
Abstract
Introduction. In clinical practice, it is difficult to define the prognosis of patients with acute encephalopathy; a syndrome characterized by cognitive dysfunction and altered sensorium. Discharges with triphasic morphology (DTM) are an electroencephalographic pattern that might be useful to establish the risk of death. The aim of this study was to define the prognostic value of DTM regarding mortality in patients with acute encephalopathy. Methods. We conducted an observational retrospective cohort study including patients with acute encephalopathy with and without DTM paired by age and gender in a 1:2 ratio. We calculated the odds ratio (OR) to determine the association between DTM and mortality. In addition, we calculated sensibility, specificity, and predictive values. Results. We included 72 patients, 24 with DTM and 48 without DTM. Mortality was higher in patients with DTM (41.6% vs 14.5%, P = .01). Factors associated with a higher risk of death were DTM (OR = 4.1, 95% confidence interval [CI] 1.3-13, P = .01) and sequential organ failure assessment score (OR = 1.3, 95% CI 1.04-1.67, P = .02). A higher Glasgow coma scale score was associated with a lower risk of death (OR = 0.65, 95% CI 0.51-0.83, P = .001). The sensibility and specificity of DTM were 59% and 75%, respectively. Positive and negative likelihood ratios were 2.36 and 0.55. Discussion. Our results revealed high mortality in patients with acute encephalopathy and DTM. This electroencephalographic pattern was associated with 4 times higher risk of death. However, its usefulness for predicting death was limited.
Introduction
Acute encephalopathy is a clinical syndrome characterized by variable degrees of cognitive dysfunction and/or altered sensorium occurring in the context of systemic or central nervous system insults. 1 Estimation of the risk of death in acute encephalopathy allows physicians to define appropriate diagnostic and therapeutic strategies. 2 However, establishing the prognosis of this syndrome is difficult because of the heterogeneity of factors involved.
Scores such as the Acute Physiology and Chronic Health Evaluation II 3 and the Sequential Organ Failure Assessment (SOFA) 4 are employed in daily clinical practice to define the prognosis of in-hospital patients. Nevertheless, these tools require data from multiple physiologic and laboratory parameters obtained in at least 24 h. It is desirable to dispose of easier and earlier prognostic markers.
Discharges with triphasic morphology (DTM) (Figure 1), former triphasic waves, are an electroencephalographic pattern associated with many medical conditions, 5 although their clinical significance is still uncertain, they might be useful as a prognostic marker.
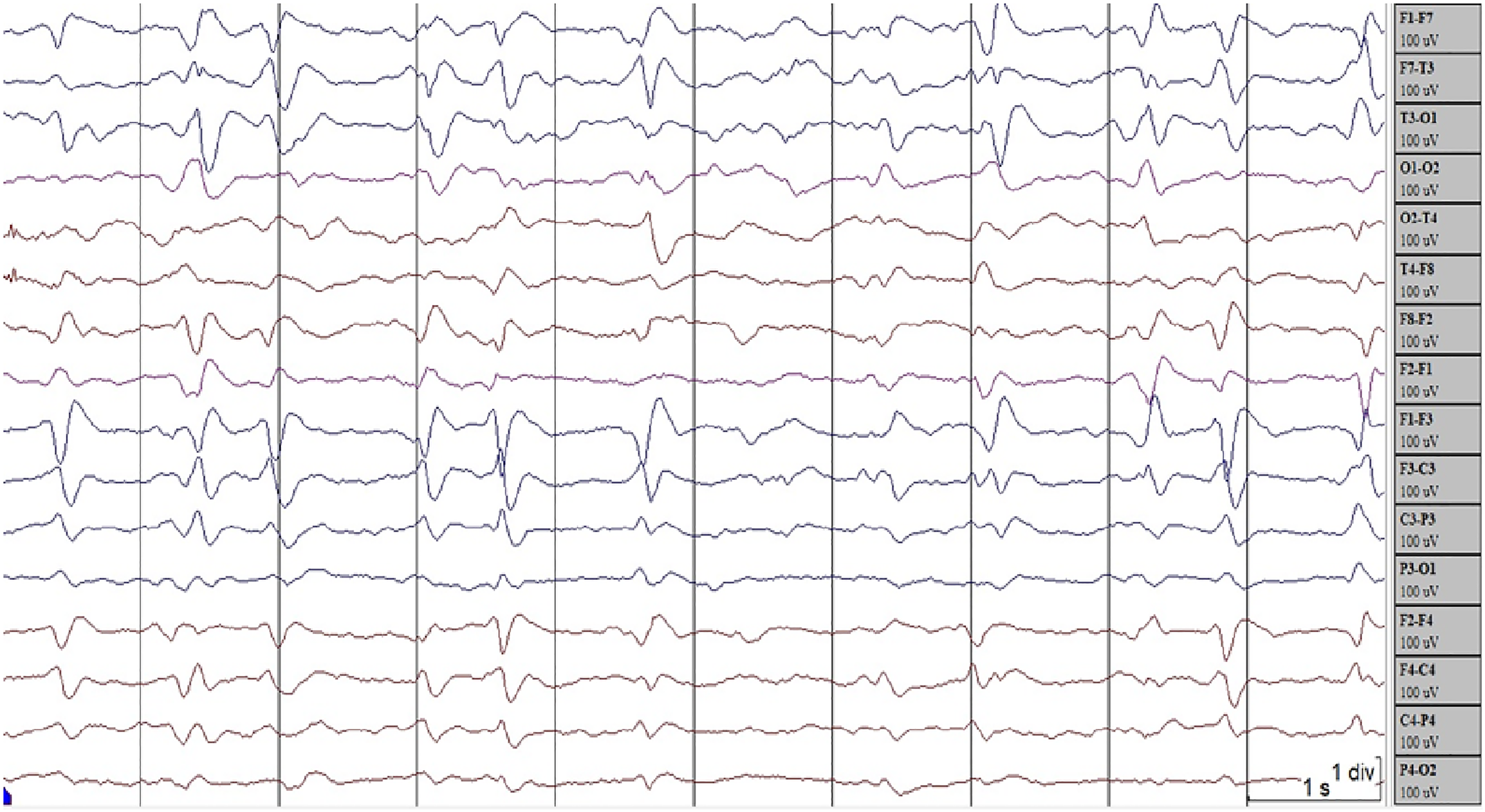
Electroencephalogram (EEG) shows discharges of triphasic morphology predominantly in the left frontal region.
The aim of this study was to define the prognostic value of DTM as a marker of the risk of death in patients with acute encephalopathy.
Methods
We conducted an observational retrospective cohort study including patients older than 21 years, hospitalized in Sanatorio de la Trinidad Mitre between January 2016 and July 2020 with a diagnosis of acute encephalopathy and studied with an electroencephalogram (EEG) during the course of their disease.
We defined acute encephalopathy based on the Diagnostic and Statistical Manual of Mental Disorders fifth edition of the American Psychiatric Association, 6 as a disturbance in attention and/or awareness associated with dysfunction in another cognitive domain, which develops in a short period of time and it is not better explained by a preexisting neurocognitive disorder.
We selected study subjects with a clinical diagnosis of acute encephalopathy and compatible EEG through a dual search in the general database of the Department of Neurology and the EEG-reports database of the Department of Clinical Neurophysiology. Then, we evaluated the clinical records of each patient and collected data on personal medical history, diagnosis, clinical status, and complementary studies. We excluded patients who did not meet the inclusion criteria or with incomplete data in their medical records.
We obtained electroencephalographic data from EEG tracings and reports. All EEG studies were performed using ATI Vertex® or Bioscience Stellate® digital equipment. Electroencephalographic signal was recorded using 8 to 20 channels with electrodes distributed according to the 10-20 international system. Monopolar and bipolar montages were used for analysis.
Three clinical neurophysiologists blinded to the EEG report and clinical information evaluated tracings and verified that they corresponded to the respective reports. In cases of discordance between the original report and the blinded evaluator, a third specialist solved the discrepancy.
We paired patients with and without DTM by sex and age, in a 1:2 ratio. DTM was defined according to the American Clinical Neurophysiology Society's Standardized Critical Care EEG Terminology, as complexes with either 2 or 3 phases, with each phase longer than the previous and the longer phase of higher amplitude, in a negative–positive–negative or positive–negative pattern. 7
To define the degree of organ dysfunction we calculated the SOFA score for each patient using clinical and laboratory parameters obtained within the 24 h of EEG performance. We recorded the length of hospital stay time and mortality in each group.
We estimated a sample size of 81 patients to find a 25% difference in mortality between both groups, with a 1:2 ratio, a 95% confidence interval (CI), and statistical power of 80%.
We performed statistical analysis in Epidat v4.2 software. We calculated percentages and absolute frequencies for qualitative variables and mean and standard deviation or median and interquartile range (IQR) for numerical variables. We used the Z test to define the association between qualitative variables and Student’s t-test and Mann–Whitney U test for numerical variables according to their distribution. We calculated the odds ratio (OR) to measure the association between DTM and in-hospital mortality. Then, we calculated sensitivity, specificity, predictive values, and likelihood ratios of DTM for predicting death during hospitalization. Analysis was performed using a 95% CI and a 5% alpha error.
The study was approved by the Institutional Research and Teaching Committee. All data was anonymized. Informed consent was waived due to the retrospective nature of the study.
Results
In a 56 months period, we identified 25 patients with an EEG report of DTM. We excluded 1 patient because of insufficient data on the medical records. Each of the remaining 24 patients were matched according to sex and age with 2 patients with acute encephalopathy without DTM (n = 48), resulting in 72 patients included in the study. Fifty-one (71%) females and 21 (29%) males.
Median age was 82 years (IQR: 76-88). Seventy-two percent (n = 52) had a history of arterial hypertension, half (n = 36) had previous cognitive impairment and 33% (n = 24) had oncologic disease history. The main cause of acute encephalopathy was toxic-metabolic disorders (n = 45, 62%), followed by systemic infection (n = 30, 41%) and structural lesions of the central nervous system (n = 15, 20%). In 22 patients (30.5%), encephalopathy was attributed to the coexistence of at least 2 disorders.
Median SOFA score was 3 points (IQR 2-4), median Glasgow coma scale (GCS) was 13 (IQR 10-14). Table 1 details the main clinical features and laboratory results.
Population Characteristics.
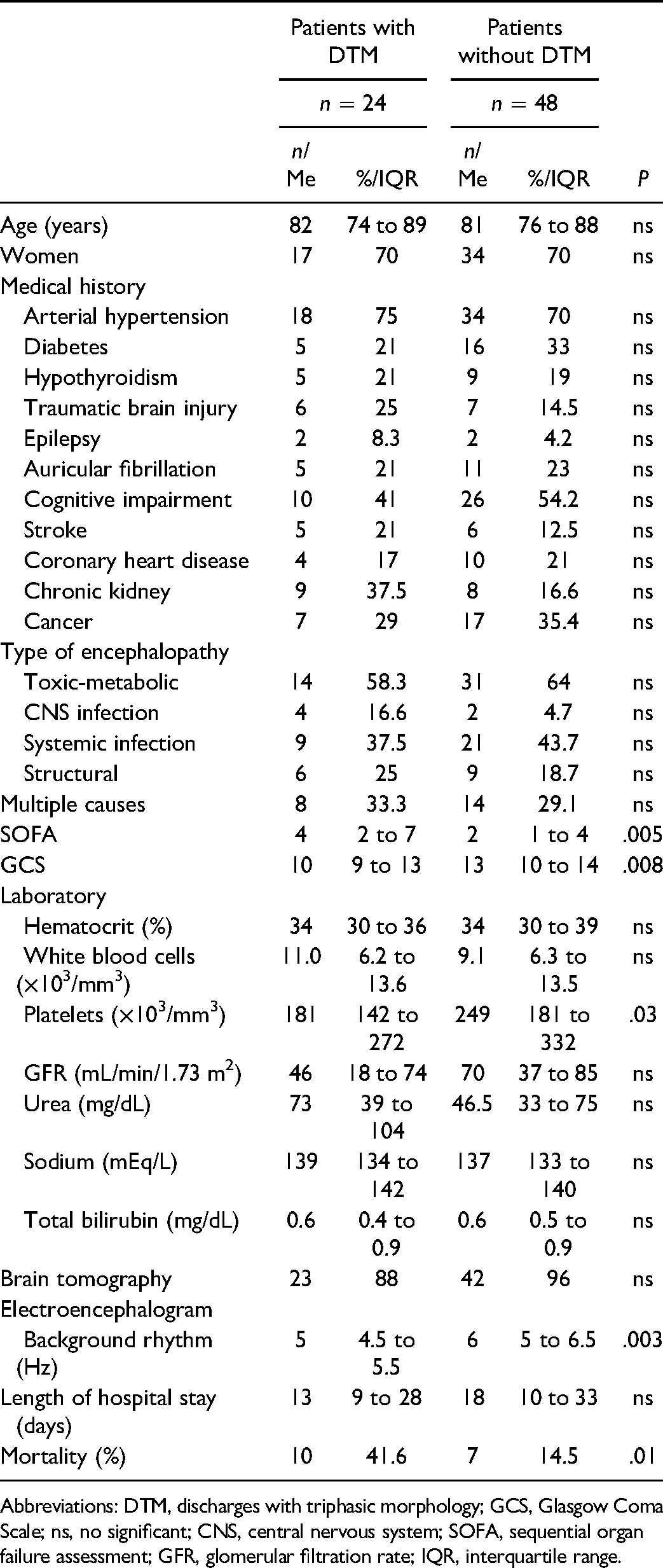
Abbreviations: DTM, discharges with triphasic morphology; GCS, Glasgow Coma Scale; ns, no significant; CNS, central nervous system; SOFA, sequential organ failure assessment; GFR, glomerular filtration rate; IQR, interquartile range.
We did not find any significant difference in personal medical history or type of encephalopathy between patients with and without DTM. Patients with DTM had higher scores of SOFA (4 vs 2, P = .005) and lower GCS (10 vs 13, P = .008).
There were no significant differences in laboratory values, except for platelet counts, which was lower in patients with DTM (181 vs 249 × 103/mm3). There were no significant differences in length of hospital stay between patients with and without DTM (13 vs 18, P = .44). Regarding electroencephalographic features, background activity was 5 Hz (IQR 4.5-5.5) in patients with DTM and 6 Hz (IQR 4.8-6.5) (P = .005) in patients without DTM. The median frequency of DTM was 2.5 Hz (IQR 2-2.5) and their localization was predominantly frontal in 50% (n = 12) of the cases. Ten patients (41.6%) had changes in amplitude or frequency of DTM with arousal or stimulation.
Overall study mortality was 23.6% (n = 17). The percentage of deceased was higher in patients with DTM (41.6% vs 14.5%, P = .01). Factors associated with a higher risk of death were DTM (OR = 4.1, 95% CI 1.3-13, P = .01) and a higher SOFA score (OR = 1.3, 95% CI 1.04-1.67, P = .02). Although a higher GCS score was associated with a lower risk of death (OR = .65, 95% CI 0.51-0.83, P = .001).
In our study, the sensitivity and specificity of DTM were 59% and 75%, respectively, with a positive predictive value of 42% and a predictive negative value of 85%. The positive likelihood ratio (LR+) was 2.36 and the negative likelihood ratio (LR−) was 0.55.
Discussion
In this study, overall mortality was superior to 20%; this cipher is in accordance with the expected mortality in patients with acute encephalopathy, which ranges between 25% and 33%. 8 The mortality in patients with DTM reached 41.6%, that is, 3 times higher than patients without DTM. The rate of death described in patients with DTM is variable; it usually oscillates between 19%9,10 and 29% 11 for all causes of encephalopathy, but can reach more than 50% in septic 12 or metabolic encephalopathy. 13
Regarding the population characteristics, in our study, the majority of patients with encephalopathy and DTM were women of advanced age. There is no clear explanation for why this electroencephalographic pattern does not appear in children or young adults, 14 but it might be linked with age-related neurostructural changes, as brain atrophy. 11 Our previous work (unpublished data) supports this theory.
In our study, the main causes of encephalopathy were toxic-metabolic disorders and systemic infections. There were no significant differences in preexisting medical conditions or the etiology of encephalopathy between both groups.
Our results revealed that DTM was vinculated with a 4-time higher risk of death. This finding is congruent with a previous report by Sutter et al 11 who found a high risk of death (OR 4.8) in patients with this electroencephalographic pattern from a cohort of 154 subjects with encephalopathy. It has been suggested that DTM represents cortical interneurons dysfunction in cortico-thalamic circuits, appearing in the context of toxic, metabolic, infectious, or structural disorders over a predisposed brain.9,14 A significant degree of systemic and/or encephalic alteration is probably needed to produce this cortico-thalamic dysfunction, independently of the cause of encephalopathy. This hypothesis is based on the fact that patients with DTM had higher SOFA scores, lower GCS scores, and slower EEG background rhythm than patients without DTM, suggesting a more severe illness and deeper alteration of consciousness. Furthermore, patients with DTM had lower platelet counts, a finding that suggests that subtle differences in each SOFA parameter might be associated with different mortality between groups.
The GCS and SOFA scores were significantly associated with a higher risk of death. Previously, Sutter and Kaplan 9 did not find significant differences in the risk of death of patients with and without DTM when they were paired by GCS and EEG background rhythm; this led them to suggest that DTM could be a less important factor than GCS in relation to mortality. Larger prospective studies are required to define the association between GCS, DTM and mortality.
Our study showed that there is some variation between the localization, frequency, and reactivity of DTM among patients with acute encephalopathy. The significance of these electroencephalographic features is still unknown and requires further investigation.
Regarding the utility of DTM for predicting death, we obtained low values of sensitivity, specificity, positive predictive value, and LR+. These results indicate that even DTM was associated with a significantly higher risk of death, their accuracy for predicting a fatal outcome was limited.
Limitations of this study include its retrospective design and the lower than expected number of patients included in our study; therefore, the statistical power was not enough to perform a multivariate analysis to define potential interactions between DTM, GCS, and SOFA score with mortality. The degree of reversibility of organ failure, usually estimated with serial SOFA measurements, was not evaluated in this study. Future studies should address the impact of this factor in the inhospital mortality in patients with DTM. Another limitation is the risk that the follow-up time would not be long enough to allow all outcomes to be recorded. However, the appropriate length of follow up in our study was expected to be short as death due to acute encephalopathy usually occurs during the first weeks of hospitalization. Our results revealed a median follow-up time (length of hospital stay) of 13 and 18 days for patients with and without DTM, with an upper interquartile limit of 28 and 30 days, respectively, which we believe should be appropriate to minimize the risk of underestimating the mortality rate.
The strengths include the long study period that allowed the identification of several cases of a relatively infrequent EEG pattern. The blind evaluation of the EEGs and the double mechanism of search and selection of patients that increases internal validity and reduces potential biases.
In conclusion, our results showed high mortality in patients with acute encephalopathy and DTM. This electroencephalographic pattern was associated with a 4 times higher risk of death, however, its usefulness in predicting mortality was limited.
Footnotes
Acknowledgments
The authors would like to thank Dr Galeno Rojas, Dr Victoria Aldinio, Dr Daniel Sacks, Dr Santiago Isa, Dr Victoria Camino, Dr Julian Fernandez Boccazzi, and Dr Jonathan Cubas for their valuable help in the acquisition of data.
Author Contributions
Xavier Merchán-del-Hierro, Gabriel Persi, Nahuel Pereira-de-Silva: conception or design of the study. Xavier Merchán-del-Hierro, Gabriel Persi, Nahuel Pereira-de-Silva, María C. Vulycher, Carla Chicco, Emilia Gatto: Acquisition, analysis, or interpretation of data. Xavier Merchán-del-Hierro, Nahuel Pereira de Silva drafted the manuscript. All authors critically revised the manuscript for important intellectual content, gave final approval and agree to be accountable for all aspects of the work in ensuring that questions relating to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval
Not applicable, because this article does not contain any studies with human or animal subjects.