
Abstract
Background. Few studies have investigated the impact of the psychopathic traits on the EEG of teenagers with conduct disorder (CD). To date, there is no other research studying low-resolution brain electromagnetic tomography (LORETA) technique using quantitative EEG (QEEG) analysis in adolescents with CD and psychopathic traits. Objective. To find electrophysiological differences specifically related to the psychopathic traits. The current investigation compares the QEEG and the current source density measures between adolescents with CD and psychopathic traits and adolescents with CD without psychopathic traits. Methods. The resting EEG activity and LORETA for the EEG fast spectral bands were evaluated in 42 teenagers with CD, 25 with and 17 without psychopathic traits according to the Antisocial Process Screening Device. All adolescents were assessed using the DSM-IV-TR criteria. The EEG visual inspection characteristics and the use of frequency domain quantitative analysis techniques (narrow band spectral parameters) are described. Results. QEEG analysis showed a pattern of beta activity excess on the bilateral frontal-temporal regions and decreases of alpha band power on the left central-temporal and right frontal-central-temporal regions in the psychopathic traits group. Current source density calculated at 17.18 Hz showed an increase within fronto-temporo-striatal regions in the psychopathic relative to the nonpsychopathic traits group. Conclusions. These findings indicate that QEEG analysis and techniques of source localization may reveal differences in brain electrical activity among teenagers with CD and psychopathic traits, which was not obvious to visual inspection. Taken together, these results suggest that abnormalities in a fronto-temporo-striatal network play a relevant role in the neurobiological basis of psychopathic behavior.
Introduction
Conduct disorder (CD) is one of the psychiatric illness frequently assessed by child mental services. 1 CD is a diagnosis typically assigned to individuals younger than 18 years, who habitually violate the rights of others, and whose behavior does not conform to the law or social norms appropriate for their age. 2 The annual prevalence of CD is 2% to 10%. It is more frequently diagnosed in boys, at least in part due to boys’ tendencies to act out violently. 2
One form of CD is marked by the presence of psychopathic traits. These traits have a core callous-unemotional component and an impulsive-antisocial component. 2 These components are related to 2 essential cognitive impairments. The first is associated with reductions in specific forms of emotional empathy. This functional alteration is associated with reduced amygdala and ventromedial prefrontal cortex responsiveness to distress cues. The second cognitive impairment is related to aspects of decision making, specifically in reinforcement learning and the representation of reinforcement expectancies. This impairment may relate more to the impulsive-antisocial component of psychopathic traits. 3
Boys with callous-unemotional conduct problems present impairments on neuropsychological tasks tapping the functionality of the ventrolateral/orbitofrontal cortex and the amygdala functioning. 4 Consistent with this finding, researchers using functional magnetic resonance imaging (fMRI) techniques have identified limbic-prefrontal circuit abnormalities in children and adolescents with high psychopathic traits5-7 and reduced activity within regions associated with empathic pain, including rostral anterior cingulate cortex, ventral striatum (putamen), and amygdala. 8 In the past decade, several studies using MRI have described brain structural differences in boys with CD. They found
reduced volumes in the temporal lobe,9,10 insula, 11 amygdala,10,11 hippocampus, orbitofrontal cortex, ventromedial prefrontal cortex, 10 right middle frontal cortex, and left parietal lobule 12
increased brain tissue volumes in the left putamen, left ansa peduncularis, right superiomedial prefrontal cortex, left inferior frontal cortex, and right medial temporal, right orbitofrontal cortex regions 12
increased gray matter and decreased white matter concentrations in the right superior frontal lobe (subgyral), right dorsal anterior cingulate (limbic lobe), right superior temporal gyrus and left precuneus13,14
decreased overall mean cortical thickness associate with thinning of the cingulate, prefrontal, and insular cortices in children with disruptive behavior disorders. 15
Two recent voxel-based morphometry studies reported paralimbic gray matter reductions in incarcerated male adolescent with psychopathic traits.16,17
Few studies have investigated the impact of the psychopathic traits on the EEG of teenagers with CD. The construct of psychopathy as a clinical syndrome has been applied as a discriminating variable in the identification and classification of children who will develop chronic offending careers.18-21 Nevertheless, there is considerable controversy regarding the assessment and diagnosis of psychopathy in juveniles. Some have argued that the early identification of psychopathic traits might allow clinicians to intervene sooner and more effectively with youths who presumably are at high risk to continue antisocial behavior into adulthood. 22
Abnormal EEG activity had been described in delinquent and antisocial adolescents. 23 Earlier studies generally based on qualitative analysis reported a high amount of slow EEG activity in children with CD 24 and paroxysmal abnormalities in repeatedly violent delinquent boys. 25 Alpha slowing among children and adolescents had been associated with later delinquency26,27 while the beta activity with externalizing spectrum disorders,28,29 such as conduct disorder and antisocial behavior. A number of studies have reported increase of beta activity and decrease of alpha power in adult psychopaths, 30 in impulsive subjects, 31 and in subjects with psychiatric disorders considered important precursors of psychopathy as moderate intermittent explosive disorder (mIED), 32 and attention deficit/hyperactivity disorder (ADHD).33-35
EEG provides an excellent index of brain activation level, particularly in cortical regions. 18 Quantitative EEG (QEEG) analysis moved away from the traditional analysis of graphoelements at certain electrodes to a comprehensive analysis of the brain’s electric field at the scalp. A deeper understanding of cortical coupling is possible by studying the correlations between current sources derived from the surface EEG using an inverse method. 36 Recent advances in EEG recording technology and EEG analysis methods make the window into the brain much more transparent, and the signal source relationship has become clearer. 37
Data from electrophysiology will be used to clarify the neurobiological basis of children with presumable psychopathy and their risk of being violent offenders later during their adult lives. In a previous study of EEG in psychopathic offenders, 30 we described a certain pattern of EEG abnormalities when compared with nonpsychopathic offenders used as controls. The aim of this study was to investigate whether EEG differences can be found between adolescents with CD with comorbid psychopathy and CD adolescents without this comorbidity and to quantify the nature of these differences. It is hypothesized that adolescents with psychopathic traits will have increased beta activity with reduced levels of alpha compared with nonpsychopathic traits adolescents. We also examined whether the QEEG abnormalities are associated differentially with traits of psychopathy assessed by the Antisocial Process Screening Device (APSD) scale.
Materials and Methods
Subjects
The study included 42 male CD teenagers, mean age was 15.7 years (SD = 1.02) from a special conduct disorder school located in Havana City. Assessment was conducted during a 2-year period, from January 2010 to December 2011.
Clinical assessment was performed by childhood psychiatrists directly related to this study. All they were well trained in the application of all structured, semistructured interviews, and diagnostic tools used. Diagnostic interviews were carried out separately with participants and caregivers. Clinical interviews incorporated information from as many sources as were available. These included a history given by a parent or guardian, school reports, data from any other health professionals and behavioral observations during the assessment. This study used DSM-IV-TR 38 criteria for the diagnosis of CD and APSD in order to evaluate psychopathic traits. 39 Twenty-five adolescents were diagnosed with CD and psychopathic traits (mean age 15.66 years, SD = 1.21). The control group consisted of 17 adolescents from the same school diagnosed with CD without psychopathic traits (mean age 15.79 years, SD = 0.82).
In order to be included in the CD with comorbid psychopathic traits group, adolescents were required to meet the full diagnostic criteria for psychopathic disorder according to APSD scale created by Frick and Hare. 39 This scale is an extension of the Psychopathy Checklist-Revised (PCL-R) for adults. 40 The APSD is a 20-item behavior rating scale typically completed by a parent and/or teacher. This instrument does not specify a particular amount of time necessary for the rater to have known the child. The APSD was designed to assess a lack of empathy and callous behavior toward others, which may reflect a distinct subtype of those with more severe externalizing behavior problems and poorer developmental outcomes. Factor analysis of the APSD uncovered 3 dimensions: Narcissism, Impulsivity, and Callous-Unemotional (CU). The CU dimension includes items such as “concerned about the feelings of others” and “does not show emotions.” 41
Sociobiographical, criminological, medical, and psychopathological information was recorded on a standardized score sheet and entered into a computer system for further processing.
Exclusion criteria in this study were presence of any current or previous history of neurological disease that can influence results of EEG records, as the presence of an abnormal prenatal, perinatal or neonatal event, a disorder of consciousness, a head injury resulting in cognitive deficits, antecedents of central nervous system (CNS) diseases, convulsions, psychiatric abnormalities (other than CD, ADHD, or Oppositional Defiant Disorder) or substance abuse disorders. None of the adolescents was taking any medication at the time of testing. Participation in the study was voluntary, written informed consent was obtained from all parents. The study was approved by the Ethics Committee of the Cuban Center for Neurosciences.
EEG Procedure
EEG was recorded using a 21-channel digital EEG hardware and software package from Neuronic SA (MEDICID IV, Cuba). Electrodes were placed in 19-electrodes sites (Fp1, Fp2, Fz, F3, F4, F7, F8, Cz, C3, C4, T3, T4, T5, T6, Pz, P3, P4, O1, and O2) according to the international 10-20 system, using surface electrodes referenced to linked earlobes with a ground electrode attached to the forehead. Impedance for all electrodes was kept ≤5 kohm during the entire record. EEG was amplified by 10 600, with a bandpass at 0.5 to 30 Hz and sampled through a 12-bit analog-to-digital converter at 200 Hz.
Electrodes were fitted while subjects were familiarizing with the testing equipment and procedures. EEG record was carried out in a quiet, air-conditioned room with the experimenter and recording equipment present. All subjects were instructed to relax and to remain still during testing to minimize artifacts produced by ocular movements and to avoid excessive blinking. During the recording the subjects were awake with eyes closed, seated on a reclining chair. All recordings were performed in the morning.
Each resting EEG was obtained during 8 to 10 minutes with the subjects eyes closed. Subsequently, 2 minutes of alternation between closed and opened eyes were recorded, following by 3 minutes carrying out hyperventilation, 2 minutes of recovery were also recorded. Taking into account that sleepiness might have caused an enhancement of theta activity, the individual vigilance level was checked during EEG acquisition, seeking for slowing of the EEG background activity or for the appearance of typical sleep patterns. In addition, at the end of the recording process, individuals were asked about whether they were awake during the whole recording.
Visual Assessment of the EEG
A clinical neurophysiologist (first author of current research report) performed and interpreted the EEG analysis. Several bipolar montages were used for off line EEG interpretation. The EEG was considered NORMAL if it had an adequate organization of the background activity (according to the subject’s age), well-defined spatial differentiation, rhythmical alpha activity, and absence of paroxysmal activity. The SLOW EEG subgroup was characterized by the presence of persistent nonrhythmic theta-delta slow waves. PAROXYSMAL category included the EEG with activity such as spikes, sharp wave, and spike and wave. EEGs with both types of previously described abnormalities were considered in the SLOW and PAROXYSMAL category. Ratios and percentages in all categories were calculated.
Quantitative EEG Analysis
Tracings were visually inspected and edited off-line in order to eliminate epochs with movement artifacts, eye blinking, muscle activity, or drowsiness. For each subject, 20 to 24 EEG segments (without artifact) of 2.56 seconds at the closed eyes state were selected. Spectral analysis using fast Fourier transform (FFT) was carried out in order to obtain the cross spectral matrices estimation in all individual records.42,43 Cross-spectral matrices were calculated for every 0.39 Hz, from 0.78 to 19.50 Hz.
EEG Source Estimation
The EEG tomography was conducted using The low-resolution electromagnetic tomography (LORETA). 44 Each LORETA file was computed from the frequency domain EEG cross spectra corresponding to the the selected EEG frequencies, one in the alpha range (9.37 Hz) and another in the beta band (17.18 Hz). These 2 specific frequencies were selected taking in consideration the results obtained from the comparison made between the Z cross spectra of the 2 groups (see below). Current density vectors (CDVs) were calculated for each individual from all the data segments using the Neuronic Source Localizer software (Neuronic SA).
Compute lead field (LF) was the first step for brain electrical tomography calculation. This software computes electric LF using the isotropic and piecewise homogeneous three spheres head model.45,46 In this research current density distribution inside the head was calculated using a 3-dimensional grid including all brain volume. Anatomical information for LF computation was provided from a brain average template obtained at the Neurological Institute of Montreal. 47 In this study, the source space predefined was cortical gray matter plus basal ganglia and grids of 4 × 4 × 4. The number of generators used was 21 926.
The tomographic solutions were seen using the Neuronic Tomographic Viewer (Neuronic SA)
Statistical Analysis
In order to determine the dependence among categorical variables (demographic, behavioral, and visual inspection of EEG), Pearson chi-square test and 1-way analysis of variance test were used for analysis (Statistica 6.0 for Windows). The level of statistical significance was set at .05 for all the tests.
QEEG Spectrum Analysis
In order to compare the psychopathic and nonpsychopathic traits groups with normative values the Cuban normative database was used. Zsava et al 48 in 1997 reported the methodology for constructing the normative database. This was constructed from the EEG of 211 normal subjects (105 males, 106 females) with an age range from 5 to 97 years. The EEG was recorded using the same conditions in each subject. The Z standardized statistic was calculated for all spectral parameters
where µ and σ are the mean and standard deviation (SD), respectively, estimated in the normative group for the specific age of the subject been compared. The x value is the observation of each subject.
Statistical Methodology to Compare the Z Spectra Mean of Both Groups
In order to evaluate differences between the Z spectra of both groups, a permutation test was used.49-52 The permutation test has the following advantages: free distribution, which controls the experiment wise error for simultaneous univariate comparisons, no assumption of an underlying correlation structure, providing exact P values for any number of individuals, frequency points, and recording sites.
Multivariate statistics were used to summarize and test differences between 2 Z spectra obtained from the method of nonparametric combination of dependent permutation tests. 53 The method of nonparametric combination methodology of a finite number of dependent permutation tests is a general tool for multivariate testing problems. These multivariate statistics are calculated according to combined univariate t test. The combine function used was the maximum. Two separate partial tests were performed of
the maximum of t statistics in each electrode for all frequencies
the maximum of t statistics in each frequency for all electrodes.
These methodologies were obtained as follows:
Step 1: The observations were repeatedly permutated between groups. Both statistics were calculated for every repetition.
Step 2: The empirical distribution was estimated using the statistics calculated in the step above for all permutations.
Step 3: Significance levels were set using the t and max(t) of the original samples in the empirical distribution estimated in step 2.49-52
Inverse Solution Analysis
In order to identify significant regional differences between groups in current density (CDV) for beta and alpha EEG bands, a t test for independent samples with correction for multiple comparisons was performed (Neuronic Statistica software, Neuronic SA). The final outcome was a map of the t test values for each voxel thresholded at a false discovery rate (FDR) q = 0.1.
Coordinates of main activation were represented in Talairach space (Neuronic Tomographic Viewer, Neuronic SA).
Results
Demographic and Behavioral Results
Analyses of demographic data indicated no significant differences in age between the 2 groups (Table 1). Scores for APSD showed significant group differences. ADHD, dissocial conduct disorder, and oppositional defiant disorder as comorbility with CD diagnosis did not show significant group differences (Table 1).
Comparison Between the Psychopathic Traits and the Nonpsychopathic Traits Groups on Demographic and Behavioral Variables.
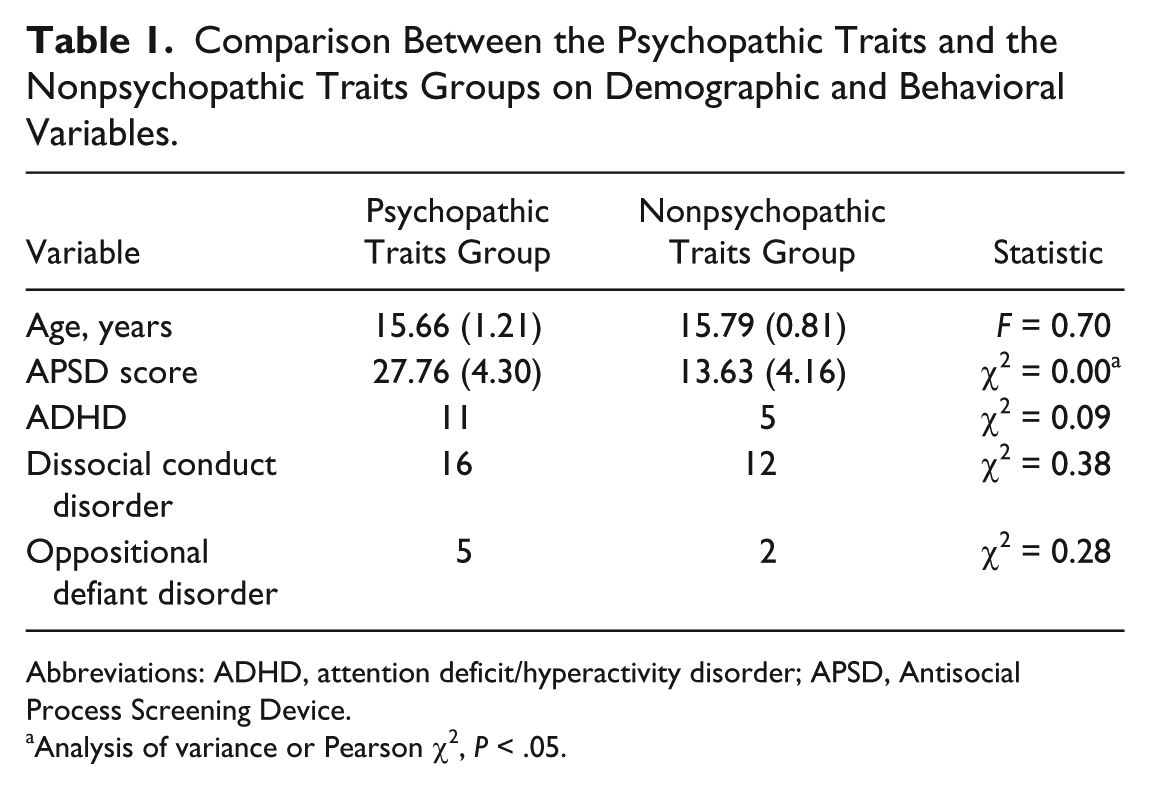
Abbreviations: ADHD, attention deficit/hyperactivity disorder; APSD, Antisocial Process Screening Device.
Analysis of variance or Pearson χ2, P < .05.
EEG Visual Inspection
The resting EEG visual analyses revealed a high percentage of EEG abnormalities in both studied groups. The total amount of abnormal EEGs were of 24 adolescent (96.0%) in the psychopathic traits group and 12 subjects (70.58%) in the control group. The number of individuals with some type of EEG abnormality in the whole sample was of 36 (85.7%).
Table 2 presents details of the EEG visual analysis results. In this analysis, both groups (psychopathic and nonpsychopathic traits) results were very similar. PAROXYSMAL EEG was the category including the highest number of subjects (around 43%), followed by SLOW EEG category (28.6%). Twelve adolescents from both groups were included in the other 2 categories.
Classification of the Adolescents’ EEG in Both Groups by Visual Inspection.
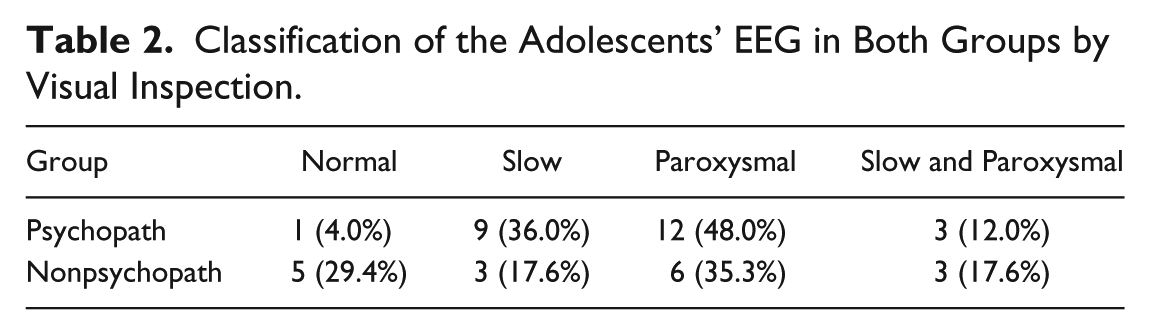
The Pearson chi-square test comparison found significant differences between the 2 groups regarding the total EEG with abnormalities versus normal EEG by visual inspection (χ2 = 5.45, df = 1, P = .02).
Table 3 shows the topographical distribution of the EEG abnormalities found in both groups. Frontal lobe was the single brain region most affected by EEG abnormalities in both groups. A comparison using the Pearson chi-square was made taking into consideration only the PAROXYSMAL category (because it was the EEG abnormality most frequent in both groups) and comparing frontal versus temporal localizations. There were differences between these topographical distributions of paroxysmal EEG activity between both groups (χ2 = 4.02, df = 1, P = .04). Paroxysmal EEG was more frequent at frontal derivations in the psychopathic traits group while temporal regions were more affected by this EEG abnormality in the nonpsychopathic traits group.
Topographic Distribution of EEG Abnormalities.

Quantitative EEG Analysis
The mean duration of EEG in the eyes-closed state for the psychopathic traits CD group was 50.08 seconds (SD ±21.86) and 49.35 seconds (SD ±12.56) for the nonpsychopathic traits CD group. No significant differences between the 2 groups were found (P = .90).
Significant statistical differences between the mean parameters of cross spectral measures of psychopathic and nonpsychopathic traits groups using the permutation test were found in the beta band within a frequency range of 13.67 to 18.75 Hz at bilateral frontal-temporal regions. The power value for this frequency was increased for the psychopathic traits group. In contrast, within the 9.37 to 9.76 Hz frequency range of the alpha band a decrease of the energy was found at the right frontal-central-temporal regions and the parietal-central lead for this same group.
Correlation Between EEG Frequencies (QEEG) and APSD Scores
Significant positive correlations were found between the “blames others for mistakes” (r = 0.38; P < .02), “lies easily and skillfully” (r =0.38; P < .01), “keeps promises” (r = 0.34; P < .03), “brags about accomplishments” (r = 0.32; P < .05) with the beta energy level at central parietal region. These correlations were not statistically significant after correction for multiple comparisons.
EEG Source Analysis
Comparison of Beta Activity Sources (LORETA) Between Groups
The sources of the increased beta activity at 17.18 Hz were localized on the following Brodmann’s areas: 11, 12 (orbitofrontal cortex); 6 medial frontal; 44 (opercular portions of the inferior frontal gyrus); 8 (superior frontal gyrus) and 13 (insula) in both hemispheres; 7 (postcentral area); 4 precentral, 22 (superior temporal gyrus), 21 (medial temporal gyrus); 38 (superior temporal pole), putamen and globus pallidus in the left hemisphere and 45 (tri portions of the inferior frontal gyrus) in the psychopathic traits group when they were compared with nonpsychopathic offenders (FDR q = 0.1) (Table 4; Figure 1).
Brain Areas Showing Statistical Differences (q = 0.1) in Beta Frequency (17.18 Hz) Between Psychopathic Traits and Nonpsychopathic Teenagers According to Voxel-by-Voxel Analysis With Low-Resolution Brain Electromagnetic Tomography (LORETA). a
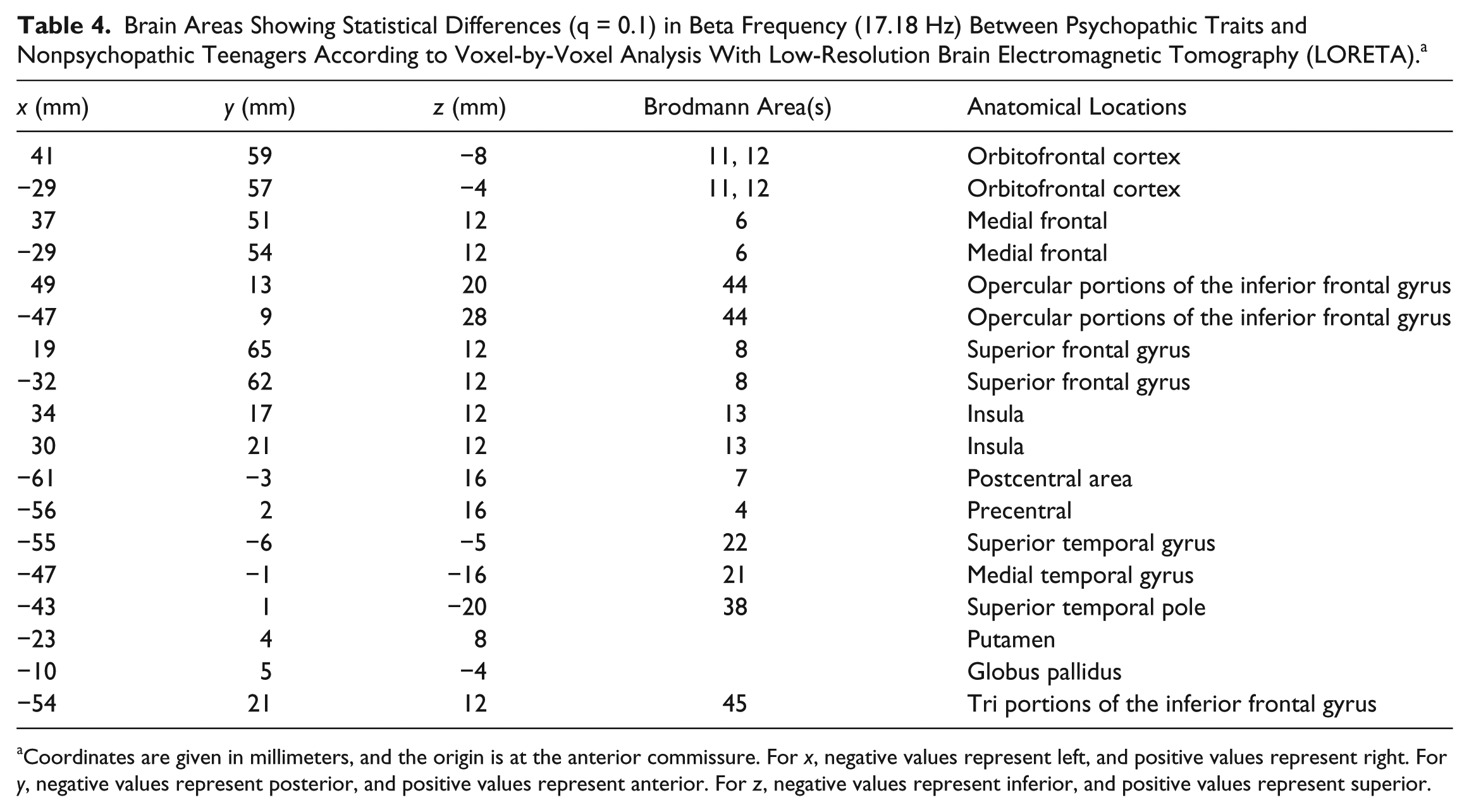
Coordinates are given in millimeters, and the origin is at the anterior commissure. For x, negative values represent left, and positive values represent right. For y, negative values represent posterior, and positive values represent anterior. For z, negative values represent inferior, and positive values represent superior.
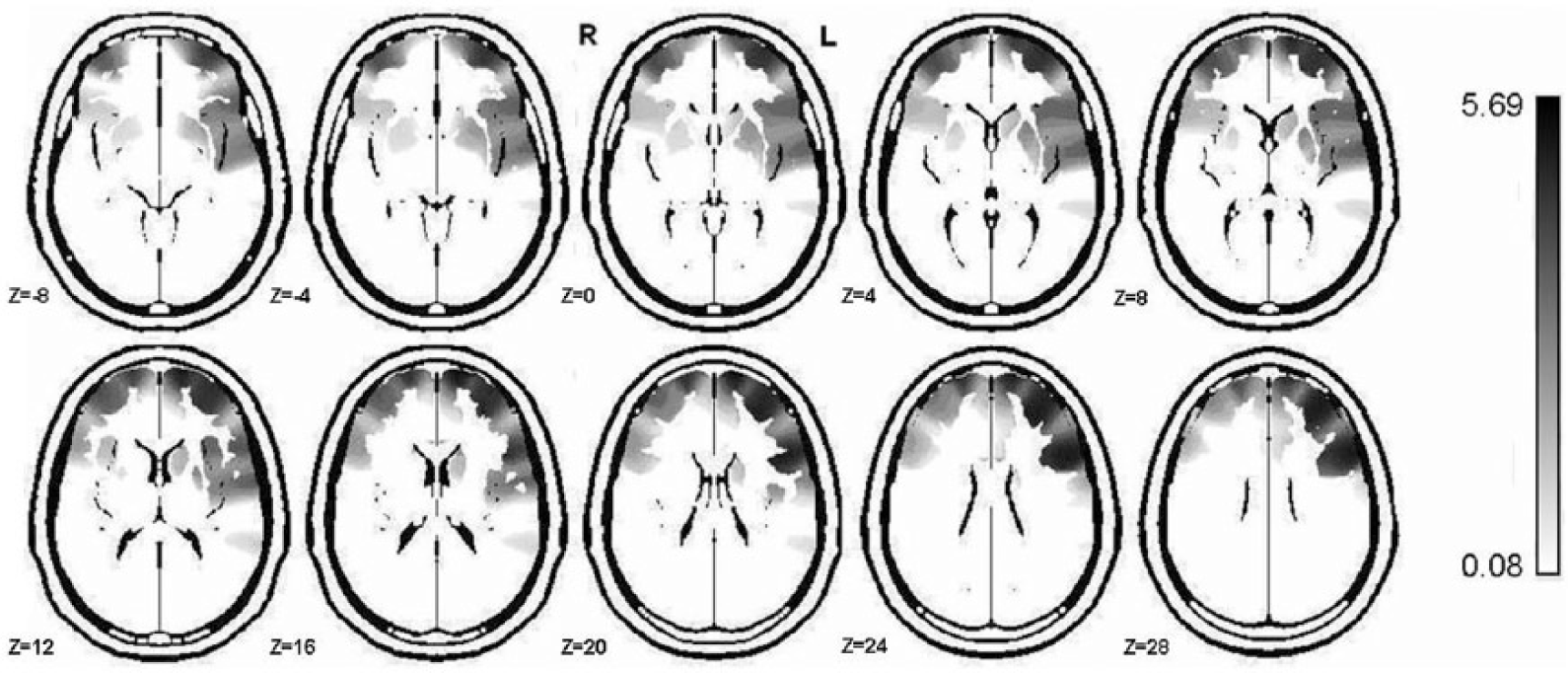
The anatomical distribution of the sources of beta activity (17.18 Hz) increased in psychopathic traits group were localized a broad region within both hemispheres. The main region where the sources were found were orbitofrontal cortex, medial frontal; opercular portion of the inferior frontal gyrus, superior frontal gyrus and insula in both hemispheres, postcentral area, precentral, superior temporal gyrus, medial temporal gyrus, superior temporal pole, putamen and globus pallidus in the left hemisphere and tri portion of the inferior frontal gyrus in the psychopath group. R, right hemisphere; L, left hemisphere. Z is the z-axis value for each image of the brain template showed.
There were no significant group differences in alpha band.
Discussion
In the present study, the paroxysmal activity was the abnormality most frequently found through EEG visual inspection. The frontal lobe was the single brain region most affected by both types of EEG abnormalities (paroxysmal and slow) in both groups. There were group differences between topographical distributions of paroxysmal EEG activity. The frontal paroxysmal activity was higher in psychopathic traits group. In the nonpsychopathic traits group, this type of EEG abnormality was localized predominantly in the temporal lobe. Other EEG studies of CD adolescent have typically found similar frequency of EEG abnormality in qualitative EEG assessment as ours.53,54
Significant differences in QEEG and regional current source density between psychopathic and nonpsychopathic traits groups were also found. The psychopathic traits group had more beta energy at bilateral frontal-temporal regions and less alpha activity in the right frontal-central-temporal regions and the midline parietal-central lead than the control group. LORETA showed differences especially in the frontal and temporal cortices.
Increase of beta activity and decrease of alpha power were found in the psychopathic traits group when QEEG results were compared with the control group. Similar findings have been demonstrated in children with ADHD,33,34 in female delinquents, 55 in psychopathic offenders, 30 and adult delinquents with ADHD. 35
Beta activity is believed to result from cortical/cortical and thalamo/cortical interactions. Activity in the beta frequency band, a presumed index of the level of cortical arousal, has consistently shown associations with externalizing spectrum disorders28,29,56 such as substance abuse disorders, conduct disorder, and antisocial behavior. 57 The increased beta may indicate cortical hyperarousal. Our findings could potentially be interpreted as evidence of cortical disinhibition in the psychopathic traits group as compared with nonpsychopathic traits group.
Decrease alpha activity in adolescents with disruptive behavior had been associated with a failure in functional cortical development (maturational retardation hypothesis).58,59 This finding is consistent with research that demonstrates less alpha activity levels in delinquent children 59 and in institutionalized children. 60 Alpha is the normal rhythm seen in a subject who is awake with his or her eyes closed. It is maximal over the occipital and, to a lesser extent, the parietal regions, and is often less evident over the dominant hemisphere. The adult pattern of dominant alpha rhythm becomes evident in late adolescence and is referred to as the mature EEG. 61 Nevertheless, by the age range of studied subject; we consider that this finding supports the existence of maturational lag of CNS in adolescents with psychopathic traits.
Studies in both animals and humans have shown the thalamus and regions of occipital and parieto-occipital cortices are involved in alpha rhythm generation. 61 Previous research reveals that the modulations of alpha frequency among neurologically intact adults depend on the structural integrity of white matter tracts. 62 Consistent with this idea, Sheridan et al 63 suggested that reduced alpha power observed in the EEG of children exposed to institutional rearing may be the result of delay in the development of cortical white matter (WM). Results from longitudinal studies have demonstrated that normal brain development shows a linear increase in white matter from childhood to adulthood. The WM increment makes the signal transduction become faster and more efficient, allowing increasingly higher frequency contributions to the overall signal. WM maturation is an essential element of brain development and is fundamental for normal function and cognitive maturity.64,65 Ineffective signal transduction due to decreases in myelination could be one explanation for alpha power reduction.
An important finding was that the sources of increase of beta activity in psychopath traits adolescents, using LORETA were localized on the frontal cortex, the temporal cortex, insula, and the striatum (putamen and globus pallidus). These results support the idea that psychopathic traits could be associated with brain abnormalities in a frontal-temporo-striatal circuit that is involved in emotion, learning, reward processing and motivational aspects of behavior. 66
LORETA solves the inverse problem by constraining the electrical neuronal activity to fulfill with the property of maximal synchronization, that is, by assuming similar activation among neighboring neuronal sources. A prerequisite to being able to define the inverse solution results within the structural MRI is the co-registration between these 2 imaging modalities, that is, the EEG space and the MRI space. 44 This step requires that electrode positions are matched to the scalp surface defined by the MRI using some transformation (rotation and translations) operations. These parameters are usually obtained by measuring some “common” landmarks during both the EEG as well as the MRI acquisition. Most commonly, MRI-visible markers are placed on the skin that correspond to the position of the electrodes and/or some fiduciary landmarks (eg, nasion, inion, pre-auricular points and vertex). In order to avoid the labor-intensive measurement of the electrodes and fiduciary landmarks on every subject, many studies use one single MRI template (such as the average brain from the Montreal Neurological Institute) and assume a standard electrode coordinate system. In this case, predefined translation parameters are used to match the EEG to the MRI space. Individual differences in head size and electrode positions are thereby ignored, leading to limited accuracy with regard to the anatomical precision of the source locations. The use of individual anatomical MRI to calculate sources of localization eliminates these limitations and contributes to increasing the accuracy of LORETA localization as has been demonstrated by different research.67,68 LORETA is a technique that facilitates a deeper understanding of the neurological findings present in the EEG. 44 In general, LORETA helped to define the structures related to the increase of beta activity as a sign of a dysfunctional (hyperexcitability) neuronal state, probably secondary to CNS injury. To our knowledge, no previous studies of LORETA using QEEG involving psychopath traits adolescent samples have been published.
While using generic minimum-norm methods, it has been shown that deeper sources may not be recovered properly because more superficial dipoles with smaller magnitudes would be privileged for the same EEG/MEG data set. That is the reason why lead field normalization can be operated to give all the sources, those close to the surface and deeper ones, the same opportunity of being nicely reconstructed with a minimum-norm technique. 69 LORETA combines the lead-field normalization with the Laplacian operator, thus, gives the depth-compensated inverse solution under the constraint of smoothly distributed sources. It is based on the maximum smoothness of the solution.69,70 The LORETA source estimates work in the entire inner volume of the head. The source space is sampled according to a regular grid of voxel. Each grid point corresponds to a regional source made of 3 orthogonal dipoles. The LORETA priors correspond to a smooth distribution of the source intensities in the entire source space.
LORETA current density findings in the present study and the surface EEG findings are also consistent with MRI studies showing a reduced frontal and temporal lobes, striatal volume71-73 and reduced cortical surface area in adolescents with CD. 74 Dysfunction within the striatum and prefrontal cortex had been observed in youths with psychopathic traits causing deficits in the capacity to relationship rewards or punishments with stimuli or responses. 3 Moreover, there is evidence that the use of outcome information by the anterior insula, inferior frontal cortex and dorsomedial prefrontal cortex to guide the individual away from suboptimal behavioural choices75,76 is disrupted in adolescents with psychopathic traits. 77
Different studies have revealed interesting and reproducible relations between current sources and network connectivity that provide a deeper understanding of the surface EEG dynamics.36,78 Our finding could be caused by abnormal functional connectivity among the structures related with the increase of beta activity.
Our results support theoretical models of psychopathy that suggest it is a neurodevelopmental disorder.4,79 A neurodevelopmental perspective of psychopathy is consistent with the fact that the disorder has its roots early in life. 80 It has been stated that psychopathic traits are present early in life and develop throughout childhood and adolescence. 81 Its course since first manifestations is steady and progressive and is relatively resistant to conventional treatments.82-84
Our results are consistent with other neurobiological perspectives that emphasize the role of frontal-temporal areas in psychopathy. The prefrontal cortex (PFC) regulates attention, behavior, and emotion through extensive network connections with other brain regions. According with frontal roles, Blair 3 emphasizes that one of the core impairments associated with psychopathic traits, is a deficit in decision making and in reinforcement learning, which reflects dysfunction in the ventromedial prefrontal cortex and striatum.
There are 2 other significant models of psychopathy that are supported by findings of deficiencies in the prefrontal cortex: the somatic marker hypothesis 85 and the prefrontal dysfunction theory. 86 Damasio hypothesis 85 suggests that a psychopathic individual may have limited ability to consider emotions when making a decision. This impairment causes self-defeating behavior and violation of social norms with detrimental consequences, all behaviors indicative of the psychopathic profile. Gorenstein and Newman 86 reported significant correlations between human disinhibition and lesions in the prefrontal cortex. Prefrontal areas of the adolescent brain may be less efficient in generating inhibitory responses and the activation in these frontal areas may be linked to “disinhibition.” 86
Consistent with other research, our findings suggest poor decision making and emotional dysregulation associated with psychopathic traits may be due to, at least in part, functional anomalies in frontal and temporal regions whereas striatal structural variations may contribute to sensation-seeking and reward-driven behavior in psychopathic traits individuals. 12 The temporal lobe is involved in theory of mind and its dysfunction is often implicated in violent psychopathy. The anterior/middle temporal gyrus has a secondary role, being recruited during working memory and general cognitive processing. The superior temporal sulcus evaluates the intentionality and social complexity of moral actions. 87 The insula has been implicated in integrating interoceptive states into conscious feelings, decision making, and empathy and pain recognition in others88-90 and thus may be important in understanding decision making deficits seen in adolescent with psychopathic traits. Our research confirms that CNS functional impairment of psychopathy concern to more than one brain region.
Several neuroimaging studies in adolescents with psychopathic traits have revealed reduction of gray matter in the prefrontal cortex, insula, striatum,71-73 paralimbic regions, including orbitofrontal cortex, bilateral temporal poles and posterior cingulate cortex16,17 and abnormal brain activation in limbic regions,91-93 as well as in the prefrontal and temporal lobes. 94 A recent study employing diffusion tensor imaging found that adolescents with conduct disorder showed reduced fractional anisotropy of the uncinate fasciculus pathway connecting the amygdala and orbitofrontal cortex. 95
Summarizing, the results of this study support the hypothesis that fronto-temporal-striatal brain functions are impaired in psychopathic trait adolescents. QEEG and LORETA results indicate that adolescents with CD do not constitute a homogeneous group in terms of EEG profile. Both types of EEG assessment could be important tools for the identification of functional abnormalities of CNS that can to be evaluated as possible biomarkers into psychopathic traits.
Some important limitations of the present report are (a) in the current study only EEG visual inspection was used to remove artifacts. However, in some EEGs, the impact of biological artefacts may still represents a significant problem, the elimination the contaminated EEG segments can bear to the loss of information and viability for clinical diagnosis. Future studies should use automated artefact rejection procedure, as independent component analysis (ICA),96-98 to remove residual artifacts not detected by visual inspection. (b) Some studies using EEG measurements have produced laterality effect; however, the majority of them have not evaluated the resting EEG or analyzed EEG frequency bands separately.99-101 Unfortunately, in this study, handedness was not controlled. It would be advisable for future research to include the evaluation of handedness preference and its possible connection with the presence of lateralized abnormalities in CD teenager subgroups.
Footnotes
Acknowledgements
The authors gratefully acknowledge two anonymous referees for their constructive comments and suggestions that were very helpful in improving the manuscript.
Author Contributions
Ana Calzada-Reyes contributed to conception and design of the study, adquisition, analysis and interpretation of the data, drafted the manuscript. Alfredo Alvarez-Amador contributed to conception and design of the study, analysis and interpretation of the data, revised the manuscrip, gave final approval. LídiceGalán-García contributed to design of the study, analysis of the data, revised the manuscript. Mitchell Valdés-Sosa contributed to conception and design of the study, interpretation of the data, revised the manuscript.
Declaration of Conflicting Interests
The author(s) declared no conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.