
Abstract
Introduction:
Suicide is the second leading cause of death among adolescents. Suicidal behavior is associated with impairments in attention. Attention can be directed toward relevant events in the environment either actively, under voluntary control, or passively, by external salient events. The extent to which the risk for suicidal behavior affects active and passive attention is largely unknown.
Methods:
Event-related potentials (ERPs) were recorded while 14 adolescents with acute suicidal behavior and 14 healthy controls performed an auditory 3-stimulus oddball task. The task consisted of standard (80%), target (10%), and novel (10%) stimuli. The participants were instructed to press a button upon presentation of the target. The novel stimuli were unexpected and irrelevant to the target detection task.
Results:
Accuracy of target detection was slightly but significantly reduced in the suicidal group. There were no significant differences in the amplitude of the target-N2 or -P3b between groups. There was a slight, but nonsignificant, increase in the amplitude of the novel-N2 and -P3 in the suicidal group.
Conclusions:
This is the first study to explore both passive and controlled aspects of attention using ERPs in adolescents with acute suicidal behavior. Although there were no significant ERP group differences, this is an important step in identifying objective markers of suicide risk among adolescents.
Introduction
The World Health Organization indicates that suicide is the second leading cause of death among 10- to 24-year-olds. 1 In adolescence, suicidal behavior is associated with cognitive impairments that are known to have debilitating impacts on psychosocial functioning, 2 with deficits in attention being one of the most consistently reported impaired functions. 3 -7 Attention allows the observer to become aware of highly relevant events. This may be a result of either passive or active attention. 8 The extent to which the risk for suicidal behavior affects active and/or passive attention is largely unknown.
Passive attentional processing (or attention capture) appears to be an obligatory, stimulus-driven process evoked by the occurrence of highly relevant, but unexpected, events. Deficits in attention capture can have negative consequences. Although it provides a means of becoming aware of potentially relevant input, the vast majority of this input turns out, in fact, to be irrelevant. An abnormally low threshold for attention capture may result in frequent interruptions of the central executive and “distract” attention away from ongoing cognitive activities. On the other hand, an abnormally high threshold may result in an inability to become aware of truly relevant events, which is critical for survival. Attention is also associated with active, voluntary processing of relevant events. Deficits in the voluntary control of attention may result in an inability to sustain attention, which is critically important for many higher aspects of cognition.
Event-Related Potentials and Attention
An auditory oddball paradigm, consisting of frequently occurring “standard” stimuli and randomly and rarely occurring “target” stimuli, is often used to study attentional processing. In an active oddball task, participants are asked to actively detect the target stimuli. 9,10 In the 3-stimulus oddball variant, rarely occurring novel stimuli are also randomly presented but are irrelevant to the target detection task. Participants are thus asked to withhold a response following their presentation. Event-related potentials (ERPs) provide an exquisitely sensitive means to monitor the extent of processing of the novel stimuli in the absence of a behavioral response. 11 -13 ERPs were thus recorded during the 3-stimulus oddball task.
Accurate target detection will elicit a parietally maximum P3b ERP component around 300 to 400 ms after stimulus onset. The P3b is commonly associated with allocation of voluntary, controlled attention and active detection of relevant events. 14,15 The task-irrelevant novel stimuli, on the other hand, may elicit a more centrofrontal earlier, 200 to 300 ms, positivity, the novel-P3. There is general consensus that it reflects an automatic stimulus-driven alerting process of the frontal lobes’ central executive and the switch of attention toward novel unexpected events. 16,17 The novel-P3 and the target-P3b have been shown to be statistically independent by the use of principal component analysis 18 and independent components analysis. 19 The sources of the P3b appear to be near the temporal-parietal junction while the sources of the novel-P3 are within the frontal region near the anterior cingulate cortex. 20
Another frontocentral ERP component, the N2, occurring around 200 ms, can also be elicited by both target and novel stimuli. The N2 is best observed in a difference waveform, obtained by subtracting the ERPs to the standard stimuli from the ERPs to both the target and novel stimuli. The novel- and target-N2 may, however, reflect different cognitive processes. Luck and Hillyard 21 suggested that the target-N2 reflects the extent of cognitive effort required for the controlled detection of stimulus change, while the novel-N2 reflects processes associated with a general mismatch/alerting system.
Event-Related Potentials and Suicidal Behavior
Only a limited number of studies have examined the P3 in association with suicidal behavior in adults. 22 -26 A history of suicide attempts has been shown to be associated with reduced target-P3b amplitudes. 23 -26 Active oddball tasks have not been run in adolescents with suicidal behavior. The executive processes involved in active target detection may well be different in the nonmature brain. Furthermore, to our knowledge, no study has investigated whether adolescent suicide attempters exhibit deficits in processes associated with the target- and novel-N2.
Very few studies have examined passive attention in individuals with suicidal behavior. 25,27 Jandl et al 25 observed a reduced P3 following both target and novel stimuli in the second half of their recording but only for participants having more violent suicide attempt methods. Differences were not apparent between those with less violent methods and healthy controls. Tavakoli et al 27 examined P3a amplitudes, suggestive of attention capture, in adolescents with acute suicidal behavior and healthy controls while participants watched a silent video and thus ignored a multi-feature auditory sequence. They reported an enhanced P3a to the novel sound deviants in the suicidal group suggesting that the suicidal patients may exhibit hypersensitivity to potentially relevant but to-be-ignored stimuli. They might be more susceptible to interruptions of the central executive by rare but irrelevant stimulus events.
The Present Study
In the present study, adolescent inpatients with acute suicidal behavior and healthy controls were compared. The same novel sounds used by Tavakoli et al 27 were presented but within an active 3-stimulus oddball paradigm, consisting of frequently occurring standard stimuli, rarely occurring targets, and novel sounds. The participant’s task was to respond to the occurrence of only the target stimulus. The novel sounds were therefore irrelevant to the task. Previous adult studies have indicated that suicidal behavior is associated with an inability to sustain voluntary, effortful attention. It might therefore be expected that active detection of the target stimulus will be more difficult in suicidal adolescents. This could result in a larger target-N2 but reduced target-P3b in this group. Tavakoli et al 27 observed that passive attention capture was enhanced in their suicidal group. It is therefore possible that the while the target-P3b may be reduced, the novel-P3 may be enhanced in the suicidal group.
Methods
Participants
The participants were 14 (9 females) adolescent psychiatric inpatients admitted to the children’s hospital for an acute risk of suicide and 14 age- and gender-matched healthy controls. Adolescents ranged in age from 13 to 17 years (mean = 15.7 years, SD = 1.1). The sample size was deemed to be appropriate based on a power analysis of effect size, using group means and SDs observed in our previous study. 27 With this effect size, a sample of 10 participants per group was found to be adequate. When the effect size was reduced to approximate mean group differences found in other studies, a sample size of 14 was found to be adequate. These estimates were calculated using G*Power software, version 3.1.9.7. 28
Clinical interviews with patients and families were conducted by a board-certified psychiatrist within 24 hours of admission to the hospital. Diagnosis was based on clinical interviews using DSM-5 (Diagnostic and Statistical Manual of Mental Disorders, fifth edition) criteria. With regard to other psychiatric diagnoses, participants having the following comorbidities were excluded: schizophrenia, pervasive developmental disorder, and attention deficit hyperactivity disorder.
A brief screening interview was conducted with the control participants by a member of the research team prior to enrollment in the study to ensure no prior diagnosis of any psychiatric illnesses or admission to a mental health facility.
None of the participants had reported a history of hearing or neurological disorders. The control participants were asked to refrain from recreational drugs and alcohol prior to the study. Written informed consent was obtained from all participants, and parents when necessary, prior to the start of the study. Participants received an honorarium for their participation. The study was approved by ethics boards at the University of Ottawa and the children’s hospital. The study was conducted according to the Canadian Tri-Council (Health, Natural, and Social Sciences) guidelines on ethical conduct involving human subjects.
Medication
A requirement was that potential inpatient participants were not being treated using benzodiazepines prior to the start of the study. All patients were treated with medication, including antidepressants (selective serotonin reuptake inhibitors [SSRIs]) and/or atypical antipsychotics.
Psychological Assessment
The severity of depression symptoms was assessed using the Revised Children’s Anxiety and Depression Scale (RCADS). 29 It assesses 6 subscales: (1) Separation Anxiety Disorder, (2) Social Phobia, (3) Obsessive Compulsive Disorder, (4) Panic Disorder, (5) Generalized Anxiety Disorder, (6) and Major Depressive Disorder, and 2 total scores (1) Total Anxiety, (2) and Total Internalizing.
The presence and severity of suicidal symptoms were assessed using the Self-Injurious Thoughts and Behaviors Interview (SITBI) 30 . The SITBI is a structured interview that assesses the presence, frequency, and characteristics of a wide range of self-injurious thoughts and behaviors, including nonsuicidal self-injury (NSSI), suicidal ideation, and suicide attempts.
Neurophysiological Recording
EEG activity was recorded using Grass gold-cup electrodes. Brain Products’ BrainAmp amplifiers and Recorder software were used for the recording of the physiological signals. The EEG was recorded from 13 electrodes (F3, Fz, F4, C3, Cz, C4, P3, Pz, P4, O1, O2, M1, M2) according to the 10/20 system of electrode placement. The nose served as a reference. Additional electrodes were placed at the supra- and infra-orbital ridges and outer canthus of each eye to record vertical and horizontal eye movements and blinks. Interelectrode impedances were kept below 5 kohm. The high-frequency filter was set at 75 Hz and the time constant was set at 2 seconds. The physiological data were digitized continuously at a 500 Hz sampling rate.
Procedure and Stimuli
Participants in both groups were tested between 14:00 and 16:00 hours. Auditory stimuli were presented monaurally to the right ear using an EAR 3A insert earphone. An auditory 3-stimulus oddball paradigm was presented consisting of standard, target, and novel auditory stimuli with probabilities of 0.80, 0.10, and 0.10, respectively. The stimuli were presented in a pseudorandom order, in that target or novel stimuli could not be presented consecutively. The participants were instructed to respond only to the target stimuli using a mouse. All stimuli had a duration of 200 ms and a rise-and-fall time of 5 ms. The standard stimulus was an 80 dB SPL 1000 Hz pure tone. The target stimulus was an 80 dB SPL 1500 Hz pure tone. The novel sounds had an average intensity of 80 dB SPL. A different novel sound 31 was presented on each trial so that none of the novel sounds were repeated. The novel sounds are described in detail by Fabiani et al. 31 The first 10 tones in the sequence consisted of only standards. The inter-stimulus interval was 1000 ms. A total of 850 stimuli were presented in a single sequence, consisting of 680 standards, 85 targets, and 85 novels. A sequence thus lasted about 17 minutes. Three brief rest periods were given within the sequence approximately every 4 minutes.
Event-Related Potential Analysis
The data were reconstructed using Brain Products’ Analyzer2 software. The continuous EEG data was band-pass filtered between 0.1 and 30 Hz (24 dB/octave slope
Quantification and Statistical Analyses
ERPs to the 3 stimuli were initially identified using the grand averaged data separately for patients and controls. The ERP waveform to the target and novel stimuli elicited a series of positive- and negative-going components that were not apparent in the waveform following the standard stimulus. These components are best observed in a difference wave, computed by subtracting point-by-point, the standard from the target ERP and the standard from the novel ERP, at each electrode site. This has the advantage of removing commonalities and leaving only processing that is unique to targets/novels. The N2 was identified at Fz, the novel-P3 at Cz, and the target-P3b at Pz, where they tend to be maximum in amplitude. All ERPs were quantified using the mean of all the data points within ±25 ms of the peak amplitude that was identified in the grand average. They were subsequently measured at Fz, Cz, and Pz.
Differences in the amplitude of the ERP components were tested separately for the target-P3b, novel-P3, and N2 using a 2 × 3 analysis of variance (ANOVA) procedures with group (patients, controls) as a between-subject factor and electrode site (Fz, Cz, Pz) as a within-subject factor. For all statistical analyses, a Geisser-Greenhouse correction was used when appropriate. 34 Correlations were also conducted on the individual participants’ target- and novel-P3 and -N2 amplitudes and the scores on the RCADS subscales and SITBI. These correlations were computed separately for patients and controls.
Results
Psychological Assessment
The demographic and clinical characteristics of both groups are listed in Table 1. The suicidal patients had significantly higher scores across all subdomains of the RCADS (P < .01 in all cases), except for obsessive compulsive disorder (P > .05). None of the control group participants exhibited any signs of NSSI, suicidal ideation, or suicidal behavior.
Demographic and Clinical Characteristics of the Control and Patient Groups.
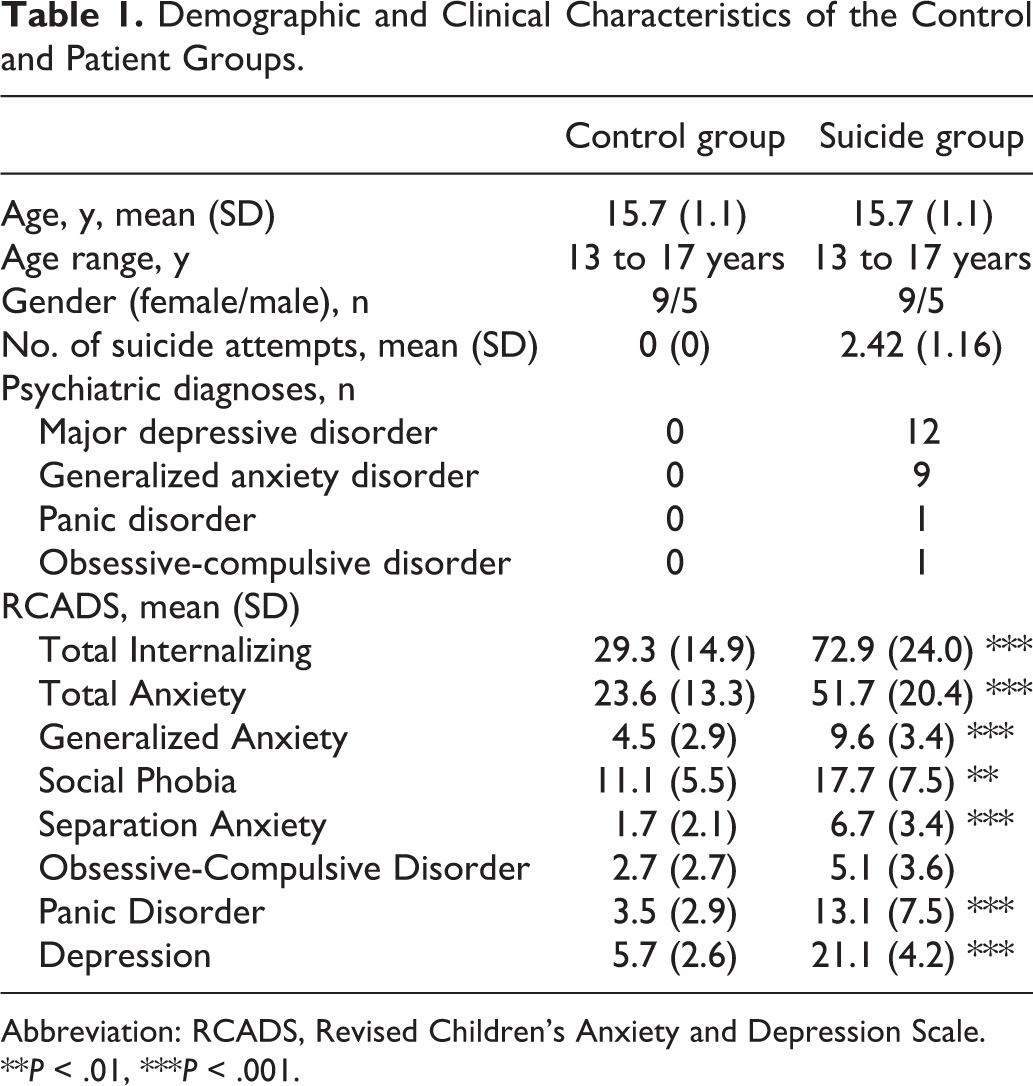
Abbreviation: RCADS, Revised Children’s Anxiety and Depression Scale.
**P < .01, ***P < .001.
Behavioral Results
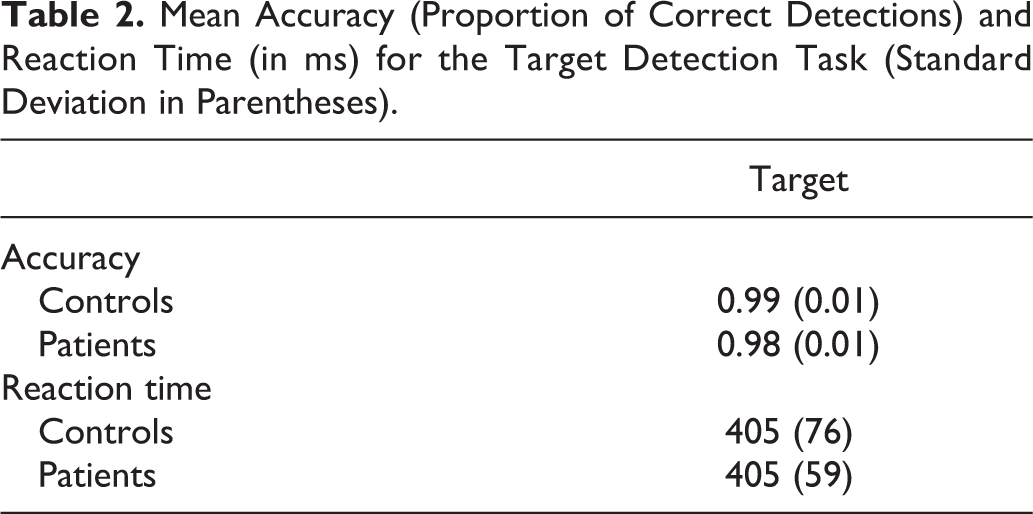
Mean accuracy and reaction time (RT) scores for both groups are listed in Table 2. Accuracy of target detection was very high for both groups. Accuracy was, however, significantly reduced in the patient group, t(26)=2.37, P = .02. For RT, there were no significant differences between patients and controls (t < 1).
Mean Accuracy (Proportion of Correct Detections) and Reaction Time (in ms) for the Target Detection Task (Standard Deviation in Parentheses).
Physiological Results
Standard ERPs
Figure 1 illustrates the ERPs to the standard stimulus for both groups. The amplitudes of both the N1and P2 (at about 100 and 180 ms, respectively), measured at Cz, did not significantly differ between groups (t < 1).
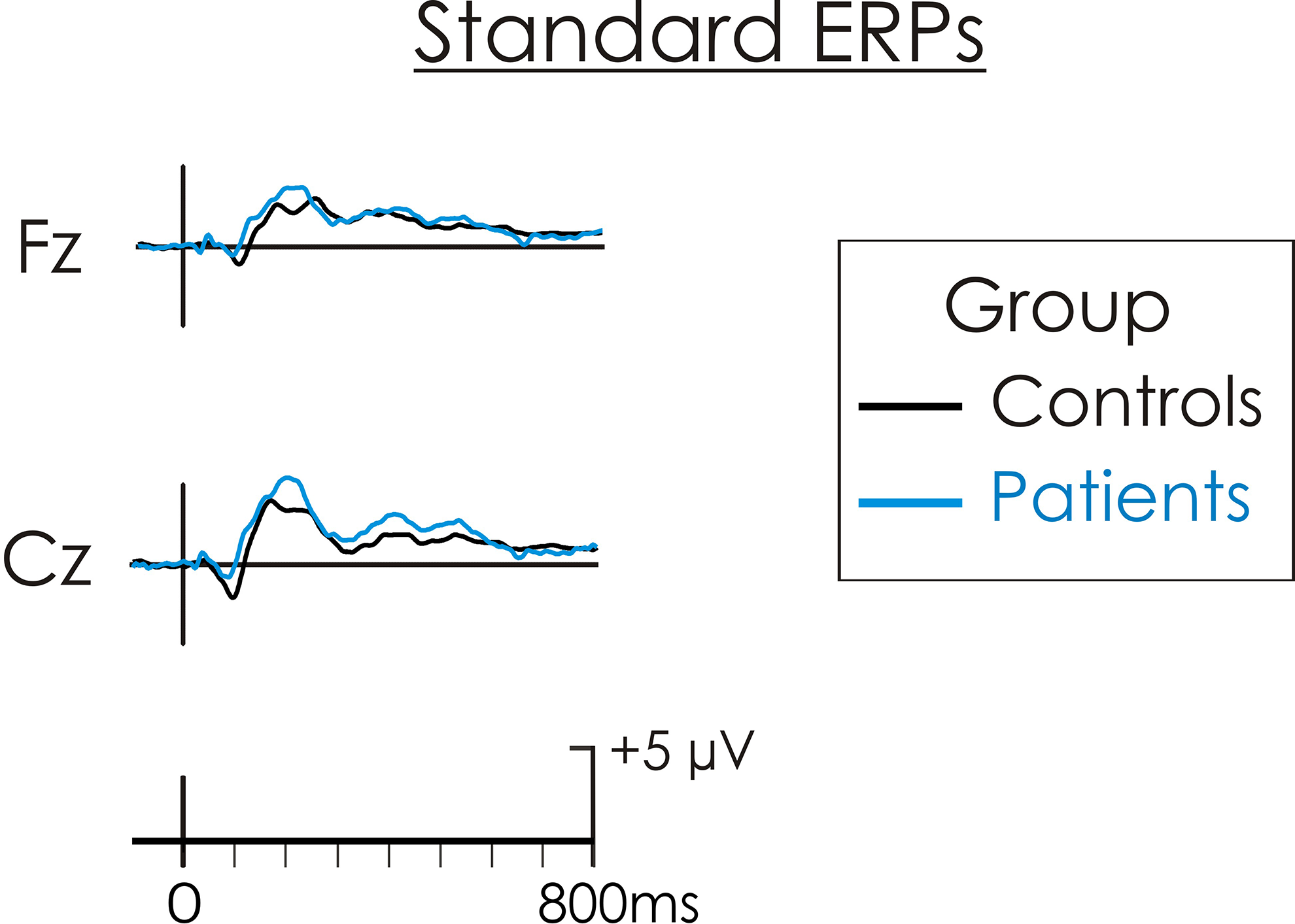
Grand average event-related potentials (ERPs) to the standard stimulus for patients (blue line) and controls (black line). The amplitudes of both the N1 and P2 did not significantly differ between patients and controls.
Target ERPs
The mean amplitudes for all ERP components are presented in Table 3. The target ERPs are illustrated in Figure 2. The target-N2 was largest at Fz, F(2, 52) = 9.75, mean square error (MSE) = 3.83, P = .0002, η2 p = 0.27. Its amplitude was larger in patients, but the difference was not significant, F(1, 26) = 2.03, MSE = 29.11, P = .16, η2 p = 0.07. The interaction between group × electrode site was also not significant, F(2, 52) = 2.14, MSE = 3.83, P = .13, η2 p = 0.08.
Mean N2 and P3 Amplitudes (in μV) (Standard Deviation in Parentheses) for Control and Patient Groups.
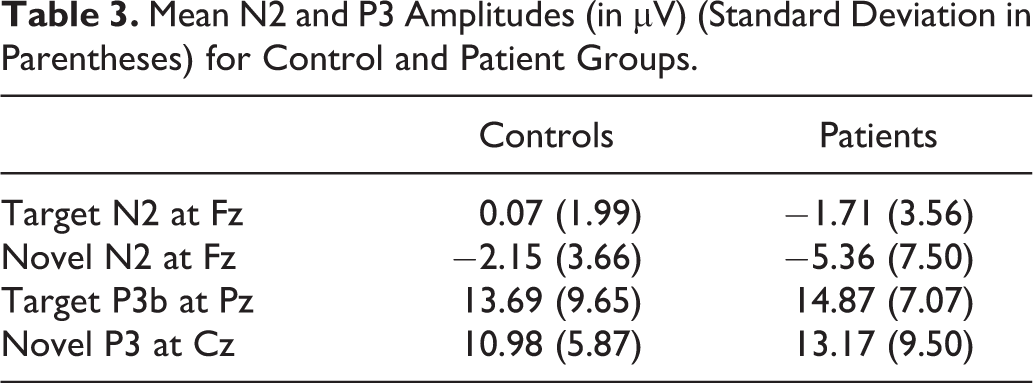
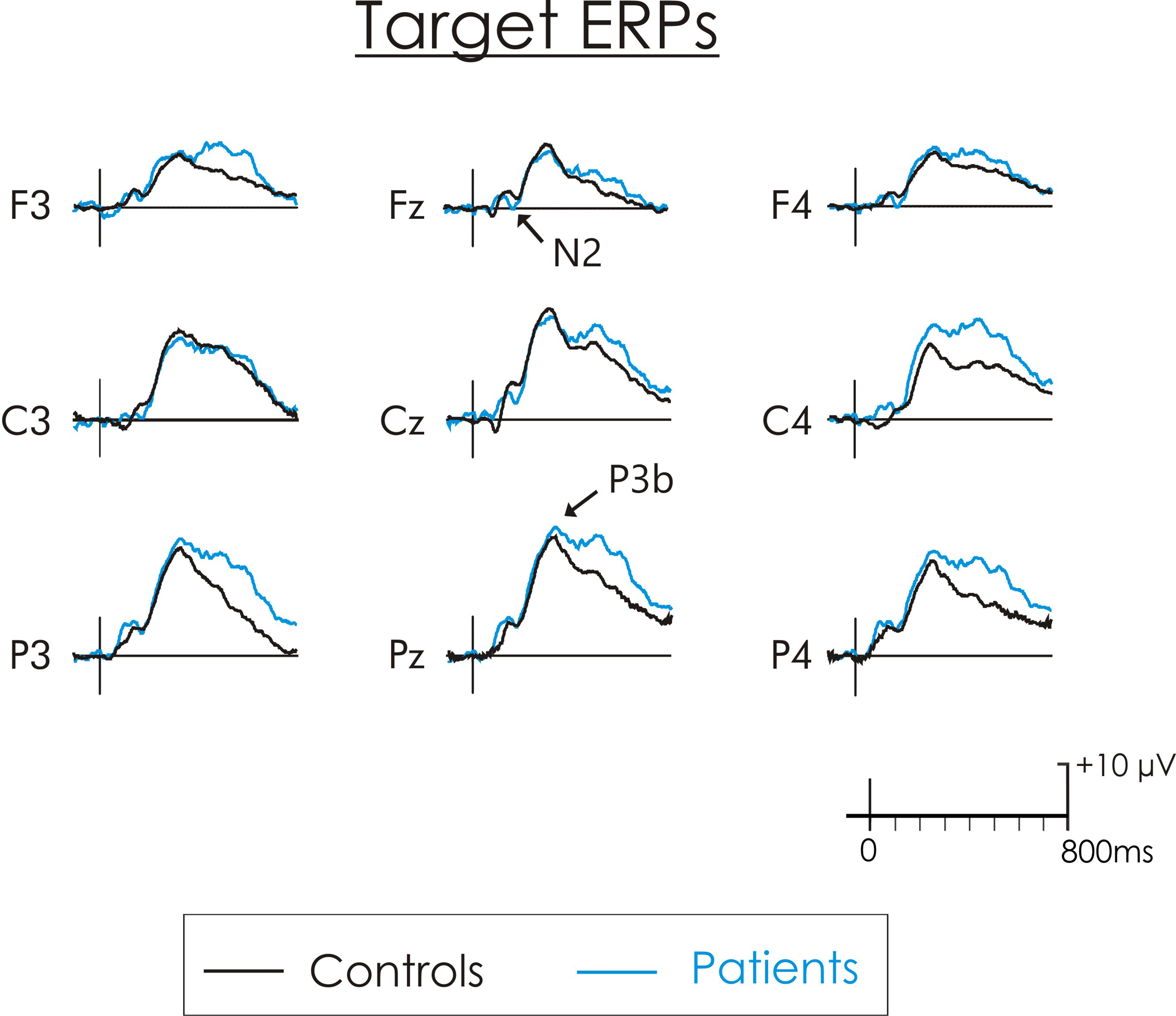
Grand average target-standard difference waves for patients (blue line) and controls (black line). The target stimulus elicited an N2 and a later P3b component. There were no significant group differences for the target-N2 or -P3b.
As expected, the target-P3b was largest at Pz, F(2, 52) = 32.65, MSE = 14.55, P = .0001, η2 p = 0.56. There was no significant difference in its amplitude between patients and controls, F(1, 26) = 0.008, MSE = 133.92, P = .92, η2 p = 0.0003. The interaction between group × electrode site was also not significant, F(2, 52) = 0.76, MSE = 14.55, P = .47, η2 p = 0.03.
Novel ERPs
The novel ERPs are illustrated in Figure 3. The amplitude of the novel-N2 was largest at Cz but the difference across electrode sites was not significant, F(2, 52) = 0.15, MSE = 3.94, P = .86, η2 p = 0.005. Its amplitude was larger in patients, but the difference failed to reach significance, F(1, 26) = 1.99, MSE = 114.05, P = .17, η2 p = 0.07. The interaction between group × electrode site was not significant, F(2, 52) = 2.21, MSE = 3.94, P = .12, η2 p = 0.08.

Grand average novel-standard difference waves for patients (blue line) and controls (black line). The novel sounds elicited an N2 and a later novel-P3 component. There were no significant group differences for either the novel-N2 or -P3.
The novel-P3 was largest at Cz, F(2, 52) = 37.59, MSE = 6.81, p = .0001, η2 p = 0.59. Its amplitude was larger in patients, but the difference was not significant, F(1, 26) = 1.15, MSE = 136.65, P = .29, η2 p = 0.04. The interaction between group × electrode site was not significant, F(2, 52) =1.51, MSE = 7.63, P = .23, η2 p = 0.05.
Additional Analyses
Many studies measure the P3 in the “raw” ERP waveform and not a difference wave. In the present study, when this was done, the results were very similar. Group differences were not significant for the target-P3b, novel-P3, or N2.
In Figures 2 and 3, a later positivity peaking at about 500 ms is apparent in both the target and novel waveforms. While, this later positivity was larger for the suicidal group, the difference compared to the control group was not significant at Pz, where it was largest, for either the target, t(26) = 1.83, P = .07, or the novel stimulus, t(26) = 1.36, P = .18.
Some researchers hypothesize that suicidal patients are unable to sustain attention for long periods of time. The averaging of all trials across the task might thus have smeared group differences over time. Separate averages were, therefore, also computed over the first and second halves of the task. There was no significant group × task interaction for either the novel-P3, F(1, 26) = 0.39, MSE = 22.81, P = .54, η2 p = 0.01, or target-P3, F(1, 26) = 0.25, MSE = 16.85, P = .62, η2 p = 0.009.
Correlations
For the patients, there were significant correlations between the target-P3b and the RCADS subscales of Social Phobia (r = −0.71), Generalized Anxiety (r = −0.63), Total Internalizing (r = −0.56), and Total Anxiety (r = −0.59). There were no other significant correlations between the ERP components and the RCADS and SITBI scores for the patients or the controls.
Discussion
Active Attention
Accuracy of target detection was very high for both groups but was, nevertheless, significantly reduced in patients. Previous oddball studies with both adolescents 35 and adults with depression 36,37 and adults with suicidal behavior 25 have failed to find group differences in accuracy of target detection. The use of different tasks that vary in difficulty make generalization difficult. It is also possible that acute suicidal behavior in adolescents may have a more profound effect on performance.
In contrast to the behavioral results, there were no significant group differences in the amplitude of either the target-N2 or P3b suggesting intact controlled stimulus detection and classification. A failure to find group differences in the amplitude of the target-N2 and P3b has also been observed in auditory oddball studies with depressed adolescents. 35,38 Jandl et al 25 did observe a significant target P3b reduction in their adult suicidal group but only in the second half of the study. This was not the case in the present study. Neither the target-N2 nor P3b significantly declined in amplitude for either controls or patients. There was thus little evidence of a failure to sustain attention in the adolescent suicidal group.
Significant negative correlations were also observed for the patient group. Patients with reduced target-P3b amplitudes tended to score higher on measures of Social Phobia, Generalized Anxiety, Total Internalizing, and Total Anxiety. Although there are some inconsistencies, studies have shown reduced target-P3b amplitudes in patients with anxiety disorders, 39,40 which is in line with the correlation findings in the present study.
Passive Attention
Few ERP studies have examined passive attentional processing in individuals with suicidal behavior. A critical feature of passive attention is that it does not require the utilization of effortful, cognitive resources. While an inability to sustain attention may affect the active detection of targets, it should not have affected the passive detection of the novels. As expected, a large centrofrontal maximum P3 was elicited by the novel stimulus. This novel-P3 was slightly larger in the patient group, but the difference was not significant. This result did, however, follow the same trend as Tavakoli et al 27 who noted a larger P3a to the same novel stimuli in their patient group when the auditory stimuli were to be ignored. In the present study, while the novel stimuli were irrelevant to the target detection task, they could not, in fact, be ignored. Upon their presentation, a decision had to be made that the novel stimuli were not targets, and as such, a response had to be withheld. Therefore, many of the processes involved in the detection and classification of targets would also be implicated for the novel stimuli. The large positivity elicited by the novel stimuli likely reflects an overlap and summation of the novel-P3 and target-P3b. 41,42 The processing involved in the detection of each stimulus are, however, not identical. The positivity that was elicited by the novel stimulus in the 3-stimulus paradigm did have a more anterior scalp distribution than the parietal target-P3b. The novel-P3 may thus reflect processing of both an initial passive attention capture process and a later active, controlled stimulus classification process. Confirmation of these processes would, however, require spatial-temporal analyses of the waveform, similar to those carried out by Spencer et al, 18 Dien et al, 20 and Debener et al 19 to decompose the novel-P3 and P3b contributions. These procedures would, however, require many more electrode placements than that used in the present study.
The frontocentral novel-N2 was also somewhat larger in the patient group compared with controls. Again, the difference was not significant, suggesting that general mismatch detection of the irrelevant novel stimuli is not affected in the suicidal group.
A later positivity occurring from 500 to 600 ms was apparent for both the target and novel. It was particularly large for the patient group, although again the difference was not significant. Few studies employing the active oddball paradigm have shown this late positivity, although results have not been reported. 35,43 The nature and purpose of this processing is unclear. It could reflect additional, but needless, post-response processing on the decision that has already been made.
Limitations
The extent to which comorbid depression and/or anxiety could influence these results has been disputed. In adolescence, no significant differences have been observed in the amplitude of the target-N2 or P3b in depressed versus control groups. 35,38 In children with depression, Lepisto et al 44 found increased P3a amplitudes compared with healthy controls. Furthermore, decreased P3b amplitudes in adult patients with anxiety disorders has been reported in some studies, 39,40 whereas an increased frontal P3 amplitude has been found to be associated with anxiety disorders in one study. 45 Future studies should examine the differential effects of depression, anxiety, and suicide on these results by including additional participant groups with depression and/or anxiety without suicidal behavior. Nevertheless, depression and anxiety are highly common in adolescents with suicidal behavior and as such, the results obtained from the present study are more likely representative of a suicidal population than results from a pure suicidal group with no other comorbidities.
Medication is another possible confounding factor. Ideally, a nonmedicated sample should also be studied. This may not, however, be ethically or morally justifiable in those seeking emergency intervention for acute risk of suicide and deemed to require pharmacological treatment. Most of our patient sample was treated with SSRIs and/or atypical antipsychotics. It is possible that these medications may influence the ERP findings. Still, Rydkjær et al 46 found no significant differences in the amplitude of the novel-P3 among those with and without SSRI use and antipsychotic use. The results of studies examining the effects of SSRIs on the P3b are mixed. Some studies have shown no significant effects of SSRIs on the P3b, 47 -49 while others have shown a decreased P3b amplitude. 50
It is possible that the relatively small sample size did not provide enough statistical power to reveal true group differences. The group differences were, nevertheless, small-to-moderate. To achieve statistical significance with these novel-P3 group differences would require a group size of 155 participants assuming a power of 0.8. Within-group variance was particularly large for the suicidal group indicating considerable individual differences. Wide variance within a suicidal group has also been observed on a similar task by Jandl et al. 25 Unfortunately, recruiting a sample size this large of acutely suicidal adolescent inpatients would require a considerable amount of time and in the end, may not be of practical significance. It is unlikely that clinical decisions would be altered based on group differences this small even if these differences were statistically significant. Still, the sample size in the present study was similar, or larger, than that used in other ERP studies of suicide attempters. 23 -25,27
Implications
Research shows that one-third of adolescents with suicidal ideation will transition to a suicide attempt within 1 year. 30 ERPs provide a promising tool to investigate cognitive deficits independent of subjective self-report measures. This is the first study to explore both passive and controlled aspects of attention using ERPs in adolescents with acute suicidal behavior. Although there were no significant ERP group differences, this is an important step in identifying objective markers of suicide risk among adolescents. Future research examining various cognitive functions using ERPs could aid in improving the clinical detection and risk profile of high-risk adolescents to ultimately reduce the alarmingly high suicide rates.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Financial support for this research was provided by funds from the Psychiatry Associates at the Children’s Hospital of Eastern Ontario to AB and an operational grant (8284) to KC by the Natural Sciences and Engineering Research Council of Canada (NSERC).