
Abstract
Introduction
Post-stroke seizures (PSS) are well-recognized clinical presentations and complications of both ischemic stroke (IS) and hemorrhagic strokes (HS). Cardio-embolic ISs and presence of large anterior circulation infarcts are associated with a high risk of PSS. 1 Patients who had suffered from PSS are observed in the form of either focal or generalized seizures with status epilepticus (SE) in both early and late phases of acute strokes. 2 Early PSS (EPSS) occurs within one week after stroke and defined as acute symptomatic seizures, while late PSS (LPSS) occur after 1 week. 3 In the current literature, EPSS are reported in 2.5–6%, with most seizures occurs within the first 24 h.4,5 Additionally, the risk of seizure recurrence in EPSS is reported in about 33% of stroke patients. 6 LPSS are more frequent than EPSS and affect approximately 10–20% of stroke patients, and carries a significantly higher risk, 71.5% of developing another unprovoked seizure in the next 10 years.5,6 Following the new practical definition of epilepsy by the International League Against Epilepsy (ILAE), diagnosis of epilepsy can be established after a single unprovoked seizure if it is associated with other conditions suggesting the risk of seizure recurrence comparable to the risk after two unprovoked seizures. 6 Following this definition, it is possible to make the diagnosis of post-stroke epilepsy (PSE) after even a single unprovoked seizure related to remote stroke.7,8
Predictors of PSS recurrence (PSSR) are not well characterized. However, HS, high higher stroke severity, and cortical lesions are most commonly associated with PSE. 9 Cortical excitability secondary to glutamate-mediated excitotoxicity, shifting of ion channels in acute phase of stroke while gliotic scarring, neurodegeneration, and persistent inflammation are possible mechanisms for PSE. 9 Seizure recurrence is associated with declined in functional status hence increasing the disease burden. 10 EEG is the best and cost-effective neurodiagnostic technique for detecting epileptic activity, and identifying the irritative zone, recognizing non-convulsive SE, and predicting seizure recurrence. 11
EEG can be used as a helpful tool for subsequent prediction of recurrence, and diagnosis of PSE in stroke patients. 12 Role of EEG in early and accurate detection of PSS-related epileptiform abnormalities (EAs) and their roles in patient’s prognosis has been studied before. 13 In one meta-analysis the pooled frequency of post-stroke ictal and interictal EAs were 7% (95% CI 3%–12%) and 8% (95% CI 4%–13%), respectively. 14 Hence, this approach may be useful in predicting the development of PSE and its management. However, there is a lack of reports investigating the association between EEG findings and seizure recurrence, particularly in LPSS.12,15 Current study highlights the importance of EEG patterns linked to seizure recurrence and with the functional outcomes in PSS patients.
To the best of our knowledge, this is the first study to report the EEG characteristics in stroke-related seizures and their association with the seizure recurrence and functional outcomes in the Saudi population and it may be useful for further large-scale research to understand pathophysiology, and predictive factors, therefore to improve the management and prevention of seizure-related complications. The objective of this study was to assess the frequencies of different EEG patterns in patients with PSS and their association with seizure recurrence and functional outcomes of these patients.
Materials and Methods
Study Design and Setting
This study involved a review and analysis of EEGs and medical records of patients with the diagnosis of either IS or HS who developed PSS.
This study was performed at King Fahd hospital, Imam Abdulrahman Bin Faisal University based in the Eastern province of the Kingdom of Saudi Arabia (KSA), and was approved by the Institutional Review Board (IRB Number: IRB 2023-01-154). The study enrolled all the patients with PSS who presented between January 2018 and December 2020. Current study is a sub-study and the part of our PSS project.
Patient's electronic charts and OPD visits were reviewed for at least 24 months following first PSS, to identify the recurrence of seizure and to document modified Rankin Scale (mRS). Patients with a history of epilepsy before stroke occurrence, transient ischemic attacks (TIA), stroke mimics (tumor, infection, and functional disorders), cerebral venous sinus thrombosis, and patients who lost follow-up were excluded. The demographic data, stroke location, and severity, seizure occurrence with time after stroke, type of seizure, recurrent seizures, development of SE, use of anti-seizure medications (ASMs), use of intravenous recombinant tissue plasminogen activator (rtPA), EEG findings, brain imaging findings either computed tomogram (CT) or magnetic resonance imaging (MRI) were recorded. EEG was performed in all the patients after their first seizure. ASMs were categorized as old generation; including valproic acid (VA), carbamazepine, phenytoin and benzodiazepines, and new generation; including levetiracetam, lamotrigine, topiramate, and lacosamide.
In EEG laboratory, Cadwell Electroencephalograph with ARC Essentia EEG Amplifier (USA) was used for EEG recording. Silver–silver chloride disk scalp electrodes were placed according to the International 10–20 System, utilizing both bipolar and average referential montages, with measured impedances<5 kΩ at all electrodes. All EEG records were performed for 20–30 min and were evaluated and interpreted by an epileptologist.
Operational Definitions
Among the strokes types, IS was defined as a sudden, focal neurological deficit of presumed vascular etiology lasting for more than 24 h, in the absence of intracranial hemorrhage (diagnosed by CT/MRI of brain). National institute of Health Stroke Scale (NIHSS) was used to assess the stroke severity and mRS was used to document stroke outcomes. NIHSS is a 15-item impairment scale used to measure stroke severity 16 The seizure was defined as “a transient occurrence of signs and/or symptoms due to abnormal excessive or synchronous neuronal activity in the brain, 7 and seizure types were divided into focal aware, focal with impaired awareness, and focal to bilateral tonic-clonic, according to the 2017 International League Against Epilepsy (ILAE) Commission on Classification and Terminology report based on their documented semiology.” 8 Seizures were categorized as EPSS and LPSS. EPSS were further analyzed as occurring within 24 h or 24 h to 7 days. 3 SE was defined as one continuous and unremitting seizure lasting for more than 5 min or recurrent seizures without restoration of consciousness for greater than 5 min. 17
PSE was defined as one unprovoked seizure occurring more than one week after stroke, following the ILAE guidelines. 7 Standard terminologies adopted from the American Clinical Neurophysiology Society's (ACNS) Standardized Critical Care EEG Terminology: 2021 Version, glossary of EEG terms was used for EEG reporting. 18 Abnormal EEG patterns were classified as focal slowing or focal slow wave activity (FSWA), focal means limited to a small area of the brain in one hemisphere, and slowing was defined as waves of frequency less than 8 Hz, which commonly appear at one or a few electrodes and non-rhythmic. 19 Generalized slowing, or generalized slow wave activity (GSWA), generalized mean an EEG activity spread over large areas of both sides of the head, and slowing was again defined as any activity of frequency less than alpha rhythm, that is, theta and delta bands as well as non-rhythmic. Focal sharp wave discharges (FSWDs) were defined as localized epileptiform activity, originating within networks limited to one hemisphere; these discharges are transient and distinguishable from background activity. FSWDs are having characteristic morphology fulfilled at least 4 of the following 6 criteria: 19
(1) Di- or tri-phasic waves with sharp or spiky morphology (ie, pointed peak). (2) Different wave duration than the ongoing background activity, either shorter or longer. (3) Asymmetry of the waveform: a sharply rising ascending phase and a more slowly decaying descending phase, or vice versa. (4) The transient is followed by an associated slow after-wave, and the background activity surrounding epileptiform discharges is disrupted by the presence of the epileptiform discharges. Generalized sharp wave discharges (GSWDs) were defined as above-mentioned epileptiform patterns spread over large areas of both sides of the head. 19 As per ACNS 2022 criteria lateralized periodic discharges (LPDS): (1) repetition of a waveform with relatively uniform morphology and duration, (2) with a clearly discernable interdischarge interval between consecutive waveforms, and (3) recurrence of the waveform at nearly regular intervals: having a cycle length (ie, period) varying by, 50% from one cycle to the next in the majority (.50%) of cycle pairs. A pattern can qualify as rhythmic or periodic if and only if it continues for at least 6 cycles (eg, 1 Hz for 6 s, or 3 Hz for 2 s). 18
Statistical Analysis
Data was collected in a specialized proforma. The analysis was performed by using Statistical Package for Social Sciences (SPSS), version 26.0. Results are presented as frequency (percentage), mean (standard deviation [SD]), or median (interquartile range [IQR]), as appropriate. Continuous variables are reported as mean ± SD, whereas categorical variables such as sex, seizure types, EEG patterns, and outcomes are presented as frequencies and percentages. Independent sample t-test or Mann–Whitney U test was used to establish the statistical significance of the differences between the groups (patients with and without recurrence) in terms of age, sex, underlying etiology, EEG patterns, and poor functional outcomes. Odds ratios (ORs) of seizure recurrence and functional decline at 2 years were calculated by using logistic regression. Variables showing p value < .25 in the univariate analysis and considered clinically or biologically significant by the researchers, were further tested in the multivariate cox-proportional hazards model for PSS recurrence. P value below .05 was taken as significant. PSS were classified as early (within one week after stroke) or late (in the second week or later) and the primary outcome was the recurrence of seizure following first PSS.
Results
A total of 106 patients were enrolled in the study. During the 2-year follow-up period, 39 (36.8%) patients had at least one recurrent seizure hence grouped as PSS recurrence (PSSR), whereas 67 (63.2%) did not (non-recurrence group). The mean age was 62.10 ± 15.87 years ranging between 20 and 107 years. Table 1 describes the comparison of baseline characteristics and univariate analysis of the study patients with PSS.
Characteristics of Patients with and Without Recurrence: Univariate Analysis.
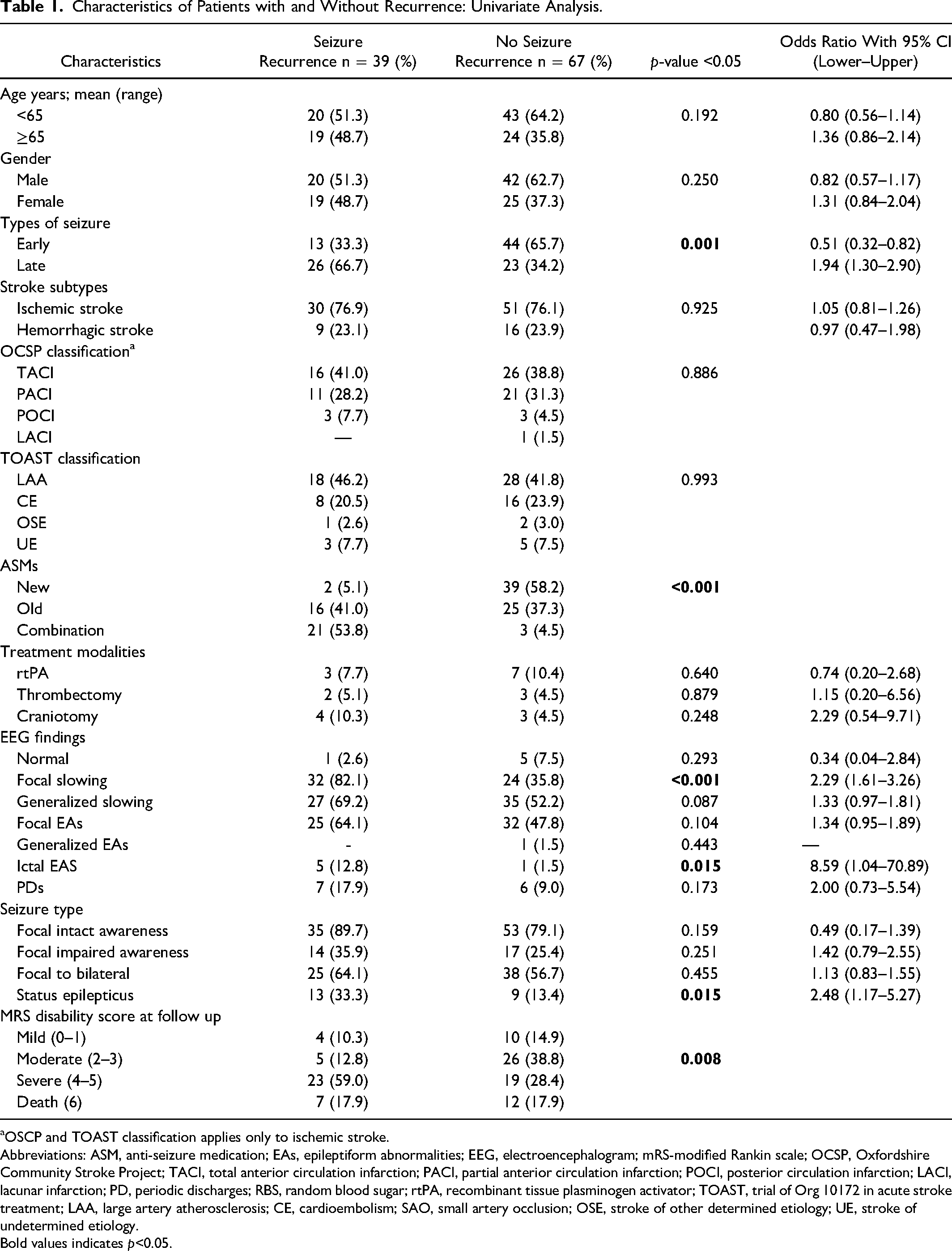
OSCP and TOAST classification applies only to ischemic stroke.
Abbreviations: ASM, anti-seizure medication; EAs, epileptiform abnormalities; EEG, electroencephalogram; mRS-modified Rankin scale; OCSP, Oxfordshire Community Stroke Project; TACI, total anterior circulation infarction; PACI, partial anterior circulation infarction; POCI, posterior circulation infarction; LACI, lacunar infarction; PD, periodic discharges; RBS, random blood sugar; rtPA, recombinant tissue plasminogen activator; TOAST, trial of Org 10172 in acute stroke treatment; LAA, large artery atherosclerosis; CE, cardioembolism; SAO, small artery occlusion; OSE, stroke of other determined etiology; UE, stroke of undetermined etiology.
Bold values indicates p<0.05.
Among the stroke types, PSS was observed in 81 patients with IS (76.5%) and in 25 patients with HS (23.6%). Within the HS patients, the majority of them presented lobar hemorrhages (n = 17). Focal to bilateral seizures were the most common seizure type observed in 63 patients (59.4%). Twenty-two patients (20.8%) had developed clinical SE. The majority of patients have been started on monotherapy ASMs.
GSWA was the most frequent EEG pattern observed (n = 62, 58.5%), followed by FSWDs (n = 57, 53.8.4%), and FSWA (n = 56, 52.8%). Ictal EAs were observed in total six patients (5.7%) while majority had LPSS (four out of six). Periodic discharges (PDs) were observed in 13 (12.3%) with almost equal distribution in both EPSS and LPSS patients, however; FSWDs were significantly more observed in LPSS group (p = .009), Table 2. Examples of various EEG patterns associated with radiological diagnoses are shown in Figure 1.

EEG epochs (longitudinal bipolar montage, sensitivity; 10 mic V/mm, LFF; 1 Hz, HFF; 70 Hz, time base; 30 mm/sec). (A) Right periodic discharges with right MCA territory infarction (axial CT head), (B) right focal sharp wave discharge with right posterior temporal parenchymal bleed (axial CT head), (C) right focal slow wave activity with right posterior temporal infarction (axial CT head) Hz, hertz; HFF, high frequency filter; LFF, low frequency filter; MCA, middle cerebral artery; CT, computed tomography.
Comparison of EEG Patterns in Different Patient's Groups.
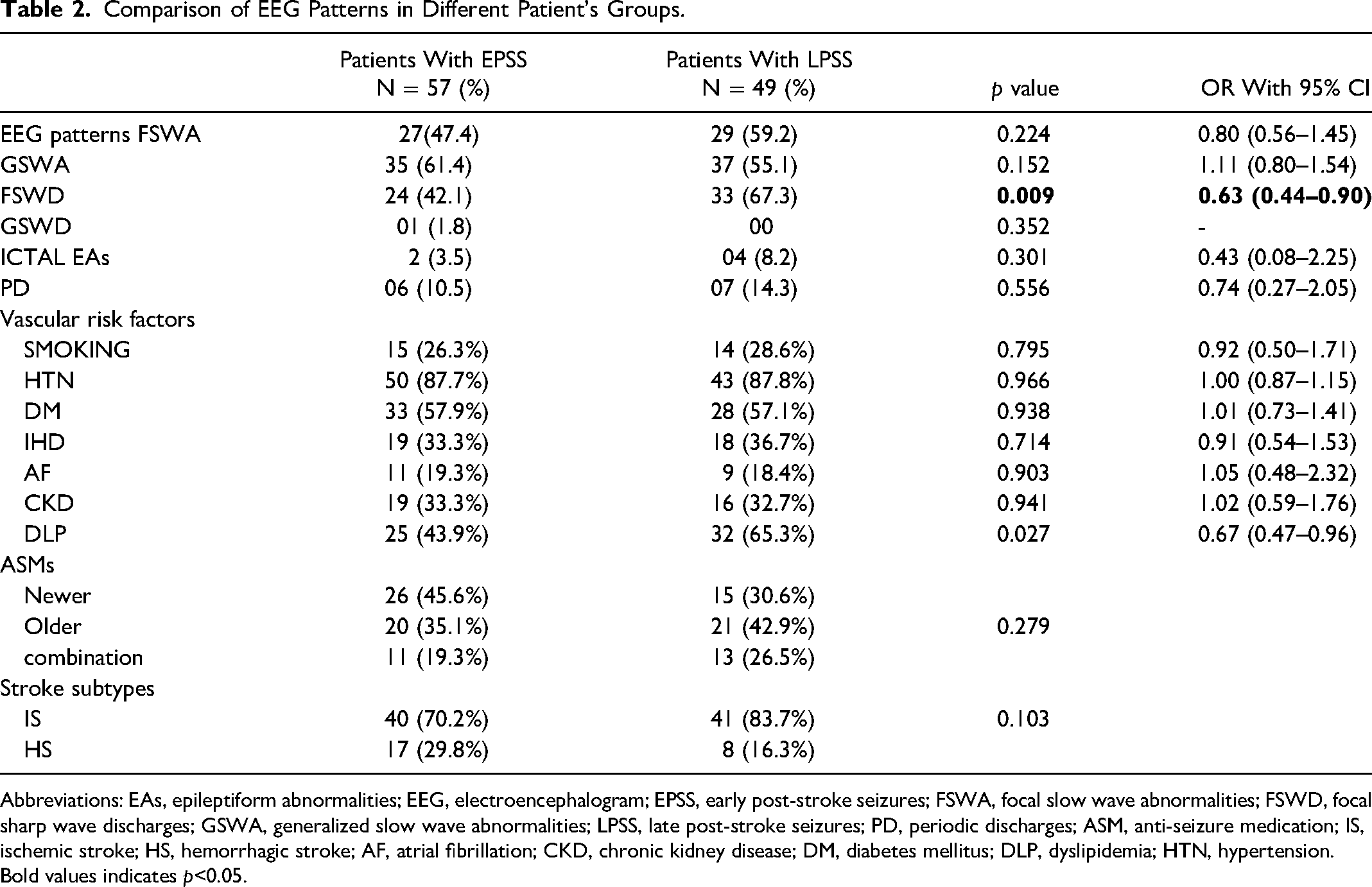
Abbreviations: EAs, epileptiform abnormalities; EEG, electroencephalogram; EPSS, early post-stroke seizures; FSWA, focal slow wave abnormalities; FSWD, focal sharp wave discharges; GSWA, generalized slow wave abnormalities; LPSS, late post-stroke seizures; PD, periodic discharges; ASM, anti-seizure medication; IS, ischemic stroke; HS, hemorrhagic stroke; AF, atrial fibrillation; CKD, chronic kidney disease; DM, diabetes mellitus; DLP, dyslipidemia; HTN, hypertension.
Bold values indicates p<0.05.
Seizure recurrence was detected in 39 patients (36.8%) and, this was observed significantly in patients who had FSWA and ictal EAs in EEG, (X2 = 21.14; p < .001 and X2 = 5.94; p = .015, respectively), with SE, (p = .015), and those who were receiving old generation of ASMs (X2 = 44.58; p < .001). Similarly severe functional disability was observed in patients who were receiving old generation ASMs, (X2 = 6.57; p = .037), who had GSWA and FSWA (X2 = 5.88; p = .015, X2 = 3.68; p = .055, respectively). DM (X2 = 4.49; p = .034), CKD (X2 = 10.04; p = .002), and IS (p = .010) were associated with poor functional outcome. GSWA was associated with poor functional outcomes only (X2 = 5.89; p = .015). FSWDs were found significantly more in LPSS group (X2 = 6.75; p = .009), however; it was not associated with seizure recurrence or poor functional outcome (Tables 2 and 3).
Comparison of EEG Patterns with Seizure Recurrence and Severe Disability.
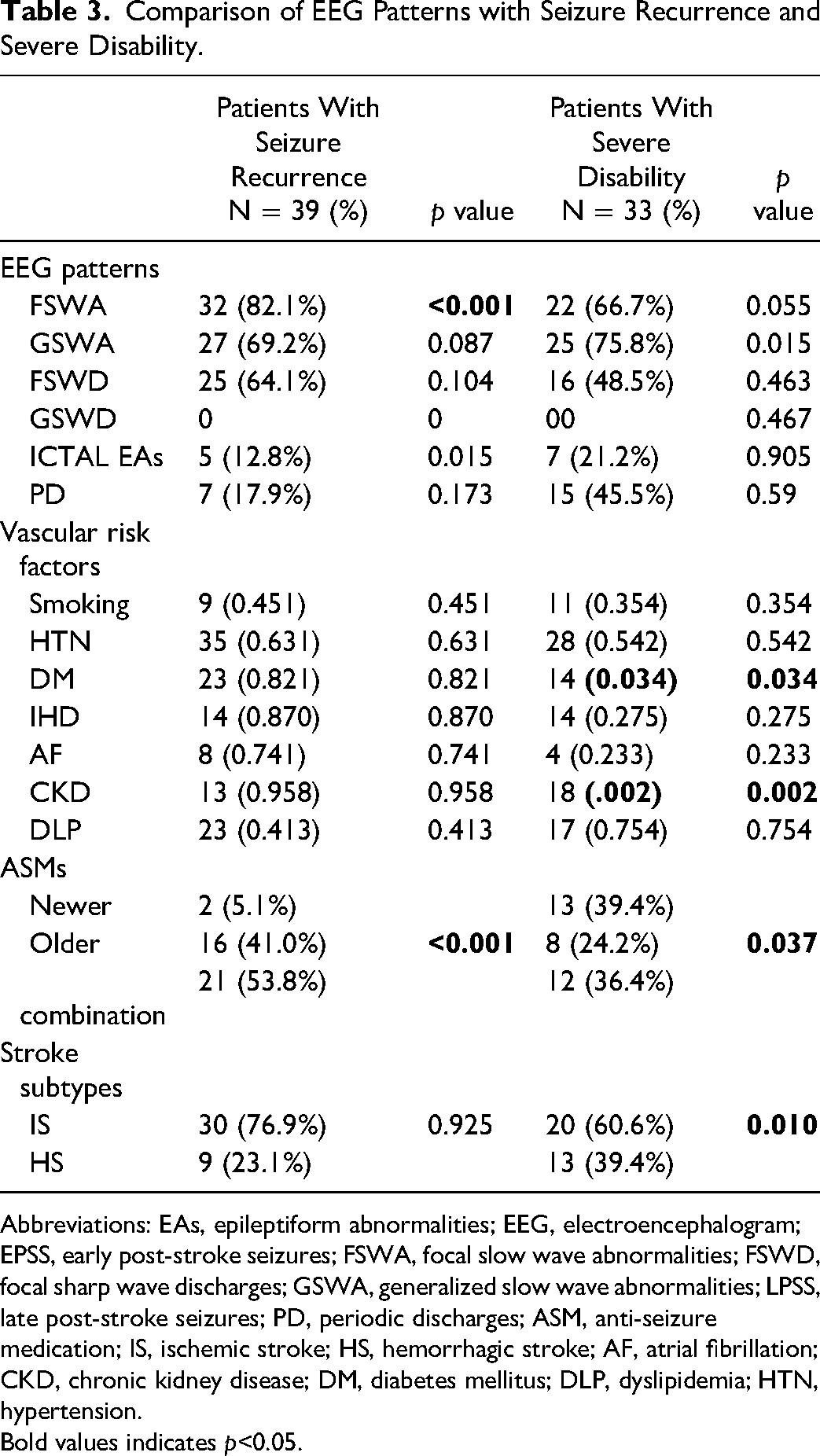
Abbreviations: EAs, epileptiform abnormalities; EEG, electroencephalogram; EPSS, early post-stroke seizures; FSWA, focal slow wave abnormalities; FSWD, focal sharp wave discharges; GSWA, generalized slow wave abnormalities; LPSS, late post-stroke seizures; PD, periodic discharges; ASM, anti-seizure medication; IS, ischemic stroke; HS, hemorrhagic stroke; AF, atrial fibrillation; CKD, chronic kidney disease; DM, diabetes mellitus; DLP, dyslipidemia; HTN, hypertension.
Bold values indicates p<0.05.
Nevertheless, multivariate cox-proportional hazards model of PSS recurrence (Table 4) showed significant association of female gender (HR = 3.28; 95% CI: 1.42–7.58; p = .006) while all other predictor variables turned out to have insignificant association. Hazard ratio (HR) was increased with older ASMs use, focal aware seizure types, Ictal EAs, and periodic discharges on EEG; however, it was not statistically significant.
Multivariate Cox Proportional Hazards Model.
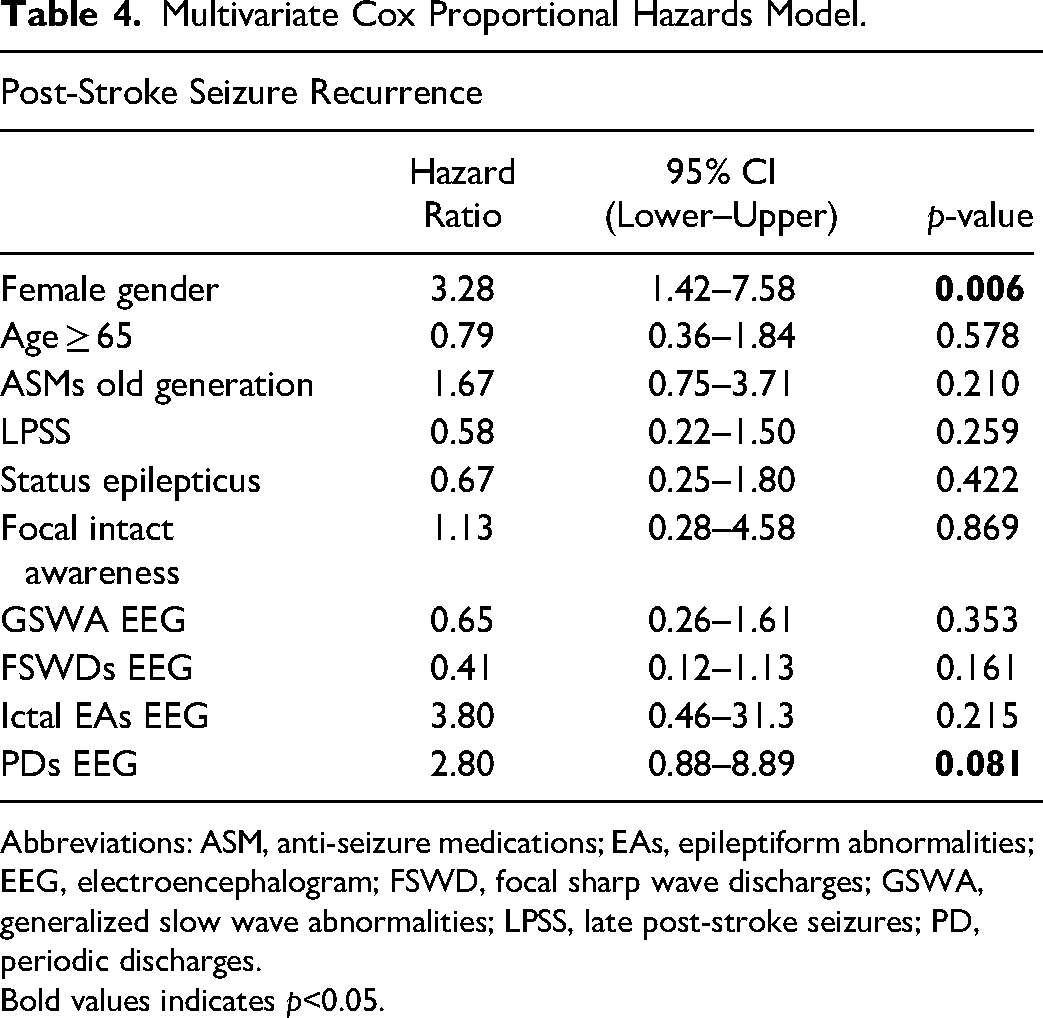
Abbreviations: ASM, anti-seizure medications; EAs, epileptiform abnormalities; EEG, electroencephalogram; FSWD, focal sharp wave discharges; GSWA, generalized slow wave abnormalities; LPSS, late post-stroke seizures; PD, periodic discharges.
Bold values indicates p<0.05.
Discussion
Stroke-related complications are getting increase in clinical practice with improvement in acute stroke care globally. Hence it is important to identify tools which could predict the occurrence as well as recurrence of PSS to better manage them and to minimize the morbidity related to seizures in stroke patients. EEG is the best neuro-diagnostic technique for identifying epileptic activity, especially in patients with non-convulsive post-stroke epileptic activity, identifying the epileptogenic zone, and predicting the seizure recurrence. 13 The EEG continues to be a reliable tool for diagnosis of PSS, with increased monitoring duration, subclinical seizures are also commonly identified. 20 Yet, reports are scanty exploring the connection between EEG findings and seizure recurrence, especially in LPSS.12,15
The present study demonstrated that certain EEG findings indicate seizure recurrence risk in patients with PSS, regardless of prior ASMs use and risk factors and highlighted the association between seizure recurrence and EEG findings in patients with PSE. We found interesting EEG findings in PSS patients. The present study showed that GSWA and FSWA with FSWDs were commonly identified in patients with PSS, with no significant difference between EPSS and LPSS, except FSWDs which were recorded most commonly with LPSS (p = .009). Belcastro et al discovered in their research that 3.6% of IS patients experienced subclinical seizures especially in the first week following stroke. 21 Patients who suffer from PSS, their EEG characteristics could be early-onset findings or late-onset findings. Elbasher Ibrahim et al have reported EEG slowing focal or diffuse having lower risk of stroke-related seizures while focal EAs and LPDs, which represent cerebral hyperactivity and elevated seizure risk. 22 De Reuck et al stated that patients with stroke might demonstrate an EEG characteristic that does not correspond with experiencing subsequent seizures. 1 They reported frontal intermittent rhythmic delta activity (FIRDA) (16.4%) and GSWA (21.8%) as early onset EEG findings, while 98 out of 110 patients had FIRDA in both late (14.3%) and early (16.4%) onset PSS. When compared with the early onset, the presence of GSWA and LPDs was significantly lower in the late stage. 1 however, these EEG findings especially in early stroke phase have low diagnostic value for seizure occurrence as it reflects acute hemodynamic brain changes rather epileptogenic activities. Similarly Wolf et al have observed that, individuals who suffer a stroke without following a seizure would still have abnormal EEG in 40 patients out of 69, showing either GSWA, which was in 7 (10.2%), or FSWA in 30 (43.5%) of the cases. 23 The presence of these EEG activities considered abnormal and linked to the stroke pathology and the side of the infarct. Sinkin et al has reported hemispheric slowing as the most prevalent finding in 42% of cases, followed by FSWA in 25% and GSWA in 12.8% of cases. 20 Current study showed that FSWDs was the most frequent EEG pattern observed in patients with LPSS. While previously asymmetry in the background rhythm, focal interictal epileptiform discharges and GSWA, FIRDA, especially in frontal lobe strokes were reported in different studies.14,24 In present study LPDs were observed in a total of 13 (12.3%) only, with equal distribution in both EPSS and LPSS groups, and showed a weak association with seizure recurrence (p = .17). While some studies explored whether there is any relationship exist between PDs and seizure recurrence, Bentes et al 11 testified that the existence of PDs was an independent predictor of interictal EAs, suggesting that sharp PDs coexist with interictal EAs in PSS patients, as in the presence of PDs, potential EAs can be masked by continuous periodic waves. Therefore, prolonged or frequent EEG recording should be considered in the presence of PDs. One of the EEG characteristics that is identified in early onset because of the focal cortical stroke is LPDs, which are mostly sharps or sharp and slow waves. Morcarelli et al has pointed out that patient with SE had EEG discharges of localized region, often accompanied by subsequent generalization and observed LPDs in 9 out of 14 patients, which mostly consists of sharp and slow waves or sharp waves. 25 Bentes et al 11 reported a 3.2 times higher risk of unprovoked seizure in patients with asymmetric EEG background and 3.8 times higher if interictal EAs were recorded.
Niedzielska et al performed EEG in all patients who had a single or multiple seizures at the onset of stroke, EEG shown FSWA in 90% and interictal EAs in 22.5%. EEG in 14 patients with disturbed level of consciousness without clinical seizures revealed SE in all patients with simple partial in majority and complex partial SE in rest of them. While majority (11 14) of those patients EEG revealed fragments of LPDs interrupted by seizure activity. 26 Another study by Stancu et al reported that initial interictal EAs are a strong predictor for the development of PSE. 27
In the present study, PSSR was observed in a total of 39 (36.8%) patients and some EEG patterns were significantly associated with PSSR; such as patients who had FSWA, and ictal EAs in EEG (p < .001, p = .015 respectively). Various EEG patterns have been reported to be linked with recurrence. George et al assessed the likelihood of a recurrence during an acute phase against a remote period, 29.2% of patient with PSS developed recurrence. EEG in 12.9% of these patients had sharp waves or spikes, which are highly correlated with the recurrence of seizures, while intermittent slowing was observed in 29%. They observed that both LPDs and GSWA have been associated with a reduced risk for subsequent seizures. 12 In some studies EAs and FSWA are reported as a risk factor for seizure recurrence. 28 A meta-analysis performed in patients with genetic, idiopathic, structural seizure reported that presence of intericatl EAs in routine EEG following a single unprovoked seizure was associated with recurrence with a sensitivity of 17.3% and specificity of 94.7% respectively. 29 Some studies have reported sharp waves/spikes on EEG in PSS positively associated with recurrence. 12 Current study reported interictal FSWDs weakly associated with seizure recurrence (p = .104). An earlier study also reported that EEG findings did not correlate with seizure recurrence with PSE. However, the study differed from our study since it was without information about ASMs regimens or thorough criteria for EEG abnormalities. Furthermore, the recognition rate of epileptic abnormalities was lower than that in our study (17.2 vs 64.1%). 15
Other significant associations of PSSR are LPSS, SE, and IS (p < .001, p = .015, p = .010 respectively). SE was observed in 20.8% of PSS patients, and the presence of SE was significantly linked to seizure recurrence (p = .015). De Reucka et al observed that 14 of 110 patients in their study had SE (4 EPSS and 10 LPSS) 1 Ramiro Castro-Apolo et al concluded that the appearance of laminar necrosis on a CT scan is a warning sign for developing SE. In addition, laminar necrosis is linked to moderate to severe focal neurological impairments that appear in the majority of patients. 30 Another study identified SE in EPSS as a risk factor for developing PSE. 31 It might be linked with severe and large stroke lesion in those patients presenting with SE as early seizures. Certain risk factors are identified for post-stroke generalized SE in IS group, such as; female sex, African American race, renal disease, alcohol abuse, sodium imbalance, and hemorrhagic transformation, whereas African American and Hispanic race, renal disease, coagulopathy, brain tumor, alcohol abuse, and serum sodium abnormalities were associated with higher rates of generalized SE in HS patients. 32
In our study, severe functional disability was observed in patients with DM, CKD, and use of older ASMs (p = .034, p = .002, p = .037 respectively). SE was found to be correlated with poor functional outcome however, statistically insignificant (p = .103). LPDs are one of the characteristics that may occur prior to or following the SE recurrence in acute cerebral injury and have been linked with a poor prognosis and a significant risk of seizures and SE. 25
A strong association has been observed in current study between GSWA, and FSWA with physical disability (p = .015, p = .055 respectively). This tends to damage greater areas of cortical tissue and causes a severe neurological deficit. 32 However, GSWA being non-specific could have been related to underlying infection, metabolic derangement, or medication use rather than seizures. Most of the recent studies and meta-analyses have suggested poorer outcomes in stroke patients with PSS. 33 We did not find use of rtPA, endovascular treatment, and craniotomy linked to either seizure recurrence or poor functional outcome in our research. One reason is that rtPA use is associated with acute symptomatic seizures but not with the late seizures or seizure recurrence, 1 and subsequently have good functional outcome. While craniotomy is reported to be associated with PSS and majority of PSS patients had worse functional outcomes and death. 9 This could be explained due to massive stroke necessitating the need for surgical decompression as well as intervention-related brain injury.
Our findings suggest that certain EEG patterns are related to PSSR and poor outcome in stroke patients. ASMs selection may affect survival among patients with cerebrovascular disease and support use of newer generation ASM. Our results with VA may suggest need for more studies before advising caution for using it in this specific patient population. Our study has some limitations. First, being a retrospective design we could not completely eliminate the possibility of confounding error for focal or generalized slowing in EEG which could be due to metabolic causes rather than seizure related. Second, it lacks the continuous EEG monitoring, and additionally, the small size of the cohort might be a limitation to derive adjusted ORs with different predictive variables and only a routine 30 min EEG may have been inadequate to identify low frequency EAs. However, we verified the distribution of all continuous variables and confirmed that they are normally distributed.
The strengths of this study include: first, all the consecutive patients with different types of strokes such as IS, and HS were included, and the follow-up period was very reasonable to have at least 24 months. Second, two board-certified epileptologists and neurologists evaluated the EEGs in detail, which may have explained the relationship between EAs and seizure recurrence. In this study, we also have correlated EEG abnormalities with respect to EPSS versus LPSS, seizure recurrence, as well as functional disability.
Conclusion
Recognition and documentation of PSS-related EEG characteristics are important, as certain EEG patterns may help to identify the patients who are having at risk to develop recurrence. Combination of various EEGs, including long-term EEG, video EEG monitoring, and ambulatory EEGs should be used to improve the sensitivity of EEG abnormalities. Further larger, long-term prospective cohort follow up design may be useful for more detailed description specific EEG patterns among this important group. Additionally, our outcomes may be helpful in recruiting the high risk patients in clinical trials for evaluating the interventions in preventing PSE.
Footnotes
Acknowledgements
This study made use of the computational resources and technical services of the Scientific & High-Performance Computing Center at King Fahd hospital, Imam Abdulrahman Bin Faisal University based in the Eastern province of the Kingdom of Saudi Arabia (KSA).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical Statement
The study was approved at Imam Abdulrahman Bin Faisal University, Dammam, Kingdom of Saudi Arabia with IRB number 2023-01-154, and was performed in accordance with the Declaration of Helsinki.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.