
Abstract
Breach rhythm (BR) is a well-recognized EEG pattern characterized by high-amplitude, sharply contoured fast activity over areas of skull defect, most often following craniotomy or trauma. Although considered physiological, BR may closely mimic epileptiform discharges, leading to diagnostic uncertainty. We report a 33-year-old man with bilateral skull defects secondary to traumatic brain injury who presented with recurrent generalized tonic–clonic seizures. EEG showed continuous fast and sharp activity over the right F4–C4 region, consistent with BR, and diffuse slow waves over the left hemisphere. During two focal seizures, ictal discharges originating from the right F8 electrode transiently modified the morphology and rhythmicity of the ongoing BR before spreading bilaterally. Interestingly, no BR was observed over the left hemisphere despite a large skull defect, likely reflecting severe cortical injury. Following treatment with levetiracetam and phenytoin, seizures resolved, while the right-sided BR persisted unchanged. This case highlights that BR is not merely a passive artifact of altered conductivity but a dynamic indicator of cortical function. Its modulation during seizures and absence over structurally damaged cortex support the concept that BR may serve as a potential marker of cortical viability. Recognizing these patterns may prevent misinterpretation of physiological BR as epileptiform activity and enhance EEG evaluation in patients with structural brain lesions.
Introduction
Breach rhythm (BR) is characterized by a focal increase in the amplitude of alpha, beta, and mu rhythms, most commonly observed over areas of skull defect, such as after craniotomy or traumatic brain injury. 1 While the presence of a skull defect appears to be a necessary condition for the emergence of BR, its expression and stability may be influenced by additional factors beyond bone anatomy, including cortical excitability and local conductivity changes. 2 In patients with epilepsy, the sharp contours and irregular morphology of BR may closely mimic epileptiform discharges, leading to potential diagnostic challenges. 3 Moreover, little is known about how BR behaves when ictal activity arises from or propagates into these regions. In some cases, despite the presence of a skull defect, BR may not be observed, and the typical pattern of fast and sharply contoured rhythms may be absent. 1 Beyond its anatomical foundation, recent clinical observations suggest that BR may also reflect the functional integrity of the underlying cortex. Its presence, absence, or transformation in different physiological states—such as during seizures or in structurally damaged cortical regions—raises the possibility that BR is not merely a static artifact of altered conductivity, but a dynamic marker of cortical viability. 4
In this report, we present a patient with bilateral skull defects, in whom BR was not only modulated by seizure activity but was also absent over the severely injured hemisphere. This case offers new insights into the complex relationship between skull anatomy, cortical function, and the evolving nature of breach rhythm.
Case Report
A 33-year-old man was admitted to the emergency department with frequent generalized tonic–clonic seizures. His medical history was notable for a severe traumatic brain injury at the age of 21, requiring decompressive surgery for a left subdural hemorrhage involving the frontal, parietal, and temporal lobes with midline shift. He also underwent right-sided surgery for parietotemporal bone fractures. Since the trauma, he had experienced recurrent generalized tonic–clonic seizures; however, he had remained seizure-free for six years under levetiracetam 1500 mg twice daily. On admission, he presented with quadriparesis, motor aphasia, and dependence on a nasogastric tube for feeding.
Cranial CT revealed large bilateral skull defects without evidence of new injury (Figure 1). EEG was performed due to seizure recurrence. On the left side, electrodes were placed over scalp regions with underlying bone defects, whereas on the right, the F8, T4, F4, and C4 electrodes were positioned directly over brain tissue without intervening bone. Continuous fast and sharp rhythms were recorded in the F4–C4 region, consistent with BR and diffuse slow waves seen on the left hemisphere with electrode artefacts (Figure 1). During monitoring, two focal seizures with impaired consciousness were captured. Ictal EEG demonstrated rhythmic fast activity at the F8 electrode, followed by alterations in the morphology and rhythmicity of the ongoing F4–C4 BR, which then spread to the left hemisphere. Clinically, these events were characterized by staring and bilateral clonic movements of the chin (Figure 2).
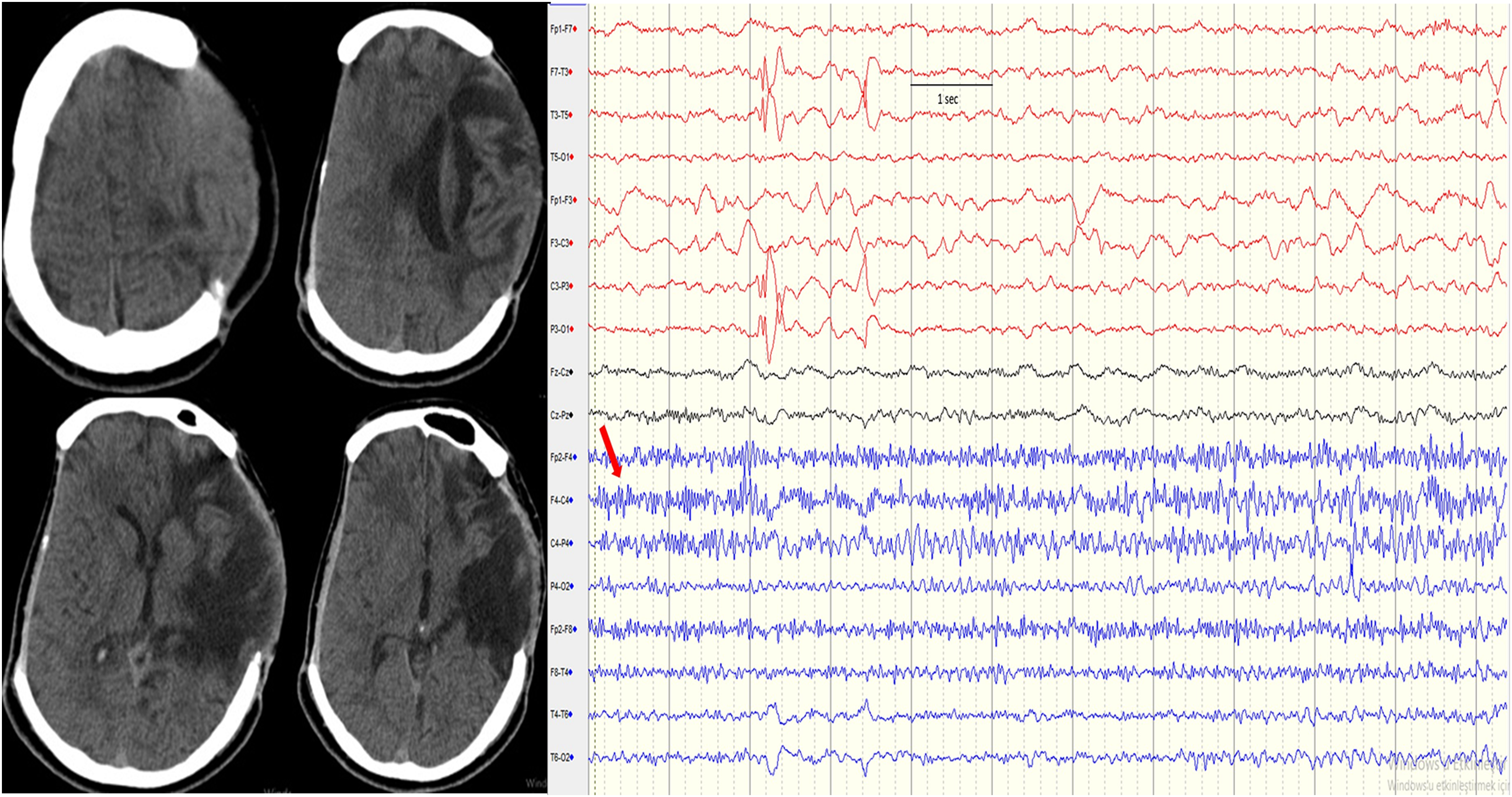
Cranial CT showing bilateral skull defects with bulging of brain tissue on the left side. Breach rhythm (BR) recorded at the F4–C4 electrodes (red arrow). It is also seen that diffuse slowness of left hemisphere and electrode artefacts.
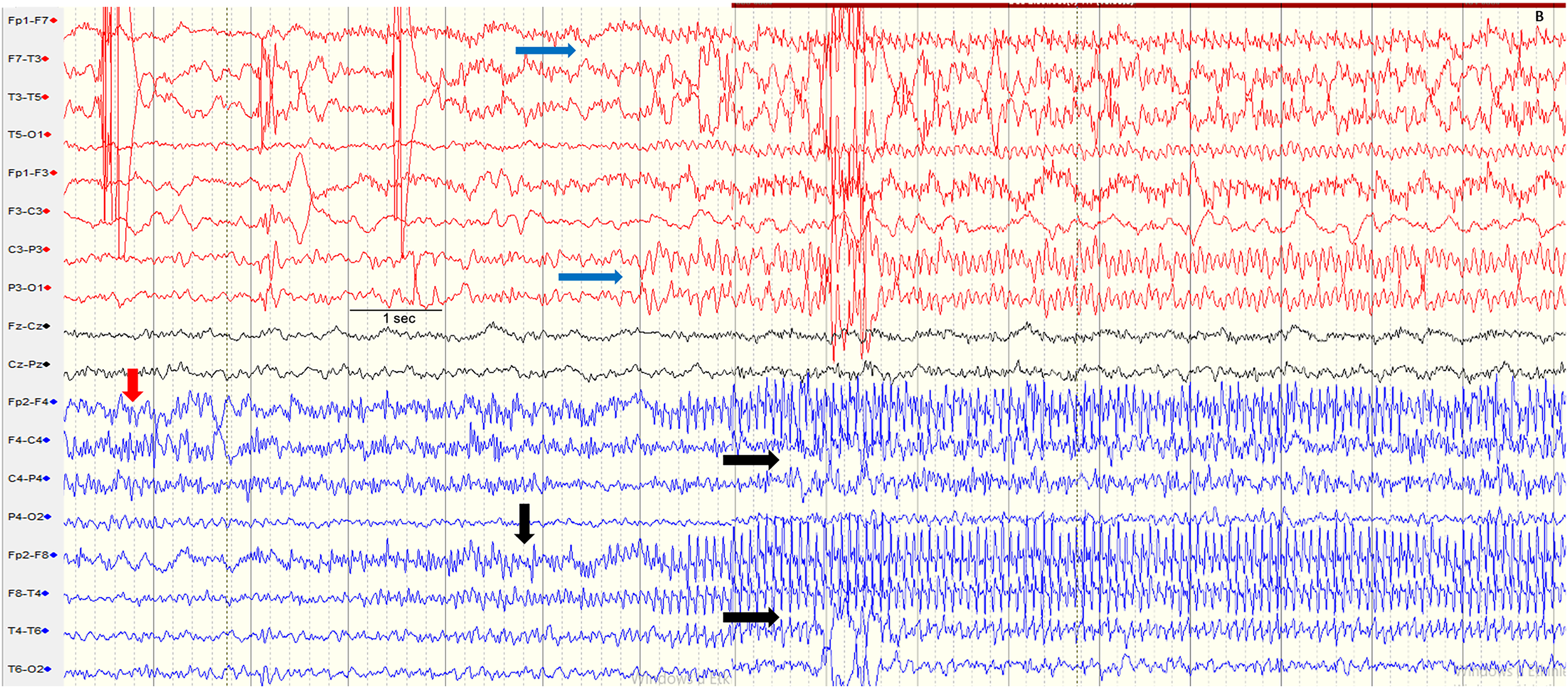
Breach rhythm (BR) recorded at the F4–C4 electrodes (red arrow). Electrographic seizure onset was observed at the F8 electrode as rhythmic fast activity (vertical black arrow), which evolved into rhythmic sharp waves with spread to the right temporal and frontocentral regions (horizontal black arrows), thereby modifying the BR (upper black arrow). Simultaneous propagation to the left hemisphere was also evident (horizontal blue arrows).
EEG monitoring continued for 20 min, after which intravenous phenytoin (20 mg/kg/hour) was administered, and oral phenytoin 100 mg three times daily was added to his ongoing levetiracetam regimen. Laboratory tests revealed a urinary tract infection, and antibiotics were initiated. Following phenytoin infusion, the patient became seizure-free. A repeat EEG on the second hospital day showed only persistent fast and sharp activity localized to the right F4–C4 region, consistent with BR with diffuse slow waves on the left hemisphere as seen in Figure 1. Considering the clinical and laboratory findings, seizures were thought to have been precipitated by infection. The patient was subsequently discharged on combined levetiracetam and phenytoin therapy.
Discussion
BR is a well-recognized EEG phenomenon defined as enhanced or high-amplitude rhythmic activity recorded over skull defects, most often following trauma or surgery. 1 The absence of bone alters the transmission of cortical signals by reducing the smoothing and attenuating effects normally provided by the skull, thereby accentuating faster rhythms such as alpha, beta, and mu. 5 While BR is considered a physiological finding rather than a marker of cortical dysfunction, its sharp and irregular morphology can mimic epileptiform activity, leading to potential diagnostic errors. 6 Several distinguishing features must be considered when interpreting BR. Pure BR is not followed by after-going slow waves, does not spread to other cortical areas, and differs in frequency and amplitude compared to true epileptiform discharges. When a skull defect is broad rather than focal, the fast, sharp, and irregular rhythms of BR may appear more diffusely across the EEG. In such situations, these rhythms can be mistakenly interpreted as ictal seizure activity, particularly in patients with frequent seizures and underlying cortical lesions. However, unlike true ictal discharges, BR does not demonstrate evolution in frequency or amplitude, nor does it spread to other regions.
In our patient, persistent fast and sharp rhythms were recorded in the right F4–C4 region, consistent with BR. These findings fulfilled the classical criteria distinguishing BR from epileptiform discharges. The activity remained stable in this region, without changes in amplitude or frequency, and persisted unchanged after antiepileptic treatment, further supporting its physiological nature. Given the non-standard electrode placement directly over brain tissue on the right, some of the recorded fast activity may reflect an ECoG-like signal rather than typical scalp BR, and thus the interpretation of this pattern requires caution. However, when ictal activity occurred, fast discharges first appeared at the F8 electrode and subsequently altered the morphology and rhythmicity of the ongoing BR in the F4–C4 region as the seizure spread bilaterally. In this context, fast activity replaced the typical sharp BR waves, showing progressive changes in frequency and morphology during seizure evolution. Therefore, while the ictal change in BR appearance is notable, it should be interpreted as most likely reflecting seizure propagation into the region, with true modulation of BR remaining possible but unproven. Interestingly, similar findings have been reported in another case involving inhibitory seizures. 7 In that case, the authors described a patient with a craniotomy and negative seizures in whom BR was suppressed during ictal activity. Following seizure resolution with antiepileptic therapy, the BR re-emerged, highlighting that BR is not solely a result of skull defects but also reflects the functional status of the underlying cortical tissue. Moreover, our case further reinforces this concept. Despite the presence of a large skull defect in the left hemisphere, no BR was observed over that region. We attributed this absence to extensive structural damage in the left hemisphere, which likely impaired the cortical tissue's ability to generate BR. The absence of BR over the left skull defect remains an important observation; however, comparisons between the right and left hemispheres are limited by profound asymmetry in electrode–cortex relationships and thus any side-to-side conclusions must be interpreted with considerable caution. Even so, the lack of BR in a structurally devastated hemisphere is consistent with the concept that viable cortex is required for BR generation, and this case still supports that principle despite technical limitations. As emphasized by Stern and Engel, the appearance of polymorphic delta activity—rather than fast rhythms—over a skull defect should raise concern for cortical injury, 8 a finding that aligns with our patient's history of severe traumatic brain damage. This interpretation is further supported by Kampf et al, who reported a case in which the disappearance of BR heralded tumor progression, again pointing to the importance of underlying cortical function in the expression of BR. 9
Conclusion
Despite the methodological limitations inherent to non-standard electrode placement, this case provides valuable clinical insight into how BR behaves in the context of seizures and structural brain damage. The findings support the concept that BR reflects not only altered skull anatomy but also the functional viability of underlying cortex. Although definitive mechanistic conclusions cannot be drawn from a single case, the observed ictal changes in BR and the absence of BR over severely damaged cortex offer meaningful, hypothesis-generating insights into the dynamic nature of BR.
Footnotes
Acknowledgments
We thank EEG technologist Ayşe Allı Aydın for her assistance in preparing the EEG recordings.
Ethical Approval and Informed Consent Statements
There is no need to take ethic permission for case reports in our University. We have obtained informed consent from the parents of the patient for the publication of this case report.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.