
Abstract
The availability of video electroencephalography monitoring (VEEGM) in neurological intensive care units has allowed the recognition and treatment of nonconvulsive status epilepticus (NCSE). However, little is known about characteristics, management, and outcomes in patients with NCSE in developing countries. We retrospectively reviewed the video-EEG reports of 120 patients who were monitored from November 2009 to March 2013. Indications for video-EEG were mostly unexplained alterations of consciousness or witnessed convulsive seizures. We identified the clinical characteristics, treatment regimes, and outcomes of patients with NCSE and tried to determine which parameters were associated with prognosis. NCSE was detected in 12/120 (10%) patients (3 females, 9 males; age 24-86 years). Admission diagnoses were: stroke (3), epilepsy (3), autoimmune limbic encephalitis (3), herpes encephalitis (1), presumed encephalitis-cardiac arrest (1), and malignancy (1). Eight patients had witnessed convulsive seizures before video-EEG. Interictal periodic epileptiform discharges were detected in 9 patients. In one-third of patients, ≥2 EEG recordings were required to capture seizures. In addition to anticonvulsants, 3 patients received immunosuppressive therapy, while intravenous anesthetics were given to 7 patients. Four patients (33.3%; 1 female, 3 males; age 51-67 years; etiology: stroke, autoimmune encephalitis, encephalitis-cardiac arrest, and malignancy; Glasgow coma scale (GCS) score <8 in 3 patients; all had periodic discharges; intravenous anesthetics were used) died in the intensive care unit. NCSE is not an infrequent finding in neurological intensive care units, thus necessitating prolonged video-EEG monitoring in patients at risk. Witnessed convulsions may indicate the presence of nonconvulsive seizures in patients with altered consciousness. Repeated recordings may increase the detection of ictal events. Periodic epileptiform discharges are commonly observed and may predict poor prognosis. Mortality seems to be influenced mostly by the underlying etiology.
Introduction
NCSE has been defined as a state of nonrecovery between seizures without convulsions, usually for more than 30 minutes.1,2 It is estimated to account for 20% to 63% of all status epilepticus (SE) cases. 3 Diagnosis is largely based on EEG since the clinical manifestations are pleomorphic. After the introduction of video-EEG monitoring (VEEGM), there has been increased identification of NCSE in lethargic or comatose patients in intensive care units (ICUs). 4 Early recognition and treatment have been associated with better outcome in some patients. 5 Although there are plenty of data on NCSE from developed countries,4-13 very little is known about the incidence, patient characteristics, treatment, and outcome in emerging countries. 14 Our objective was to identify the incidence of NCSE in the neurological ICU (NICU) of a tertiary referral center in our Turkey, and determine patients’ profiles and parameters related to outcome.
Patients and Methods
The study cohort was selected among consecutive patients who underwent continuous VEEGM in our adult NICU between November 2009 and March 2013. Indications for VEEGM were mostly an unexplained decrease in the level of consciousness in patients with ischemic or hemorrhagic stroke, toxic–metabolic encephalopathy, central nervous system infection, and hypoxic–ischemic encephalopathy. Five patients were diagnosed before admission to the NICU, either in the emergency department (n = 3) or referring center (n = 2). The underlying etiology of NCSE was explored and treated accordingly when identified. Laboratory investigations included routine blood tests, metabolic profile, neuroimaging (magnetic resonance imaging and/or compute tomography) and other appropriate tests, including lumbar puncture. Patients’ clinical information was collected by chart review and included age, gender, primary diagnosis that led to NICU admission, neurologic status, and GCS at the initiation of monitoring, seizure/epilepsy history, coexisting convulsive seizures before or during VEEGM, time of recording the first seizure, number of episodes and total duration of monitoring, neuroimaging findings, type of anticonvulsants and anesthetics used, and outcome (assessed as modified Rankin score [mRS]) at discharge from NICU.
Continuous video-EEG (Grass Telefactor Comet, West Warwick, RI) was recorded using 21 electrodes arranged according to the International 10-20 System. Filter settings were 1 to 70 Hz, sampling rate was 200 Hz, and sensitivity was adjusted accordingly. Interelectrode impedances were initially <5 kohm. Video-EEG monitoring was available 24 hours per day and 7 days a week. In all the patients, EEG recordings were evaluated once a day. Quantitative EEG analysis was used online in some, and off-line in all the patients to facilitate seizure recognition. Nonconvulsive seizures were defined electrographically according to published criteria as rhythmic discharges with evolution in frequency, amplitude, and morphology lasting at least 10 seconds. 15 Therefore, we excluded patients with hypoxic–ischemic encephalopathy who displayed burst-suppression pattern or generalized periodic discharges <3 Hz. Patients with stimulus-induced rhythmic, periodic, or ictal discharges were not included. We also recorded the presence of periodic epileptiform discharges (PEDs) interictally. All recordings were interpreted by an experienced electroencephalographer (ND). Categorical variables were expressed as n (%) and continuous variables as median (interquartile range [IQR]). The study was approved by the university’s research ethics board.
Results
Out of 120 patients, we identified 12 (3 females, 9 males; age 24-86 years, median = 58 years, IQR = 43-64 years) who fulfilled the above criteria of NCSE (Table 1). Duration of stay in NICU varied from 5 to 131 days (median = 14.5, IQR = 13.5-37.5). Duration of VEEGM was 28 to 372 hours (median = 70.5, IQR = 60-185) hours, and number of episodes was 1 to 6 per patient (median = 2, IQR = 2-3). Five patients had complex partial SE, and 7 patients were diagnosed as NCSE in coma.
Clinical Characteristics of the Study Group.
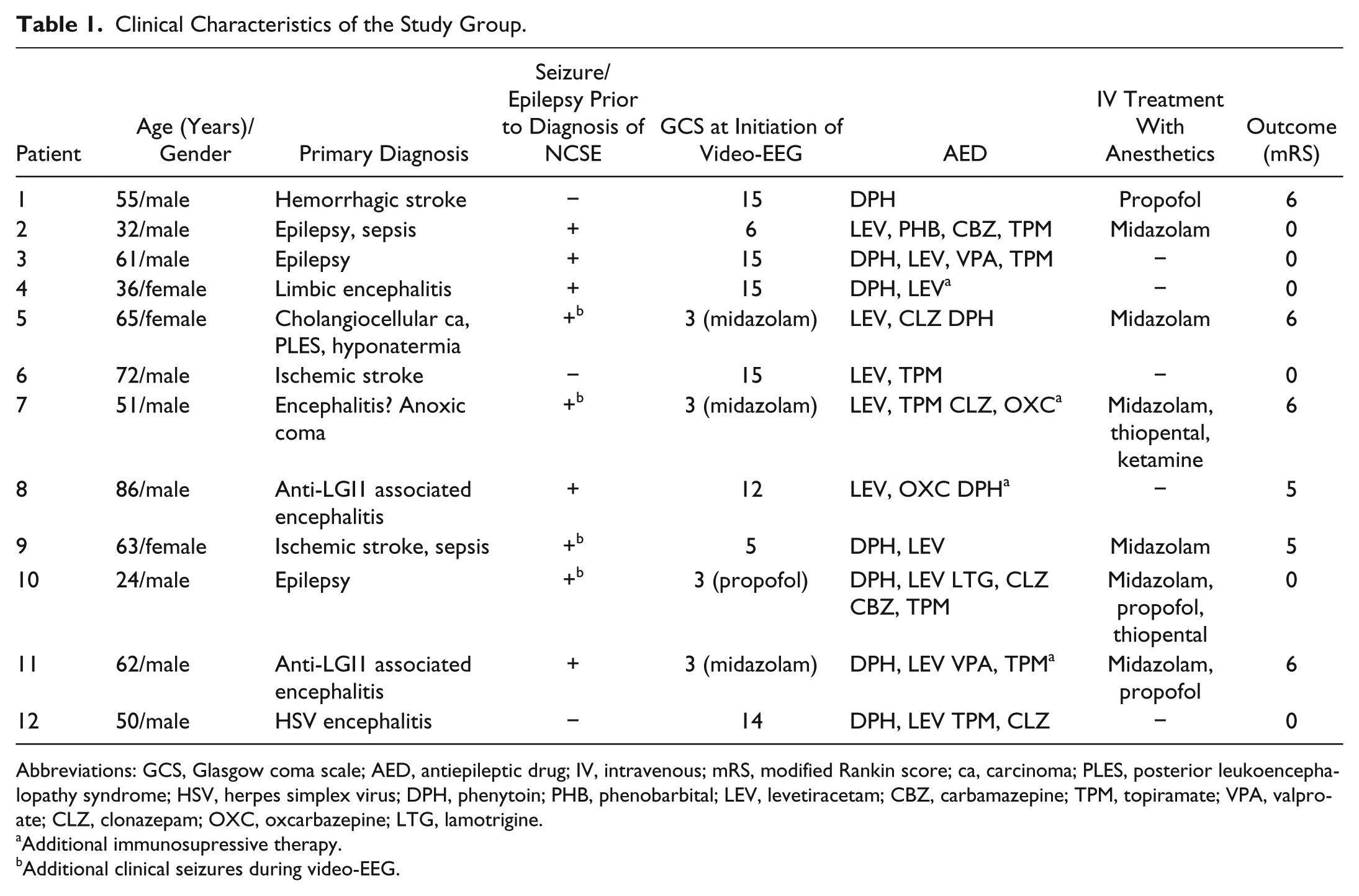
Abbreviations: GCS, Glasgow coma scale; AED, antiepileptic drug; IV, intravenous; mRS, modified Rankin score; ca, carcinoma; PLES, posterior leukoencephalopathy syndrome; HSV, herpes simplex virus; DPH, phenytoin; PHB, phenobarbital; LEV, levetiracetam; CBZ, carbamazepine; TPM, topiramate; VPA, valproate; CLZ, clonazepam; OXC, oxcarbazepine; LTG, lamotrigine.
Additional immunosupressive therapy.
Additional clinical seizures during video-EEG.
Admission diagnoses were stroke in 3 patients (2 ischemic, 1 hemorrhagic). Three patients had epilepsy; 1 was initially hospitalized elsewhere and transferred to our center due to sepsis and refractory SE. Autoimmune encephalitis was diagnosed in 3 patients. Two of them had anti-LGI-1 antibody related autoimmune encephalitis. In the third case, extensive investigations for infectious, paraneoplastic or nonparaneoplastic etiologies were negative. Another patient had a history of presumed encephalitis and suffered cardiac arrest in the ICU where he was followed; the patient was referred to our center several weeks later due to refractory SE. One patient was diagnosed as herpes simplex encephalitis. The last patient had multiple co-morbid disorders such as cholangiocellular carcinoma, posterior leukoencephalopathy syndrome, intracerebral hemorrhage, and hyponatremia. Apart from the primary diagnosis, 2 patients (patients 2 and 9) were in sepsis. In fact, patient 9 developed a convulsive seizure after the initiation of ertapenem, and although she was already in coma, the neurointensivists were suspicious of ongoing nonconvulsive seizures that were captured after VEEGM. Overall, 9 patients (75%; 2 epileptic and 7 nonepileptic) had witnessed convulsive seizures before (n = 8) and/or during (n = 4) VEEGM. Interictally, PEDs were detected in 9 (75%) patients and were focal in 7 and generalized in 2 (Table 2). Duration of seizures usually varied between 1 and 2 minutes and lasted for 11 to 120 hours with different frequencies. Five patients had bilateral independent seizures, as well as lesions in both hemispheres. In 5 patients (41.6%; patients 2, 3, 5, 9, and 11) the seizures had a cyclic pattern (Figure 1), as previously described by Friedman et al. 16 The seizures were recorded within the first hour of VEEGM in 7 patients (58.3%). In 1 patient, the first seizure was recorded at the 34th hour of continuous EEG. In the remaining 4 patients (33.3%), the seizures were captured at the second (n = 2; 6th and 10th days of hospitalization) or fourth (n = 2; 18th and 28th days of hospitalization) episode of VEEGM.
EEG Characteristics and Imaging Findings of the Patients in the Study Cohort.
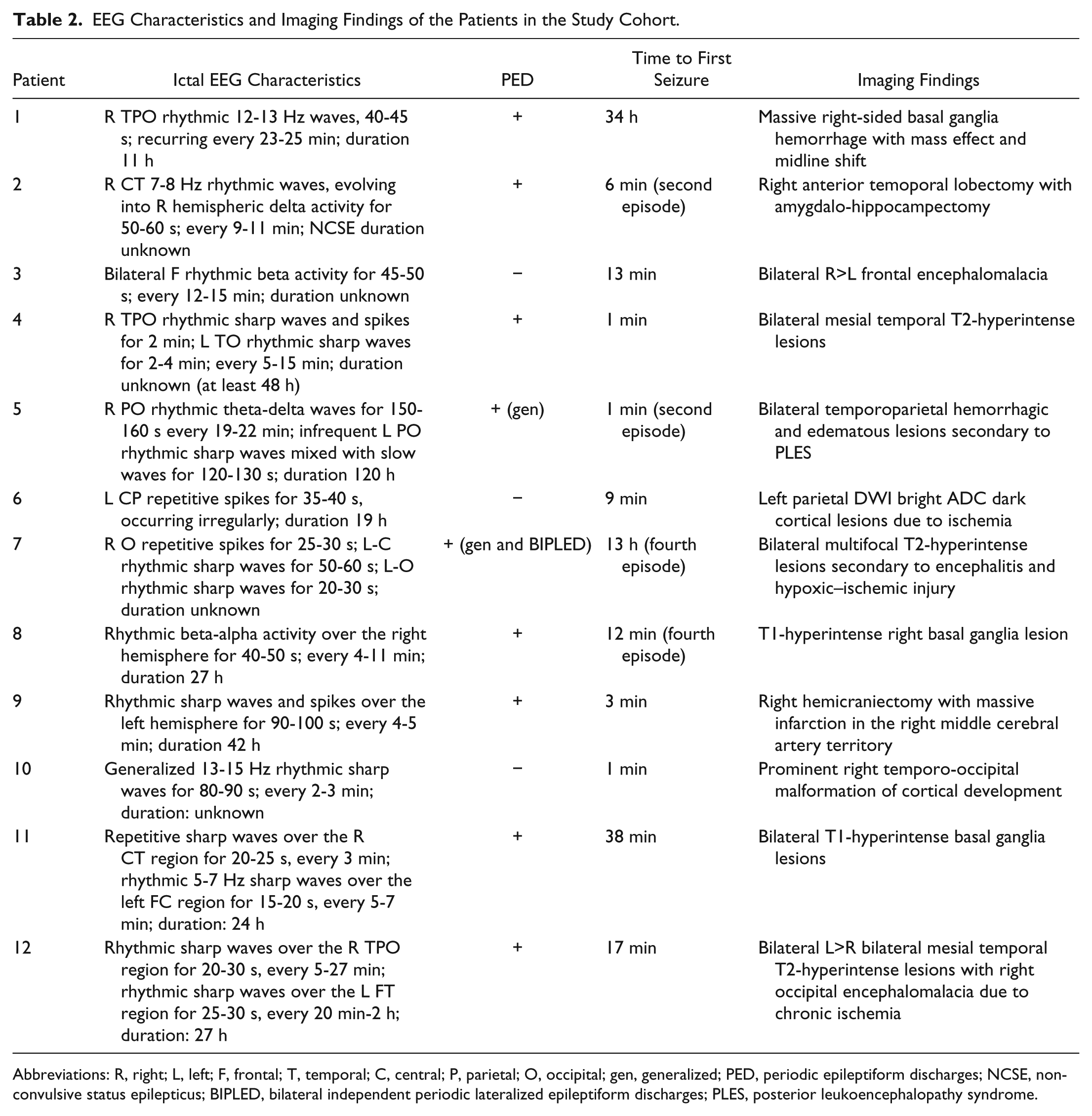
Abbreviations: R, right; L, left; F, frontal; T, temporal; C, central; P, parietal; O, occipital; gen, generalized; PED, periodic epileptiform discharges; NCSE, nonconvulsive status epilepticus; BIPLED, bilateral independent periodic lateralized epileptiform discharges; PLES, posterior leukoencephalopathy syndrome.
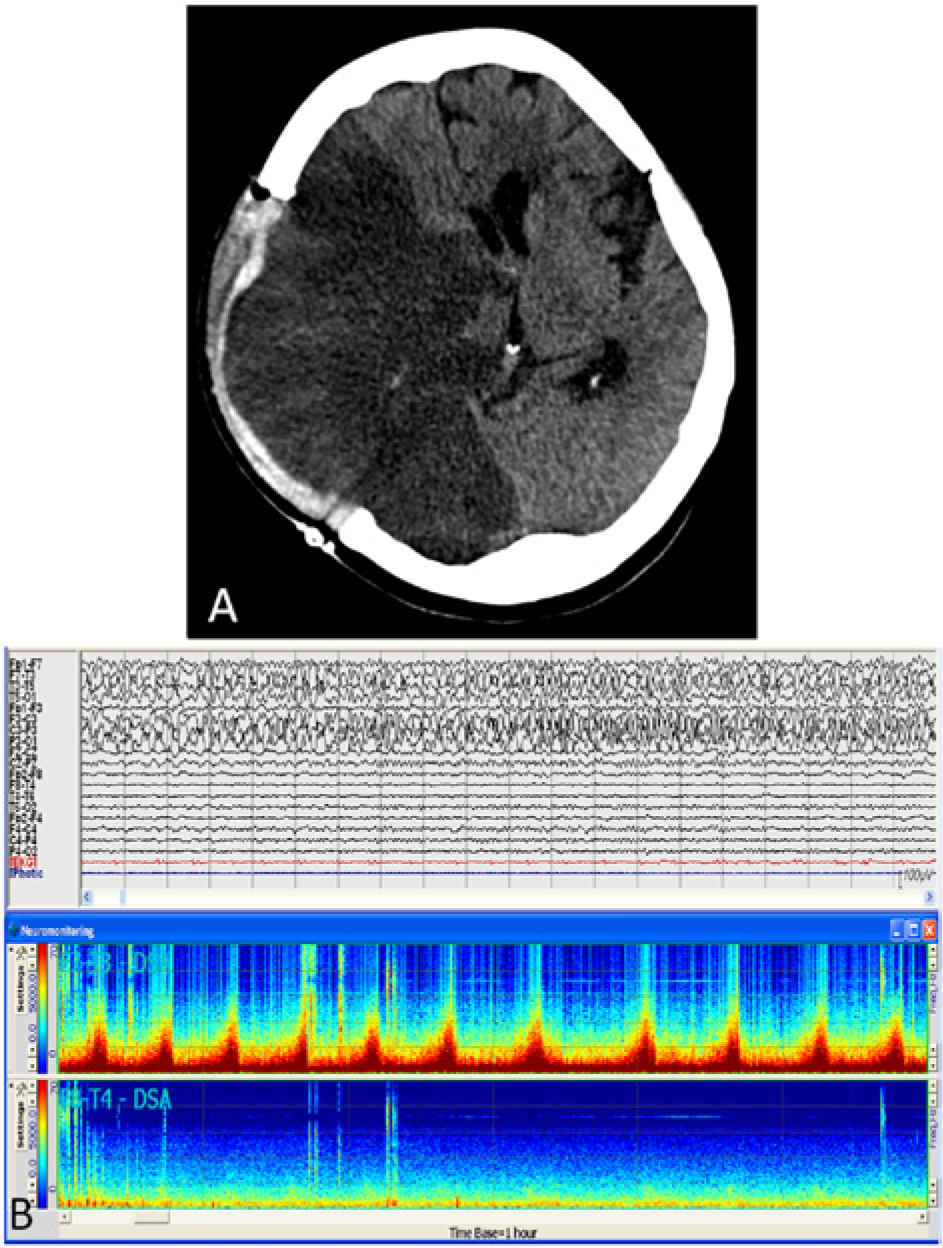
Axial computed tomography scan of patient #9 reveals massive infarct in the right middle cerebral artery territory, together with a craniectomy defect in the skull (A); an ictal pattern characterized by repetitive sharp waves and spikes over the left hemisphere in a longitudinal bipolar EEG montage (B; upper panel), background activity is considerably depressed over the right hemisphere due to severe tissue destruction, with lack of prominent ictal patterns; cyclic seizures are evident on density spectral array (F7-T3 and F8-T4) over the left hemisphere (B; lower panel; time base = 1 hour).
At the onset of monitoring, GCS score was <8 in 6 patients (50%), with 4 of them on midazolam. Three more patients received intravenous (IV) anesthetics after the diagnosis of NCSE in NICU. Four patients with noninfectious encephalitis also received immunosuppressive treatment (pulse steroid, IV immunoglobulin, and plasma exchange; alone or in various combinations). Midazolam was the initial anesthetic and was followed by propofol and/or thiopental, respectively. One patient was also given ketamine. Ambulatory patients received IV diazepam and phenytoin, followed by loading doses of PO (per os) antiepileptic drugs (AEDs), without further aggressive treatment. All the patients were given maintenance PO anticonvulsants.
Four patients (33.3%; 1 female, 3 males; mean age = 61 years; mean stay in NICU = 38 days; etiology: hemorrhagic stroke, encephalitis-cardiac arrest, anti-LGI1 related encephalitis, and malignancy; GCS at VEEGM onset: <8 in 3 patients; all of them had PEDs; IV anesthetics were used in all) died in NICU. In the rest, the mRS at discharge was either 0 (n = 6; 50%) or 5 (n = 2; 16.6%). The mRS in all the patients with complex partial SE was 0, at discharge from NICU.
Discussion
We reviewed one medical center’s experience with well-documented NCSE in the NICU. Prolonged VEEGM findings in our prospectively collected series of patients indicate that the incidence of NCSE was 10%. The majority of patients were male. Most common primary diagnoses were stroke, epilepsy, and encephalitis. About two-thirds of patients had witnessed convulsive seizures before the initiation of monitoring. In one-third of the study group, ≥2 recording sessions were required to capture seizures. The level of consciousness was considerably impaired in half of the patients. Intravenous anesthetics were used in 58%, and all of them were given maintenance PO/IV anticonvulsants. Mortality rate was 33%.
Recent technical improvements have allowed the implementation of VEEGM in ICUs leading to increased diagnosis and management of NCSE. 4 In ICU patients with unexplained coma and no clinical signs of seizure activity, Towne et al 8 have reported the frequency of NCSE as 8%. In other series, the numbers vary between 9% and 37%,4,9,14,17,18 probably owing to different patient characteristics or methodological issues. Despite the small number of patients in our series, the frequency of NCSE in our NICU was very similar to some other studies.14,17
Unlike the previous study from a developing country where most of the patients had central nervous system infection and venous thrombosis, 14 in our series etiologies were mostly stroke, epilepsy and predominantly autoimmune encephalitis. This patient profile resembles those in developed countries, where most cases occur due to cerebrovascular disorders8,10,12,17,19 or epilepsy,12,19 after excluding hypoxic–ischemic encephalopathy. Autoimmune encephalitis was another common cause of NCSE in our NICU, making up 25% of the cases. This may be because of recent advances in immunology that allow prompt recognition of clinical features and definitive diagnosis of the patients that may have been overlooked in the past. In our series, only 1 patient (<10%) had viral encephalitis. Infection has been reported as a rare cause in developing countries, constituting 5% to 10% of the patients with NCSE.6,9,17 Antibiotics have been blamed in about 10% of SE cases, 20 which again occurred in 1 patient in our series. In fact, she captured the neurointensivists’ attention after she had a single convulsive seizure. In previous studies, clinical seizures were reported to precede EEG documentation of NCSE in 76% to 84% of the patients,6,10 which is similar to our observation of 66%. Therefore, earlier seizures should raise the possibility that a persistently abnormal mental status could be due to ongoing nonconvulsive seizures. In patients with NCSE, the first seizure is usually detected within the first hour in about 55% of the cases9,14 and within 24 hours in 88% of all patients. 9 Like previous reports we recorded the first seizure within the first hour in 58% of our patients. However, in one-third of the cases in our series, ≥2 monitoring sessions were necessary to detect the first ictal EEG, implying that we should keep investigating patients at risk.
It is generally accepted that NCSE in ambulatory patients (ie, absence and complex partial SE) can readily be treated with AEDs, without necessitating aggressive intervention with IV anesthetics in most patients. 12 There is, however, no consensus on whether or how to treat NCSE in coma. It is claimed that EEG patterns in these patients might reflect the end stages of a severely damaged brain and many of these patients die of severe underlying causes regardless of treatment,21,22 while others believe that continuous seizure activity may lead to raised intracranial pressure and increased metabolic demand, potentially causing further neuronal damage.23,24 In accordance with the above statement, all the patients with complex partial SE in our series were treated with PO AED polytherapy and were discharged without deficit. All the patients who died, on the other hand, were given IV anesthetics that failed to halt the grave prognosis related to severity of the underlying disease or comorbid conditions. Three more patients received IV anesthetics. In 2 of them the underlying etiology was epilepsy, and both were discharged with full recovery. The third patient was already in coma because of cerebrovascular disease and comorbid medical disturbances; the cause of NCSE was antibiotic therapy. The seizures subsided after removal of the offending drug and IV midazolam infusion; she was discharged with severe morbidity due to the underlying disorder.
In NCSE, the reported mortality rates vary from 14% to 67%,5-10,12,14,19 depending on patient characteristics and study design. The mortality rate among critically ill cases is much higher (50% to 61%)5,7,12 when compared with ambulatory patients (6% to 30%).12,25 The following characteristics have been associated with mortality in SE: etiology,5-7,9,13,26-28 age,9,26,28,29 the presence of acute life-threatening complications,6,7 severe mental status impairment,5-7,26,28 delay in diagnosis, 5 seizure duration,5,27 and refractory SE. 28 Nonetheless, it has also been reported that duration27,30 and type26,27 of SE, gender, 26 time to treatment, 26 and presentation with coma 27 are not associated with mortality, especially once etiology is accounted for. An invariable finding is that mortality is low when the cause of NCSE is preexisting epilepsy.6,31,32 As far as the EEG findings in SE are concerned, it has been reported that the type of EEG discharge is unrelated to mortality, 6 whereas others have claimed that PEDs33,34 and generalized EEG patterns 7 are related to poor outcome. In our series, PEDs were a common finding and presented in all fatal cases. However, the small number of patients precludes definitive conclusion regarding their prognostic value. Cyclic seizures on the other hand, were observed in about 40% of our patients; a heterogeneous subgroup with regard to age, gender, etiology, and prognosis. Previously, the frequency of this pattern in NCSE was reported as almost 6% 16 ; however, compressed spectral array was not always used in conjunction with EEG, and therefore this frequency may be an underestimate, as the authors have indicated. Our findings suggest that cyclic pattern may be more common in NCSE; nevertheless, the underlying pathophysiology and significance of cyclic seizures are still unknown and await further investigations.
It is not clear if treatment alters outcome. 10 Earlier diagnosis and treatment have been reported to improve prognosis5,35,36; however, others have emphasized that etiology is an independent predictor of mortality, 10 regardless of treatment. Higher doses or greater number of AEDs were not shown to improve prognosis, and aggressive treatment prolonged ICU stay. 7
Our study has certain limitations. Like most of the previous publications, the results in our study are biased by the neurointensivists’ level of suspicion, and therefore may underestimate the real frequency of NCSE. The number of patients is small compared with other studies; however, we excluded patients who were monitored in the medical or neurosurgical ICU. Also, patients with hypoxic–ischemic encephalopathy, known to comprise most of the patients in some series, were not also included. Many authors believe that these patients should not be included in SE studies, because they already have a severe brain damage that determines the grave prognosis itself, and EEG findings are merely a reflection of the disorder rather than ongoing epileptic activity. Even though the number of patients in our series was small, our findings were in accordance with most of the previous studies from developed countries. To the best of our knowledge, this is the first study investigating NCSE with prolonged VEEGM in adult NICUs in Turkey.
In summary, the frequency of NCSE in our NICU was 10%; with 33% mortality rate, which seemed to correlate mostly with the underlying etiology. Our results are in agreement with the findings in developed countries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received financial support, for the research, authorship, and/or publication of this article, from the Hacettepe University Research Fund Grant No. 1-801 105 001 (Dr Nese Dericioglu).