
Abstract
Continuous electroencephalography (cEEG) and quantitative analysis of EEG (qEEG) are used in various circumstances such as detecting seizures, identifying acute or delayed cerebral ischemia, monitoring sedative therapy, or assessing prognosis. The authors report 2 cases: (1) Case #1 was a patient with unilateral cerebral edema and uncal herniation with asymmetric cEEG and qEEG changes detected an hour before clinical examination changes were noted and (2) Case #2 was a patient with diffuse cerebral edema and trans-tentorial herniation with symmetric cEEG and qEEG changes detected an hour before clinical examination changes were noted. These cases demonstrate the ability of cEEG and qEEG in early detection of different types of cerebral herniation. qEEG can be utilized by intensive care unit (ICU) staff not trained in EEG interpretation as a surveillance method to detect cerebral herniation, which may provide an opportunity for early intervention in high-risk patients.
Introduction
cEEG and qEEG are widely used in hospitalized patients, especially in the critically ill populations. Indications of cEEG and qEEG are not restricted to detecting seizures. Other indications were proposed such as identification of acute ischemia intraoperatively, delayed ischemia caused by subarachnoid hemorrhage, monitoring for sedation and high-dose suppressive therapy, assessment of severity of encephalopathy, and prognosis. 1 Here, we report 2 cases where cEEG and qEEG detected early signs of cerebral herniation and possibly differentiated different types of herniation.
Case Presentation
Case #1
A 60-year-old woman with history of end-stage renal disease underwent deceased donor renal transplant and was started on immunosuppression (tacrolimus, mycophenolate mofetil, and prednisone). On postoperative day 5, she developed altered mental status and fever. Computed tomography (CT) of the chest, abdomen, and pelvis showed evidence of pneumonia. She was started on Piperacillin/Tazocin and levofloxacin. Micafungin was later added due to concern regarding urinary tract infection with Candida. The hospital course was complicated by rising creatinine, lactate, and troponin suggestive of shock. Immunosuppressants were discontinued. She developed liver failure with elevated aspartate aminotransferase (2600 IU/L equivalent to 43.33 µkat/L) and alanine transaminases (3000 IU/L equivalent to 50 µkat/L). Antibiotics were broadened to Piperacillin/Tazobactam, vancomycin, acyclovir, and micafungin. The patient's mental status continued to worsen, which resulted in intubation and consideration for liver transplant by postoperative day 10. The patient's platelet level had dropped to 33 K/µL (equivalent to 33 × 10⁹/L), and laboratory results showed coagulopathy (prothrombin time 20.6 s, partial thromboplastin time 28.3 s, international normalized ratio 1.9). CT of the head was unremarkable. cEEG showed diffuse background slowing and disorganization (Figure 1A). Patient was started on Argatroban due to concerns for heparin-induced thrombocytopenia. On postoperative day 13, patient was examined at 15:01 off sedation and was able to follow commands such as “squeeze fingers”, “wiggle toes,” and “move all extremities.” Both pupils were reactive to light. Spontaneous antigravity movement was noted in all four extremities. The next routine physical examination was conducted at 17:00. Patient was found unresponsive to verbal, tactile, and noxious stimuli. Pupillary, oculocephalic, corneal, gag, and cough reflexes were all absent. Urgent CT head was obtained at 17:37 and showed large right hemispheric subdural hematoma (SDH) with midline shift and uncal herniation (Figure 1D). Retrospectively, cEEG started to show changes at approximately 15:50, with abrupt-onset voltage attenuation to burst suppression over the right hemisphere (Figure 1B) followed by generalized background suppression within 20 min (Figure 1C). qEEG showed asymmetric increase in the power of low-frequency activity on fast Fourier transform (FFT) spectrogram and asymmetric increase in suppression ratio (right side worse than left) (Figure 1, upper panel).
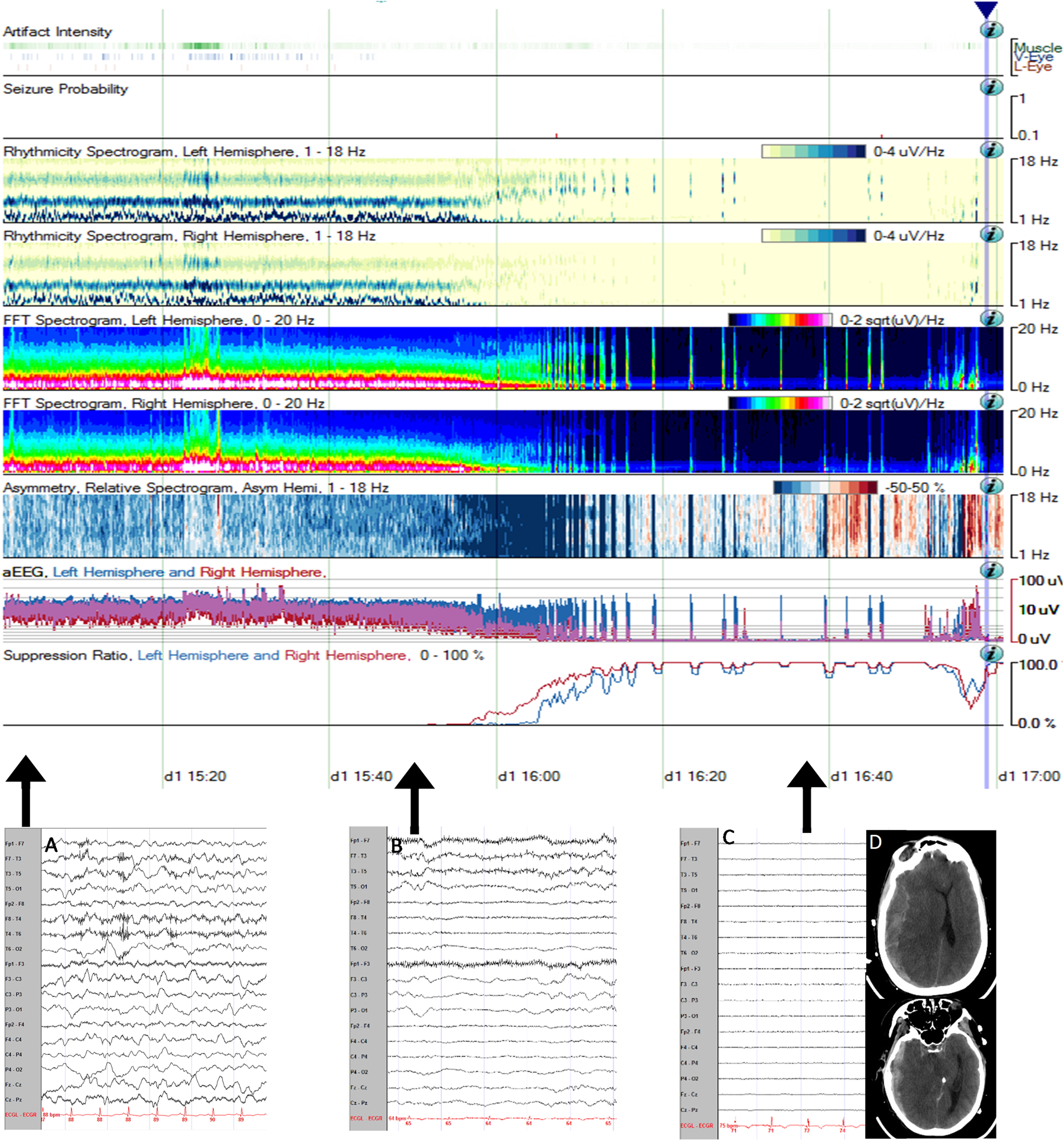
Upper panel: qEEG shows asymmetric increase in the power of low-frequency activity on FFT spectrogram and asymmetric increase in suppression ratio (right side worse than left). Lower panel: cEEG (low-frequency filter 1 Hz, high-frequency filter 70 Hz, sensitivity 10 µV/mm), bipolar longitudinal montage. Left epoch (A) shows baseline diffuse background slowing and disorganization. Middle epoch (B) shows abrupt-onset voltage attenuation followed by burst suppression over the right hemisphere, and subsequent generalized background suppression within 20 min as demonstrated on the right epoch (C). CT Head without contrast (D) shows large right hemispheric SDH with midline shift and uncal herniation.
Case #2
A 73-year-old woman with history of chronic lymphoid leukemia and idiopathic thrombocytopenic purpura developed petechial rash, gingival hemorrhage, and hematuria. A few days later, she reported headache followed by altered mental status. CT head showed increased density along the falx cerebri and right tentorium, measuring 3 mm in thickness and highly suspicious for a small SDH, as well as a 5 mm thick right lateral convexity SDH, with a 3 mm left midline shift. Initial cEEG showed attenuated activity over the right hemisphere and diffuse background slowing (Figure 2A). Laboratory results were remarkable for anemia and severe thrombocytopenia: hemoglobin = 7.2 g/dL (equivalent to 4.47 mmol/L) and platelets = 2 K/µL (equivalent to 2 × 10⁹/L). The patient was subsequently intubated for altered mental status. She received 2 packs of platelets and prednisone 80 mg, and intravenous immunoglobulin. A baseline examination showed reactive pupils bilaterally and all 4 extremities symmetrically withdrew to noxious stimuli. On hospital day 7, routine examination was conducted at 05:40 and was deemed at baseline. At 06:55, cEEG demonstrated abrupt-onset diffuse background attenuation (Figure 2B) progressing to suppression (Figure 2C). qEEG showed symmetric increase in power of low-frequency activity on FFT and symmetric increase in suppression ratio (Figure 2, upper panel). The primary team examined the patient at approximately 08:00 after being notified about the above EEG change. The patient was found to be unresponsive to verbal, tactile, and noxious stimuli. Pupils were fixed and dilated bilaterally. No motor responses were elicited with noxious stimuli. A CT head obtained at 12:02 showed worsening SDH, diffuse cerebral edema, and multifocal infarcts in the left occipital, right temporal, and bifrontal regions (Figure 2D).
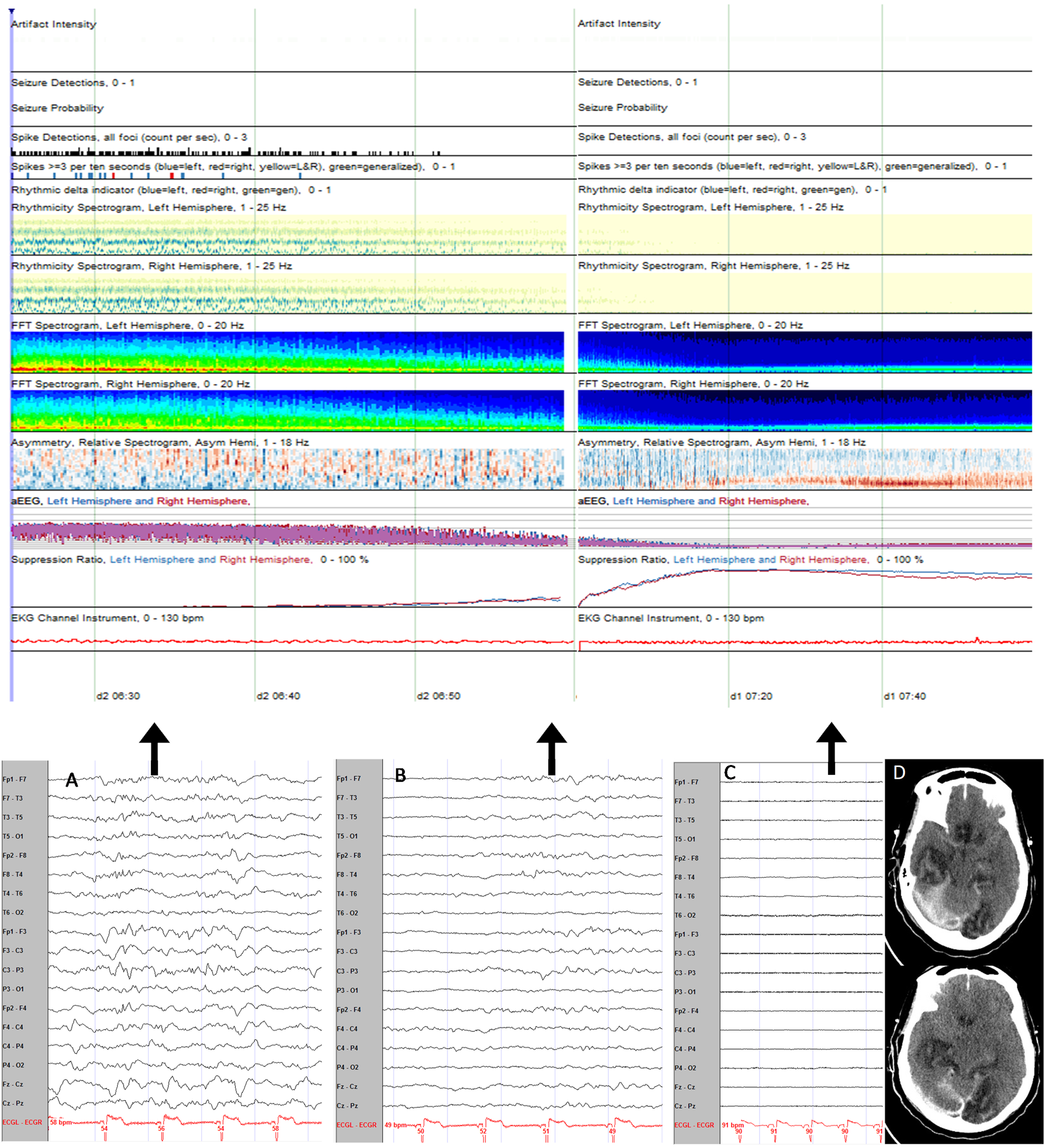
Upper panel: qEEG shows symmetric increase in power of low-frequency activity on FFT spectrogram and symmetric increase in suppression ratio. Lower panel: cEEG (low-frequency filter 1 Hz, high-frequency filter 70 Hz, sensitivity 10 µV/mm), bipolar longitudinal montage. Left epoch (A) shows attenuated activity over the right hemisphere and diffuse background slowing. Middle epoch (B) shows transition into diffuse background attenuation and eventually suppression (C). CT head without contrast (D) shows worsening SDH, diffuse cerebral edema, and multifocal infarcts in the left occipital, right temporal, and bifrontal regions.
Discussion
As part of the consensus statement by the International Multidisciplinary Consensus Conference on multimodality monitoring in neurocritical care, cEEG is strongly recommended in all patients with unexplained and persistent altered consciousness and suspected seizures, and is suggested for detecting delayed cerebral ischemia. 2 cEEG has also proved its importance as a noninvasive method for detecting delayed cerebral ischemia in the setting of subarachnoid hemorrhage by various means such as focal slowing, decreased alpha variability, and decreased alpha/delta ratio.3,4 Endovascular intervention within a 2 h window of vasospasm secondary to aneurysmal subarachnoid hemorrhage (aSAH) was associated with better outcome. 5 This demonstrates the importance of detecting early changes and provides an opportunity for early intervention where changes may be reversible.
Ischemia from vasospasm or intraparenchymal hemorrhage may ultimately lead to increased intracranial pressure (ICP). Studies have shown a clear relation between ICP changes and EEG activities.6,7 This relation is thought to be attributed to the neurovascular coupling mechanism. Indeed, cerebral blood flow has been found to be altered in epileptic activity and in cortical spreading depression. Several animal studies8,9 and reports in humans 10 have shown that aSAH and ischemic stroke may lead to increased cortical spreading depression and subsequently decreased cerebral blood flow (CBF). Interestingly, 1 study showed a Granger causality from the EEG activity to high ICP in 37.88% of the time suggesting that EEG may predict and measure ICP in a noninvasive manner. 6 Further studies showed that patients with EEG burst suppression had transient increase in ICP after a burst and this had a significant correlation with the duration of the burst. This has been attributed to a sudden increment in metabolic demand caused by the burst resulting in increased supply (ie, cerebral blood flow), and ultimately resulting in rise in ICP. 7
Acute intracranial hypertension is a medical emergency and may lead to irreversible damage and herniation if not managed early. 11 Newey et al 12 reported a patient with focal cerebral edema detected on cEEG 24 h prior to herniation. Notably, the cEEG showed rapid development of background EEG suppression 6 h prior to clinical signs of herniation. Fantaneanu et al 13 reported another case with diffuse cerebral edema and herniation, where cEEG revealed loss of cerebral activity 1.5 h before clinical change. All these demonstrate the utility of cEEG in detecting early signs of high ICP and herniation. In both of our cases, cEEG and qEEG changes were detected more than 1 h before clinical examination findings. In Case #1, asymmetric increment in low-frequency power with subsequent diffuse suppression on qEEG was consistent with ipsilateral cerebral edema and uncal herniation. However, Case #2 showed abrupt onset of symmetric increment in low-frequency power and suppression ratio on qEEG. This correlated with diffuse cerebral edema and trans-tentorial herniation. In addition to the previously published papers, our cases demonstrate that combining cEEG with qEEG may help detect early cerebral edema and herniation, and may potentially help differentiate the type of herniation.
We propose training ICU staff to recognize the illustrated qEEG patterns demonstrated above, which may facilitate implementing early recognition and thereby early intervention. The recognition of these qEEG patterns can be learned without the need to be trained in reading raw EEG data and serves as a rapid noninvasive method of surveillance in high-risk patients.
Conclusion
These 2 cases demonstrate how qEEG may be used by ICU staff not trained in EEG interpretation to identify patients with evolving cerebral herniation in real time. Recognizing the unique pattern of progressive increment of low-frequency power, suppression ratio, and degree of symmetry of the aforementioned parameters may aid in early detection of herniation, differentiation of herniation types, and possibly providing early intervention.
Footnotes
Author Contributions
FA and LL contributed to the conception and design of the article. FA and LL drafted the manuscript and prepared the figures. All authors revised the manuscript and assisted in data collection for important intellectual content. All authors approved the final version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.