
Abstract
Interictal focal EEG features were frequently observed in generalized, epilepsies, but there is limited information about interictal, epileptiform/nonepileptiform generalized paroxysms in focal epilepsies. We aimed to report the frequency and associated factors of generalized EEG discharges in focal epilepsy with unknown cause (FEUC) and mesial, temporal lobe epilepsy with hippocampal sclerosis (MTLE-HS). A total of 200 patients (FEUC in 90 patients; MTLE-HS in 110 patients) were included. Generalized epileptiform (spike/sharp waves simultaneously in all regions) and nonspecific generalized discharges (paroxysmal slow waves) were investigated. All clinical and laboratory findings of 2 groups were compared with each other and with remaining control group, without generalized paroxysms, statistically. Generalized EEG features were present in 22 (11%; 4 males) patients; 9 in the FEUC group (10%; 2) and 13 in the MTLE-HS group (11.8%). Female gender (P < .021), febrile seizure (P < .034), precipitant factors (P < .025), and parental consanguinity (P < .033) were significantly higher in the group with generalized EEG findings. Monotherapy rates were lower in the MTLE-HS group (P < .05). The relationship of generalized EEG features with female gender and parental consanguinity may point out to a genetic property among focal epilepsies, while the relationship with febrile seizures and precipitant factors may be a clue about mechanisms with more extensive involvement of the neuronal networks.
Keywords
Introduction
Over the past decades, it is well established that focal and generalized epilepsies do not show a clear-cut dichotomy with regard to many points, including their interictal electroencephalography (EEG) features. Although, for the most part, the dichotomy is quite clear between idiopathic/genetic generalized epilepsy and focal epilepsy, there are some difficult cases to diagnose. The old concept of dichotomy1,2 mostly relied on the belief that focal and generalized epilepsies may have different levels of susceptibility to epileptogenic activity based on different etiologic precipitating and triggering factors. 3 This susceptibility is relatively high in generalized epilepsies where many brain regions are affected equally and simultaneously, thus reaching seizure threshold together, whereas in the focal epilepsies, a specific brain region has more tendency than the others to reach this threshold and trigger a limited seizure. It is now thought that the dichotomy between epilepsies is rather artificial in some patients, but it is accepted that a continuity exits between them. In line with this point, there have been many studies reporting the presence of focal EEG features in various forms of generalized epilepsies, in recent years.3-7 The presence of focal EEG abnormalities was reported up to very high rates such as 65% in some EEG studies. 3 On the contrary, for unknown reasons, there is a lack of studies about the presence of epileptiform or nonepileptiform “generalized” discharges in the interictal EEG of focal epilepsies. In a handful of studies, the presence of rare generalized-like EEG discharges is assumed to originate from deeply located and fast propagating focal foci representing secondary bilateral hypersynchrony.8,9
The aim of our study is to report the frequency and associated factors of generalized EEG discharges and the relationship of these discharges with prognosis, in interictal EEG studies of 2 different and large cohorts of focal epilepsies; namely the focal epilepsy with unknown cause (FEUC) and mesial temporal lobe epilepsy with hippocampal sclerosis (MTLE-HS).
Material and Methods
Patient Selection
Patients followed up in our epilepsy center and diagnosed as FEUC or MTLE-HS according to the criteria of International League Against Epilepsy (ILAE) 10 with a minimum of 1 EEG available for reevaluation in our EEG laboratory were included to the study.
The diagnosis of focal epilepsy was determined by at least 2 of the following criteria:
A definite clinical description of recurrent “aura” and/or the presence of a lateralizing sign in seizure semiology.
Focal seizure recordings in ictal EEG or the presence of a definite focal epileptiform abnormality in interictal EEG of the patient.
The diagnosis of focal epilepsy was supported by the presence of clear focal hypometabolism in positron emission tomography (PET) imaging of the patients with normal magnetic resonance imaging (MRI).
The local ethics committee has approved the study protocol.
Other additional inclusion criteria for FEUC were a minimum of 5 years of follow-up to define the prognosis clearly, ages between 16 and 75 years, and at least 1 normal 1.5- or 3-T MRI performed with specific epilepsy protocol. The presence of hippocampal sclerosis in MTLE was determined by presence of atrophy in T1-weighted images and hyperintensity with the degeneration of internal structure of hippocampus in T2/FLAIR (fluid-attenuated inversion recovery) weighted images as previously described.11,12
We excluded all other various structural focal epilepsies and also focal epilepsies with other known causes (like autoimmune epilepsies) because we did not want to include nonhomogeneous epilepsy groups. We assumed that the different localizations, magnitudes and multiplicity of the lesions and different etiologies like encephalitis and so on might create misleading generalized appearances and contaminate our findings.
Seizure types and epileptic syndromes were classified and the auras, if present, were classified according to Report of the ILAE Task Force on Classification and Terminology. 13 Drug resistance was defined according to the criteria published by Kwan et al. 14 Precipitant factors were defined as having 1 or more of the following in the history: febrile seizure, head injury, preterm or difficult delivery but without any lesion on MRI. Investigated triggering factors for seizures include stress, fatigue, sleep deprivation, menses, mental activity, showering, brilliant light, sound, fear, emotions, and listening to music.
Data Collection
We collected following data from the medical records: age, sex, age of onset, duration of epilepsy, family history of epilepsy, presence of aura, history of febrile seizure and status epilepticus, drug resistance, psychiatric comorbid diseases, precipitant factors, parenteral consanguinity, monotherapy, presentation with a focal to bilateral tonic-clonic seizure as the first seizure, having nonspecific white matter lesions (WML) on MRI, and mental retardation. The initial EEG and all other follow-up EEGs of both focal epilepsy cohorts were reviewed by 2 senior board-certified clinical neurophysiologists (BB and NB) working in the tertiary epilepsy center of our university hospital with a minimum of 10 years of experience in epileptology with regard to the presence of epileptiform (presence of spike/sharp waves simultaneously in all regions) and nonspecific generalized (paroxysmal generalized slow waves) discharges, in their interictal EEG examinations. Although nonspecific generalized discharges do not have the same relevance with epileptiform discharges, we aimed to discuss if these 2 separate groups of generalized EEG changes might have common points and therefore compose a large group and included both types of generalized EEG changes. EEGs were recorded with scalp electrodes placed according to the International 10-20 system with bipolar and reference montages. Standard activating procedures were performed in all participants. The definitions for EEG activities were as follows: spike, a transient activity with a duration between 20 and 70 ms that can be clearly distinguished from the background activity; sharp wave, an epileptiform transient with variable amplitudes and a duration of 70 to 200 ms that can be clearly distinguished from the background activity; slow wave, a wave with a longer duration than alpha activity. 15
The files of the patients with generalized interictal EEG features were reviewed with a standardized form by 2 investigators systematically and compared with the remaining patients without any generalized interictal EEG findings.
Moreover, all available PET scans of the groups were reevaluated by an experienced nuclear medicine specialist.
Statistical Analysis
Descriptive statistics were applied and the 2 focal epilepsy groups were compared between and with the control group consisting of rest of the patients according to their clinic, semiological, PET and EEG properties statistically. Chi-square test, Fisher’s exact test, and t test were used where appropriate. IBM SPSS Statistics Version 24 was used, and the level of significance was set at P < .05.
Results
A total of 200 patients fulfilling our inclusion criteria (90 with FEUC and 110 with MTLE-HS) with a mean of 4.8 ± 2.7 EEG examinations were included. The mean age of the main group was 39.38 ± 11.28 years, the mean age of onset was 16.31 ± 12.04 years, and disease duration was 21.53 ± 10.83 years.
Generalized EEG features were present in a total of 22 (11%) patients; 9 in FEUC group (10%; 4 epileptiform, 5 nonspecific generalized) and 13 in MTLE-HS group (11.8%; 6 epileptiform, 7 nonspecific). The clinical and laboratory features of both focal epilepsy groups, including the postoperative EEG findings of the operated patients, are summarized in Table 1. Figures 1 and 2 demonstrate examples of focal and generalized epileptiform EEG findings, and ictal seizure activity of the patient diagnosed with FEUC. Figures 3 demonstrated example of nonspecific generalized EEG findings of a patient with FEUC.
Clinical Characteristics of Patients With Generalized EEG Features. a
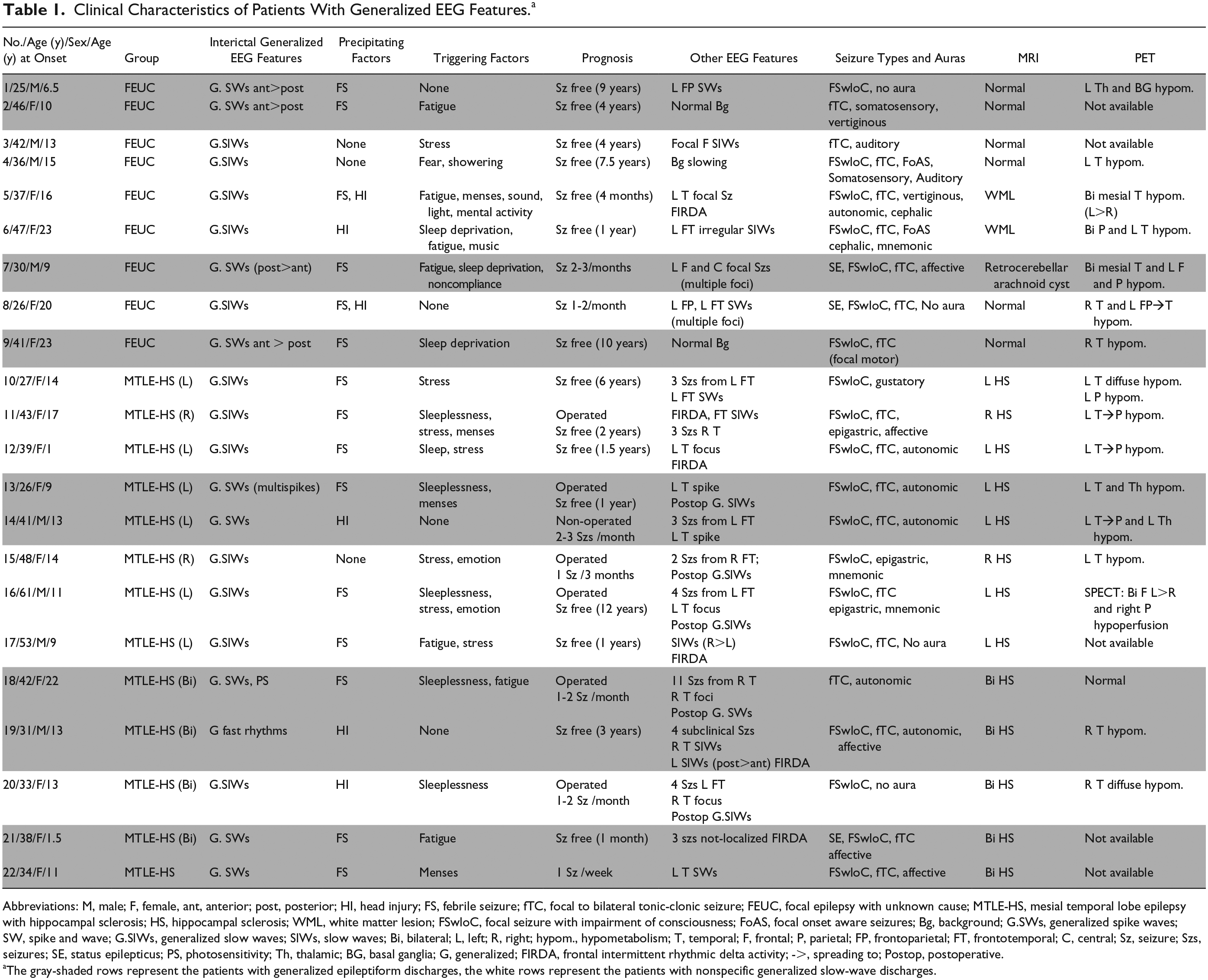
Abbreviations: M, male; F, female, ant, anterior; post, posterior; HI, head injury; FS, febrile seizure; fTC, focal to bilateral tonic-clonic seizure; FEUC, focal epilepsy with unknown cause; MTLE-HS, mesial temporal lobe epilepsy with hippocampal sclerosis; HS, hippocampal sclerosis; WML, white matter lesion; FSwloC, focal seizure with impairment of consciousness; FoAS, focal onset aware seizures; Bg, background; G.SWs, generalized spike waves; SW, spike and wave; G.SlWs, generalized slow waves; SlWs, slow waves; Bi, bilateral; L, left; R, right; hypom., hypometabolism; T, temporal; F, frontal; P, parietal; FP, frontoparietal; FT, frontotemporal; C, central; Sz, seizure; Szs, seizures; SE, status epilepticus; PS, photosensitivity; Th, thalamic; BG, basal ganglia; G, generalized; FIRDA, frontal intermittent rhythmic delta activity; ->, spreading to; Postop, postoperative.
The gray-shaded rows represent the patients with generalized epileptiform discharges, the white rows represent the patients with nonspecific generalized slow-wave discharges.
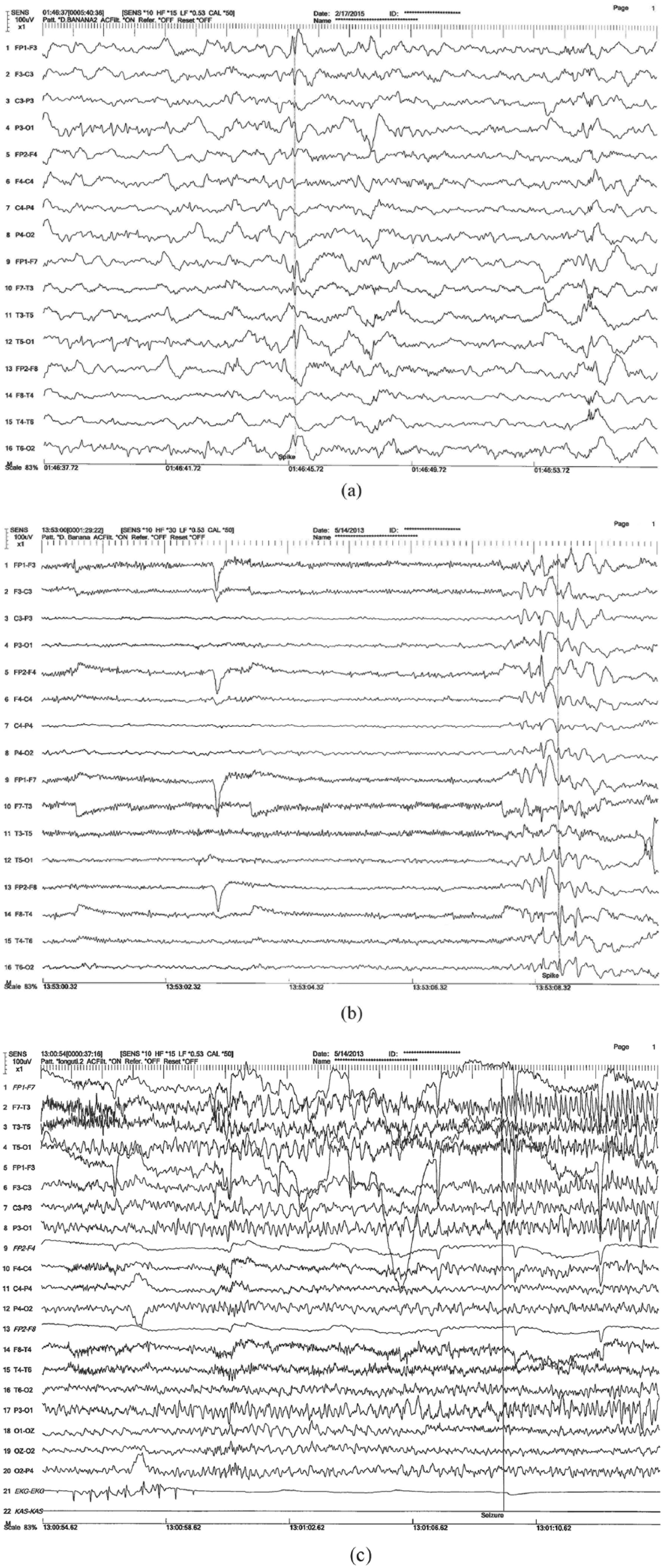
The EEG examples of a 30-year-old female patient (Table 1, No. 7). She had focal seizures with impairment of consciousness with an affective aura and ictal oral-alimentary automatisms since she was 9 years old. (a) Interictal focal spike and waves over the left temporal area. (b) Atypical generalized interictal epileptiform discharges of the same patient. (c) Her ictal EEG showing left temporal onset of a focal seizure with automatisms.
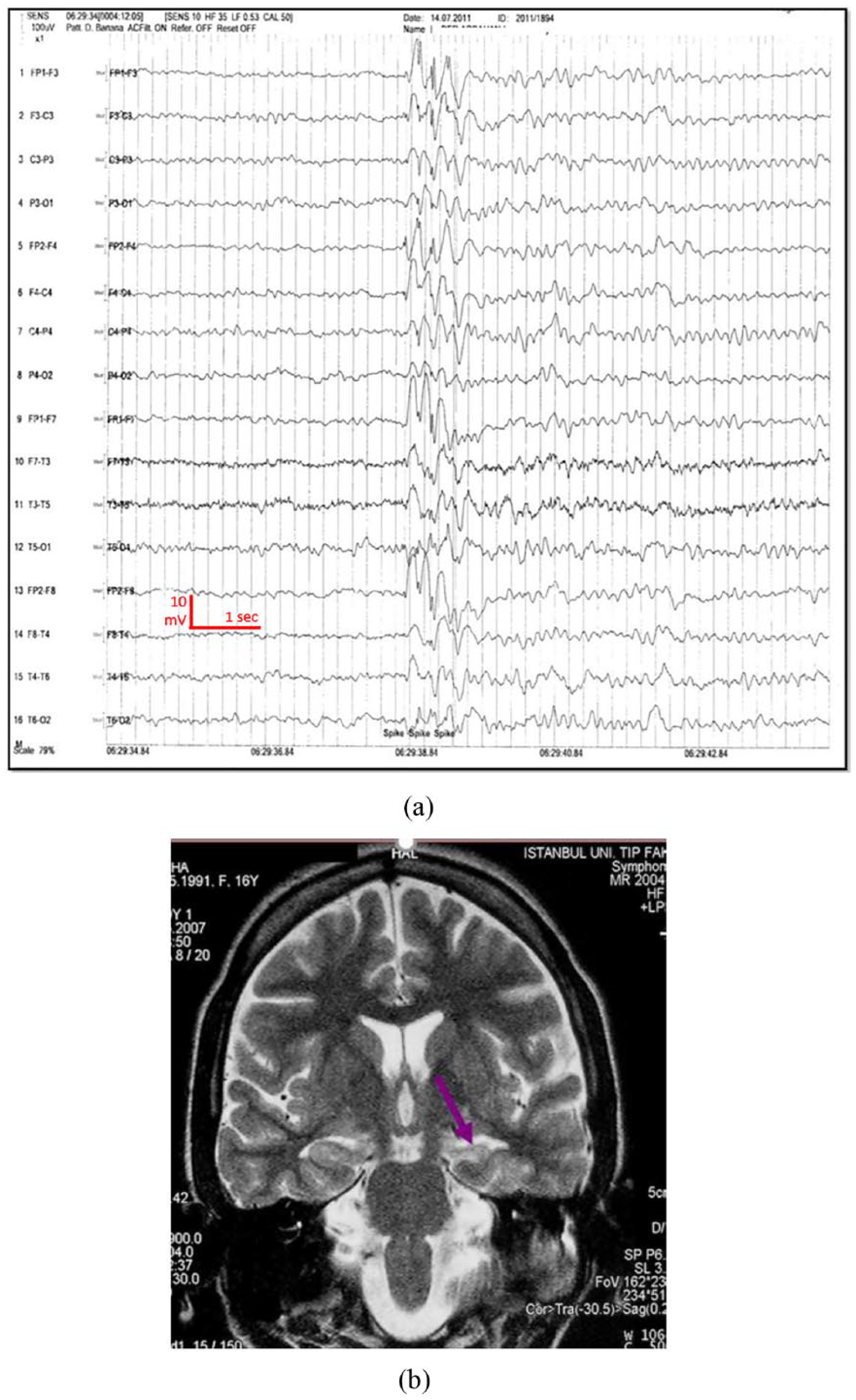
The examples of a 26-year-old female patient (Table 1, No. 13) with an autonomic aura and ictal oral automatisms. She had focal seizures with impairment of consciousness since she was 15 years old. (a). The interictal EEG of the patient with intermittent slow generalized waves. (b). The MRI showing the left hippocampal sclerosis on coronal plane.
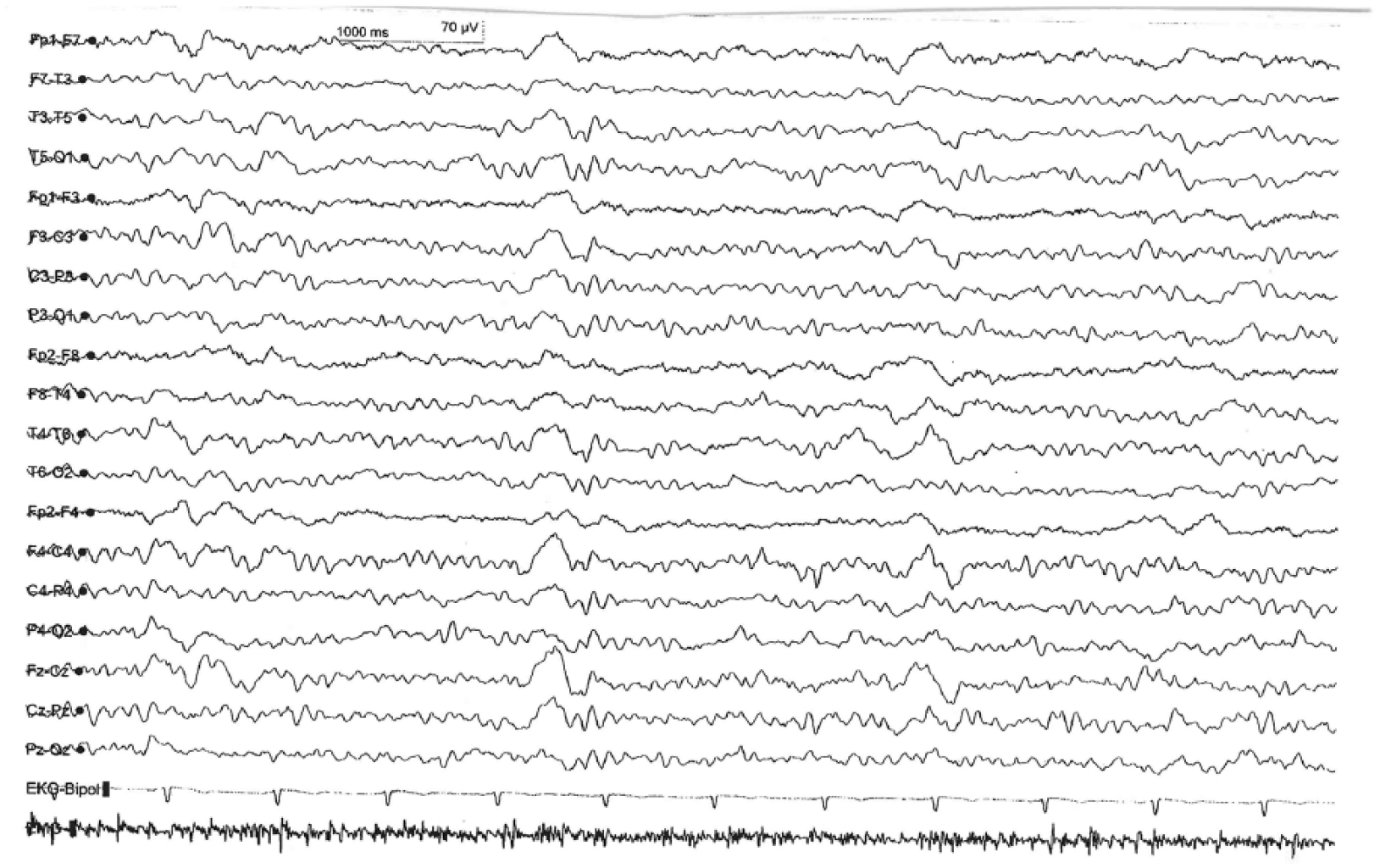
The example of nonspecific generalized EEG bursts of a patient with focal epilepsy with unknown cause (FEUC).
Only 4 of these patients were male. Female gender (P < .021), history of febrile seizure (P < .034), presence of precipitant factors (P < .025), and parental consanguinity (P < .033) were significantly different between generalized EEG group and the rest of the group. The mean current age of 22 patients with generalized EEG features was 38.58 ± 9.11 years, whereas their mean age at seizure onset was 13.13 ± 6.12 years, and disease duration was 23.84 ± 10.33 years. These values were not different from the control group. The comparisons of all patients with interictal generalized EEG features and without generalized EEG features are shown in Table 2.
The Comparisons of the Patients With or Without Generalized EEG Features. a
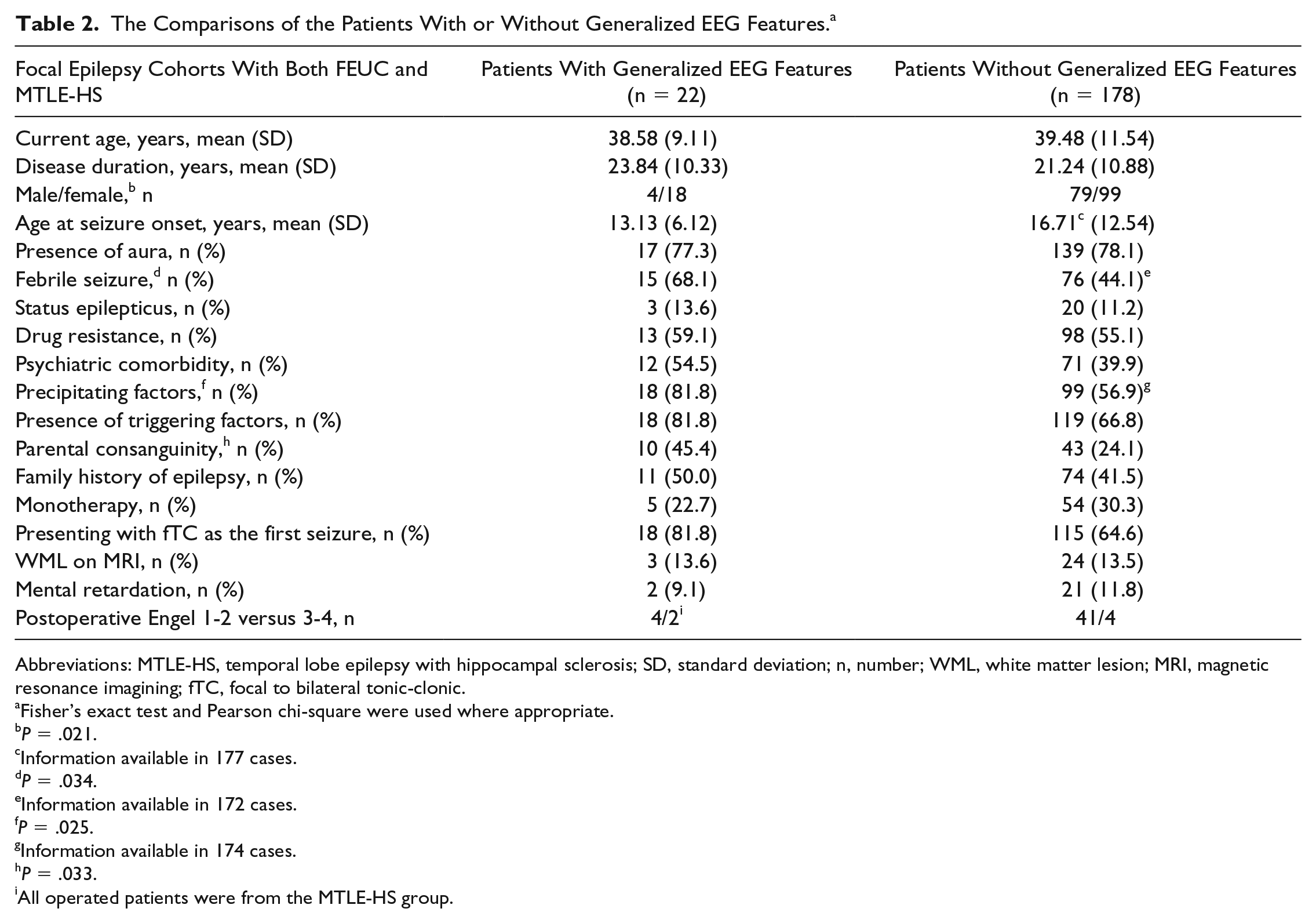
Abbreviations: MTLE-HS, temporal lobe epilepsy with hippocampal sclerosis; SD, standard deviation; n, number; WML, white matter lesion; MRI, magnetic resonance imagining; fTC, focal to bilateral tonic-clonic.
Fisher’s exact test and Pearson chi-square were used where appropriate.
P = .021.
Information available in 177 cases.
P = .034.
Information available in 172 cases.
P = .025.
Information available in 174 cases.
P = .033.
All operated patients were from the MTLE-HS group.
Febrile seizures (P < .029) were observed more frequently in the FEUC group, whereas triggering factors (P < .02) and parenteral consanguinity (P < .009) were higher in the MTLE-HS group compared with the control group.
The comparisons of patients with only generalized epileptiform EEG findings and nonepileptiform generalized EEG findings separately, with the control group showed that the presence of precipitating factors (P = .011), presenting with focal to bilateral tonic-clonic seizure (fTC) as the first seizure (P = .030), family history of epilepsy (P = .042) were found significantly different in patients with generalized epileptiform discharges when compared with other patients with focal epilepsy.
When we evaluated the EEGs of our 10 patients with generalized epileptifom discharges with regard to the presence of secondary bilateral synchrony (SBS) (because the concept of SBS does not include patients with slow activities), 1 patient in FEUC group had discharges suggesting SBS, with a latency of 100 ms but, the leading discharges were coming from left side in some of the EEGs and in some other EEGs, they came from the right side, which is not compatible with the SBS concept. The epileptiform generalized discharges of the rest of the patients were bilateral synchronized without a leading discharge.
A comparison among the patients with generalized features between the 2 focal epilepsy syndromes showed that monotherapy rates were significantly lower in the MTLE-HS group compared with the FEUC group (P < .05), but there was no difference with regard to other clinical properties.
Discussion
This retrospective study investigated a neglected topic of clinical epileptology and found that interictal generalized EEG discharges, either epileptiform or nonepileptiform could be observed in 10% to 12% of the patients diagnosed with 2 common types of focal epilepsies, namely FEUC and MTLE-HS, with similar rates. Female gender and parental consanguinity, as well as febrile seizure history and presence of precipitant factors appeared to associate with these generalized discharges. Two focal epilepsy groups with generalized EEG features had no difference in terms of other clinical aspects except the lower monotherapy rates in MTLE-HS, as expected.
To our knowledge, this is the first study investigating the presence of generalized EEG features in 2 different, large focal epilepsy cohorts, simultaneously with the same methodology. The possible mechanisms for explaining the presence of these discharges were coexistence of focal and generalized epilepsy in the same patient or SBS, a term first coined by Tukel and Jasper 16 in 1952. SBS can be described as bilateral synchronous EEG discharges, possibly arising from a unilateral cortical focus.9,16 Discharges from abnormal cortex spread to the bilateral hemispheres rapidly by using extensive brain connections like corpus callosum or other subcortical pathways.17,18 SBS could be supported either by showing the presence of a neuroradiologic lesion in a critical location as the focal origin of the seizures or by using invasive EEG electrodes to demonstrate the relationship of focal epileptogenic lesion and generalized discharges generated from this focus. 19 Moreover, new noninvasive techniques like continuous EEG–functional MRI recording, independent component analysis of generalized spike-and-wave discharges, coherence phase analysis and magnetoencephalography (MEG) have been developed to localize the ictal onset zone and to help for differentiating SBS from primary bilateral synchrony (PBS).17,18,20-22 Although SBS was first shown in frontal lobe lesions, other cortical regions like temporal and occipital lobes may also be associated with these discharges.17,23 It should be noted, however, that interictal scalp EEG may not always distinguish SBS from PBS accurately because the leading focal spike may not be noticed or may be originated from a deep mesial sulcus and may be invisible on routine recordings from the scalp. 21 We did not use invasive evaluations in our patients, because of the lack of clinical needs and could not show any responsible lesions except HS, thus we did not have any evidence for SBS. Moreover, PET studies also did not support any focal critical lesion associating with the generalized EEG discharges in these patients with focal epilepsy.
A handful of articles point out to the coexistence of generalized EEG findings in patients with focal epilepsy. In a retrospective analysis, 9 patients representing <1% of the total group showed generalized EEG abnormalities coexisting with focal interictal EEG features, despite the presence of focal onset seizures as the major seizure type. 4 Regarding the associated factors, they could not find an association between febrile seizure history and the presence of generalized epileptic discharges 4 although it was one of the determinants of the occurrence of these generalized discharges in patients with focal epilepsy in our study. In another large study on patients with drug-resistant temporal lobe epilepsy (TLE), the coexistence of TLE and idiopathic generalized epilepsy (IGE) was reported as 1.8% (12 patients). Only 5 patients had interictal generalized discharges in the preoperative phase, and the majority of the patients (7 patients) showed the EEG and clinical manifestations of IGE at the postoperative follow-up period. Similar to our results, febrile seizure rates were high in their series, suggesting a genetic predisposition. 24
In the current study, female gender and parental consanguinity seemed to be associated with interictal generalized EEG features in focal epilepsy which resembles the positive association of these features with photosensivity (PS). PS is generally accepted as a marker of IGE and shown to be more common in female patients and associated with parental consanguinity.25-28 The female:male ratio of PS was reported as 1.5:2.1 in a recent study. 29 This predominance in females remains still to be uncovered and it might be attributed to the influence of hormonal mechanisms or a genetic background.30,31 The parenteral consanguinity also might be accepted as another evidence of a genetic background in these patients.32,33 These common features of female dominance and parenteral consanguinity both in our group and in patients with PS may suggest a clue of a coexisting IGE with a focal epilepsy in our patient cohort. There are other well-known examples of genetic epileptic syndromes with coexisting focal and generalized seizures like genetic epilepsy with febrile seizures plus (GEFS+). 34 This is a genetic disorder with autosomal-dominant inheritance, in which members of the families with this disorder may develop febrile seizures, generalized tonic-clonic seizures and also focal seizures especially originating from temporal lobe. 35 Additionally, syndromes like Dravet syndrome and Lennox-Gastaut syndrome are other established examples of both seizure types existing in an individual patient and expressing EEG findings of both generalized and focal epileptiform discharges. 36 It should be noted that both focal and generalized seizure types can be part of a genetically transmitted epileptic process. 37
The lower monotherapy rates in MTLE-HS group is understandable, owing to the higher drug resistance rates in this focal epilepsy group.38-40 Five patients in our FEUC group were on monotherapy regimen while all patients were on polytherapy in MTLE-HS group compatible with higher drug resistance rates in the latter.
It can be conflicting to decide epilepsy surgery as a therapeutic option in focal epilepsy with generalized discharges. In a retrospective study on a large pediatric cohort, 50 patients with an early acquired or congenital brain lesion had satisfactory seizure-free rates after surgery (72%) and interestingly they could not find any significant difference of benefit from surgery between the patients with or without generalized interictal EEG findings. Most of the patients in this cohort underwent more extensive epileptic surgeries than normal surgical candidates; therefore, a generalization of these results may not be applicable to the whole population. 41 There are other reports about successful surgery in patients with both focal and generalized EEG findings. 42 Jeha et al 43 reported the coexistence of focal and generalized epilepsy as 0.2% in adults and they stated that the presence of generalized EEG findings did not affect their surgical success rates. They also reported a high incidence of febrile seizure history (57%) in their patients which is similar to our findings suggesting a link to a genetic background. 43 Another retrospective study revealed successful surgery rate of 57.1% in their patients despite having preoperative interictal generalized EEG findings, though 42.9% continued to have recurrent seizures, suggesting that patients who had little benefit from surgery might have coexistent generalized and focal epilepsy. 44 In our series, 6 MTLE-HS with generalized EEG findings were operated and 4 patients had favorable results as seen in Tables 1 and 2. These results indicated that generalized discharges did not contradict with successful epilepsy surgery but showed somewhat lower rates of seizure freedom without reaching statistical significance in our small group.
There are controversial reports about the benefits of surgery in FEUC.23,45 Sunwoo et al 23 reported unfavorable surgical outcomes in focal epilepsy groups, including FEUC with generalized interictal EEG discharges. Their seizure-free rate was relatively low (18.2%) indicating the involvement of more extensive epileptogenic networks by SBS leading to poor ictal localization and rapid seizure propagation. 23
Our large clinical study has several limitations due to its retrospective design; however, all clinical data and MRI findings, ictal/interictal EEG recordings were carefully reanalyzed by 2 epileptologists with a standardized form. Also, some of the patients in our study group had a favorable prognosis without drug resistance therefore did not have ictal EEG and PET studies. In the light of our limitations, more caution should be warranted interpreting our results with a statistical significance.
In conclusion, our study showed that generalized EEG findings can exist at substantial rates (10%-12%) in 2 different common focal epilepsy cohorts. Focal and generalized epilepsies should be assumed as overlapping groups since they may use similar neuronal networks, therefore could not be separated with sharp boundaries. Planning further studies and clinical management on this fact seem to be more precise.
Footnotes
Author Contributions
AÇA contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. ENVY contributed to conception; contributed to acquisition; drafted manuscript; critically revised manuscript; agrees to be accountable for all aspects of work ensuring integrity and accuracy. EY contributed to analysis and interpretation; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. NB contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. BB contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research and/or authorship of this article: This study was supported by the Istanbul University Research Fund (Project No. TDP-2018-31114).