treatment parameters due to its more localized nature, and therefore it holds great promise in controlling stimulation parameters that may impact clinical outcome. Specifically, MST-induced electrical currents are confined to superficial cortex, while ECT induces radial currents that penetrate more deeply. 10 Therefore, with MST it may be possible to induce seizures that originate in superficial cortex, sparing deeper brain structures that might be related to side effects. In particular, if MST can offer more precise control over intracerebral current paths, it opens the possibility of inducing more focal seizures and of protecting neural tissue such as the medial temporal regions that are implicated in amnesic side effects following ECT. However, to date little has been reported regarding the EEG characteristics of seizures induced by MST.
Lisanby et al. 10 used a non-human primate model to characterize the neurophysiological effects of MST and compared it to the findings with ECS treatment. In that study, intracranial electrodes were implanted to enable intracerebral recordings of the electric field changes during seizures induced by ECS and MST. Lisanby et al. reported that the induced field in the MST treatment depended on coil size, shape, orientation and distance from recording sites, as well as on the overall lower magnitude of the MST-induced voltage relative to that produced by ECS. Overall comparison of MST- and ECS-induced seizure in rhesus monkeys revealed that MST resulted in less induced current and seizure spread that had a lesser effect on the hippocampus. 10,11
Comparison of MST- and ECT-induced seizure in depressed patients also revealed a difference in seizure expression. 12 Specifically, for each frequency band (delta, theta, alpha and beta), MST induced seizures had less robust ictal expression than ECT. Moreover, postictal EEG suppression was greater with ECT than MST, and recovery of full orientation was faster for MST compared with ECT. Overall the cognitive sequelae appeared to favor MST to ECT. The findings in these studies supported the expectation that MST treatment may offer better control over the electric field distribution during seizures, and illustrated the potential of improving the risk/benefit ratio of convulsive therapy.
Moscrip et al. 13 developed a Primate Cognitive Profile in nonhuman primates sensitive to the effects of ECS on cognitive outcome. In a later study, Moscrip et al. 14 used that battery to examine cognitive outcome following both ECS and MST treatment. Moscrip et al. found that MST results in more benign cognitive side effects than ECS. Overall, the monkeys were less accurate in long- and short- term memory and recall tasks following ECS compared to sham and MST. Moreover, the monkeys were slowest to complete the tasks following ECS, whereas sham and MST did not differ in completion time. In addition to cognitive measurements, that study included noninvasive scalp EEG recordings. The current paper used those recordings to compare the neurophysiological characteristics of MST-induced seizure to those of ECS, and test the hypothesis that a complete course of MST would result in differential neurophysiological expression than a course of ECS, matched for dosage relative to seizure threshold. EEG was recorded from two scalp sites during and following the ictal period induced by MST and ECS, and the power of four EEG frequency bands was compared between these two treatment types. An anesthesia-only sham control condition was included to allow for a comparison when no treatment was given, and to control for the effects of anesthesia.
METHODS
Complete details about the subjects and treatment procedures are provided in Moscrip et al. 13,14 This study was approved by the Institutional Animal Care and Use Committee of New York State Psychiatric Institute and Columbia University.
Study design and procedure
The study was conducted on two experimentally naïve male macaca mulatta monkeys with a mean age of 52 (+/− 1) months. The study had a within-subject design in which each monkey underwent three experimental conditions, ECS, MST and Sham, each over 25 consecutive days of treatment. Order of the conditions to which subjects were assigned was pseudo-random. The risk of carry-over effects was reduced by giving each subject a recovery period for a minimum of 3 weeks, and ensuring that their cognitive performance had returned to baseline. Titration for seizure threshold for the ECS and MST conditions was performed on the first and 11th sessions, and dosage adjusted to remain at 2.5 × seizure threshold.
Anesthesia
Pre-anesthesia sedation for transport to the treatment suite was achieved with methohexital (4.75 mg/kg i.v.) via voluntary venepuncture in the home cage. The anesthetic agents were methohexital (0.5 mg/kg i.v.) and succinylcholine (2.5 mg/kg i.v.). One hundred percent oxygen was given throughout.
ECS, MST, and Sham Procedures
Skin underlying the ECS and EEG electrodes was shaved. Bilateral ECS was administered with a MECTA Spectrum 5000Q ECT device (MECTA Corporation, Tualatin, OR, USA), with self-adhesive stimulating electrodes that were modified to fit the small cranium of a monkey (Somatics Corporation, Lake Bluff, IL, USA). ECS electrodes were placed bilaterally on the right and left temples (just forward and above the ears). MST was administered using a custom-made MST device (Magstim, Inc., Wales UK) which could deliver sustained trains of 50Hz at 100% maximal output for 8 seconds, with a pediatric-sized round coil (6.2 cm diameter) placed on the vertex of the head. Seizure thresholds for both ECS and MST were determined using the ascending method of limits titration procedure. 15 Subsequent daily dosage of ECS and MST was set at 2.5 times the seizure threshold.
EEG seizure activity was obtained with bilateral fronto-mastoid EEG channels using the amplifiers of the MECTA Spectrum (gain = 5000, band passed 1.4 Hz-48 Hz, sampling rate = 100 Hz) and digitized on a PC using the MECTA Spectrum program. Sham intervention involved anesthesia and monitoring only, with no stimulation or seizure induction. Seizure duration was measured from the time of ECS- or MST-induced stimulation until the end of convulsion seen in the arm, which had been spared the effects of the paralytic agent with a tourniquet, and by visual inspection of the EEG recordings.
Data Analyses
All the EEG recordings were visually inspected to remove artifacts. The artifact-free data were subjected to fast Fourier transformation, using 1-second epochs over-lapping by 0.5 sec, and tapered with a Hanning function. Mean absolute power (in squared micro-volts per Hertz) was computed within four frequency bands: delta (0.5–3.5 Hz), theta (3.5–7.5 Hz), alpha (7.5–12.5 Hz) beta (12.5–29.5 Hz). This was done separately for the ictal period and for two 10-sec periods (S1 and S2) following the ictal period. Ictal activity for the ECS and MST conditions was defined by off-line inspection of the EEG data, and secondarily by the time periods noted during the stimulation. The ictal period was more clearly visible in the EEG recordings of the ECS than in the MST condition. For the sham condition, the ictal period was defined as the sixty seconds time period one minute after injection of the anesthetic, approximating the times of occurrence of stimulation and seizure. In a preliminary analysis no difference was found in the ictal power measured at the left and right electrode locations, and therefore an average of the two measures was used in all subsequent analyses. Statistical analyses were performed on the logarithmically transformed EEG power.
EEG data were collected on each of the treatment days. However, due to technical failures and noise, data were not available for all subjects in all conditions and time periods. Therefore we selected six treatment sessions for which data were complete for all the subjects, conditions, and time periods. These days were 2, 4, 7, 10, 20 and 23. ANOVAs were performed using SPSS V. 15 for Windows. Omnibus analysis was based on a within-subject model, with the following factors: Frequency (delta, theta, alpha, beta), Condition (ECS, MST, sham), Period (Ictal, S1, S2) and day of Treatment (T1, T2, T3, T4, T5, T6). This analysis was followed by separate analyses for each of the frequency bands and for each condition. Where appropriate, significant main effects and interactions were followed-up with simple effects procedures and/or post-hoc analyses.
RESULTS
Figure 1 presents examples of EEG recordings for each condition and period. As expected, in the sham condition, when only anesthesia was given, EEG did not change over the recording time. In contrast, when ECS was administered, clear seizure activity followed by a postictal suppression period was observed. The EEG recordings following MST treatment were similar to those seen with ECS, although the amplitude of the seizure and the postictal suppression appeared attenuated. To quantify these observations the data were first submitted to omnibus repeated measures ANOVA and the results are presented in Table 1. Two main findings can be inferred from this ANOVA. First, the main effect and interactions with Treatment were not significant, indicating a lack of change in EEG expression over the course of treatment. Second, a three-way interaction of Condition, Frequency and Period indicated a difference in EEG expression as a function of all these factors. Thus, simple effects were performed for each condition. As was expected from Figure 1, for the sham condition, there was a main effect of Frequency (F3,3= 107, p<0.002), but no main effect of Period, indicating that EEG expression stayed the same over the recording period. In contrast, for the ECS condition, in addition to the main effect of Frequency (F3,3= 62, p<0.003), there was a main effect of Period (F2,2= 134, p<0.007) that post hoc testing indicated was due to greater power during the ictal period than both S1 and S2 periods. The analysis for the MST condition, yielded a main effect of Frequency (F3,3= 58, p<0.004), but no significant effect of Period indicating that the change in power between ictal and post ictal periods was not large enough to reach significance. A summary of the findings are depicted in Figure 2 which presents the power measured in each of the frequency bands for each of the time periods and conditions. It is clear that there was greater EEG power overall during the ictal period in the ECS compared to the MST and sham conditions. The reverse was true for the S1 and S2 periods, where there was greater reduction in power, or EEG suppression, for the ECS compared with the MST or sham.
Results of the omnigbus ANOVA ov the EEG power
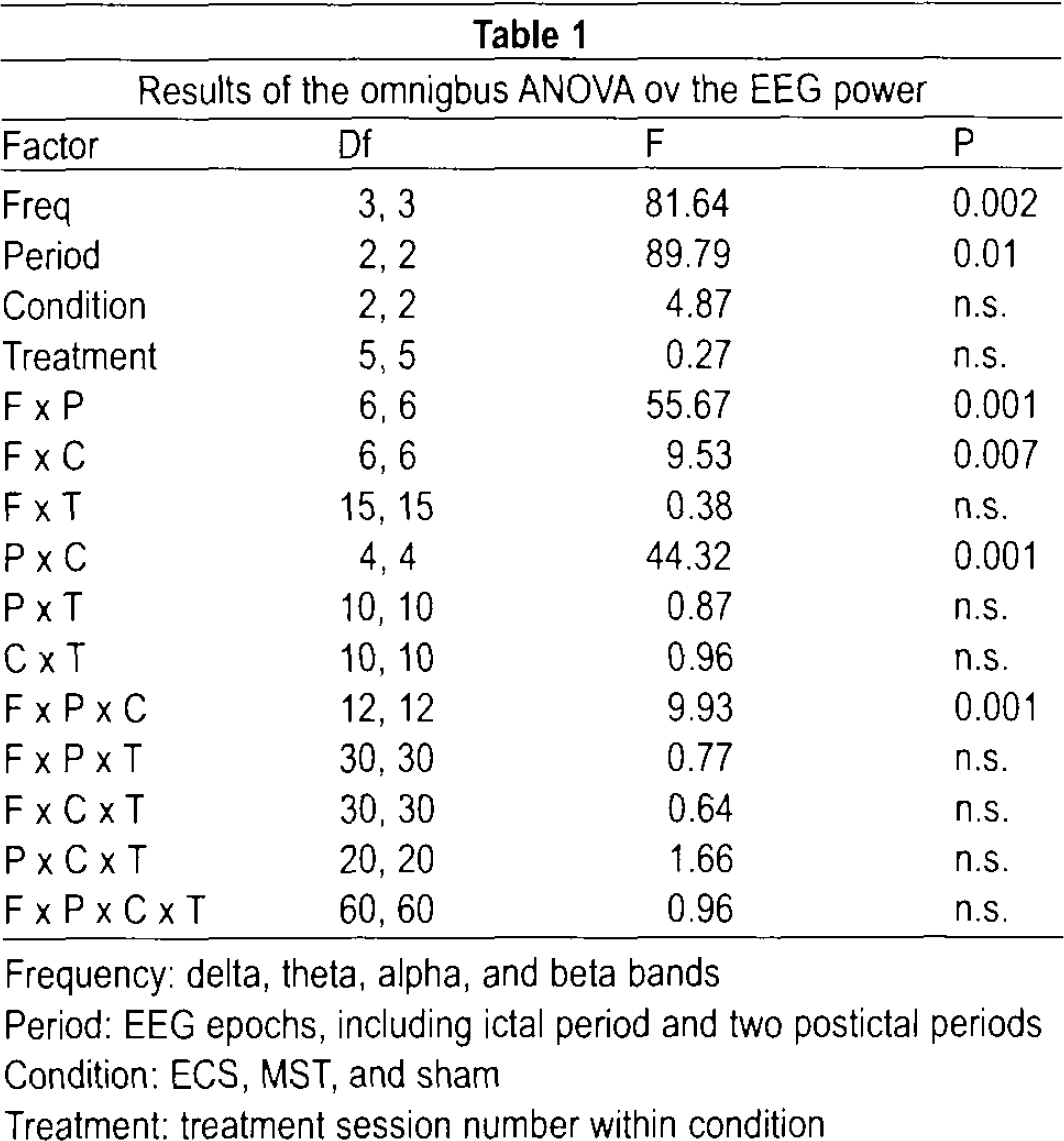
Frequency: delta, theta, alpha, and beta bands
Period: EEG epochs, including ictal period and two postictal periods
Condition: ECS, MST, and sham
Treatment: treatment session number within condition
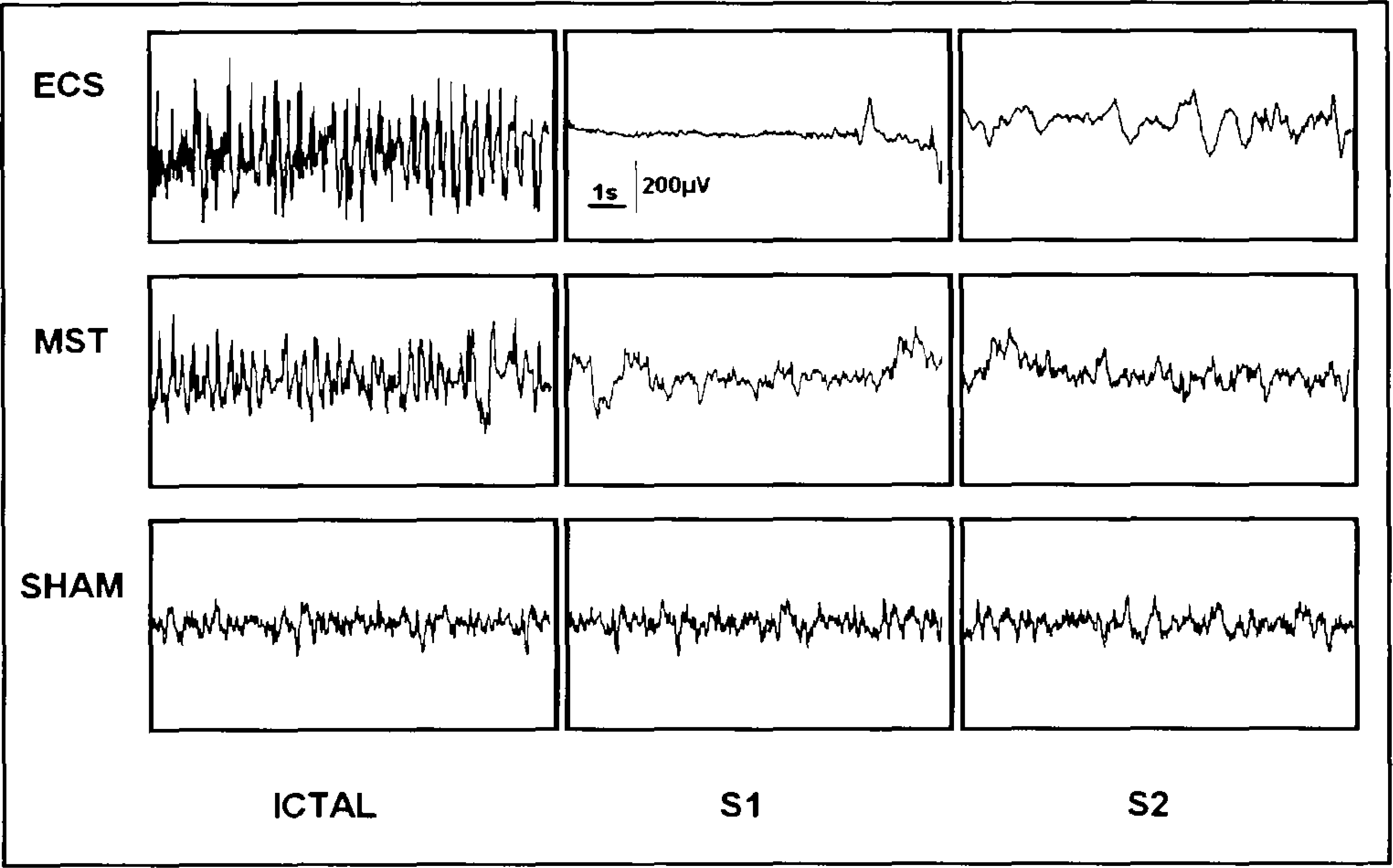
Examples of EEG recording for ECS, MST and sham conditions during the Ictal and Postictal (S1 and S2) periods. Each tracing represents a 10 second epoch.
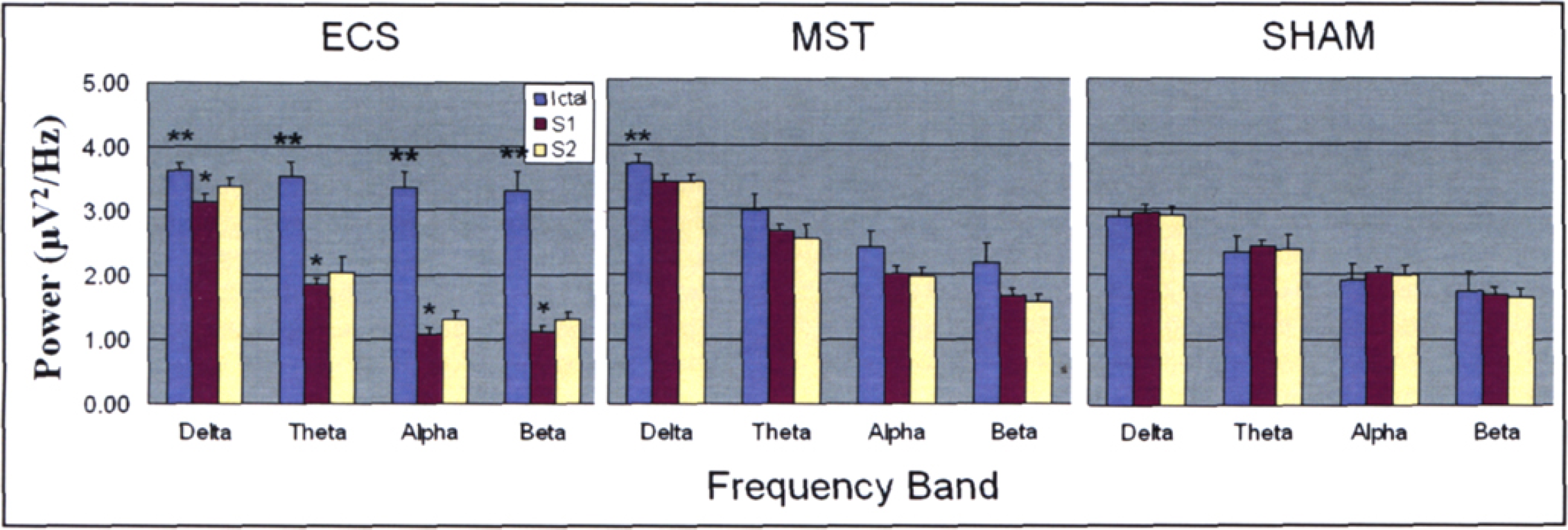
EEG power (Means and Standard Errors) for the four frequency bands and three time periods averaged over the six treatments for the ECS, MST and sham conditions. A significant difference from ictal at p< .05 is indicated by an asterisk. A significant difference from sham at p< .05 is indicated by two asterisks.
To further explore the main effects Frequency, additional ANOVAs were performed for each frequency band and the results are presented in Table 2. For all frequency bands the main effects of Period are modulated by the Period by Condition interactions. Only for delta band is there a main effect of Condition. To aid in parsing the Period by Condition interactions, simple effects analyses were performed. First, we performed analyses separately for each Condition (3 Periods by 6 Treatments), then for each Period (3 Conditions by 6 Treatments).
Results of the ANOVA of the EEG power
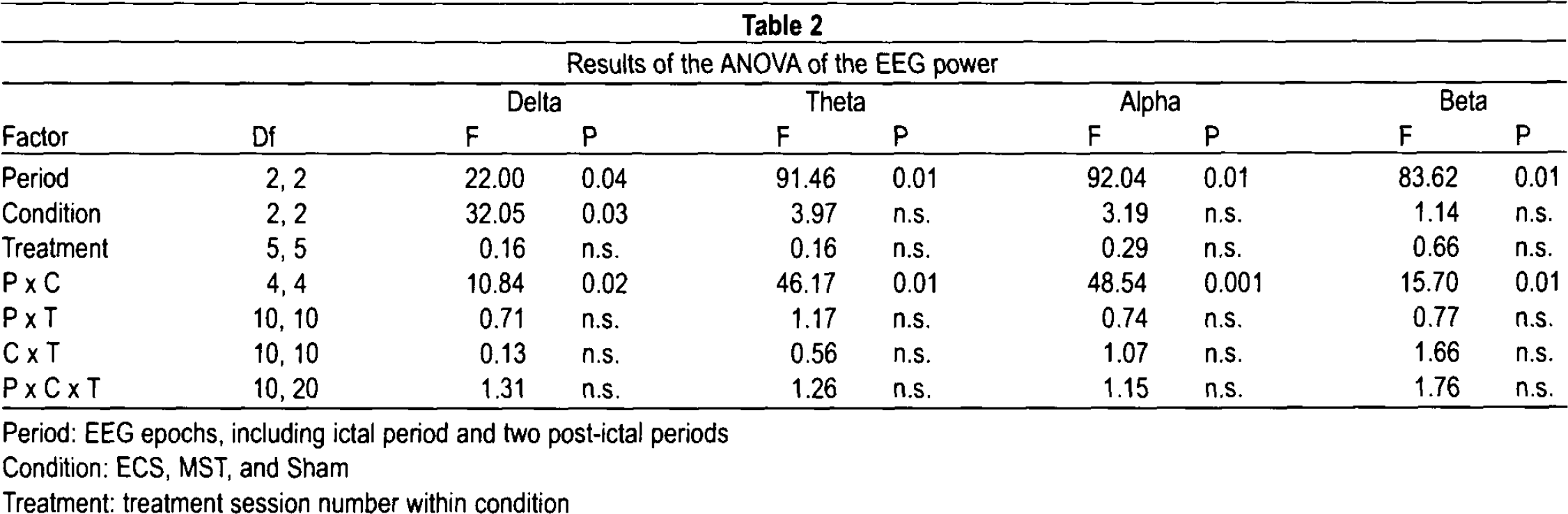
Period: EEG epochs, including ictal period and two post-ictal periods
Condition: ECS, MST, and Sham
Treatment: treatment session number within condition
For the sham we expected to see no difference across period in all the frequencies. Surprisingly, there was a main effect of Period in the theta band during sham; however, post hoc test indicated that this was due to smaller power during the ictal period compared to S1 and S2. In contrast, it was expected that for the ECS, in all frequency bands there would be a difference in EEG power between ictal and postictal period. This was confirmed by main effects of Period (for delta F2,2= 35, p<0.05; for theta F2,2= 501, p<0.01; for alpha F2,2= 221, p<0.01; for beta F2,2= 52, p<0.05). Post hoc analyses revealed that in all bands power during the ictal period was larger than power measured during the two post-ictal periods. For the MST condition, there were no main effects or interactions for any of the frequency band, suggesting no significant change in EEG power among the time periods.
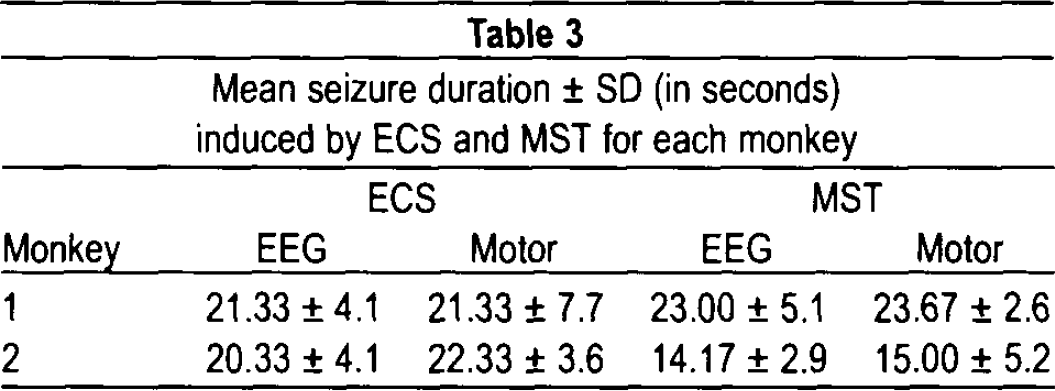
Analyses for each of the periods (Ictal, S1 and S2) revealed the following: For the Ictal period, there were main effects of Condition for the delta (F2,2= 117, p<0.01) and alpha bands (F2,2= 23, p<0.05), whereas main effect of condition approached significance (p=0.08) for the theta and beta bands. Inspection of the data revealed that these main effects were the results of a gradation in power in the theta, alpha and beta between the conditions, in which ECS always had higher power than MST which in turn was higher than that in sham. In the delta band, there was no difference in power between the ECS and MST condition, and both were greater than Sham. For the S1 and S2 periods, there was no significant difference among the three conditions in the delta band, but differences did emerge in the theta, alpha and beta bands, with smaller power in the ECS condition than in MST or sham. Table 3 presents the mean seizure duration induced by ECS and MST for each monkey. ANOVA on these data did not reveal any significant effects.
Mean seizure duration ± SD (in seconds) induced by ECS and MST for each monkey
DISCUSSION
The analyses of the EEG data provide additional support for earlier observations that MST- and ECS- induced seizures elicit differential patterns of EEG activation. The current data demonstrated that ictal EEG power was larger in ECS than in MST for all frequency bands with the exception of the delta band, for which MST actually had higher expression. The data also reflected differences in the post-ictal period for which there was a greater suppression of EEG power following ECS than following MST or sham in the theta, alpha and beta band (see Figure 2). These are the first EEG data in non-human primates that directly compared two convulsive treatments (ECS and MST). The fact that non-invasive measures of the neurophysiological characteristics mirrored those of invasive measures reported by Lisanby et al. 10 supports continuation of non-invasive measures as a means to further our knowledge regarding the neurophysiological impact of MST-induced seizure.
The present data do not speak directly to the treatment efficacy; however, they highlight interesting possibilities regarding EEG features associated with efficacy. As was mentioned above, clinical efficacy following ECT treatments was linked to a change in EEG delta power in prefrontal regions. 6,7 Interestingly, only for the delta band during the ictal period was there no difference in power between ECS and MST (and both were different than sham). Thus, these data suggest that MST retains an EEG characteristic related to clinical efficacy, while resulting in fewer cognitive side effects as seen in the prior report on these same subjects. 14 However, the clinical significance of these effects awaits examination in clinical trials.
Our data demonstrate clear differences between ECS and MST in post-ictal suppression. ECS-induced seizure resulted in a marked reduction in power while a change in power was not so pronounced following MST-induced seizure. The importance of the post-ictal suppression has been shown by Nobler et al. 16 and more recently Azuma and colleagues 17 who suggest that postictal suppression after ECT -induced seizure can predict therapeutic outcome. In both of those studies, EEG suppression was associated with better outcome. However, more recent work has challenged the proposed relationship with outcome. 9 It is possible that the relations among EEG characteristics and clinical outcome may differ for different modalities and may thus need to be empirically determined.
Limitations of this study include the small sample size, and risk of carry-over effects due to the within-subject cross-over design. Given the considerable individual differences in seizure expression with ECT, the within-subject design did have the strength of allowing each subject to serve as its own control, thereby reducing a source of variability. Another limitation in this study is the use of an MST dosage at 2.5 × seizure threshold. More recent work has examined the utility of higher dosages of MST, up to 6 × seizure threshold. 18 It is possible that higher dosage of MST may show a different pattern of effects than the moderate dosages studied here.
These results demonstrate the feasibility of conducting quantitative comparisons of the neurophsyiological characteristics of convulsive therapy in non-human primates, supporting future studies that may further probe the similarities and differences among various seizure induction techniques. The data also support significant differences between MST and ECS in seizure expression and post-ictal suppression. With larger sample size, it may become possible to link measures of cognitive outcomes to that of EEG expression during and following ECS and MST-induced seizure. The relevance of these differences to antidepressant outcome will await clinical trials in depressed patients.
Footnotes
ACKNOWLEDGMENTS
This research was supported by NIMH R01 MH60884. Support for the development of Magnetic Seizure Therapy has also come from the Stanley Medical Research Foundation, American Federation for Aging Research / Beeson Scholars Program, and the National Alliance for Research on Schizophrenia and Depression (NARSAD). The authors thank Mr. Matt Truesdale and Mr. Daniel Kaplan for their assistance in data analysis, and Mr. Niko Reyes for his assistance with research procedures.
DISCLOSURE AND CONFLICT OF INTEREST
Yael M. Cycowicz, Bruce Luber, Timothy Spellman have no conflicts of interest in relation to this article. For work unrelated to the present study, Dr. Lisanby has received research support from Magstim Company, Neuronetics, Cyberonics, NIH, AFAR, NARSAD, Stanley Medical Research Foundation, DARPA, and NYSTAR. Columbia University has filed a patent application for novel TMS technology developed in Dr. Lisanby's laboratory, not related to the topic presented here.