
Abstract
The current study examined frontal alpha asymmetry (FAA) as a marker of approach- and avoidance-related prefrontal activity in participants with and without trauma exposure and posttraumatic stress disorder (PTSD). We investigated FAA in an inhibitory control paradigm (threatening vs nonthreatening cues) under 2 levels of cognitive demand (baseline: images constant within a block of trials; vs filtering: images varied randomly within a block) in 3 groups of participants: individuals with PTSD (n = 16), exposed to trauma but without PTSD (n = 14), and a control group without PTSD or trauma exposure (n = 15). Under low demand (baseline), both PTSD and trauma-exposed participants exhibited significantly greater relative left than right frontal brain activity (approach) to threatening than to nonthreatening images. Under high demand (filtering), no FAA differences were found between threatening and nonthreatening images, but PTSD participants revealed more relative left than right FAA, whereas trauma-exposed participants showed reduced left relative right FAA. In all conditions, healthy controls exhibited reduced left relative to right FAA and no differences between threatening and nonthreatening images. Study findings suggest dysfunctional prefrontal mechanisms of emotion regulation in PTSD, but adaptive prefrontal regulation in trauma-exposed individuals without PTSD.
Keywords
Posttraumatic stress disorder (PTSD) is a serious psychiatric disorder affecting 6.8% of the population in their lifetime. 1 PTSD is classified by 4 symptom clusters: reexperiencing of trauma-related memories, avoiding reminders of the trauma, negative alterations in mood and thought, and heightened arousal and reactivity. 2 Patients with PTSD experience severe difficulties in inhibitory control (eg, capacity to inhibit automatic responses or to suppress task-irrelevant memories and experiences)3-8 emerging from interference in 2 separate but related pathways 3 : (1) distressing trauma-related thoughts and memories distract traumatized individuals from current task focus and (2) preexisting deficits in executive control disadvantage those with PTSD from avoiding threatening stimuli or memories and modulating physiological arousal. Deficits in inhibitory control in PTSD have been traced in part to dysfunction in the prefrontal cortex (PFC). 9 Yet little is known about the prefrontal processes linking cognitive deficits to PTSD symptomatology.
Neural Correlates of Attentional Control in PTSD
Disturbances in attentional control networks of individuals with PTSD are thought to impact various forms of cognitive control, including inhibitory control. 10 The basolateral (BLA) complex of the amygdala codes the valence of environmental cues as positive or negative.11-14 Top-down control of BLA from PFC modulates the strength of an animal's behavioral approach to rewarding (positive) cues 15 or avoidance of threatening (negative) cues.16,17 Healthy individuals employ attentional PFC control of valence information to discern safety from danger.18,19 But these attentional control mechanisms have been shown to be dysregulated in PTSD,20,21 thereby disrupting normative approach and avoidance behaviors.
Three distinct stages of altered attentional control to threatening stimuli have been identified in PTSD: (1) detection and approach toward trauma-related stimuli (attentional facilitation); (2) difficulty disengaging from threatening stimuli at the expense of task performance (attentional interference)22,23; and (3) reorienting of attention from threatening stimuli (attentional avoidance). 24 Threat detection and approach have been identified with early, automatic stages of stimulus processing and associated with the enhanced speed and accuracy of participants with PTSD in responding to trauma-related stimuli.24-27 By contrast, avoidance is evident during later stages of attentional processing, 24 has been observed equally in tasks employing threat-related 28 or neutral stimuli, 29 and increases with the severity of PTSD symptoms. 10 In the context of an inhibitory control task, we used frontal alpha asymmetry (FAA) to investigate PFC activity during attentional processing in individuals with and without trauma exposure and individuals with PTSD.
Frontal Alpha Asymmetry
FAA provides a quantitative index of approach-oriented versus avoidance-oriented PFC activity. 30 The measure focuses on hemispheric imbalance in alpha band (8-13 Hz) power across frontal regions of scalp and rests on the widely accepted assumption that alpha band power is inversely related to brain activity. 31 A common approach is the calculation of an asymmetry index or difference score that indicates the relative activity of the right and left hemispheres, with zero representing equal contributions from each hemisphere. 32 Higher scores (FAA > 0) represent greater left than right hemispheric activity; scores lower than zero represent lower left than right hemispheric activity. Conceptual models 33 suggest that FAA reflects the hemispherically-divided systems of motivation and affect, with greater left relative to right frontal brain activity (F > 0) indicating approach motivations and positive affect (eg, appetite, sexual desire, anger, and aggression) and reduced left relative to right activity (FAA < 0) indicating avoidant motivations and negative affect (eg, fear, panic, activation of the flight response, and withdrawal from a stimulus). From this perspective, FAA may serve as a neurophysiological correlate of psychopathology, mapping onto the specific disturbances in affective and motivational systems of psychiatric disorders. Indeed, extant research suggests a link between reduced left versus right FAA to increased symptoms of both depression and anxiety.34-42
Research probing FAA in PTSD remains limited. Moreover, the majority of studies have considered only resting-state FAA in PTSD, which is thought to reflect trait-level differences. 43 This approach is problematic as PTSD potentially engages a mixture of both disrupted approach (hypervigilance, heightened aggression) and avoidance (anxiety, dysphoria) networks. Instead, it may prove more fruitful for purposes of characterizing tendencies of approach versus avoidance in PTSD to focus on state-dependent contexts (social interactions and cognitive challenges). In fact, systematic review 44 of trait-level and state-dependent data confirms the predictive power of state-dependent over trait-level FAA in discriminating traumatic stress pathology. Most recently, a 3-way comparison of individuals with PTSD, trauma-exposed individuals without pathology and individuals without trauma exposure identified a potential FAA marker of resilience, namely, significantly greater left relative to right frontal brain activation in the asymptomatic, trauma-exposed group than the PTSD and control groups during a negative mood state induction. 45
Present Study
Despite the growing evidence for a link between state-dependent FAA and PTSD, no research currently exists examining FAA in PTSD during attentional and cognitive tasks. The aim of the current study was to probe electrophysiological responses to threatening and nonthreatening stimuli during an inhibitory control task in individuals with PTSD, individuals with trauma exposure but no PTSD, and healthy individuals without trauma exposure using FAA. The current study aimed to extend our knowledge regarding the role of FAA in PTSD by investigating FAA in participants engaged in a threat-cued inhibitory control paradigm, a modification of the traditional flanker conflict task, 46 where we varied demand for inhibitory control processes from relatively low (baseline task: cues held constant) or relatively high (filtering task: cues varying randomly). We examined FAA for 200 ms from the onset of a threatening or nonthreatening face or scene, dividing the alpha band (8-13 Hz) into lower and upper sub-bands. Analysis of stimulus-elicited FAA within a 0 to 200-ms time window has been shown previously to reveal early and automatic processes of inhibition.47-49 Low alpha (8-10 Hz) has been found to reflect diffuse nontask-related cognitive processes, such as anticipation or attention,50-52 whereas upper alpha (10-13 Hz) appears implicated in task-related cognitive processes.53-55 To identify potential FAA biomarkers for posttrauma pathology and resilience, we compared FAA in a sample grouped by level of trauma exposure and symptomatology: individuals diagnosed with PTSD, a group exposed to trauma but asymptomatic, and a control group without trauma exposure or trauma-related pathology. We focused our analyses on group differences in approach-oriented versus avoidance-oriented brain states (operationalized as FAA) to threatening cues during early stimulus processing. We hypothesized that FAA would differentiate those with versus without PTSD. Because the examination of state-dependent FAA in PTSD samples to date has only employed a much longer duration of emotion provocation (2 min) and has not included a concurrent cognitive task, 45 we refrained from making a directional hypothesis.
Method
Participants
Forty-five participants were recruited from printed flyers and online postings. Eligibility requirements included being between the ages of 18 to 65 and having 20/20 vision. Exclusion criteria included the presence of a past or current substance use disorder, major depressive disorder, suicidality, and current or history of psychosis or bipolar disorder. During the screening, the nature of the procedures was explained fully, and informed consent was obtained from each participant; the Institutional Review Board of The City College of New York approved the protocol.
Three groups were formed: 1). PTSD (n = 16, 8 males, mean age = 33), participants who met full Diagnostic and Statistical Manual of Mental Disorders Fourth Edition Text Revision (DSM-IV-TR) 56 criteria for PTSD, or subthreshold criteria of a minimum Clinician-Administered PTSD Scale (CAPS) score of 20 and symptoms in each of the 3 clusters (ie, intrusive recollections, avoidance and numbing, hyperarousal). 57 Trauma-Exposed Healthy Controls (TEHC; n = 14, 7 males, mean age = 35), participants without PTSD and having no Axis I diagnoses, but who experienced a traumatic event that met Criterion A for PTSD; and 3). No Trauma Healthy Controls (NTHC; n = 15, 10 males, mean age = 34), participants without PTSD, an Axis I diagnosis, or Criterion A trauma exposure.
Measures
To assess for exclusion criteria (past or current substance use disorder, major depressive disorder, bipolar disorder, or psychosis), the Structured Clinical Interview for DSM-IV 58 and Beck Depression Inventory®-II 59 were administered. To assess lifetime exposure to a potentially traumatic event and PTSD diagnosis, participants were administered the Life Events Checklist 60 and the CAPS for DSM-IV. 61 Both measures define a traumatic event as directly experiencing or witnessing a Criterion A traumatic event as defined by the DSM-IV 61 (eg, sexual abuse, physical abuse, combat, etc). Endorsement of at least 1 traumatic event classified a participant as “trauma-exposed.”
Stimulus, Apparatus, and Procedure
Each participant completed 24 blocks of experimental trials (ie, 8 tasks × 3 repetitions), and 1 or more blocks of practice trials of a temporal flanker paradigm. 62 The study was carried out in an electrically and acoustically shielded Industrial Acoustics Company (New York) chamber at the City College of New York. Stimuli were created in Presentation (Neurobehavioral Systems, Berkeley) on a Dimension 5150 Dell desktop computer and were presented to participants on a 17-inch Dell Model P1130 RGB computer monitor with a refresh rate of 75 Hz. Building upon the traditional flanker conflict task, 46 our modified version temporally distinguishes distractor from target, affording separate neurophysiological measurement of distractor stimuli. 62 Each of the 8 tasks in the paradigm comprised a block of 80 trials, which lasted approximately 3 min. Participants completed a total of 1920 trials (8 tasks × 3 repetitions × 80 trials). As shown in Figure 1, each trial consisted of a fixation square (0.67°) followed by 3 stimulus displays presented sequentially: (1) First Flanker, (2) Target, and (3) Second Flanker. Each display appeared for 150 ms separated by an interstimulus interval varying between 153 ms and 390 ms in random distribution. The first and second flankers were identical on each trial: a vertical line, a horizontal line or a cross. Each target was a vertical or horizontal line superimposed on an image, either a grayscale threatening (ie, fearful) or nonthreatening face from the NimStim set 63 or a colored threatening or nonthreatening picture from the International Affective Picture System (IAPS). 64 Line stimuli, subtending a visual angle of 0.57°, appeared in gray on a black background; face and IAPS stimuli subtended 9.93° (V) × 7.13° (H) and 10.85° (V) × 9.74° (H) of a visual angle, respectively.
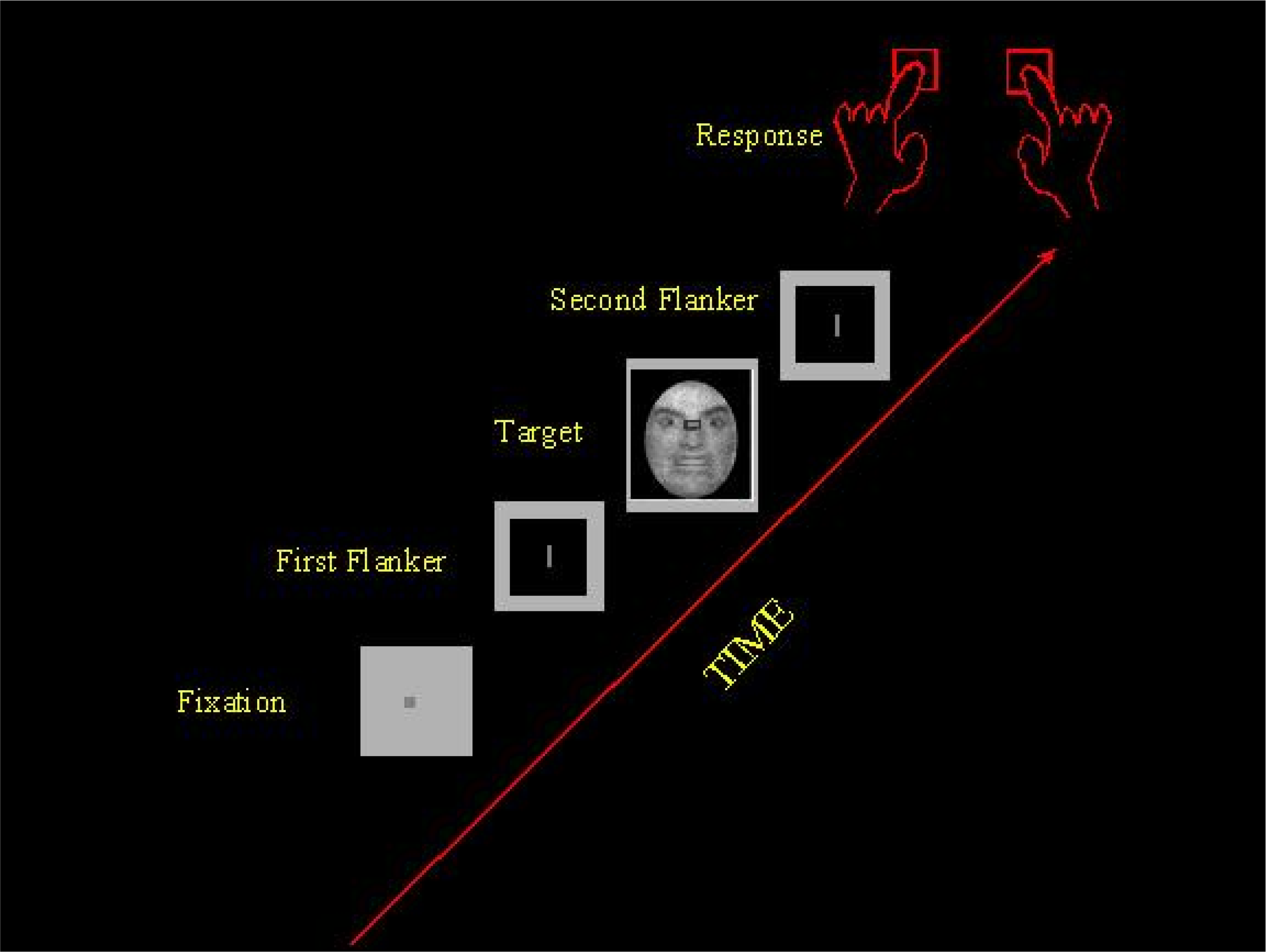
Sequence of displays in the temporal flanker task.
On each trial of each task participants were asked to respond by key press as quickly and accurately as possible to the orientation of the target line, ignoring the flanker lines and the surrounding image. The duration of stimuli was 1265 ms on average within a trial that lasted approximately 3665 ms. Assignment of line orientation to response keys was counterbalanced across participants. The 8 tasks were divided into 4 baseline tasks (distractor constant) and 4 filtering tasks (distractor random). 65 In each baseline task, distractors (flankers and images) were held constant across the block of trials: Two crosses always flanked the target. For each participant, a single face or IAPS image appeared on each of the baseline trials in a block, 1 of 8 images drawn from 1 of 4 stimulus sets–threatening faces, nonthreatening faces, threatening IAPS, nonthreatening IAPS–creating 4 different baseline tasks. The face stimulus sets comprised an equal number of male and female images. The image selection from each stimulus set was balanced across participants. Both faces and IAPS images were chosen to ascertain if different displays of the emotions of threat and nonthreat would yield divergent responses among participants. Baseline tasks performed below 80% accuracy were repeated immediately. On each trial of each filtering task, the distractor was drawn randomly from a pool of 8 images. During each block of filtering trials, all 8 images from 1 of the 4 sets (threatening faces, nonthreatening faces, threatening IAPS, nonthreatening IAPS) appeared randomly an equal number of times with the target line, creating 4 different filtering tasks. Each of the 8 tasks (4 baselines, 4 filterings) was performed as a set (task order balanced across participants); each set of 8 tasks was repeated 3 times in a session, creating 24 blocks of experimental trials. Participants were given short breaks throughout testing. The entire experiment, including electroencephalogram (EEG) preparation, lasted approximately 3 hours.
Data Recording and Analysis
Continuous recordings of the EEG were collected at a sampling rate of 512 Hz using a BioSemi Active-Two system in a high-density (160 electrodes) montage arranged in an elastic cap. Blinks and other eye movements were monitored by electrooculogram from 2 electrode montages, 1 on the infra- and supra-orbital ridges of the right eye (VEOG), the other on the outer canthi of each eye (HEOG). Trials containing mastoid activity exceeding 100 μV were rejected. Trials contaminated by blinks, eye movements, or other movement artifacts were defined as z-values on the VEOG, HEOG, and lowermost scalp channels exceeding 4.5 in a frequency band between 1 and 140 Hz; artifact trials were removed automatically (fewer than 10%) using a Matlab routine 66 (Fieldtrip).
We analyzed EEG activity to the target during baseline and filtering trials separately to threatening faces, nonthreatening faces, threatening IAPS, and nonthreatening IAPS. Stimulus-locked waveforms (sweep time = 2000 ms) were referenced to linked mastoids,
67
baselines corrected (200 ms prestimulus), and band-pass filtered between.1 and 30 Hz. Induced alpha power (9-12 Hz) calculated on each trial was extracted using a Morlet wavelet transform (spectral bandwidth = 6-8 Hz; wavelet duration = 80-106 ms) individually on each trial of each task in an epoch 200 ms in duration from stimulus onset, separately for each of 2 pairs of lateral electrode locations: frontal (F3, F4) and frontocentral (FC3, FC4). Alpha power was log transformed (Gasser, Bacher, & Mocks, 1982) to derive a composite measure of FAA
45
:

To test our hypothesis, we performed mixed model analyses of variance (ANOVA) on FAA scores separately for face and IAPS stimuli using Statistica® software, with Group (3 levels: PTSD, TEHC, and NTHC) as the between-subjects factor and Frequency (2 levels: upper alpha [11-12 Hz] and lower alpha [9-10 Hz]), Task (2 levels: baseline and filtering), and Emotion (2 levels: threat and nonthreat) as within-subject factors. Power analysis revealed that a sample size of n = 15 in each group was adequate (86% power) to reveal medium-sized (Cohen f = .35) within-between interactions. To guard against violations of the sphericity assumption with the repeated-measures data, all main effects and interactions reported as significant were reliable after Greenhouse-Geisser correction. 69
Results
Sample characteristics are summarized in Table 1. No differences between groups were found in age or education. Each of the 3 groups of participants was racially and ethnically diverse. Analysis of this study's behavioral data indicated that task accuracy of PTSD participants (0.88) was significantly worse than that of either TEHC (0.92) or NTHC (0.93) participants, who did not differ from each other, F(1,42) = 49.09, P <.001, MSe = 14.78, η2 = .42, suggesting that the visual flanker paradigm was effective in identifying diagnostic differences (see Melara et al 62 for more details).
Summary of Participant Demographic and Clinical Characteristics in the PTSD, TEHC, and NTHC Groups.
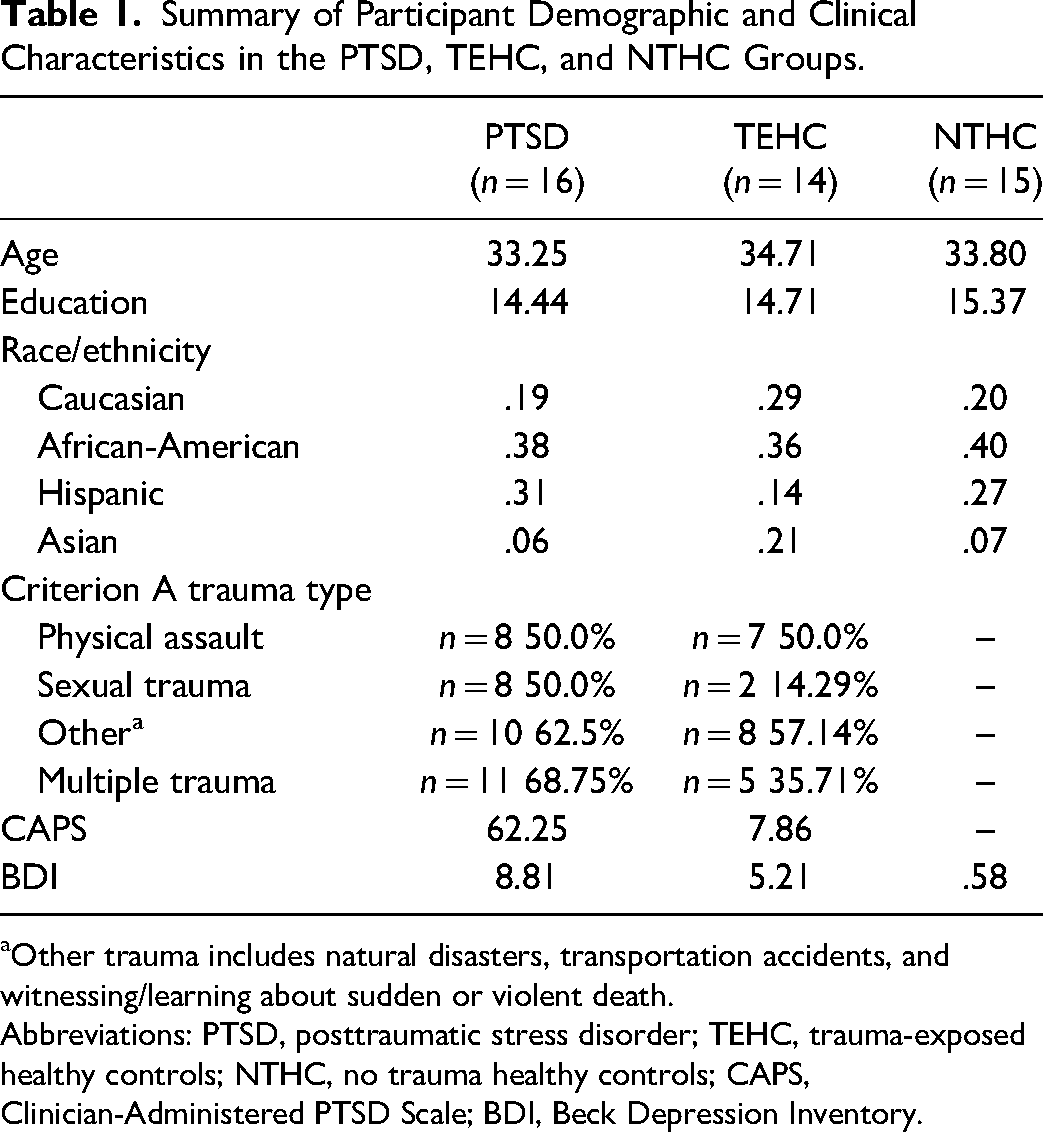
Other trauma includes natural disasters, transportation accidents, and witnessing/learning about sudden or violent death.
Abbreviations: PTSD, posttraumatic stress disorder; TEHC, trauma-exposed healthy controls; NTHC, no trauma healthy controls; CAPS, Clinician-Administered PTSD Scale; BDI, Beck Depression Inventory.
ANOVA of FAA to IAPS stimuli uncovered a main effect of Emotion (1,42) = 9.99, P < .01, MSe = .01, η2 = .001, no effect of Group, F(2,42) = 2.43, ns, MSe = .40, η2 = .01, and a significant interaction between Group and Emotion, F(2,42) = 4.25, P < .01, MSe = .06, η2 = .002, which were significant after epsilon correction for violation of sphericity. PTSD participants evidenced greater relative left than right FAA (approach: FAA > 0) in response to IAPS stimuli, t(15) = 2.28, P < .05, particularly to threatening stimuli, whereas NTHC participants demonstrated lower relative left than right FAA (avoidance: FAA < 0) to both threatening and nonthreatening stimuli, t(14) = −2.30, P < .05, with TEHC participants evincing numerically (but nonsignificantly) greater relative left FAA to threatening stimuli and reduced relative left FAA to nonthreatening stimuli. As shown in the left panel of Figure 2, both PTSD and TEHC participants displayed greater relative left FAA in response to threatening stimuli and a significant difference between threatening and nonthreatening stimuli.
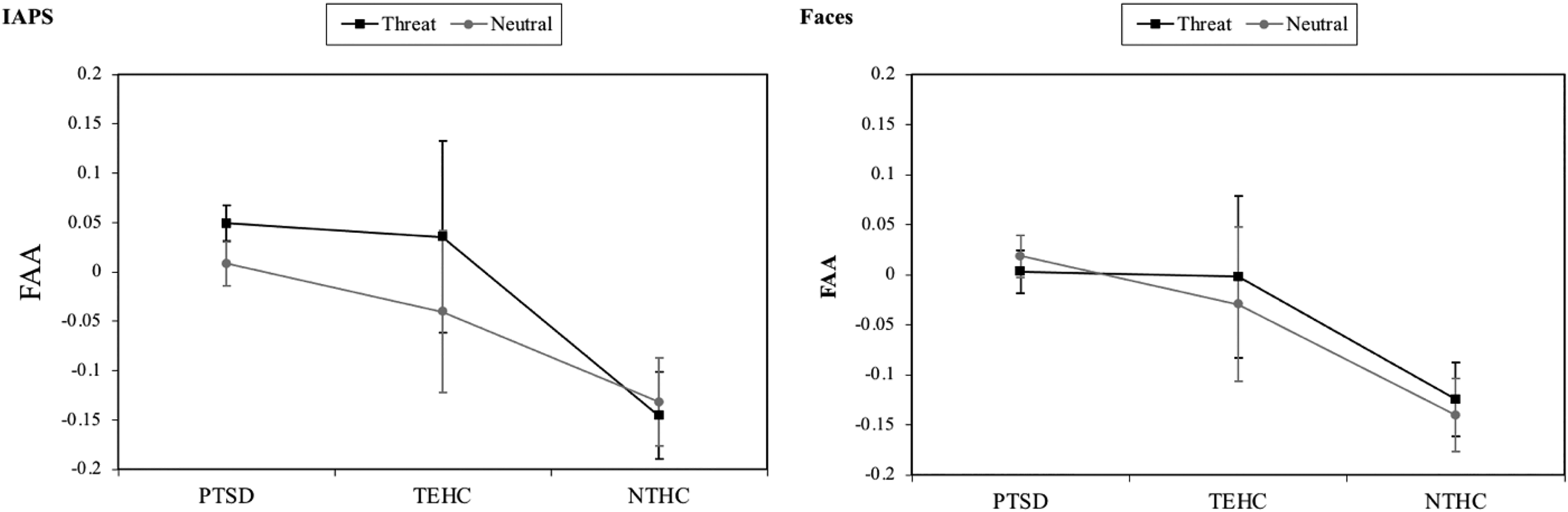
Average magnitude (with standard error bars) of FAA to threatening and nonthreatening (neutral) IAPS and face stimuli in PTSD, TEHC, and NTHC groups.
The effects of emotion on the group were modulated by task, yielding a significant 3-way interaction of Group, Emotion and Task, F(2,42) = 4.22, P < .05, MSe = .008, η2 = .0003. As can be seen in Figure 3, trauma-exposed individuals (especially the PTSD group) exhibited greater relative left FAA (ie, greater low alpha) than nontrauma-exposed control participants; but, primarily during trials where emotional salience/valence could be consistently anticipated (vs trials where stimuli were randomized). However, in the filtering task, where distractors varied randomly from trial to trial, only the PTSD individuals evinced a greater relative left FAA, F(2,42) = 3.65, P < .05, MSe = .15, η2 = .01, and equally to both threatening and nonthreatening stimuli; by contrast, in filtering both TEHC and NTHC participants revealed a reduced relative left FAA (equivalent between groups), again equally to both threatening and nonthreatening stimuli. Greater relative left FAA in the PTSD and TEHC groups was slightly greater at upper alpha, especially in the PTSD group, yielding a significant Group × Emotion × Frequency interaction, F(2,42) = 4.59, P < .01, MSe = .0002, η2<.0001.
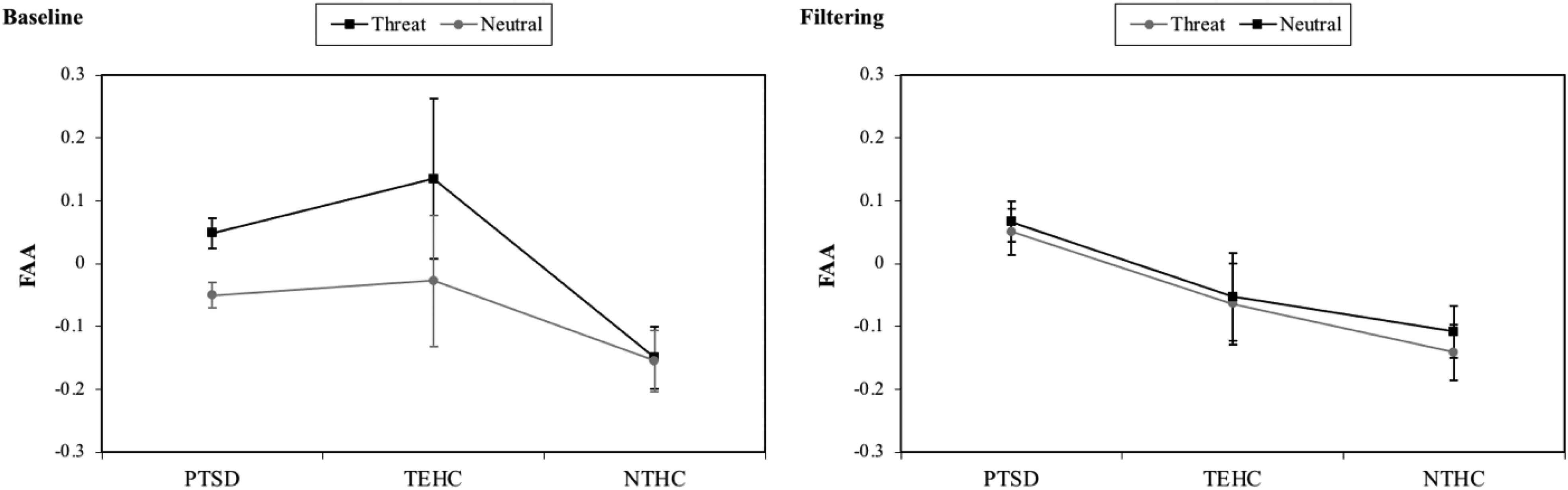
Average magnitude (with standard error bars) of FAA to threatening and nonthreatening (neutral) IAPS stimuli during baseline and filtering tasks in PTSD, TEHC, and NTHC groups.
ANOVA of FAA to face stimuli yielded no main effects of Group, F(2,42) = 1.41, ns, MSe = .31, η2 = .01, or Emotion, F(1,42) = 1.70, ns, MSe = .004, η2<.0001, but a significant interaction between factors, F(2,42) = 3.43, P < .05, MSe = .004, η2 = .0002, though the effect size was small. Here, as shown in the right panel of Figure 2, FAA in PTSD participants was slightly greater to nonthreatening stimuli whereas FAA in TEHC and NTHC participants was greater to threatening stimuli. There were no other interactions to face stimuli involving Group.
Discussion
By examining the relationship in an inhibitory control paradigm between PTSD and FAA, a neurophysiological indicator of approach and avoidance motivations, 30 the current study aimed to bring further precision to the field's understanding of PFC processes in PTSD and to enhance the status of FAA as a biomarker for posttraumatic pathology. In the first examination of its kind, we compared hemispheric differences in frontal brain activation to stimuli designated as either threatening or neutral in 3 groups of participants: those meeting DSM-IV criteria for PTSD, those exposed to trauma but reporting no PTSD symptoms, and a control group without trauma exposure or trauma-related pathology. Three notable findings emerged. Firstly, when cues were comprised of IAPS stimuli, we found evidence of a greater left relative to right frontal brain activity in individuals with PTSD in comparison to healthy controls. Secondly, when demand for inhibitory control was relatively low (IAPS baseline task), the trauma-exposed (PTSD and TEHC) groups differed from healthy controls: Both groups demonstrated significantly greater relative left FAA (approach) with the presentation of threatening than neutral stimuli. Healthy controls, by contrast, consistently showed only lower relative left to right frontal brain activation (avoidance), undifferentiated by stimulus type (whether the cue was threatening or neutral) or task (whether inhibitory demand was low vs high). Lastly, when the task's cognitive demand increased (IAPS filtering task), the clinical group was distinguishable from both the TEHC and healthy groups: Those with PTSD exhibited more left relative right frontal brain activity while the 2 other groups displayed reduced left relative right frontal brain activity.
Study findings reveal 2 significant divergences in how individuals with PTSD process visual stimuli. First, we found a generally greater relative amount of left than right frontal brain activity in PTSD. This suggests that greater approach-oriented brain activity may be a distinguishing feature of PTSD during rapid cognitive tasks. Second, we found that when the cognitive demands were comparatively low for individuals with PTSD, greater relative left FAA was discriminant to the emotional salience of the stimuli—showing more approach tendencies with threatening cues. Taken together, these 2 features of approach-related brain activity in individuals with PTSD highlight the potential mechanism of hypervigilance, a hallmark aspect of trauma-related pathology, whereby attention is automatically biased towards the detection and processing of threatening information. 2 As described in the Introduction, approach to trauma-related stimuli—attentional facilitation—has been linked to early, automatic stages of stimulus processing in PTSD.24-27 The current findings appear to further support the primary role of exaggerated approach-related, PFC states in the array of dysregulated attentional patterns demonstrated by individuals with PTSD. 70 Relatedly, our results reveal how attentional processes may be altered by not only the psychiatric condition of PTSD, but also by a history of trauma exposure without overt symptomatology. In comparison to the healthy control group's consistent attentional avoidance of threatening and neutral cues, FAA for the group with TEHC but no PTSD symptoms paralleled that of the PTSD group, but to a lesser degree, during low demand (baseline) trials. Such approach orientation could be considered the attentional sequalae of experiencing a traumatic event, regardless of pathological consequence.
Implications for Attentional Facilitation
Although our findings with PTSD showing approach to threat-related stimuli at baseline converge with prior findings of early attentional facilitation, 71 our findings during filtering of greater relative left FAA in PTSD participants to both cue types suggests a pattern of early attentional engagement indiscriminate in approach orientation, complicating an enhanced threat-detection mechanism exclusive to threat and negative stimuli.24,25 One possible explanation for the absence of a facilitated detection towards threat during high demand is misattribution by the PTSD group: Neutral stimuli are perceived as potentially threatening. For those with PTSD, the networking of attentional PFC control over information from the BLA appears disrupted, decoupled from the specific emotional saliency of the stimuli, and suggestive of an over-sensitization of human's “innate alarm system.” 72 Alternatively, early approach tendencies in PTSD may prioritize threatening stimuli in response circuitry, leading to attentional facilitation of threat in dot probe and other attention paradigms. FAA analysis during dot probe may help in future studies to understand the interplay between approach behavior and attentional bias in PTSD.
Task-Related Processing to Faces
Unlike with IAPS stimuli, we found no group differences in FAA to threatening versus neutral face stimuli at either low or high alpha. One possible explanation is that manipulation of threat in the IAPS stimuli (eg, threat was signaled using scenes of domestic violence, public violence, dangerous animals, and catastrophic weather) was more overt than in the face stimuli (fearful faces vs neutral faces). Thus, perhaps resolving emotion to faces places a premium on task-related activity in PTSD, while engaging more diffuse activity (lower alpha) when confronted with scenes.
Neural Basis of Resilience
Whereas the approach bias observed in PTSD may reflect emotional dysregulation of PFC mechanisms, the results with TEHC, or what could be considered the resilient participants, may be a healthy adaptive response to threat in individuals previously exposed to trauma. Specifically, the TEHC group showed greater relative left than right frontal brain activity to threatening over nonthreatening stimuli at baseline (low demand) but reduced left relative to right FAA to both stimuli during filtering (high demand). Characteristics of resilient individuals include tolerance for negative affect,73,74 adaptability, 75 self-efficacy,76,77 and confidence in handling life challenges. 78 The different FAA patterns in TEHC during baseline versus filtering could therefore reflect a PFC mechanism to sensitively gauge, confront, and regulate threat, a mechanism that is absent or dysfunctional in PTSD. In fact, Melara et al 62 found in the same group of participants tested in the present study showed significantly greater activation in TEHC than PTSD in ventromedial PFC, an area heavily involved in emotion regulation.79-81
Limitations and Future Directions
By moving beyond trait-level and state-dependent investigations of FAA in PTSD, the present study's novel focus on the impact of trauma exposure and PTSD on brief attentional tasks is a major strength. Findings are strengthened using 3 participant groups (individuals with PTSD, individuals with trauma exposure without PTSD, and individuals without trauma exposure), which allowed for the distinguishing of FAA patterns unique to exposure to trauma and those related exclusively to PTSD. The sample's diversity in terms of type of trauma exposure and the significant representation of racial and ethnic minorities also bolster the generalizability of results. Nevertheless, several limitations are important to note. Firstly, our findings must be interpreted within the relatively small sample size and their replication in future work is critical. A larger sample size would also allow for more precision in the matching of groups across trauma exposure types and demographic characteristics (ie, race and ethnicity) than was possible in the present study. Secondly, the study was limited by certain methodological decisions. Despite the high co-occurrence of PTSD and substance use disorders (SUD), 82 we excluded individuals who reported an addiction history, and thus our findings cannot be applied to the large subpopulation of individuals who suffer from comorbid PTSD and SUD. Since substance misuse in the context of PTSD is often understood as an avoidance coping strategy, 83 the study of FAA may be particularly relevant in understanding and identifying individuals at risk for problematic substance use and the development of SUDs after trauma exposure. Because the symptoms of PTSD encompass both alterations in avoidance (fear and negative mood) and approach (anger) motivations and affect, our classification of participants by diagnostic status rather than by PTSD symptom type did not allow for observing potential associations between FAA and specific PTSD symptoms such as reexperiencing, hyperarousal, or dysphoria. Furthermore, prior studies have noted that a significant portion of the relationship between PTSD and FAA is not unique to the disorder but is accounted for by comorbid anxiety and depressive pathology. 45 Moreover, source localization of FAA to the PFC region can only be hypothesized in the current study. Future research would benefit from the integrative strength of simultaneously combining EEG recording with functional magnetic resonance imaging to confirm the anatomical regions activated during FAA. Finally, the present study underscores the utility of FAA as an indicator of PTSD-related attentional and inhibitory control deficits, and thus a potential target of intervention. We recommend that future research explore the amenability of FAA in PTSD to neurofeedback techniques akin to the alpha-asymmetry neurofeedback protocols developed for major depressive disorder 84 that have recently garnered support for comorbid anxiety and depression. 85
Conclusions
The current study supports the potential use of FAA as a clinical marker of PTSD. Our analysis suggested greater relative left to right frontal brain activity in PTSD, particularly to threatening baseline stimuli, indicative of dysfunctional regulatory mechanisms in PFC. We also found differences in FAA patterns in TEHC depending on whether demand for inhibitory control was low (approach) or high (avoidance), perhaps suggesting a flexible PFC mechanism to regulate threat. Our results are the first to use FAA to explore approach-avoidance activity in individuals with and without trauma exposure and individuals with PTSD and provide the foundation for future inquiry into FAA as a potential target for ameliorating the effects of PTSD.
Footnotes
Author Contributions
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This research was funded by a City Seeds grant from the City College of New York.
Ethical Approval
This research was approved by The City College of New York's Institutional Review Board.