
Abstract
Medically intractable seizures appear to be highly correlated with focal slow activity (delta or theta). They also correlate highly with decreases in the coherence of theta. Normalization of focal slowing and of decreased theta coherence will probably be the neurofeedback approaches most likely to decrease or eliminate seizures in future cases.
Neurofeedback has been used for over 35 years to reduce the incidence and severity of seizures. With power training to decrease theta and increase the sensorimotor rhythm (12–15 Hz), an average of 82% of patients experienced a significant reduction in seizure frequency, and occasional remissions were seen. Recent improvements using QEEG to guide neurofeedback training have made it possible to eliminate seizures in most patients, even those with intractable seizures.
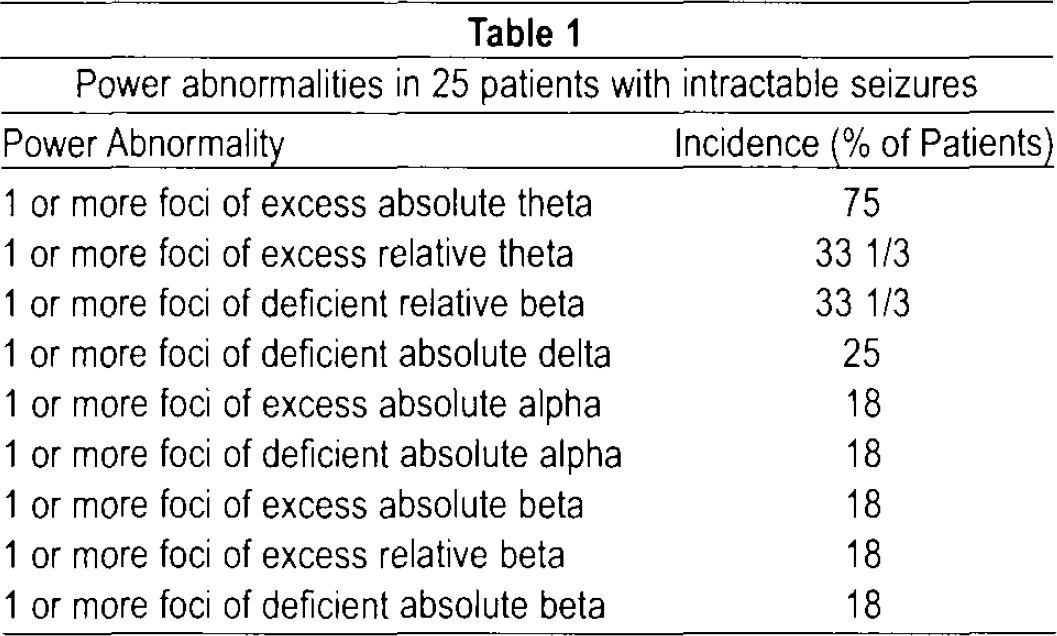
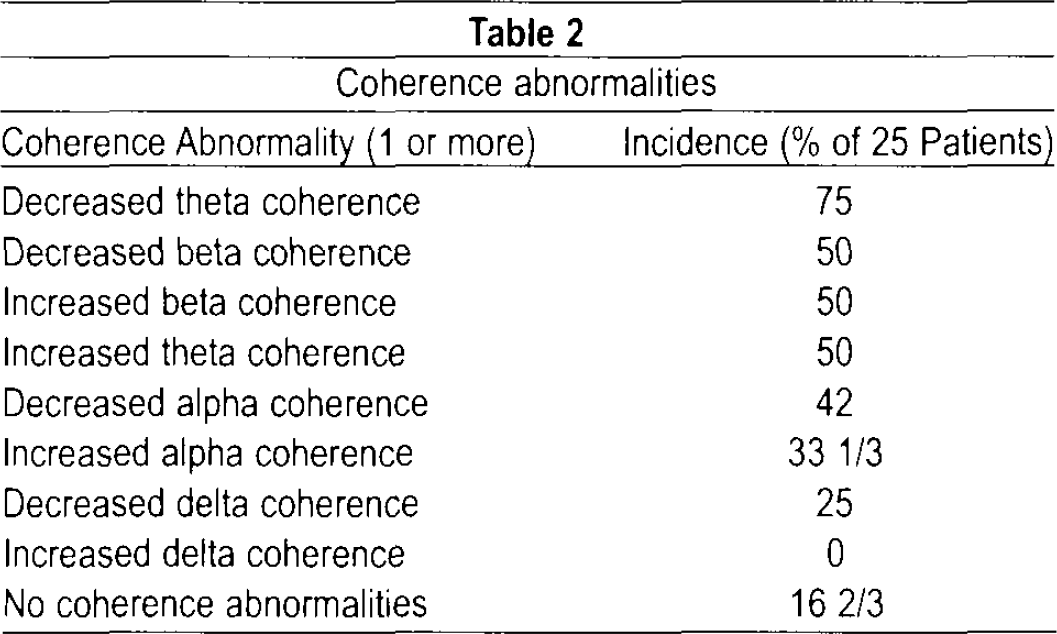
Following our previous study in 2005, we report an additional 25 patients so treated. We also report an analysis of the frequency of QEEG abnormalities in this patient group. All of the intractable epileptic patients had one or more slow foci (excessive theta or delta compared with the normal database). One third had a relative deficiency of beta power. One fourth had a deficiency of absolute delta. Eighteen percent had excessive absolute alpha power, 18% had deficient absolute alpha power, 18% percent had excessive absolute beta power, and 18% percent had deficient absolute beta power. Hypocoherence of theta was found in 75%, and decreases in alpha coherence were noted in 42%. Hypocoherence of beta was found in 50%, and hypocoherence of delta was found in 25%. Increases in alpha coherence were noted in 33%. Seventeen percent had no coherence abnormalities.
When most of the power and coherence abnormalities were normalized with neurofeedback training, all the patients became seizure-free; 76% no longer required an anticonvulsant for seizure control.
INTRODUCTION
Epilepsy which is not controlled with anticonvulsant medication is seen in a substantial percentage of epilepsy patients. 1 Some patients experience cessation of seizures after surgical treatment. 2 However, many patients continue to have seizures after surgery, and many others are not candidates for epilepsy surgery because of multiple areas of onset or an inconsistent spike focus. Vagal nerve stimulation can control seizures in some patients. 3 There remain a large number of patients who continue to have seizures after all of these measures. Neurofeedback can substantially reduce the frequency of seizures. 4 If quantitative EEG (QEEG) is used to guide neurofeedback training, most patients with intractable epilepsy become seizure-free. 2
The first study of QEEG in epilepsy was reported by Lombroso and Duffy in 1982. 6 Subsequent studies were carried out by Harner, 7 Coppola, 8 Baldy-Molineri et al., 9 and Nuwer. 10 These early studies reported mild to moderate increases of the spectral energy component in the theta range. Diaz and colleagues 11 found not only increased relative power in the theta band, but decreased values for absolute power in the alpha band. These deviations from normality were widespread over the scalp and were not related to antiepileptic medication. Similar findings were noted in patients with and without paroxysmal activity in their electroencephalograms (EEGs). The most striking finding was that epileptogenesis may have a generalized impact on the frequency components of EEG.
The purpose of this paper is to report QEEG abnormalities in a group of medically refractory epilepsy patients. We studied and followed these patients using QEEG findings to guide neurofeedback training and to determine its usefulness in remediation of seizures.
METHODS
Twenty-five patients (ages 20–55 years, 15 females and 10 males) with intractable seizures were studied and treated with neurofeedback training. All were having 1 or more seizures per month despite trials of 3 different anticonvulsants in therapeutic doses, often in combination. They had either partial complex seizures, 6 partial complex seizures with secondary generalization 8 or primary generalized seizures. 11 Soon after their first visit to our clinic, each patient had a QEEG. After artifacting, the data were analyzed using the NX Link Database. 12 Patients then had 17–82 sessions of neurofeedback training, using Brainmaster® equipment and software. Each protocol consisted of 5 sessions. The four most statistically significant power abnormalities were trained. Four subjects experienced remission of seizures with power training alone. The remaining 21 patients were then trained to normalize the four most statistically significant coherence abnormalities. If seizures continued, the QEEG was repeated and an additional 20–40 sessions of power and coherence training were done based on the persistent abnormalities.
RESULTS
When both power and coherence abnormalities were corrected with neurofeedback training, all the patients experienced a remission of their seizures, which had persisted for 3–11 years (average 5.1). Nineteen of the 25 patients (76%) no longer required an anticonvulsant to control their seizures. Six have required a single anticonvulsant to maintain a seizure-free state and have remained so for 2 years or longer.
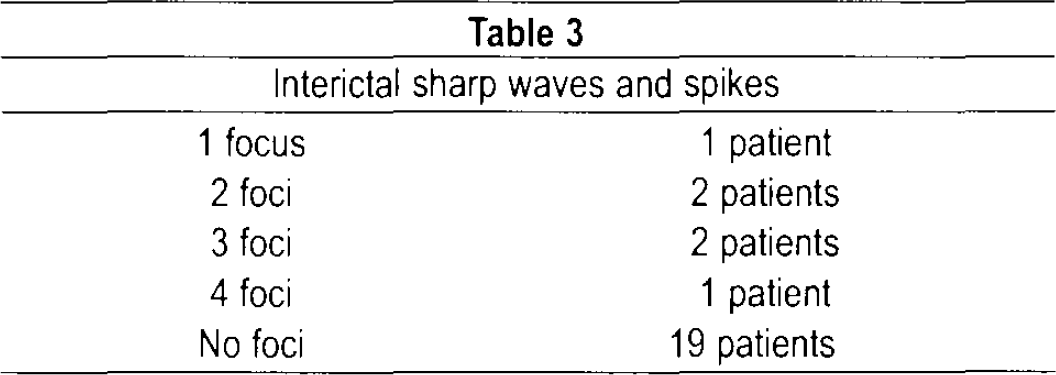
Table 1 shows the incidence of various power abnormalities in these 25 intractable seizure patients. Some abnormalities had no foci. Table 2 indicates the coherence abnormalities and Table 3 indicates the incidence of epileptiform abnormalities in these patients. Previous experience has demonstrated that neurofeedback training over the spike focus is not usually effective in eliminating seizures. 4,5 In any case, this would not have been an option in those patients who did not have interictal foci.
Power abnormalities in 25 patients with intractable seizures
Coherence abnormalities
Interictal sharp waves and spikes
DISCUSSION
QEEG-guided neurofeedback training is an effective approach to reduce medically intractable seizures. At the completion of neurofeedback treatment, 100% of our patients were no longer experiencing seizures. Following neurofeedback training their medications were tapered and stopped. If a seizure occurred, a single anticonvulsant was restarted at the previously effective dosage. Seventy-six per cent were seizure free and no longer required medication for control of seizures, while 24% required only a single anticonvulsant for seizure control. All had previously had one or more seizures per month on 1–3 medications in therapeutic doses. No adverse effects or complications occurred. Normalization of focal slow activity and decreased coherences of theta were most likely to result in fewer or no seizures.
QEEG-guided neurofeedback represents an attractive alternative to drug treatment for seizures. The majority of our patients became seizure free and medication free. In medication-resistant patients, this treatment represents a particularly attractive alternative to epilepsy surgery, which is invasive and expensive, and is not always effective. Neurofeedback is a noninvasive and relatively inexpensive way to accomplish the same goal as surgery—freedom from seizures. The success rate appears to be higher with neurofeedback vs. surgery. Neurofeedback training also represents a good alternative for those patients with intractable seizures who do not have epileptic foci, as was the case in 19 of our 25 patients. It remains to be seen if this approach will be equally successful in all patients who do have one or more clear-cut epileptic foci, but it was successful in all 6 of our patients who had clear-cut foci.
CONCLUSION
Medically intractable seizures appear to be highly correlated with focal slow activity (delta or theta). They also correlate highly with decreases in the coherence of theta. Normalization of focal slowing and of decreased theta coherence will probably be the neurofeedback approaches most likely to decrease or eliminate seizures in future cases.
DISCLOSURE AND CONFLICT OF INTEREST
Jonathan E. Walker is associated with the Neurotherapy Center of Dallas, Inc. and has no conflicts of interest in relation to this article. This study was not funded. It has not been previously presented at a meeting.