
Abstract
Introduction
Epileptiform K complexes (eKC) and small sharp spikes (SSS) have been explored in a limited number of studies, with their relationhip to epileptic disorders remaining controversial. This retrospective study aimed to evaluate the significance of eKC and SSS in patients with epilepsy for clinical practice.
Methods
Among 370 consecutive patients over the age of 18, who underwent long-term video EEG monitoring, 63 were included based on having at least 20 min of recording after sleep onset and sufficient clinical data. eKC and SSS were visually analyzed by two investigators. Statistical comparisons were made between demographic and clinical data, EEG and neuroimaging features, prognostic evaluations of patients with and without eKC and SSS.
Results
Among the 63 patients investigated, 38.1% exhibited eKC, and 14.3% showed SSS in their sleep recordings, with all affected individuals diagnosed with focal epilepsy syndromes. Compared to patients without eKCs, those with eKCs showed more frequent interictal bilateral slow waves during wakefulness (p = .045), and their ictal EEGs were less lateralized (p = .041). We found that eKCs were more likely to be detected with longer sleep analysis durations (p = .004). In the presence of SSS, ictal EEG was significantly more lateralized (p = .017) and associated with favorable surgical outcomes in patients who underwent epilepsy surgery (p = .015).
Conclusion
Our analysis highlight that eKC and SSS can be present in focal epilepsy syndromes. When considered as an epileptiform EEG phenomenon in drug-resistant epilepsy, these EEG findings may provide additional information during presurgical evaluation and SSS may help to predict surgical outcome.
Introductıon
K complex (KC) was first described by Loomis et al in 1938 as high voltage diphasic slow waves, occurring spontaneously or in response to sudden sensory stimuli, often accompanied by sleep spindles. 1 Later, Nierdermeyer defined epileptic K complexes (eKC) as the overlap of epileptiform discharges and KC in patients with generalized epilepsy.2,3 He termed this abnormal arousal phenomenon either ‘spiky K complexes’ or ‘dyshormia’. 4 Although eKCs were first described in generalized epilepsy,2,3 unilateral focal eKCs have also been reported in focal epilepsies. 5 In these cases, KC-related epileptiform discharges have been found to be ipsilateral to the epileptogenic zone and are more frequent in frontal lobe epilepsy compared with temporal lobe epilepsy. Seneviratne et al reported eKCs in 64% of patients with epilepsy, 6 noting that the occurrence of KC was not influenced by clinical markers, such as epilepsy duration, seizure-free duration, or anti-seizure medication (ASM). 6 This observation suggests that the occurrence of KC is rather intrinsic and independent, supporting the hypothesis that microarousals are responsible for these discharges.
There is no widely accepted objective description or definition for eKCs because they have been investigated in only a limited number of studies. Furthermore, the well-known variable appearance of KC complicates the objective detection of the subtle epileptiform abnormality components associated with this complex. This variability can lead to misinterpretation of pathologic findings as physiological. Additionally, the possible pathologic and diagnostic role of eKCs remains controversial.
Another sleep-related electroencephalography (EEG) variant is small sharp spikes (SSS). These spikes are defined as independent waveforms in the temporal regions with an amplitude of less than 50 millivolts (mV) and a duration of less than 50 milliseconds (ms) during light sleep. They usually appear in the midtemporal region but can also spread to a large area. Although frequently considered a “normal” variant, some studies have reported it as a potential marker for epilepsy, particularly in focal epilepsies.7–9 A case series with concurrent EEG recordings from scalp and depth electrodes demonstrated that SSS on scalp EEG exhibited a time-locked relationship with hippocampal epileptiform discharges recorded using invasive EEG. 10 This finding may be explained by the volume conduction of hippocampal discharges to the scalp EEG. 10
In the light of these data, we aimed to evaluate the clinical significance of sleep-related variants —specifically eKCs and SSS— during long-term video-EEG monitoring (VEM) in patients with epilepsy. Furthermore, we investigated their potential use as markers for lateralization and localization of the epileptogenic zone in focal epilepsies.
Methods
The recordings of consecutive patients who underwent long-term VEM for diagnostic purposes or presurgical evaluation between 2010 and 2020 were reviewed. Patients aged over 18 years with at least 20 min of uninterrupted recordings after sleep onset on VEM were included in this study. Those with insufficent clinical data and patients with only psychogenic seizures were excluded from the study.
Clinical Features
The patients’ demographic features, age of epilepsy onset, seizure types, epilepsy syndrome diagnosis, family history of epilepsy, and the presence of drug-resistant epilepsy were evaluated by the first author and verified by the mentor. Drug-resistant epilepsy is defined as the failure to achieve sustained seizure freedom despite adequate trials of two tolerated and appropriately chosen ASMs whether used as monotherapies or in combination. 11
In patients undergoing epilepsy surgery due to drug-resistance, prognosis was evaluated in the first year post-surgery according to the Engel classification. 12 Engel class I was categorized as a good surgical outcome (no disabling seizures), and Engel classes II-IV were grouped as poor surgical outcomes (ongoing disabling seizures).
Neuroimaging Features
Highly epileptogenic lesions identified on magnetic resonance imaging (MRI), such as hippocampal lesions, cortical encephalomalacia, cortical developmental malformations, and vascular malformations were categorized as epileptogenic MRI findings. In contrast, incidental findings such as arachnoid cysts or nonspecific white matter lesions were not considered. 13 These lesions were compared with the EEG and clinical data for consistency, and their lateralizations were noted for further analysis.
The presence of hypometabolism in positron emission tomography (PET), assessed visually, were classified as normal, right, left, bilateral based on their lateralization.
Neuropsychological Tests
Neuropsychological test results were grouped as normal, lateralized to right (visual memory), lateralized to left (verbal memory), bilateral (visual and verbal memory) and others (mental retardation and frontal lobe dysfunction).
Electrophysiologic Evaluation
Electrophysiologic evaluations were conducted in a detailed and structured manner by the first author and were subsequently verified by the mentors. The key points noted were as follows:
Interictal EEG Evaluation
Interictal slow waves, when present during wakefullnes, are grouped as generalized or focal. Focal discharges are evaluated for lateralizaton (right, left, bilateral, multifocal) and localization (frontal, temporal, parietal, occipital, central and combinations).
Interictal epileptiform discharges, sharp waves, and spike waves were evaluated as epileptiform discharges and were also grouped as generalized or focal. Focal discharges were detailed to localization (frontal, temporal, parietal, occipital, central and near combinations) and lateralization (right, left, bilateral, multifocal).
Ictal Evaluation
Ictal onset:
Lateralized (amplitude difference is at least two times greater than the other hemipshere in reference montages): right/left. Bilateral (amplitude difference is less than twice the other hemipshere in reference montages). Nonlateralized.
Ictal discharge localization
Localized (an amplitude difference of electrodes on the lobe of one hemisphere greater than twice that in bipolar montages). Nonlocalized.
Ictal ending
Lateralization and localization of ictal ending are evaluated.
Ictal ECG
Ictal ECG is grouped into no change/increased/decreased/not evaluated according to awake dominant heart rate. Heart rate increased or decreased was determined if there was at least a 10% increase or decrease in the baseline cardiac rate just before the clinical seizure onset.
14
Postictal Evaluation
During the postictal period, slow wave and paroxysmal discharges were evaluated for lateralization and localization.
KC Evaluation
Well-delineated, negative sharp waves that continue with a positive component standing out from the background EEG, with total duration ≥0.5 s and maximal in amplitude, are accepted as KC. 15 eKCs are defined when a clear spike with a duration less than 70 miliseconds was present on KC (Figure 1). Both KCs and eKCs were counted during the first 20 min of sleep recording.

An example of the epileptic K complex.
Demographic, clinical, electrophysiologic, and neuroimaging results were compared between patients with and without eKCs. The presence of eKCs was also evaluated according to the Engel classification in patients undergoing epilepsy surgery.
SSS Evaluation
SSS was defined as independent sharp waves over the temporal region, with an amplitude <50 microvolts, duration with <50 ms, seen at the beginning of sleep (NREM 1 and 2) (Figure 2). SSS were counted during the first 20 min of sleep. Demographic, clinical, electrophysiologic, and neuroimaging results were compared between patients with SSS and those without.
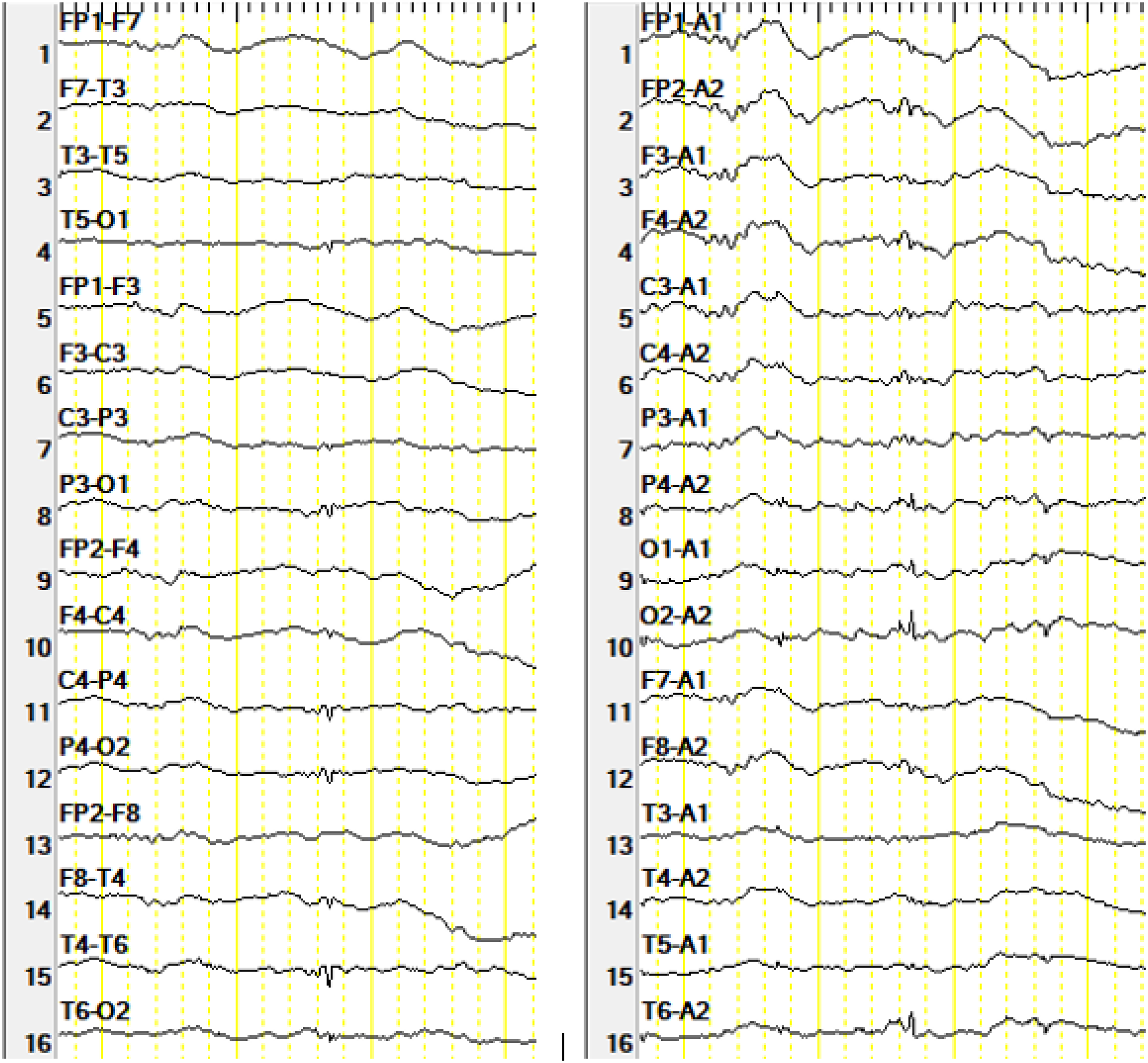
An example of small sharp spikes (marked by arrow): bipolar and avarage montages; sensitivity 10 u V/mm. low frequent filter 1 Hz and high frequency filter 70 Hz.
The relationship of post-operative seizure freedom and presence of SSS was evaluated in patients undergoing epilepsy surgery. Patients with SSS at the same localization with interictal epileptic discharges were also noted.
Ictal Semiology
Careful ictal semiologic evaluation of the recorded seizures, which was dependent solely on the clinical data, was conducted according to the previously reported criteria. 16
Statistical Analysis
Statistical analysis was performed using the SPSS software (Statistical Package for the Social Sciences, version 23.0). Frequency and percentage values for qualitative values, mean and standard deviation, and minimum and maximum values for quantitative variables were calculated. The suitability of the data for normal distribution was tested using the Shapiro-Wilk test. For quantitative variables with normal distribution, Student's t-test or the Mann-Whitney U test was used to compare the ratios of independent groups. The Chi-square test was used to compare the ratios in patient groups without normal distribution. Statistical significance was accepted as p < .05.
Results
A total of 370 patient records were initially identified through a search for patients who underwent VEM between January 2015 and December 2020. According to the exclusion criteria, 32 patients were excluded because they were aged under 18 years, 23 patients for having only psychogenic seizures, and 252 patients due to insufficient storage of recordings for evaluation. The remaining 63 patients who had adequate records to evaluate the interictal, ictal, and postictal periods with at least 20 min sleep recordings and sufficient medical data, were included in the study. The overall demographic and clinical features are presented in Supplementary Table 1. Eighteen (28.6%) patients had focal epilepsy with unknown cause, 43 (68.3%) had symptomatic focal, and only two (3.2%) patients had idiopathic generalized epilepsy.
Neuroimaging and Neuropsychological Test Results
All patients underwent cranial MRI, and epileptogenic lesions were identified in 45 (71.4%) patients. Among the 46 patients who had a PET study, three (7%) showed normal results; the remaining 43 patients had lateralized or bilateral involvement.
Among the 49 (77%) patients who underwent neuropsychological testing, 11 (22%) had normal results, 30 (61%) exhibited lateralized or bilateral dysfunction, and eight (17%) patients had mental retardation.
KC Evaluation
Among the investigated 63 patients, 24 (38.1%) showed eKCs. The clinical features of these patients are presented in Table 1.
The Clinical Features of the Patients with Epileptic K Complexes.
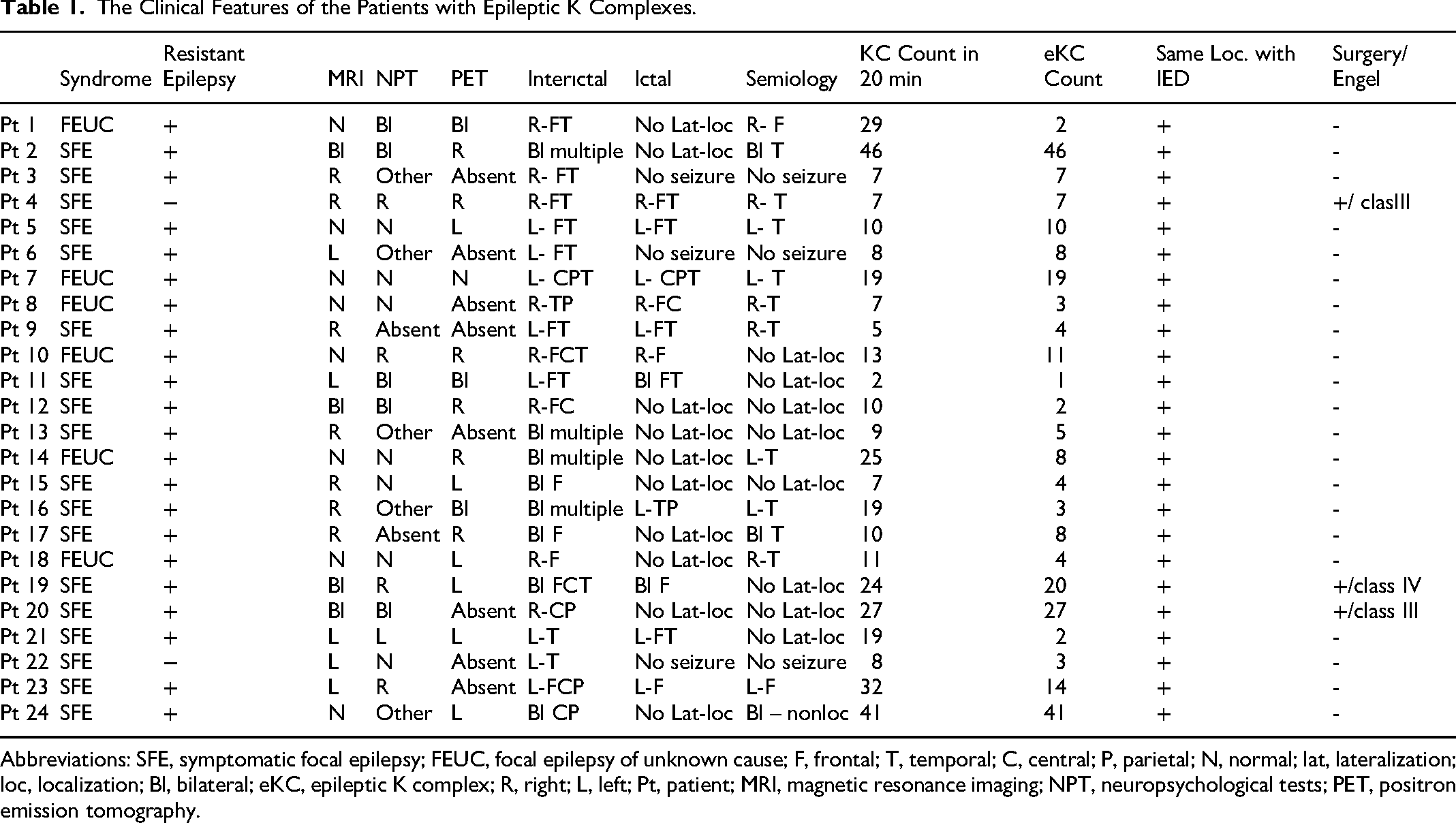
Abbreviations: SFE, symptomatic focal epilepsy; FEUC, focal epilepsy of unknown cause; F, frontal; T, temporal; C, central; P, parietal; N, normal; lat, lateralization; loc, localization; Bl, bilateral; eKC, epileptic K complex; R, right; L, left; Pt, patient; MRI, magnetic resonance imaging; NPT, neuropsychological tests; PET, positron emission tomography.
In all patients with eKCs, the epileptic discharge on KC was located on the same side as the interictal discharge of the same patient (Figure 3). eKC-related epileptic seizures were observed in two patients.
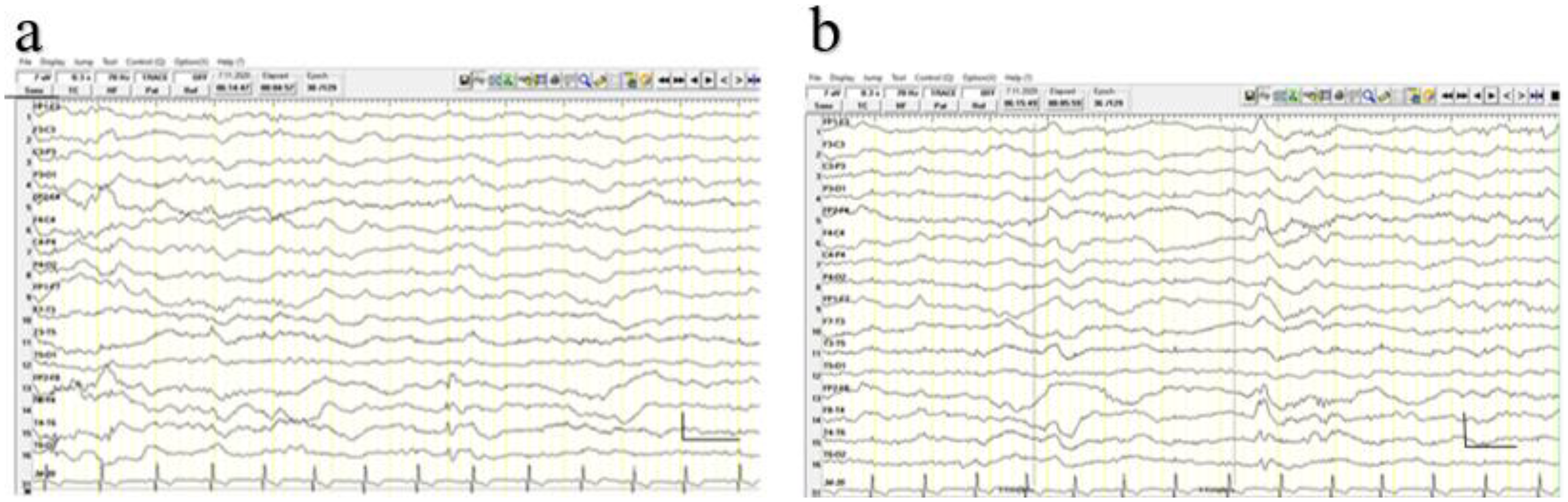
(a) and (b) similar localization of the interictal epileptiform discharge and epileptiform K-complex of the same patient.
The demographic, clinical, and electrophysiologic comparisons between patients with and without eKC are presented in Table 2. The findings revealed that ictal onset and the presence of interictal slow waves were found to be more bilateral, and that the sleep recording time was longer in patients with eKC when compared to the patients without.
The Comparative Features of Patients with and Without Epileptic K Complexes.
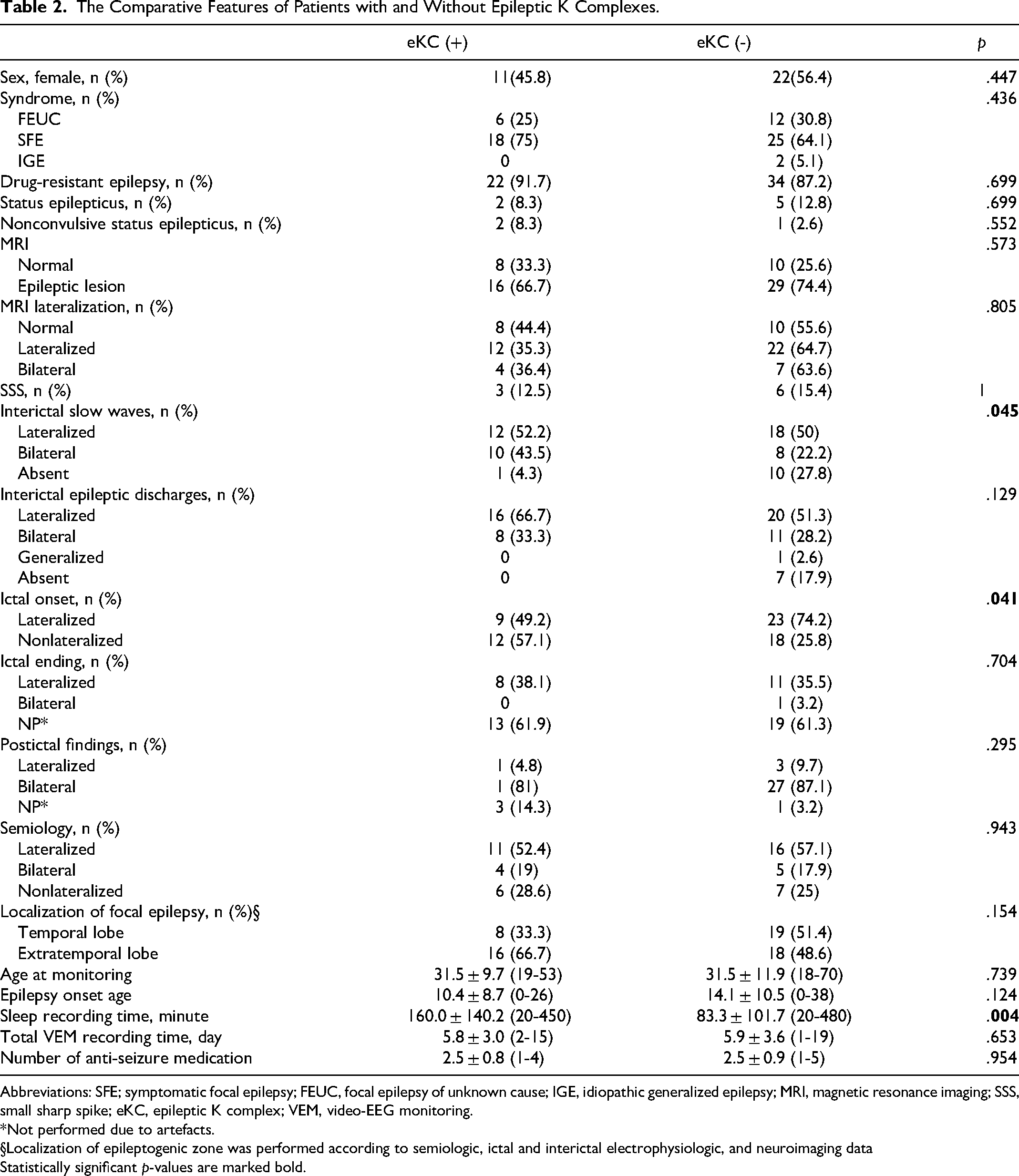
Abbreviations: SFE; symptomatic focal epilepsy; FEUC, focal epilepsy of unknown cause; IGE, idiopathic generalized epilepsy; MRI, magnetic resonance imaging; SSS, small sharp spike; eKC, epileptic K complex; VEM, video-EEG monitoring.
*Not performed due to artefacts.
§Localization of epileptogenic zone was performed according to semiologic, ictal and interictal electrophysiologic, and neuroimaging data
Statistically significant p-values are marked bold.
According to the semiological, electrophysiological and MRI findings, 27 patients have temporal lobe epilepsy (TLE) and 34 patients have extratemporal lobe epilepsy (ETLE). The eKC were present in 8 of 27 TLE patients and 16 of 34 ETLE patients. Amoung ETLE patients, only five have frontal lobe epilepsy (FLE). eKC was found in 2 of 5 FLE patients. The presence of eKC did not differ among subgroups according to the localization (temporal vs extratemporal, Table 2).
SSS Evaluation
SSS were observed in nine of the 63 patients (Table 3). SSS were lateralized to the left in seven (77.8%) patients and in eight of nine patients with SSS; epileptiform discharges demonstrated the same lateralization when awake. There was no significant relationship regarding the syndrome, EEG features, MRI findings, and semiology between the patient groups with SSS who exhibited epileptic discharges ipsilateral or contralateral to SSS.
Features of Patients with Small Sharp Spike.
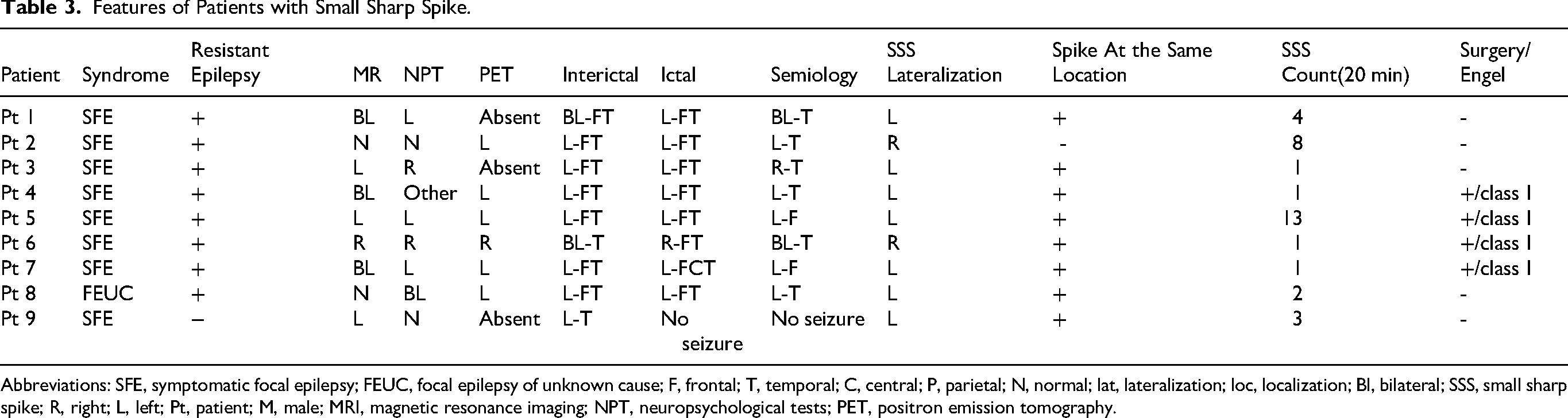
Abbreviations: SFE, symptomatic focal epilepsy; FEUC, focal epilepsy of unknown cause; F, frontal; T, temporal; C, central; P, parietal; N, normal; lat, lateralization; loc, localization; Bl, bilateral; SSS, small sharp spike; R, right; L, left; Pt, patient; M, male; MRI, magnetic resonance imaging; NPT, neuropsychological tests; PET, positron emission tomography.
None of the investigated parameters were found to be significantly different between patients with and without SSS, except for ictal onset which was significantly more lateralized in patients with SSS compared with those without (Table 4).
The Comparative Features of Patients with and Without Small Sharp Spikes.
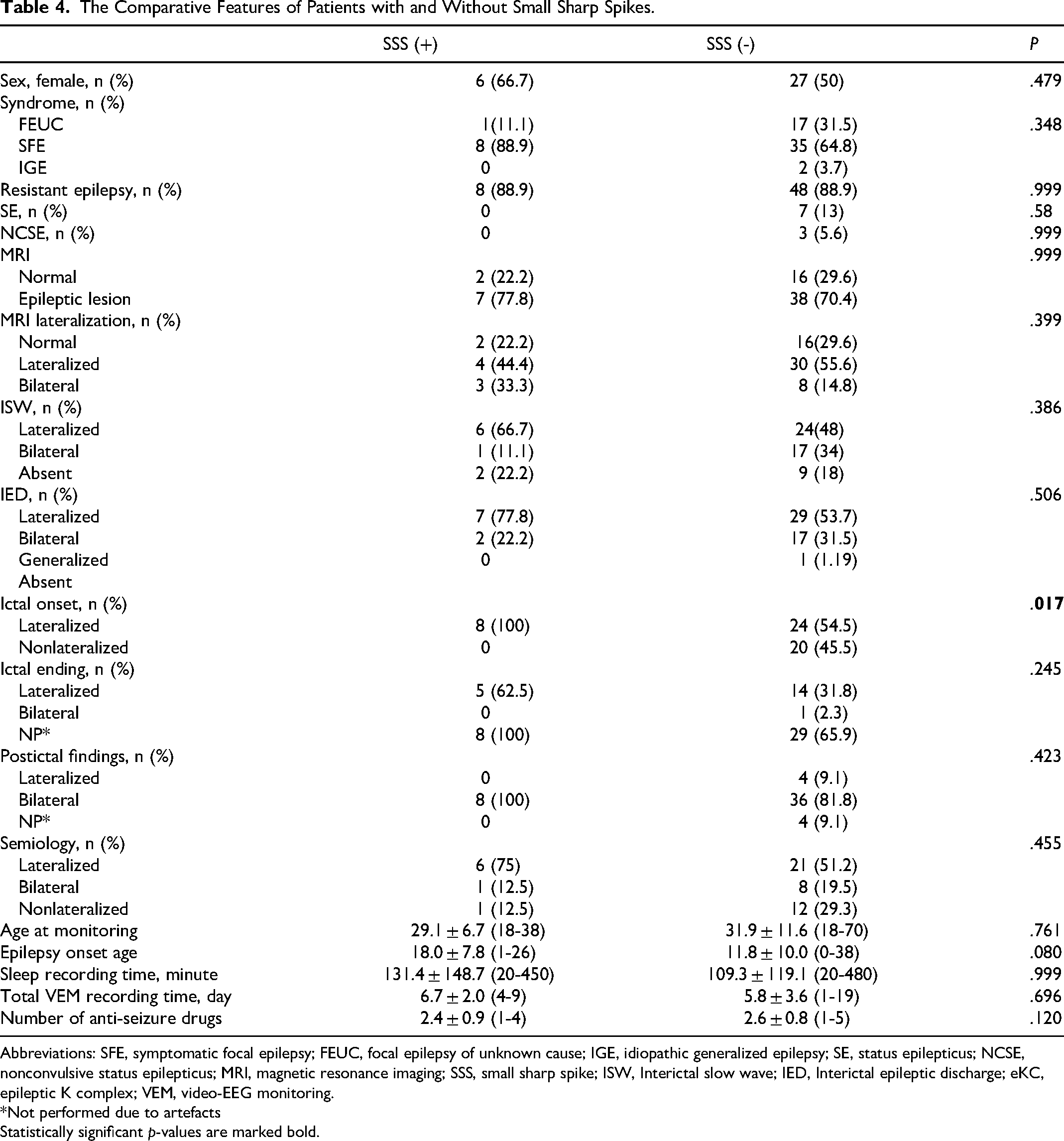
Abbreviations: SFE, symptomatic focal epilepsy; FEUC, focal epilepsy of unknown cause; IGE, idiopathic generalized epilepsy; SE, status epilepticus; NCSE, nonconvulsive status epilepticus; MRI, magnetic resonance imaging; SSS, small sharp spike; ISW, Interictal slow wave; IED, Interictal epileptic discharge; eKC, epileptic K complex; VEM, video-EEG monitoring.
*Not performed due to artefacts
Statistically significant p-values are marked bold.
Prognostic Evaluation
Invasive EEG was performed in only two (3.2%) patients, and 11 (17.5%) patients underwent epilepsy surgery - temporal lobectomy in six patients, callosotomy in one patient, and lesionectomy in four patients. The prognosis after epilepsy surgery did not differ based on the presence of eKCs; however, patients with SSS (four with Engel 1 and none with Engel II-IV vs one with Engel 1 and six with Engel II-IV; p = .015) tended to have a better prognosis compared with those without (Supplementary Table 2).
Discussion
In contrast to certain studies, our research demonstrates that eKCs are also evident in focal epilepsies, which is consistent with observations reported in additional literature.5,6,17,18 The number of our patients with IGE was limited beacuse the majority of patients undergoing long-term VEM typically presented with drug-resistant focal epilepsy and were referred for presurgical evaluation. Most patients in our cohort were on polytherapy, and it is possible that ASMs may suppress eKCs, similarly with other interictal epileptiform discharges. 19 However, in our study, the number of ASMs did not differ between patients with and without eKCs. Nevertheless, the potential influence of various ASM combinations and dosages cannot be fully excluded. In our study, 38% of the patients with focal epilepsy exhibited eKCs and the localization of additional focal epileptic discharges during KCs was consistent with their usual interictal epileptiform discharges. This finding supports the hypothesis that discharges occurring during KC would show the same localization and lateralization values as interictal epileptiform discharges. Similar results were reported in Geyer et al's study, which involved 40 patients with focal epilepsy grouped according to their localization and 40 control subjects. During each day of monitoring, the first 20 min of stage 2 sleep were analyzed by the authors, similar to our method. The presence of eKCs was investigated for each patient, and were detected in 11 (27%) of the 40 patients. They also found that the discharges during KC were ipsilateral to ictal onset and concluded that eKCs could be helpful in defining the epileptogenic zone, 5 supported by our data.
Although the lateralization of interictal epileptiform discharges did not differ between patients with and without eKCs, slow waves were more frequent and predominantly bilateral in those with eKCs. Moreover, nonlateralizing ictal onsets were commonly observed in the eKC-positive group. It can be hypothesized that these novel electrophysiologic findings may indicate that epilepsy in patients with eKCs involves more widespread hemispheric networks, potentially related to the mechanisms underlying K-complex generation. Nevertheless, no other quantitative network-measuring tools, such as quantitative EEG, functional MRI or PET, were utilised in this study. Consequently, the potential influence of epileptic networks on K-complexes could not be elucidated. The discordance between ictal and interictal EEG findings may be explained by the theorotical zones in epilepsy. 20
In accordance with previously reported findings, there was no relationship between clinical features and eKCs in our study.19,21 Additionally, we examined detailed EEG findings as ictal onset, ictal ending, and postictal EEG features, neuroimaging, and semiologic findings, but no significant results were observed. Notably, the longer duration of sleep recordings in patients with eKCs compared with those without underscores the importance of extended sleep recordings in the evaluation of these patterns.
In our study, SSS was observed in 9 patients (14.3%) with focal epilepsy, and ipsilateral interictal epileptic discharge was detected in all but one patient. We found no relationship between SSS and clinical variables, except in patients who underwent epilepsy surgery. Interestingly, patients with SSS tended to have better surgical outcome than those without. Among the EEG features, ictal onset was significantly more lateralized in patients with SSS. These two notable findings underscore the potential value of SSS in the lateralization of the epileptogenic zone, thereby contributing to the selection of appropriate surgical candidates. Although small sample size restricts its prognostic interpretation, SSS may serve as a potential prognostic marker for favorable surgical outcomes.
Although SSS are accepted as a ‘benign’ variant in EEG practice, some studies have reported SSS as an epileptiform pattern due to similar incidences observed in patients with epilepsy,22–24 along with a high incidence of seizure rates in their presence.7,9,25 Controversial results have also been found in intracranial EEG recordings. Westmoreland et al found that SSS are time-locked to intracerebral discharges originating from a widespread area in deep structures; however, these discharges were not always co-localized to the seizure onset zone. 26 Another interesting study conducted by Issa et al analyzed simultaneous scalp and intracranial recordings from 27 patients retrospectively and found time-locked hippocampal discharges in 15 patients. 10 In a similar recent study of Bruzzone et al, 20 patients with temporal lobe epilepsy (TLE) who has scalp and intracranial EEG recordings were evaluated and demonstrated that hypocampal spikes were associated with morphologically heterogenous corrolates including small sharp spikes. 27 These results indicate that SSS may have various intracranial correlates, and a need for further prospective larger studies.
The clinical and electrophysiological significance of SSS remains controversial, especially in nonepileptic patients. There is a need for further investigations if nonepileptic patients will develop epilepsy in follow up which raises the possibility that these patients are likely in the latent period. 28
In a retrospective study with a large population that underwent VEM recordings, 542 patients (59.6%) were diagnosed as having epilepsy, and 110 patients (12.1%) had SSS, similar to our rate. Focal epilepsy was the most frequent epilepsy syndrome type. Similar to our findings, interictal epileptic discharges were significantly ipsilateral to SSS. 29 This observation highlights the high lateralization value of SSS in determining the epileptogenic zone, supporting our results. The presence of SSS in patients with drug-resistant focal epilepsy may contribute to a more accurate pre-surgical evaluation and increase the likelihood of favorable postoperative outcomes. However, no robust conclusions can be drawn due to limited sample size of patients with SSS.
The present study has several limitations. First, its retrospective design inherently limits the ability to establish causality and may introduce selection bias. Although the results are valuable, the overall sample size (63 patients with focal epilepsy) limits the statistical power of the study and precludes to perform certain subgroup and multivariate analyses. Furthermore, the small number of patients with IGE restricts interpretation and generalizability of the findings to this subgroup, warranting further validation in larger, prospective cohorts. Secondly, without a non-epileptic comparison group, missing in our cohort, it is difficult to determine the specificity of eKC and SSS as epileptiform markers and distinguish them from benign sleep variants. Another limitation is the lack of longer and more comprehensive sleep recordings, which could have provided a better representation of all interictal patterns. Furthermore, sleep recording durations were not standardized across all patients, potentially affecting the detection of sleep-related patterns. Finally, SSS and KC were evaluated visually by a researcher who was not blinded to the clinical data, although assessments were supervised by experienced mentors, introducing a potential observer bias. The inter-rater reliability analyses also have not been performed. In addition, automated detection validation, which could have improved objectivity and reproducibility, were not employed.
Conclusions
In conclusion, eKCs and SSS can be observed in focal epilepsy syndromes and may serve as potential EEG markers for epilepsy, pending further validation through future studies. eKc may possess similar localization and lateralization values as interictal epileptiform discharges, potentially aiding in the identification of the epileptogenic zone in patients with focal epilepsy. Moreover, the lateralization value of SSS could contribute to selecting appropriate candidates for epilepsy surgery and may serve as a predictive marker for favorable surgical outcomes.
Supplemental Material
sj-docx-1-eeg-10.1177_15500594261425525 - Supplemental material for Are Epileptic K-Complexes and Small Sharp Spikes During Sleep Clinically Useful in the Evaluation of Epileptic Patients? Important Phenomenology Needs Consideration
Supplemental material, sj-docx-1-eeg-10.1177_15500594261425525 for Are Epileptic K-Complexes and Small Sharp Spikes During Sleep Clinically Useful in the Evaluation of Epileptic Patients? Important Phenomenology Needs Consideration by Havva Tuğba Çelik, Nermin Gorkem Sirin, Nerses Bebek and Betül Baykan in Clinical EEG and Neuroscience
Supplemental Material
sj-docx-2-eeg-10.1177_15500594261425525 - Supplemental material for Are Epileptic K-Complexes and Small Sharp Spikes During Sleep Clinically Useful in the Evaluation of Epileptic Patients? Important Phenomenology Needs Consideration
Supplemental material, sj-docx-2-eeg-10.1177_15500594261425525 for Are Epileptic K-Complexes and Small Sharp Spikes During Sleep Clinically Useful in the Evaluation of Epileptic Patients? Important Phenomenology Needs Consideration by Havva Tuğba Çelik, Nermin Gorkem Sirin, Nerses Bebek and Betül Baykan in Clinical EEG and Neuroscience
Footnotes
Ethical Considerations
This study was approved by the Istanbul University, Istanbul Faculty of Medicine, Ethics Committee (25.09.2020/1274) and informed consent was obtained from each subject
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Bilimsel Araştirma Projeleri Birimi, Istanbul Üniversitesi, (grant number Project No. TYL-2021-37660).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
Data available on request from the corresponding author.
Supplemental Material
Supplemental material for this article is available online.