
Abstract
Disturbances of the autonomic nervous system (ANS) are common in neuropsychiatric disorders. Disease specific alterations of both sympathetic and parasympathetic activity can be assessed by heart rate variability (HRV), whereas electrodermal activity (EDA) can assess sympathetic activity. In posttraumatic stress disorder (PTSD), parasympathetic HRV parameters are typically decreased and EDA is increased, whereas in major depressive disorder (MDD) and dissociation, both parasympathetic and sympathetic markers are decreased. ANS abnormalities have also been identified in psychogenic nonepileptic seizures (PNES) by using HRV, indicating lower parasympathetic activity at baseline. In addition to reviewing the current literature on ANS abnormalities in PTSD, MDD, and disorders with prominent dissociation, including borderline personality disorder (BPD), this article also presents data from a pilot study on EDA in patients with PNES. Eleven patients with PNES, during an admission to our epilepsy monitoring unit (EMU), were compared with 9 with generalized tonic-clonic seizures (GTCS). The area under the EDA curve, the number of EDA responses lasting longer than 2 seconds, and the number of EDA surges during sleep (sympathetic sleep storms) were calculated on ictal and interictal days by an automated algorithm. EDA changes in PNES patients did not follow a systematic pattern of sympathetic hyperarousal (like EDA after GTCS) but were more variable. How specific PNES semiologies, and/or underlying neuropsychiatric disorders, may influence ictal and interictal EDA patterns, and lead to a novel diagnostic biomarker remains to be evaluated in future larger studies.
Keywords
Introduction
Disturbances of the ANS have been increasingly recognized in many neuropsychiatric disorders, including PNES. Initial observations such as tachycardia in PTSD, and similar conditions, are now supplemented with more sophisticated and detailed parameters of the ANS. These biomarkers not only contribute to a pathophysiological understanding of neuropsychiatric syndromes, but also serve as an adjunctive diagnostic tool. In this article, we provide a focused overview of various ANS biomarkers, and the current literature on ANS dysfunction in neuropsychiatric disorders, specifically PTSD, MDD, and dissociation, to contextualize the literature describing ANS disturbances in PNES. We also present pilot data on EDA in patients with PNES, and suggest future approaches.
Parameters of the ANS
For a considerable time, the ANS has been of interest in neurological and neuropsychiatric diseases. It is widely recognized that ANS dysfunction may be associated with many neurological disorders, especially conditions presenting with paroxysmal symptoms, including epilepsy. Autonomic disturbances in epilepsy may be directly involved in the pathogenesis of the disorder, or aid our understanding of the relationship between a disorder and frequently associated comorbidities within the same or different organ systems.1,2
Heart Rate, Blood Pressure, Skin Temperature
The most basic parameter for ANS assessment is heart rate (HR), which is controlled by both sympathetic and parasympathetic influences. Along with blood pressure and skin temperature, these parameters often indicate changes of ANS function and interaction between the antagonistic sympathetic and parasympathetic subsystems. For an in-depth analysis of ANS function and dysfunction, separate biomarkers of sympathetic or parasympathetic activity alone are usually of greater value than markers that are influenced by both subsystems. Among these are parameters derived by HRV and EDA.
Heart Rate Variability
HRV refers to the interbeat variations of HR signals. It was first described by Hon and Lee 3 in 1965 in fetuses, and since then several aspects of the interval and oscillations of intervals between heart beats have been described. At least 5-minute intervals/segments are used to measure and calculate markers for parasympathetic, possibly sympathetic or mixed activity. 4 HRV can be described by measures of time or frequency (see Table 1). 4 Examples of parameters in the time domain include the standard deviations of all normal-to-normal (NN) intervals (SDNN), the standard deviation of the averages of NN intervals in all 5-minute segments of the entire recording (SDANN), the square root of the mean of the sum of the squares of differences between adjacent NN intervals (RMSSD), the standard deviation of differences between adjacent NN intervals (SDSD), and the total number of all NN intervals divided by the height of the histogram of all NN intervals, measured on a discrete scale (HRV triangular index). Since the late 1960s, frequency domain methods have increasingly been used by applying spectral density analyses. Mainly, 3 spectral components (very low frequency [VLF, <0.04 Hz), low frequency [LF, 0.04-0.15 Hz], and high frequency [HF 0.15-0.4 Hz]) are calculated. 4 Frequencies in the high power range are mainly mediated by parasympathetic nerve fibers, 5 and can be inhibited by administering atropine. 6 These frequencies are also modulated by respirations leading to respiratory sinus arrhythmia (RSA), which also reflects parasympathetic activity and is calculated similarly to HF power.7,8 RSA and HF power are also often used to determine vagal tone (VT), which may also be assessed by determining the fast phase of the pupillary response that has been shown to correlate with RSA and other parameters of HRV 9 , but has not been described very frequently in research. LF and VLF power values cannot conclusively be attributed solely to either sympathetic or parasympathetic control. One should therefore carefully interpret these parameters and not prematurely conclude pure sympathetic influence, as LF, which has previously been discussed to reflect sympathetic activity, is also sensitive to vagal blockade (like RSA). 10 Determination of pure sympathetic activity may therefore be challenging by using HRV alone, whereas HF power of HRV provides a solid biomarker for the assessment of parasympathetic activity.
Overview of Selected HRV Parameters. a
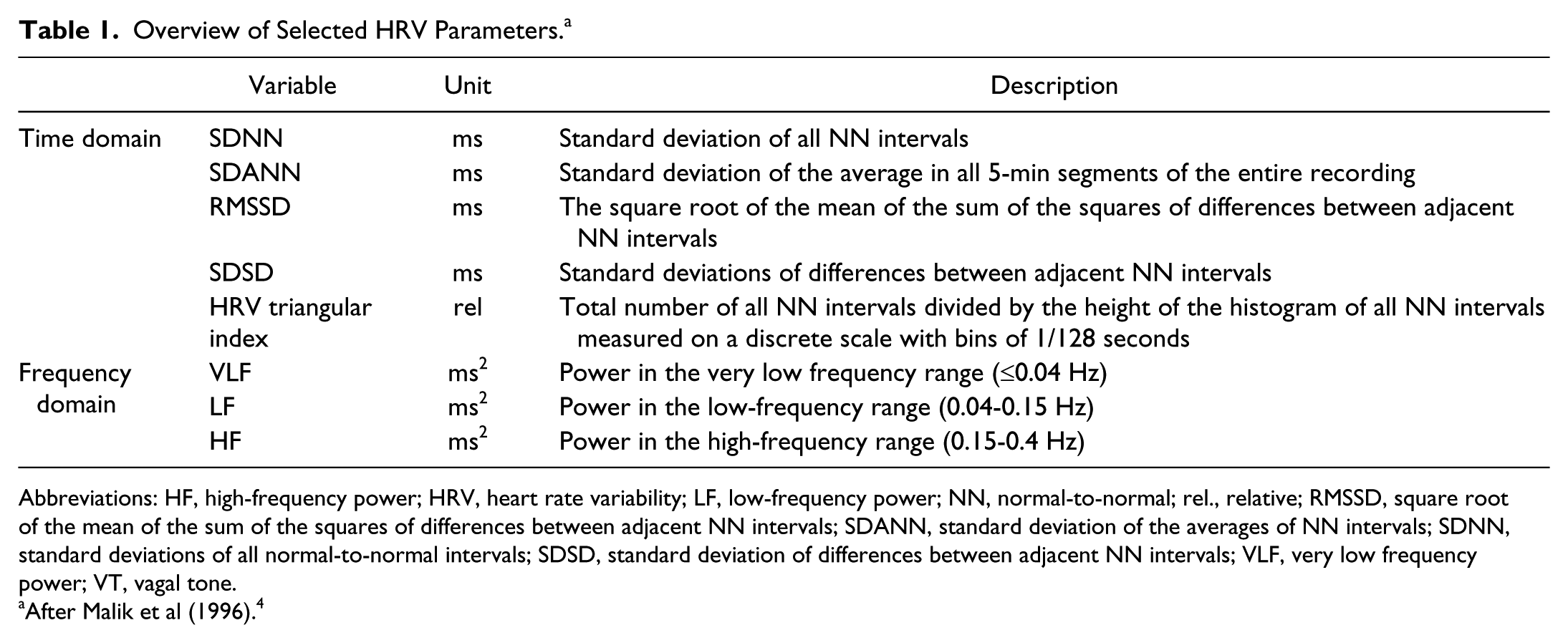
Abbreviations: HF, high-frequency power; HRV, heart rate variability; LF, low-frequency power; NN, normal-to-normal; rel., relative; RMSSD, square root of the mean of the sum of the squares of differences between adjacent NN intervals; SDANN, standard deviation of the averages of NN intervals; SDNN, standard deviations of all normal-to-normal intervals; SDSD, standard deviation of differences between adjacent NN intervals; VLF, very low frequency power; VT, vagal tone.
After Malik et al (1996). 4
Electrodermal Activity
Characterization of EDA allows for the focused exploration of sole sympathetic activity. Since the first description of EDA in the late 19th and early 20th centuries, 11 the underlying central and peripheral pathways of EDA have been well described. 12 Depending on the applied method, EDA can be described as skin conductance (in direct current mode, if voltage is kept constant) or skin resistance (in direct current mode, if current is kept constant). Without application of any current or voltage, endosomatic EDA may be measured as skin potential, which is no longer regularly performed because of the lack of standardization and baseline stability. Changes in either skin conductance or resistance depend on the hydration provided by sympathetically innervated eccrine sweat gland. 12 Because of the unique sympathetic transmitter system of eccrine glands, no direct parasympathetic antagonism is possible. 13 In preganglial sympathetic and parasympathetic synapses, acetylcholine is used, but postganglionic sympathetic activity is mediated through epinephrine/norepinephrine and parasympathetic activity through acetylcholine. Eccrine sweat glands as the cardinal mediators of EDA, however, use acetylcholine as a postganglionic sympathetic transmitter, which therefore prevents direct parasympathetic antagonism.13,14 For EDA, usually a baseline (tonic) activity with fluctuations and a stimulus induced (phasic) response can be described. It is important to consider that normalization of EDA data is crucial, given that tonic EDA baseline levels may vary considerably across individuals because of variability in constitution and skin composition. Sympathetic thermoregulation may also be mediated through eccrine sweat glands, which is usually present in temperatures >26°C. To keep this effect constant, it is recommended to keep temperatures under lab conditions stable and at <26°C. For psychophysiological use, technical requirements for measurements of EDA have been well standardized. 15 However, phasic EDA is often difficult to be compared across studies because of variable stimuli (eg, acoustic, painful, emotional).
Central Networks Involved in ANS Control
Recently, more data have been gathered to explore the central networks that are involved in ANS control. It has been hypothesized that the central activity of EDA originates in the left hemisphere, but this lateralization remains controversial. 16 Prefrontal networks (especially medially), however, have consistently been demonstrated to modulate sympatho-inhibitory impulses and inhibit sympathetic activity, potentially through amygdalar and related hypothalamic interaction.17,18 EDA, in particular, may be mediated through 2 different pathways: ipsilateral influences have been demonstrated within the limbic system via hypothalamus and thermoregulatory pathways and, to a lesser degree, contralateral modulation by the premotor cortex and basal ganglia. 12 Similarly, HRV (especially HF power) is mediated through the parabrachial nucleus, locus coeruleus, amygdala, hypothalamus, periaqueductal gray, posterior insula, and dorsolateral prefrontal cortex. 19 Many neuropsychiatric disorders affect these frontolimbic pathways and prefrontal networks, and an association with autonomic dysfunction is therefore not surprising. 20
ANS Dysfunction in Neuropsychiatric Disorders and PNES
It is commonly believed that the ANS plays an important role in many neuropsychiatric disorders. Porges proposed the involvement of ANS dysfunction in neuropsychiatric disease through a “polyvagal theory of social engagement.” 10 A “vagal break” may enhance restoration and growth in situations that do not pose a threat, but are disrupted in response to external demands. 10 It is, however, important to not only consider parasympathetic (vagal) efferent effects on effector organs but also acknowledge the diversity of neural pathways within the parasympathetic (and sympathetic) system, leading to organ specific subsystems with particular mechanisms of modulation and neural regulation. 21 Restricting the view to single neurophysiological ANS parameters may not mirror this complex interaction appropriately, yet helps understand and demystify parts of these interactions. In this context, it should also be considered that biomarkers in neuropsychiatric disorders, may indicate an actual state or a trait. As discussed in the “polyvagal theory,” this may account for some variability and potentially contradictory results in the literature.
Importantly, ANS abnormalities have been identified in PNES as well as in related psychiatric disorders frequently comorbid in PNES populations. To contextualize PNES-related ANS abnormalities, which will subsequently be discussed, the following section summarizes ANS abnormalities in PTSD, MDD, and disorders with prominent dissociation including borderline personality disorder (BPD).
Posttraumatic Stress Disorder
In PTSD, sympathetic activity is chronically increased above baseline.22,23 In fact, one of the hallmarks of PTSD is hyperarousal, which is due to autonomic dysregulation and can be found in several of the described electrophysiological ANS parameters. A higher baseline HR, elevated LF/HF-HRV Ratio and less HR differences and variability between day and night indicate chronically blunted parasympathetic activity in PTSD. 24 This is confirmed by the observation that in active duty combat marines lower HF HRV values correlated with a later PTSD diagnosis. 25 When compared with patients with past traumatic experiences without subsequent PTSD and with healthy controls, PTSD patients also exhibited decreased LF and HF HRV levels. 26 Given these findings, it may be suggested that hyperarousal in PTSD is associated with lower parasympathetic activity, as measured by a reduced level of HF power of HRV.
Similarly, studies using EDA as a sympathetic marker in PTSD revealed increased EDA, possibly linked to threat-induced hypervigilance. 27 At baseline, PTSD patients showed higher EDA and lower parasympathetic activity (as measured by low RSA), when compared with patients with panic disorder. 22 In a recent study, less habituation to periodic stimulation with prolonged excitation of the tonic EDA component was described in PTSD patients during experimentally induced fear states. 28 This response has been proposed to be lateralized (eg, left EDA increase in PTSD), 29 but these findings have not been consistently replicated. 30 Direct stimulation of the amygdala demonstrates ipsilateral EDA activation, challenging previous concepts of contralateral EDA responses. 31 While the electrodermal response per se may physiologically be lateralized, the laterality of pathological EDA in PTSD requires further investigation.
In conclusion, PTSD is associated with dysautonomia, specifically increased sympathetic and decreased parasympathetic activity. This hyperarousability may be indicative of functional and structural alterations in brain networks mediating ANS control.32,33
Major Depressive Disorder
Autonomic dysfunction in MDD is less consistent than in PTSD. Two large meta-analyses found HF-HRV decreased (and therefore reduced parasympathetic activity) in patients with MDD.34,35 These results have recently been confirmed by 2 further studies36,37; however, no correlation was observed between HRV parameters and depression in the aforementioned cohort of active duty marines. 25 Results on VLF-HRV are even more mixed, potentially in part because VLF most likely resembles mixed sympathetic and parasympathetic activity. Baseline resting VLF power has, however, been reported as a possible marker for successful treatment response in MDD, as a lower baseline VLF was shown to predict a reduction in depressive symptom severity after treatment with escitalopram. 38 In a series of 53 MDD patients, LF was higher in the MDD group compared with healthy subjects. 36 Significant changes were also found in several HRV parameters of the time domain, such as SDNN, SDANN, and RMSSD. Also, a linear relationship between depression severity index and the LH/HF-index as well as SDNN indicate a higher amount of dysautonomia. 36 The described (mixed) parameters and findings to date do not allow definitive conclusions to be drawn about the directionality of sympathetic or parasympathetic subsystems.
EDA phenomena have also been extensively studied in MDD. In general, most of the studies found EDA hypoactivity and hyporeactivity as a common feature in MDD. 12 Low EDA after a neutral tone was associated with depression, and low EDA may suggest a higher risk of relapse (particularly if EDA baseline levels are not reached after initial recovery). 39 Similarly, EDA was found to be low in depressive patients with symptoms of psychomotor inhibition like slowness of movements, concentration difficulties, inability to feel, and lassitude,40,41 but no EDA differences were found between suicidal or nonsuicidal depressed patients. 42 In an EDA habituation experiment using acoustic stimuli, however, Wolfersdorf and Straub 43 found that violent suicidality with impulsivity in MDD was associated with faster habituation. Similarly, LF power of systolic blood pressure variability (LFSBP), which is equal to LF-HRV resembling sympathetic activity, was found to be blunted in a female depression cohort after a 3-minute cold pressure test. 44 At baseline, EDA (measured as skin conductance levels) was found to be significantly lower in 31 patients with MDD, when compared with 71 healthy controls, 45 but LFSBP was reportedly high in depressed females. 44 Lateralization of EDA abnormalities in depression have also been reported,30,46 but this feature requires further investigation.
In summary, studies examining ANS dysfunction in MDD indicate that depression is associated with lower sympathetic activity and sympathetic reactivity, as most consistently suggested through studies using EDA measurements.
Dissociation and Borderline Personality Disorder
Neurobiological models of dissociation have been discussed since Geschwind’s concept of disconnection of neurolimbic networks, emphasizing the role of the amygdala and its connections with the medial prefrontal cortex, including the anterior cingulate cortex. 47 More recently, dissociative states have been explained by neural disintegration that may reflect various independent processes by means of neural complexity. 48 Failure of neural integration has been linked to EDA complexity, which was measured by a pointwise correlation dimension algorithm, calculated by a short time average over the whole signal for each point compared with the distance reflecting radius of the neighborhood of that point. Increased baseline EDA complexity and neural disintegration is reportedly associated with vulnerability in stressful events and subsequent dissociative states of consciousness. 48
These hypotheses may be confirmed by ANS biomarkers: A greater tendency to dissociate has been found to correlate with decreased frequency domain parameters of HRV during an orthostatic challenge in patients with panic disorder 49 or bipolar disorder. 50 Similarly, reduction of parasympathetically mediated HRV has been described in patients with dissociative identity disorder when confronted with trauma-related memories. 51
EDA has also been used for some time to describe dissociative states. First reports, dating back to 1907 and 1908, demonstrated EDA changes in patients with dissociation.52,53 Since then, many studies confirmed that patients with dissociation, or dissociative tendencies, exhibit different EDA responses compared to healthy controls.29,49,50,54 In particular, low baseline EDA, habituation and lack of fluctuation after an unspecific stimulus, were observed to be prominent features in dissociation. In a larger study of 85 female rape victims with peritraumatic dissociation, Griffin et al 55 found that a more suppressed skin conductance (lower EDA) response, during description of the trauma, was associated with a higher level of dissociation on the peritraumatic dissociation index 2 weeks following the trauma.
ANS responses have also been altered in patients with BPD, a cohort with prominent dissociative symptoms. BPD patients demonstrated increased sympathetic and decreased parasympathetic (RSA) activity during a social stressor task, when compared with healthy controls, indicating a pattern consistent with hyperarousability. 56 These findings were replicated using EDA: Higher EDA (measured as skin conductance response) was discovered in patients with BPD. 57 In contrast, HF-HRV at baseline (measured over 24 hours) was found to be higher in patients with BPD. 58 Though surprising, one way of interpreting this observation is to consider sympathetic and parasympathetic upregulation in patients with BPD, although sympathetic activity was not uniquely examined in this particular study. 58 Other studies did not find significantly altered HRV responses in BPD, and challenged the concept of affective hyperresponsiveness in the disorder. 59 While future research will help clarify the degree and nature of ANS dysfunction in BPD, it is noteworthy that medial prefrontal cortex hypoactivation, and increased amygdalar activation, were observed in a cohort of women with BPD compared with healthy subjects, using a functional magnetic resonance imaging task probing negative emotional processing in the context of behavioral constraint. 60 These neural activation patterns provide further support for a model of ANS hyperarousability and decreased regulation in BPD.
In conclusion, despite methodological differences among various studies and intermittent oversimplification of autonomic function in the context of disregarding organ specific neuronal organization with organ specific neural pathways within the sympathetic and parasympathetic system, emerging patterns of dysautonomia are increasingly recognized in neuropsychiatric disorders using HRV and EDA. While PTSD, and possibly BPD, seem to be associated with increased sympathetic and potentially decreased parasympathetic activity, patients with MDD, or dissociation, appear to exhibit a lower sympathetic baseline tone and response.
ANS Changes in Patients With PNES
Psychopathology and psychiatric comorbidities of PNES are heterogeneous, and include PTSD, MDD, and dissociative disorders among other conditions. It is therefore not surprising that ANS biomarkers in PNES may not resemble a uniform and “classic” ANS response, but may instead follow dysautonomic features related to psychiatric comorbidities and PNES-specific pathophysiology.
Heart rate, as a basic marker for ANS activity, was shown to be elevated ictally and postictally in temporal lobe epileptic seizures (ES), but not in PNES. 61 Data from our group, however, did not support this observation. We not only observed ictal tachycardia in both ES and PNES, but also found increased heart rates prior to the onset of PNES (and not ES). In addition, postictal HR values were significantly lower in PNES than in ES, indicating faster autonomic recovery. 62 A faster return to baseline in PNES versus ES, after ictal tachycardia, was also reported previously. 63 In the study by Oliveira et al, 63 event tachycardia was also found to be related to (psychogenic) seizure severity measured by the degree of ictal motor activity. Recently, ictal tachycardia has been proposed as a mechanism for seizure detection, especially since approximately 82% of patients with epilepsy are associated with significant increases of heart rate. 64 This mechanism is currently investigated as a stimulus for vagal nerve stimulation during a seizure (NCT01325623). However, considerable intraindividual variability of ictal heart rate changes, and the high likelihood of ictal tachycardia, in PNES 62 have to be considered, when this parameter is used to distinguish between ES and PNES.
Various HRV metrics have been examined during, and between, events in PNES. Interictal changes were reported between patients with either PNES or ES compared with healthy controls, but not when PNES were compared with ES. 65 Specifically, RMSSD, HF power, and the cardiovagal index (a graphical index in which each RR interval is plotted against the subsequent RR interval) were found to be low in PNES, when compared to normal controls, indicating a lower VT. RMSSD in PNES patients was also found to be significantly reduced at baseline, and after recovery, from a social stress induction in comparison with normal controls. 66 No difference between groups was found during the stress induction portion of the study, indicating that much of the underlying pathology in PNES is explained by sustained baseline vulnerabilities rather than discrete alterations during stressful stimulations. The cardiosympathetic index (similar to cardiovagal index) has reportedly been lower during PNES events. LF and HF power, as well as RMSSD were higher in PNES in comparison with ES, 67 indicating greater sympathetic system activation during ES and greater parasympathetic activation during PNES. In light of the aforementioned polyvagal theory, low VT and RMSSD, as a parameter of the parasympathetic activity, are interpreted as a physiological marker of stress vulnerability. Low VT could indicate a lower functioning “vagal break.” The “vagal break” is hypothesized to “enhance restoration in phases without challenges for the organism, but disruption occurs when sympathetic tone increases to install readiness to deal with external demands.” 10 The polyvagal theory, and the concept of a vagal break, also support the notion of the parasympathetic system as a “buffer” that allows individuals to react to external stimuli. This vagal break may be altered in PNES and other neuropsychiatric disorders. 65
EDA in PNES: A Pilot Study
To date, there are no published studies on EDA data in PNES. EDA during, and after, generalized tonic-clonic seizures (GTCS) is known to be markedly elevated, indicating prolonged excessive sympathetic activation.68,69 We explored ictal and interictal EDA differences between GTCS and PNES in patients admitted to the EMU of the Edward B. Bromfield Epilepsy Service at Brigham and Women’s Hospital.
Methods
After obtaining internal review board approval, 126 consecutive patients gave consent and were enrolled prospectively. Patients wore wireless sensors that measure EDA, skin temperature, and 3-dimensional accelerometry continuously on the distal forearm during most days of admissions (Q Sensor, Affectiva Inc, Waltham, MA, USA). Details and technical specifications of the sensors can be found in Poh et al. 70 Eleven patients had a PNES event captured on EEG (to confirm the diagnosis in addition to clinical history and witness reports) while wearing EDA sensors. Nine patients with EEG-captured GTCS were used as a control group. One hundred and six patients had neither GTCS nor PNES, or were not wearing a sensor at the time of the seizure. EDA recordings were lowpass linear-phase FIR digital filtered (cut-off frequency: 0.4 Hz, Filter order: 32). Continuous EDA of ictal and nonictal days was analyzed separately and compared. An ictal period was defined as a 24-hour interval with either a PNES or GTCS event. An interictal period is a 24-hour period without a PNES, GTCS or any other seizure type. We then used an automated algorithm to calculate the area under the EDA curve over a 24-hour period (AUC) for each day, the total number of EDA responses (EDR) lasting longer than 2 seconds with a significant change from baseline (first derivative of filtered EDA signal) of >0.02 μS/s, and the duration of EDR. In addition, we also determined surges of EDA during sleep (“sympathetic sleep storms”) as defined by Sano and Picard 71 (≥3 EDR within 30 seconds and absence of motion in actigraphy). If storm epochs were adjacent or within five minutes of each other, they were combined into one single “storm.” Figure 1 presents 2 actual and 1 pseudo-sympathetic sleep storm, indicated by light red, on the first derivative of the EDA signal (Figure 1B). A pseudo-storm was defined as an event that satisfied all the criteria to be a sympathetic storm, but did not occur during sleep (motion algorithm detected motion activity in actigraphy data—see Figure 1D for the first storm). Differences between EDA variables of PNES and GTCS were assessed by performing a Wilcoxon rank sum test.
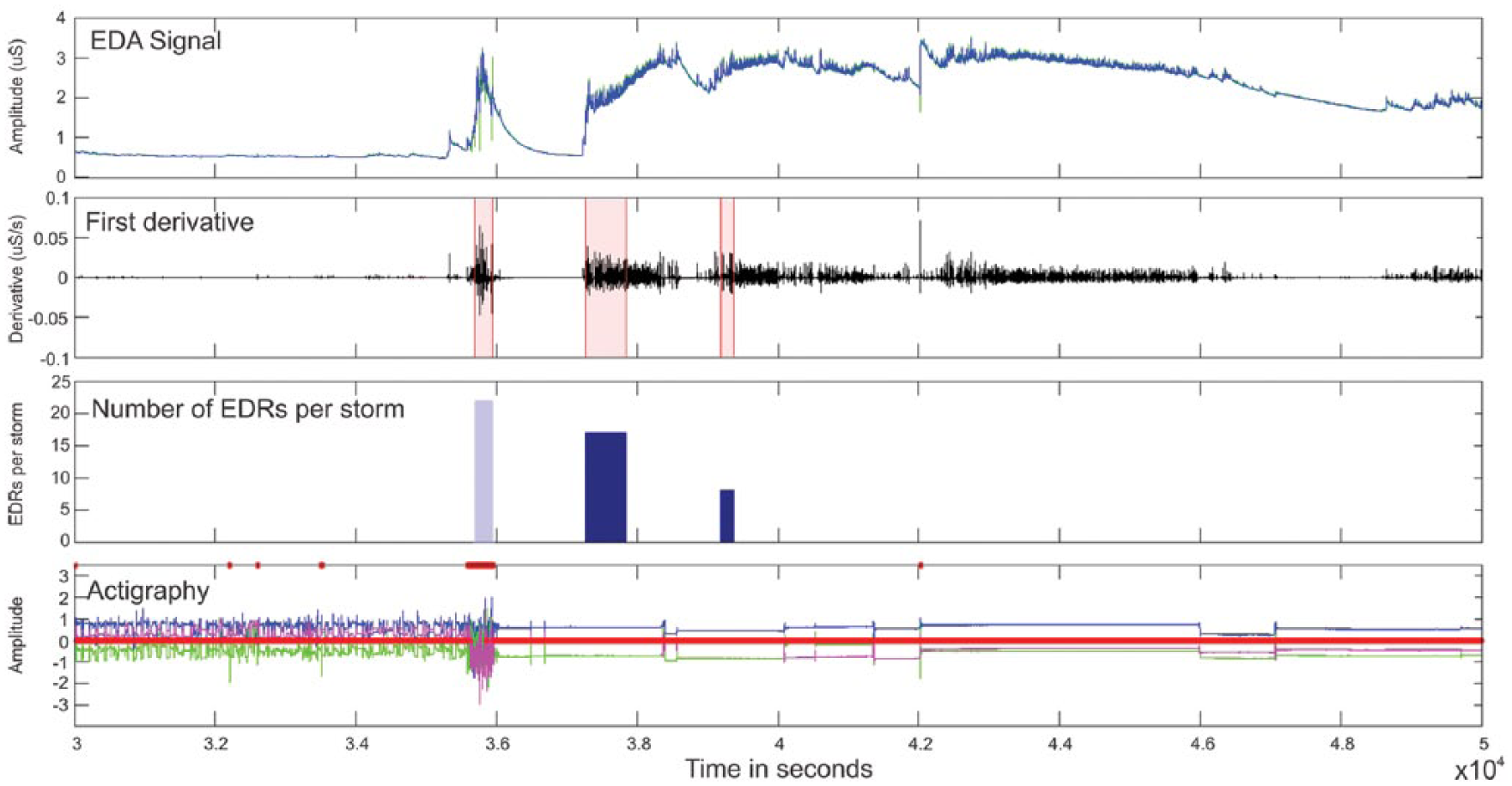
EDA variables and actigraphy data. (a) EDA signal (in μS) (green: unfiltered, filtered (low-band filter 0.4 Hz, 32nd order FIR filter) from one of our epilepsy patients (duration: 333.33 min). (b) First derivate of filtered EDA signal (in μS/s). Light red indicates the time where a storm was identified. (c) Number of EDRs per storm (dark blue: actual storms, light blue: storm excluded from analysis due to motion detection. (d) Actigraphy data for the three accelerometers (blue: x-axis, green: y-axis, magenda: z-axis). Motion detection algorithm indicates motion on red (no motion: zero; motion: max value).
Results
Clinical data of PNES and GTCS patients are presented in Table 2. Among the 11 PNES patients, 5 were MDD, 1 PTSD, 1 generalized anxiety disorder (GAD), 1 both PTSD and GAD, and 3 did not meet criteria for a neuropsychiatric disorder based on clinical psychiatric interviews. Interictally, no differences were found in the EDA measures between the 2 patient populations (Table 3). On event days, the longest EDR was found to be significantly greater in the GTCS group in comparison to the PNES group (P = .0074). No further significant differences were found, but values of several indices were highly variable within both groups. Some patients with PNES had EDRs that were higher than ictal GTCS values, but overall an expected amount of interindividual variability was found in all EDA parameters. 12 The limited number of complete data sets and the inclusion of patients with subjective symptoms (yet highly indicative of PNES based on clinical history and EEG findings) precludes a more detailed and systematic statistical analysis comparing ictal and interictal values. However, all GTCS patients, for whom complete data sets were available, had an (mostly excessive) increase of the AUC of EDA on ictal days as compared with interictal values (patients 1, 2, 4, 5, and 7). In contrast, PNES patients either had mild increases (PNES patients 1 and 5) or decreases (patients 2 and 11), when AUC values are compared on ictal and interictal days. Interestingly, the patient with the largest increase (patient 1) presented with a major motor PNES semiology, while 1 patient with very mild increase (patient 5) and 2 patients with ictal AUC decrease presented with nonmotor or subjective PNES symptoms. Similarly, the number of EDRs increased in all but one GTCS patient from interictal to ictal days, but only in 1 of 3 PNES patients (and in that 1 case only from 0 to 1).
Clinical Characteristics of the Cohort of 11 PNES Patients and 9 Epilepsy Patients.
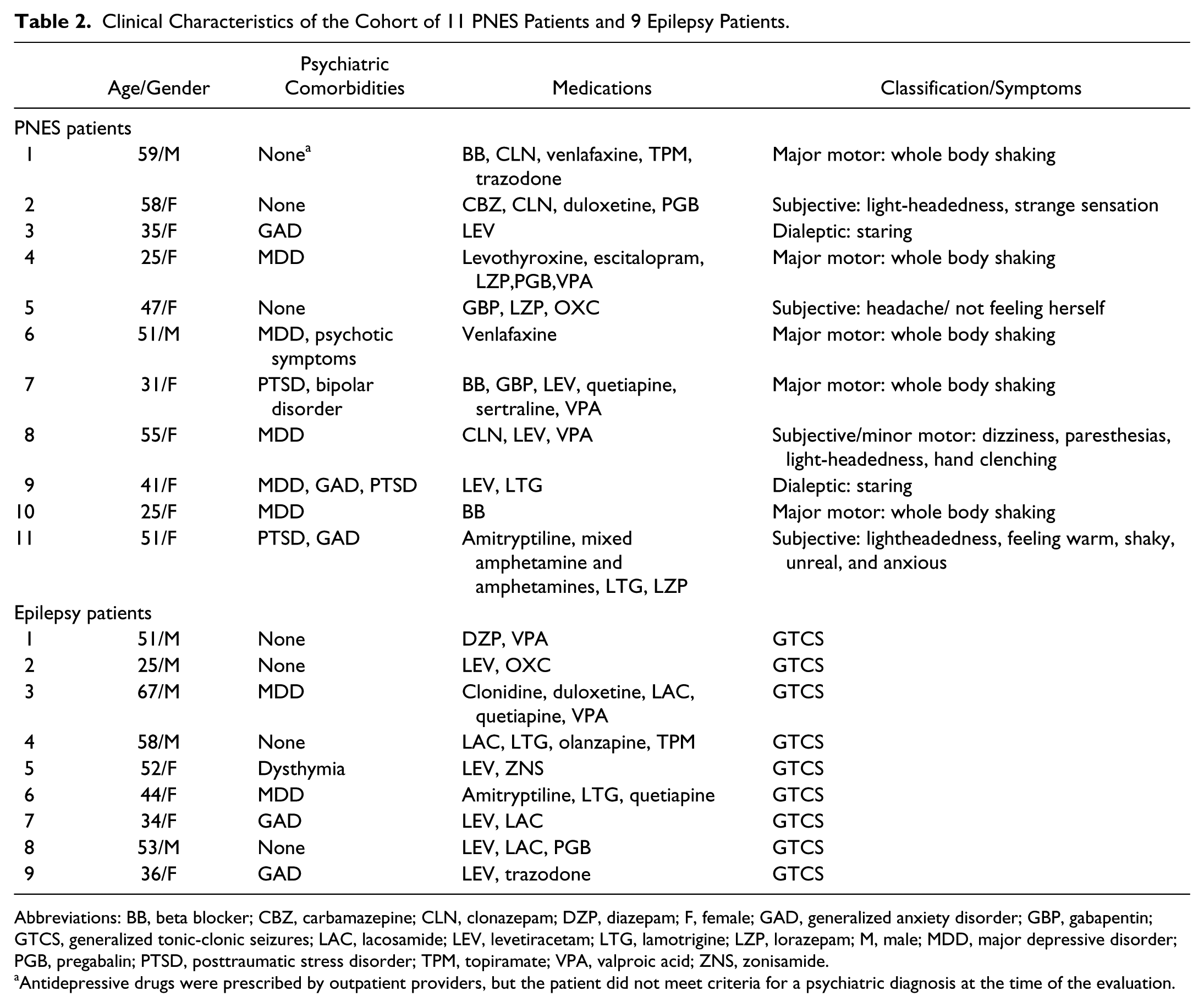
Abbreviations: BB, beta blocker; CBZ, carbamazepine; CLN, clonazepam; DZP, diazepam; F, female; GAD, generalized anxiety disorder; GBP, gabapentin; GTCS, generalized tonic-clonic seizures; LAC, lacosamide; LEV, levetiracetam; LTG, lamotrigine; LZP, lorazepam; M, male; MDD, major depressive disorder; PGB, pregabalin; PTSD, posttraumatic stress disorder; TPM, topiramate; VPA, valproic acid; ZNS, zonisamide.
Antidepressive drugs were prescribed by outpatient providers, but the patient did not meet criteria for a psychiatric diagnosis at the time of the evaluation.
EDA Variables in 11 PNES Patients and 9 Epilepsy Patients With Documented GTCS.
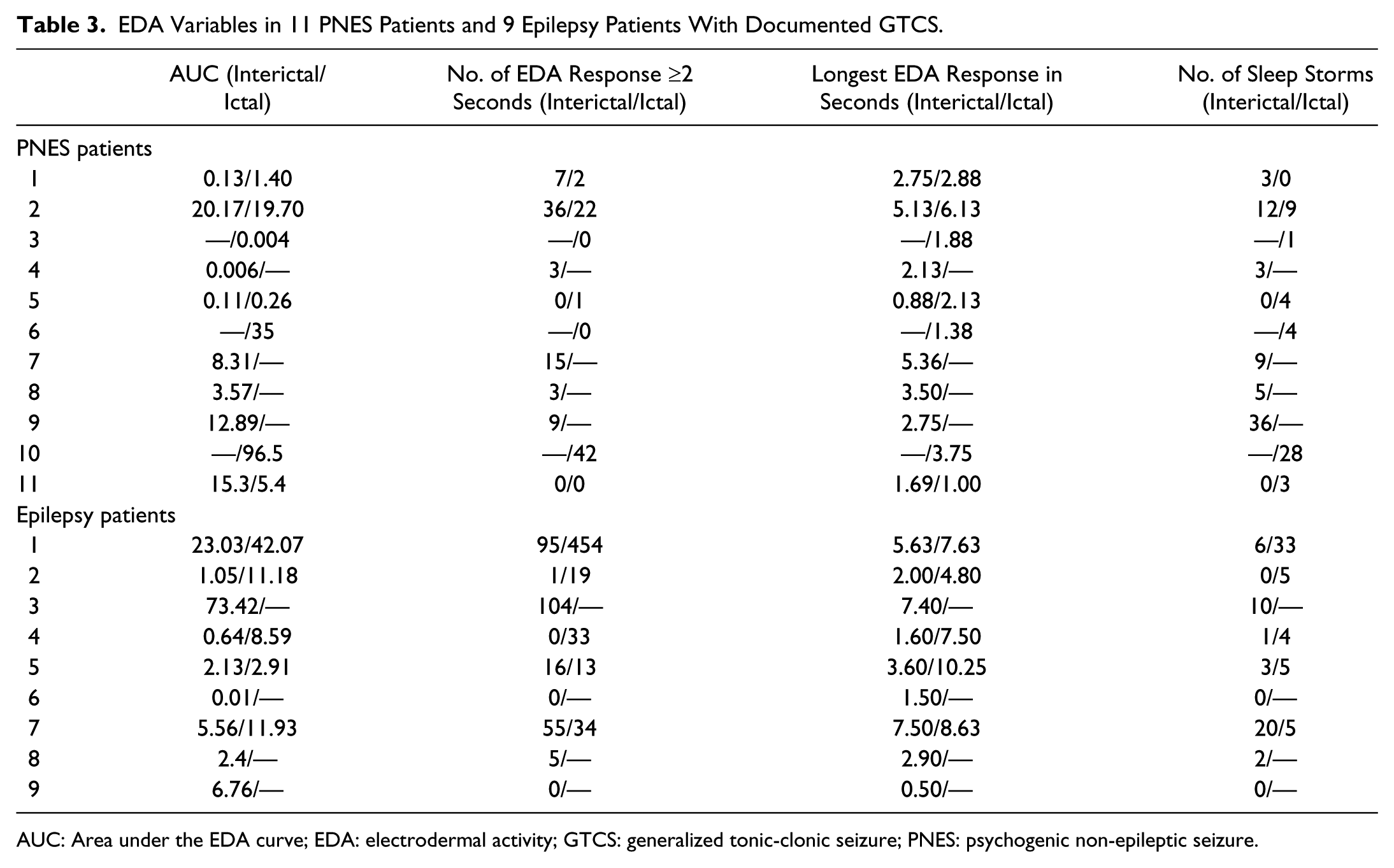
AUC: Area under the EDA curve; EDA: electrodermal activity; GTCS: generalized tonic-clonic seizure; PNES: psychogenic non-epileptic seizure.
Conclusion
The increase in the number of EDRs, the duration of the longest EDR and the AUC of EDA on ictal days supported the hypothesis that GTCS are associated with a more profound sympathetic arousal than PNES. In contrast to the previously reported EDA responses following GTCS, 69 PNES are associated with less intense EDA response and often lack the typical large peak that is seen after GTCS, which may be utilized as a tool to differentiate between the 2 seizure types. Whether and how ictal autonomic parameters of PNES are different from baseline states in these patients will be evaluated in future studies, which should include more subjects and more complete datasets. Similarly, our dataset did not allow interpretation of EDA with respect to the underlying psychopathology or neuropsychiatric syndrome, because of our limited sample size. For instance, an ictal increase of AUC of EDA was found in 2 patients without evidence of a neuropsychiatric disorder at the time of presentation, a remarkable decrease on ictal days was found in a patient with comorbid PTSD, and a slight decrease in a patient without a neuropsychiatric disorder. Inclusion of further patients will allow for the investigation of PNES subtypes with potentially distinct ANS peri-ictal patterns, as well as elucidate the association between psychiatric comorbidities and ANS patterns in PNES. It may also help clarify the influence of antidepressant medications on the ANS, specifically EDA. Trazodone, which may be associated with orthostatic hypotonia and arrhythmias, and amitriptyline, which has anticholinergic properties, may well influence EDA responses both ictally and interictally.
The appearance and number of sleep storms in neurological and neuropsychiatric disorders is still poorly understood. Four of 5 patients in our study had an increase of sympathetic sleep storms during the night after a GTCS. Similarly 1 patient with PTSD, and 1 without neuropsychiatric disorder, showed this phenomenon the night after a PNES, while 2 without neuropsychiatric disorders had a decrease in storms. These data seem to support a prolonged sympathetic arousal after a GTCS, but the relationship between sleep storms and PNES remains to be elucidated.
Overall, EDA changes in PNES patients did not follow a systematic sympathetic hyperarousal pattern like EDA after GTCS, but rather exhibited variable patterns. Specific PNES semiologies, and/or underlying neuropsychiatric disorders, may influence the ictal and interictal EDA pattern, and will be further evaluated by assessing these ANS values in larger samples. The small sample size in each group, and the high number of incomplete data sets, are notable limitations of this pilot study, which should be addressed in future research. It will also be useful to include a complex partial seizure control group, as the differentiation between CPS and PNES may often be clinically challenging. Our pilot data did not allow inclusion of a CPS group because of the low number of captured seizures.
Summary
Changes in ANS physiology are commonly associated with neuropsychiatric conditions. As the methods and biosensors become more widely available, central changes in ANS in neuropsychiatric disorders, including PNES, will be further clarified (see Table 4 for an overview). Improved understanding of ANS disturbances in PNES will significantly contribute toward further classification of the pathophysiological mechanism behind this functional neurological symptom disorder. Future research on ANS variables in PNES may offer a potential diagnostic biomarker, and further contribute to the classification of PNES into subgroups, which may help development of more specific diagnostic tests and treatments.
Overview of ANS Patterns in Select Neuropsychiatric Disorders and PNES.
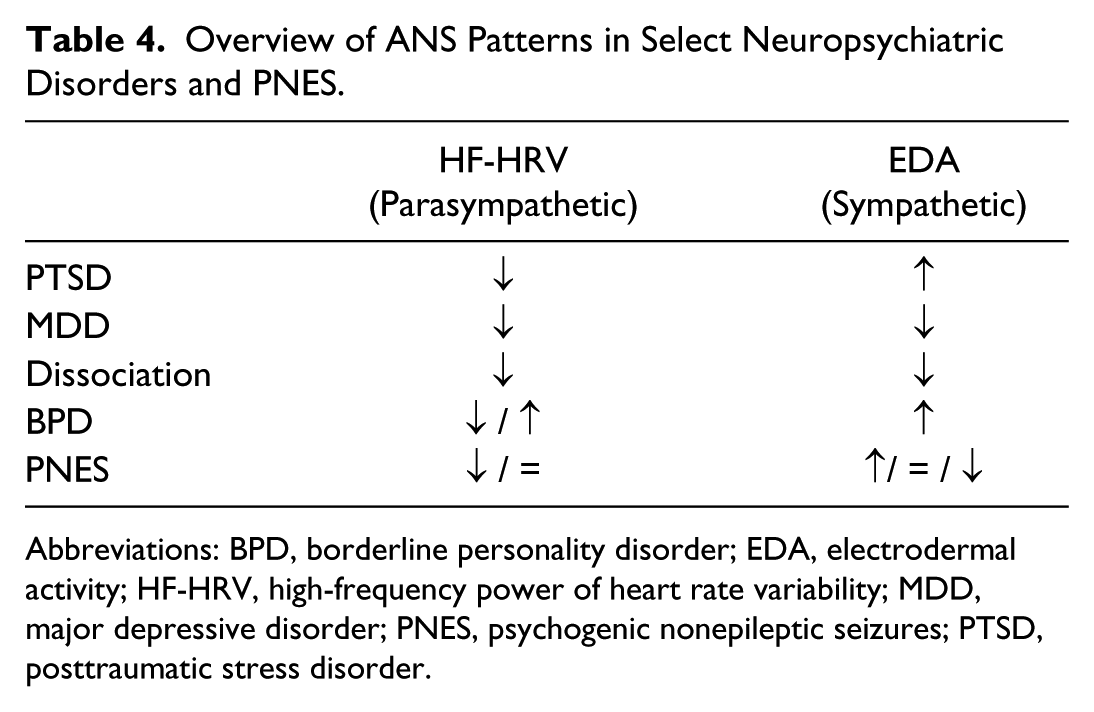
Abbreviations: BPD, borderline personality disorder; EDA, electrodermal activity; HF-HRV, high-frequency power of heart rate variability; MDD, major depressive disorder; PNES, psychogenic nonepileptic seizures; PTSD, posttraumatic stress disorder.
Footnotes
Acknowledgements
Biosensors used in this study were donated by Affectiva Inc.
Author Contributions
CR, DLP, GB and BAD performed the literature research and wrote the manuscript. CR, RS, TL and BAD performed the study on EDA signals. CP and CD performed the computational analysis of EDA signals. RS performed the statistical analysis on EDA signals. All authors participated in editing the manuscript.
Declaration of Conflicting Interests
The author(s) declared the following conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Reinsberger has received grants from the Epilepsy Foundation (EF#179308, not relevant to this article) and receives compensation for clinical consulting for SleepMed Inc (not relevant to this article). Dr Reinsberger also received grants from the Epilepsy Foundation (EF#213882, relevant to this article). Dr Sarkis received travel funding for an investigators meeting from Sunovion (not relevant to this article). Dr Papdelis and Mr Doshi have no disclosures. Dr Perez was funded by a NINDS R25NS065743-05S1 grant (not relevant to this article). Dr Baslet has no disclosures. Dr Loddenkemper serves on the Laboratory Accreditation Board for Long Term (Epilepsy and Intensive Care Unit) Monitoring, on the Council of the American Clinical Neurophysiology Society, on the American Board of Clinical Neurophysiology, as an Associate Editor for Seizure, and performs video electroencephalogram long-term monitoring, electroencephalograms, and other electrophysiological studies at Boston Children’s Hospital and bills for these procedures and evaluates pediatric neurology patients and bills for clinical care. He is part of a pending patent application to detect seizures. He receives research support from the American Epilepsy Society, the Epilepsy Foundation of America, the Center for Integration of Medicine and Innovative Technology, the Epilepsy Therapy Project, the Pediatric Epilepsy Research Foundation, Cure, Danny-Did Foundation, HHV-6 Foundation, and from investigator-initiated research grants from Lundbeck and Eisai. His wife, Karen Stannard, MD, is a practicing pediatric neurologist who evaluates pediatric neurology patients and bills for clinical care. Dr Dworetzky receives compensation for clinical consulting for SleepMed Inc and for Best Doctors (not relevant to this article).