
Abstract
Background
Brain–computer interface-driven functional electrical stimulation (BCI-FES) is a promising approach for post-stroke upper limb rehabilitation. However, considerable variability exists in stimulation parameters and task designs across studies, and evidence remains insufficient to support definitive protocol recommendations.
Methods
We searched PubMed, Embase, Web of Science, and the Cochrane Library for randomized controlled trials (RCTs) up to September 2025. Eligible studies applied BCI-FES and reported the Fugl-Meyer Assessment for the upper extremity (FMA-UE). Risk of bias was assessed with the PEDro scale, and evidence certainty graded with GRADE. Random-effects meta-analyses were performed.
Results
Twelve RCTs (n = 619) showed BCI-FES improved FMA-UE scores versus controls (MD = 5.82, 95% CI 3.04-8.59, p < 0.00001; I2 = 39%), with larger benefits in subacute stroke (MD = 8.45). Dynamic-threshold paradigms and motor imagery were associated with higher effect sizes. Higher stimulation frequency (>50 Hz), narrow-pulse width (150 µs) more frequent sessions (≥5/week), shorter session duration (≤30 min), greater total sessions (>20), and longer intervention (>4 weeks) tended to be associated with larger effect sizes, though evidence is limited and based on few studies. Secondary outcomes (ARAT, WMFT, MBI) improved, and no serious adverse events were reported. Evidence certainty was moderate.
Conclusion
BCI-FES was associated with improvements in upper limb motor recovery after stroke, especially in subacute patients. Some stimulation and training features may relate to greater effects, but current evidence remains insufficient for definitive clinical guidance. Larger multicenter RCTs are needed to clarify dose-response relationships and support biomarker-guided, personalized interventions.
Keywords
Introduction
Stroke is a major global health burden, characterized by high incidence, disability, mortality, recurrence, and substantial socioeconomic costs. It ranks as the second leading cause of death and the third leading cause of disability among adults worldwide, with one in four individuals experiencing a stroke during their lifetime. 1 According to Global Burden of Disease data, the absolute incidence of stroke increased by 70% and its prevalence by 85% between 1990 and 2019. 2 Approximately two-thirds of stroke survivors suffer from persistent upper limb motor impairment after the acute phase, typically presenting as loss of voluntary control of the shoulder, elbow, and wrist joints, along with deficits in fine finger movements, which markedly compromise daily activities. 3 Current rehabilitation practices for post-stroke upper limb dysfunction remain dominated by “passive-assisted” approaches,4,5 such as repetitive passive exercises and single-modality interventions including electrical or magnetic stimulation.6,7 While these approaches may support peripheral recovery, evidence from comparative studies of passive and active training paradigms suggests that passive-assisted approaches are associated with relatively limited engagement of central neural circuits, as reflected by weaker neuroplastic changes and less pronounced neural network remodeling.8,9These limitations are particularly relevant for patients with severe deficits or absent voluntary movement.4,10 Consequently, developing rehabilitation paradigm that integrates “central-peripheral closed-loop” mechanisms and promote “active-passive synergy” remains a critical challenge.
Brain computer interface (BCI) is an emerging neurorehabilitation technology that enables real-time recording and decoding of motor intentions, thereby driving external devices to execute movements synchronized with the user's intent. This creates an active training closed loop of “mind-driven action”. 11 Unlike conventional approaches that rely on peripheral neural and muscular pathways, BCI directly leverages neural activity to control external devices for therapeutic purposes. It is regarded as a promising strategy to overcome the limitations of passive rehabilitation and to foster active engagement in recovery. 12 Among peripheral effectors, functional electrical stimulation (FES) is the most widely integrated with BCI systems. 13 BCI-FES technology decodes cortical potentials elicited by motor imagery to trigger muscle-specific stimulation in real time, thereby establishing “central-peripheral-central” closed-loop feedback. This mechanism reinforces cortical α/β-event-related desynchronization (ERD) and cerebral hemodynamics, and through synaptic plasticity and mirror neuron mechanisms, promotes functional reorganization of the sensorimotor network.14,15
Although BCI-FES has been extensively investigated for post-stroke upper limb rehabilitation, its clinical efficacy remains inconclusive. Several RCTs and systematic reviews have demonstrated significant improvements in FMA-UE scores, with benefits sustained for 6 months or longer,16,17 whereas other studies reported no significant between-group differences. 18 This inconsistency largely reflects heterogeneity in outcome measures, training dosage, and control protocols. Consequently, there is an urgent need to harmonize assessment tools and intervention parameters, and to conduct registered systematic reviews and individual patient data meta-analyses. Such efforts are essential to generate high-quality evidence that can inform guideline development and clinical translation.
The aims of this meta-analysis were threefold: (1) to evaluate the clinical efficacy of BCI-FES in enhancing upper limb motor recovery after stroke; (2) to identify potential moderators of treatment effects, including control intervention type, stroke phase, training intensity, and specific BCI and FES parameters; and (3) to explore associations between BCI-FES protocol features and clinical outcomes in patients with post-stroke upper limb motor impairment.
Methods
This systematic review and meta-analysis was conducted in accordance with the PRISMA 2020 statement. 19 The study protocol was prospectively registered in PROSPERO (CRD420251139639). All procedures adhered to the 27-item PRISMA 2020 checklist 20 to ensure methodological transparency and reproducibility (Supplementary Table S1).
Search Strategy and Selection Criteria
A systematic search of PubMed, Cochrane Library, Web of Science, and Embase was conducted in September 2025 by a professional librarian. Search terms, strategies, and selection criteria were guided by the PICOS framework and tailored for each database (Supplementary Table S2). No language restrictions were applied; however, all abstracts were in English. In addition, a final updated search was conducted immediately prior to manuscript submission to ensure inclusion of the most recent evidence, and no additional eligible studies were identified.
Studies were included if they met the following criteria:
Study design: randomized controlled trials (RCTs); Participants: adults (≥18 years) with stroke, irrespective of stroke type (ischemic or hemorrhagic) or stage (subacute or chronic); Intervention: BCI-driven functional electrical stimulation (BCI-FES), with or without conventional rehabilitation, but without additional active interventions. Comparator: sham BCI-FES, conventional rehabilitation, or FES alone; Outcome: reporting of Fugl-Meyer Assessment for the upper extremity (FMA-UE) scores.
Exclusion criteria were as follows:
Non-randomized studies (eg, observational studies, case series, or quasi-experimental designs); Conference abstracts, reviews, protocols, or duplicate publications; Studies with incomplete or non-extractable outcome data, including those not reporting FMA-UE results ; Studies with unclear or insufficiently described BCI-FES interventions; Trials combining BCI-FES with additional active interventions beyond standard rehabilitation (eg, transcranial magnetic stimulation, transcranial direct current stimulation, robotic-assisted therapy), where the independent effect of BCI-FES could not be isolated.
Study Selection and Data Extraction
Study selection was independently performed by two researchers. After removal of duplicates, conference abstracts, and other ineligible records, titles and abstracts were screened, followed by full-text review of potentially relevant studies. Discrepancies were resolved through discussion or adjudication by a third researcher, with consensus meetings held if necessary. Overlapping datasets were represented by the most complete report. For studies reporting outcomes at multiple time-points, data from the endpoint closest to the end of the intervention were used.A standardized data extraction form was employed to collect study characteristics and outcome data. Given the variability in assessment tools and data reporting across studies, mean and standard deviation (SD) values were extracted when reported. When SDs were not available, they were derived from 95% confidence intervals (95% CI) or estimated from change scores using standard formulas assuming a baseline-post-intervention correlation coefficient of 0.7, in accordance with the Cochrane Handbook for Systematic Reviews of Interventions. For studies reporting medians and interquartile ranges (IQR), values were converted using the formulas: mean ≈ median, SD ≈ IQR × 1.35.



Quality Assessment and Assessment of Risk of Bias
The methodological quality of included studies was evaluated using the Physiotherapy Evidence Database (PEDro) scale, 21 which comprises 11 items addressing randomization, blinding, allocation concealment, intention-to-treat analysis, and data reporting. Total scores range from 0 to 10, with >=9 classified as “excellent,” 6–8 as “good,” 4–5 as “fair,” and <4 as “poor.” Overall evidence quality and the strength of recommendations were assessed using the GRADE framework, which categorizes evidence as very low, low, moderate, or high. Risk of bias was additionally assessed using the Cochrane Risk of Bias (ROB) tool, with results recorded in Review Manager 5.4. All evaluations were conducted independently by two researchers, with disagreements resolved by discussion to achieve consensus.
Statistical Analysis
For continuous outcomes, post-intervention values or change scores (mean ± SD) were pooled for the BCI-FES and control groups. Effect sizes were expressed as mean differences (MD) with 95% confidence intervals (CI). Heterogeneity was assessed using the I2 statistic. Considering the conceptual and clinical heterogeneity across studies, all pooled analyses were performed using a random-effects model (DerSimonian-Laird), irrespective of I2 values, to provide more conservative effect estimates. Potential publication bias and small-study effects were evaluated using visual inspection of funnel plots, Egger's regression test, and calculation of the fail-safe N. Pre-specified subgroup analyses included: (1) Stroke phase (subacute ≤6 months vs chronic >6 months); (2) Control intervention (sham BCI, conventional therapy, FES alone); (3) Training intensity (session duration, weekly frequency, total intervention weeks); (4) FES parameters (stimulation site, intensity); (5) BCI parameters (threshold adjustment strategy, type of mental task).FMA-UE was the outcome measure for all subgroup analyses. Sensitivity analyses were performed to assess the robustness of the pooled estimates to assumptions related to variance imputation. Studies that did not directly report raw outcome data or mean ± standard deviation (SD) values and required SD estimation using transformation formulas were excluded. The results were compared with the primary analyses to evaluate the potential impact of these assumptions.
Results
Search Results
Systematic searches of PubMed, Embase, Cochrane Library, and Web of Science up to September 2025 yielded 4059 records. After removing duplicates, books, letters, preprints, and conference proceedings, 1920 studies remained. Initial screening of titles and abstracts reduced this number to 236 articles for full eligibility assessment. Following full-text review, 12 studies were included in the meta-analysis. The study selection process is illustrated in Figure 1.
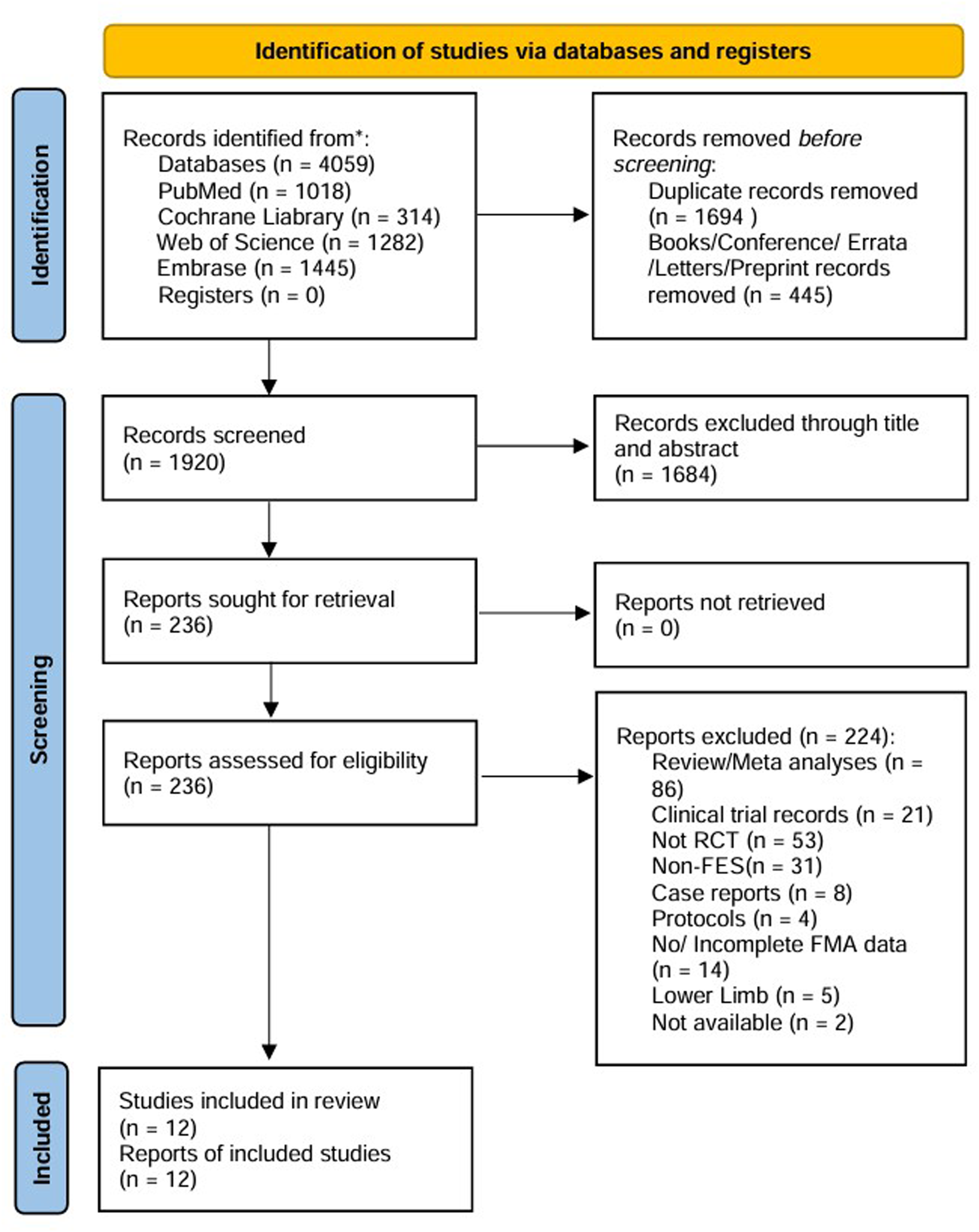
PRISMA flow diagram of study selection.
Characteristics of Studies
The 12 included studies were published between 2014 and 2025 and involved a total of 619 patients (309 in the BCI-FES group and 310 in the control group). Control interventions comprised FES in four studies, sham BCI training in three studies, and conventional rehabilitation in the remaining studies. BCI training durations ranged from 3 days to 6 weeks, with 2–3 sessions per week, and individual session durations ranged from 20 to 90 min, most commonly 30 min. All studies reported the Fugl-Meyer Assessment for the upper extremity (FMA-UE) as a primary outcome. Secondary outcomes included the Action Research Arm Test (ARAT), Modified Barthel Index (MBI), and Wolf Motor Function Test (WMFT), assessing upper limb motor performance, functional capacity, and activities of daily living. Detailed characteristics are provided in Table 1 and Supplementary Tables S3-S4.
Characteristics of the Included Studies.
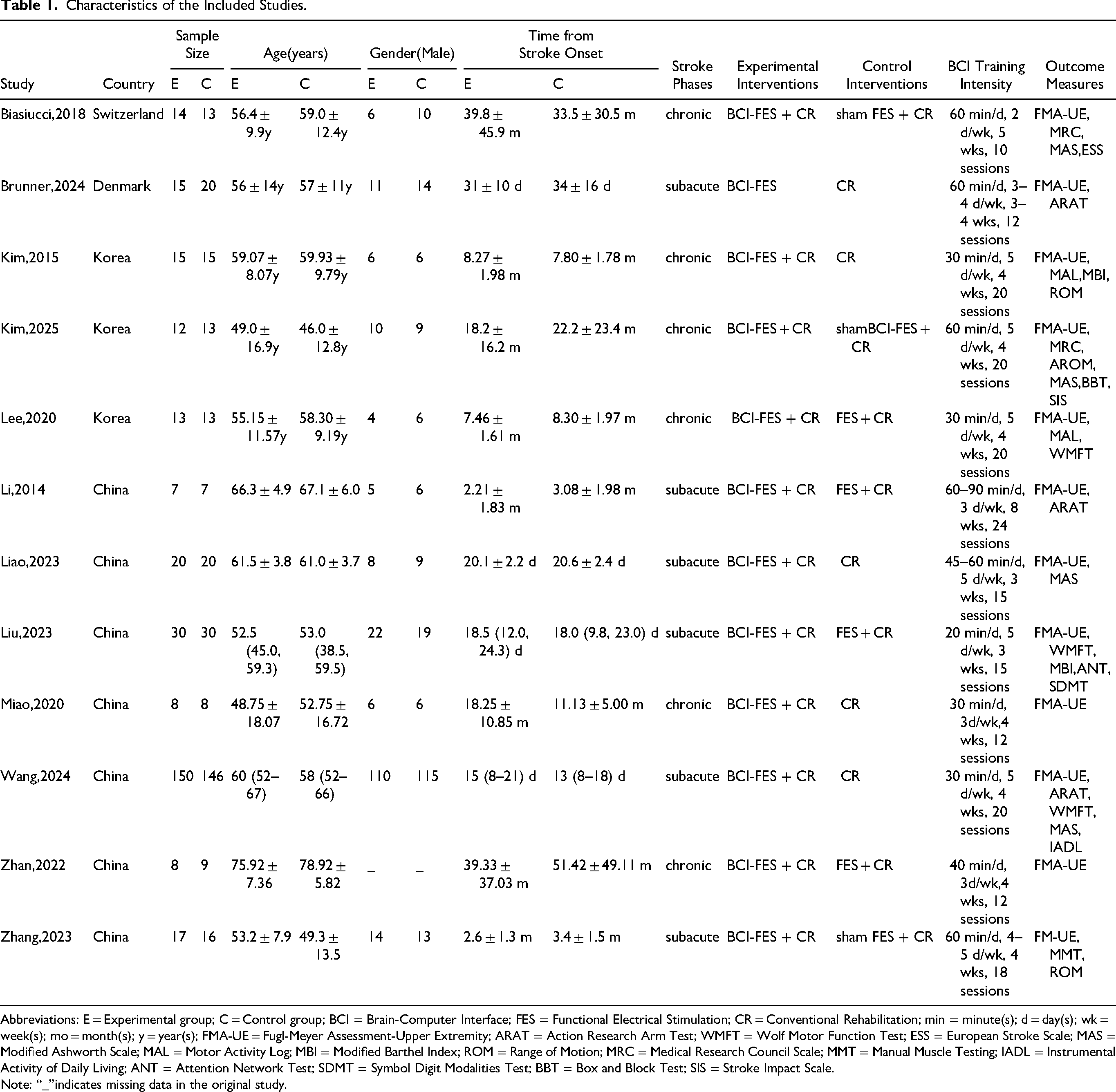
Abbreviations: E = Experimental group; C = Control group; BCI = Brain-Computer Interface; FES = Functional Electrical Stimulation; CR = Conventional Rehabilitation; min = minute(s); d = day(s); wk = week(s); mo = month(s); y = year(s); FMA-UE = Fugl-Meyer Assessment-Upper Extremity; ARAT = Action Research Arm Test; WMFT = Wolf Motor Function Test; ESS = European Stroke Scale; MAS = Modified Ashworth Scale; MAL = Motor Activity Log; MBI = Modified Barthel Index; ROM = Range of Motion; MRC = Medical Research Council Scale; MMT = Manual Muscle Testing; IADL = Instrumental Activity of Daily Living; ANT = Attention Network Test; SDMT = Symbol Digit Modalities Test; BBT = Box and Block Test; SIS = Stroke Impact Scale.
Note: “_”indicates missing data in the original study.
Methodological Quality and Risk of Bias
The methodological quality of included studies was evaluated using the PEDro scale (Supplementary Table S5), with scores ranging from 4 to 9 (mean 6.92 ± 1.38). One study was classified as “excellent,” nine as “good” (≥6 points), and two as “fair”; no study was rated “poor.” Risk of bias assessments are shown in Figures 2 and 3. Most studies were judged to have low risk of bias for random sequence generation, selective reporting, and other domains, while allocation concealment and participant blinding were frequently rated as unclear or high risk. This potential performance bias may have influenced observed effect sizes and contributed to the downgrade of evidence certainty in the GRADE assessment.
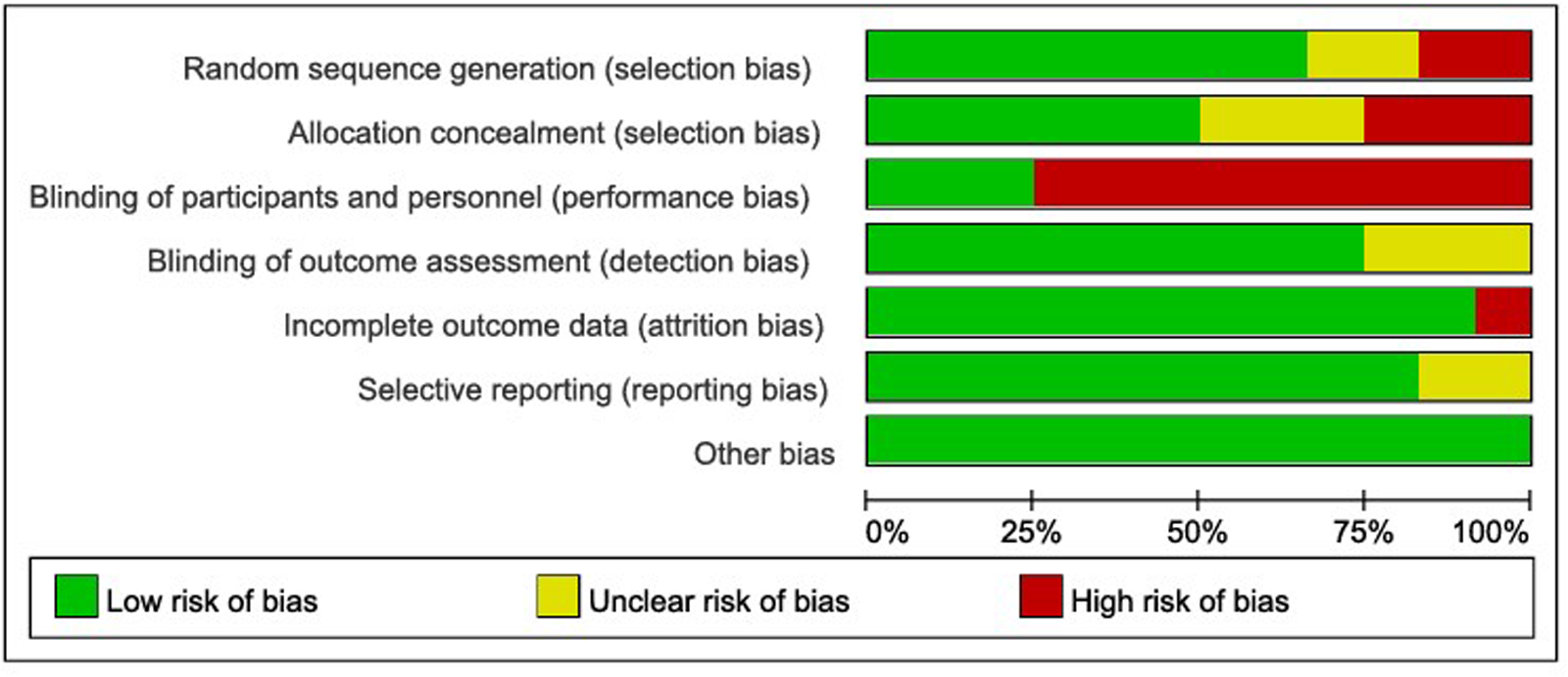
Risk of bias graph.
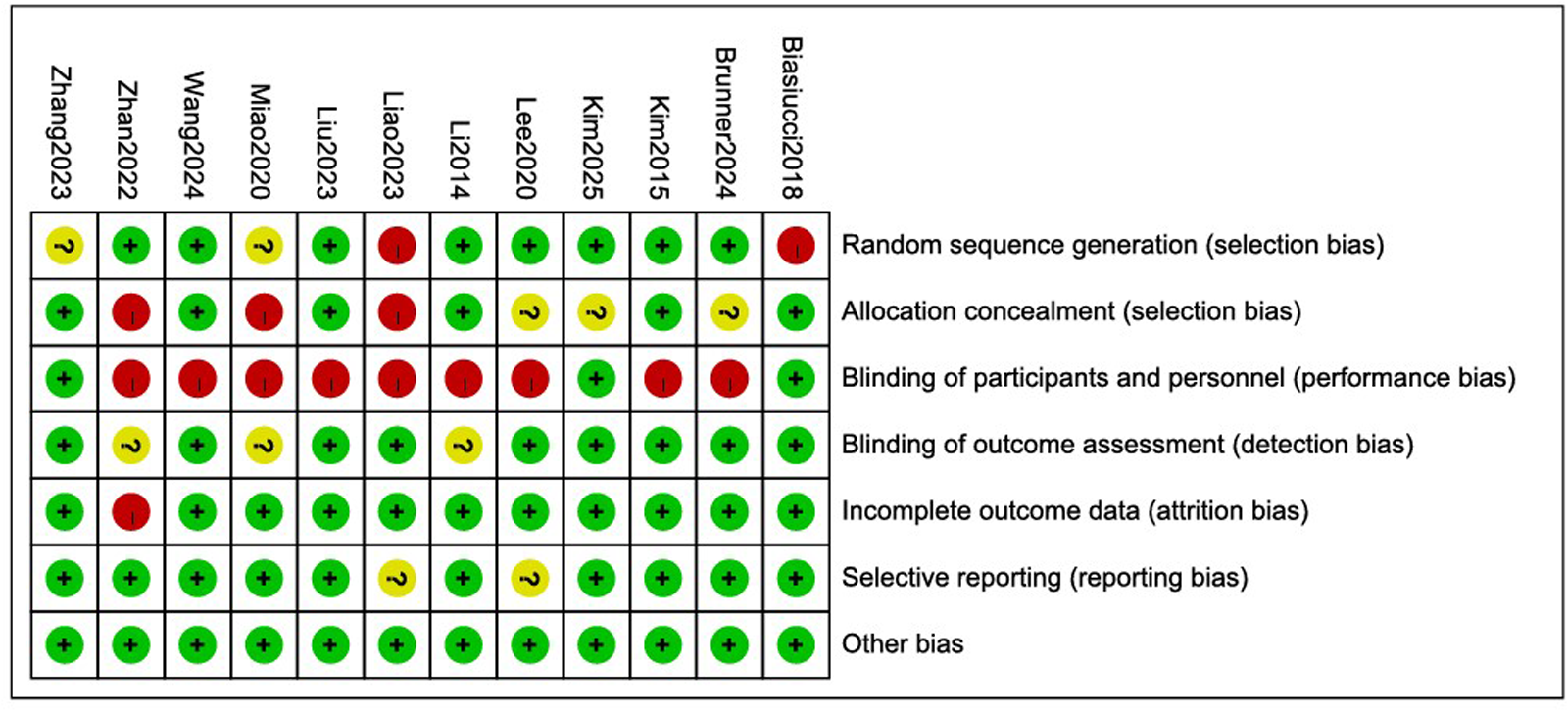
Risk of bias summary.
Effects on Functional Outcomes
FMA-UE
The meta-analysis of FMA-UE included 12 RCTs. Pooled results indicated that BCI-based interventions were associated with greater improvements in FMA-UE scores compared with controls (MD = 5.82, 95% CI 3.04-8.59, P < 0.00001; I2 = 39%, P = 0.08) (Figure 4). Sensitivity analysis excluding three studies lacking direct reporting of raw data or mean ± SD values for FMA-UE (Supplementary Figures S2–S3) yielded consistent results (random-effects model, MD = 4.81, 95% CI 1.74-7.88, P = 0.002). Analysis of pre-to post-treatment changes showed an average improvement of 4.11 points in FMA-UE scores (MD = 4.11, 95% CI 2.67-5.54, P < 0.00001) (Supplementary Figures S4–S5).
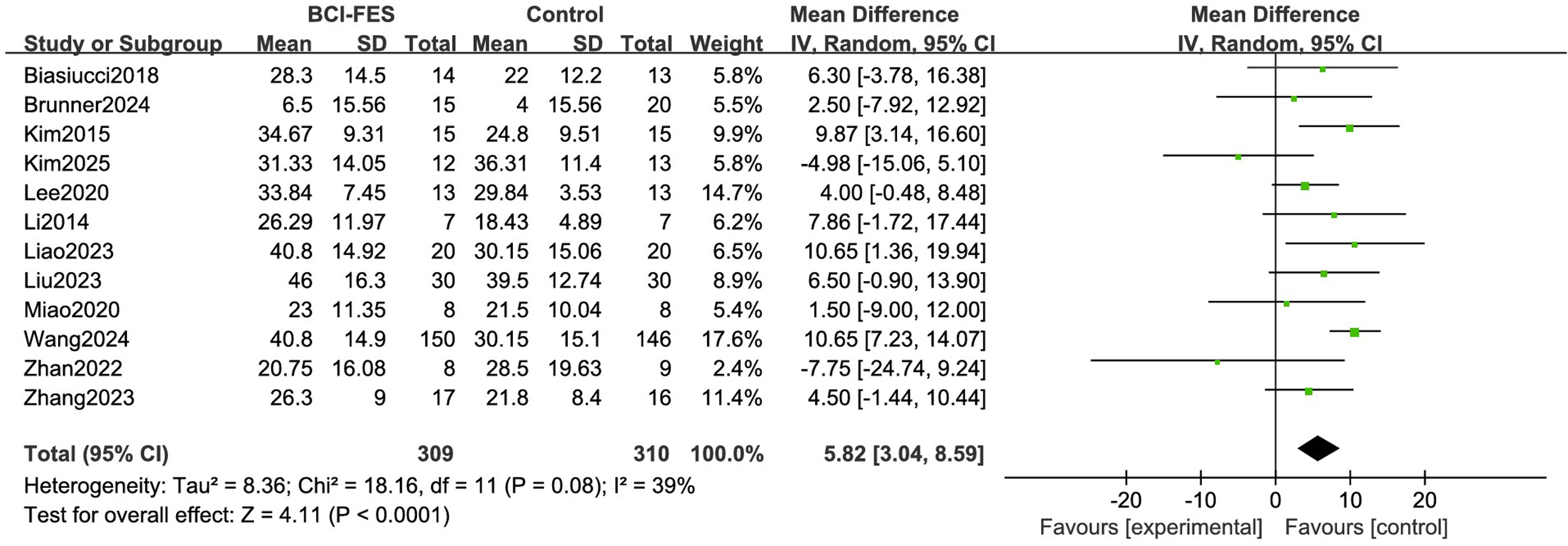
Forest plot of the pooled effect of BCI-FES on upper limb function.
ARAT/WMFT/MBI
Three RCTs(345 patients) were included for ARAT, three RCTs for WMFT, and two studies (85 patients) for MBI. BCI-FES were associated with greater improvements in ARAT scores (MD = 4.3, 95% CI 1.66-6.95, Z = 3.19, P = 0.001; I2 = 6%). For WMFT, moderate heterogeneity was observed (I2 = 56%, P = 0.1), and a random-effects model showed a statistically significant difference favoring BCI-FES training (MD = 5.08, 95% CI 0.97-9.19, P = 0.02). Similarly, BCI-FES interventions were associated with greater improvements in MBI scores (MD = 17.92, 95% CI 11.98-23.87, Z = 5.91, P < 0.00001), with negligible heterogeneity (I2 = 0%, df = 1, P = 0.9) (Figure 5).
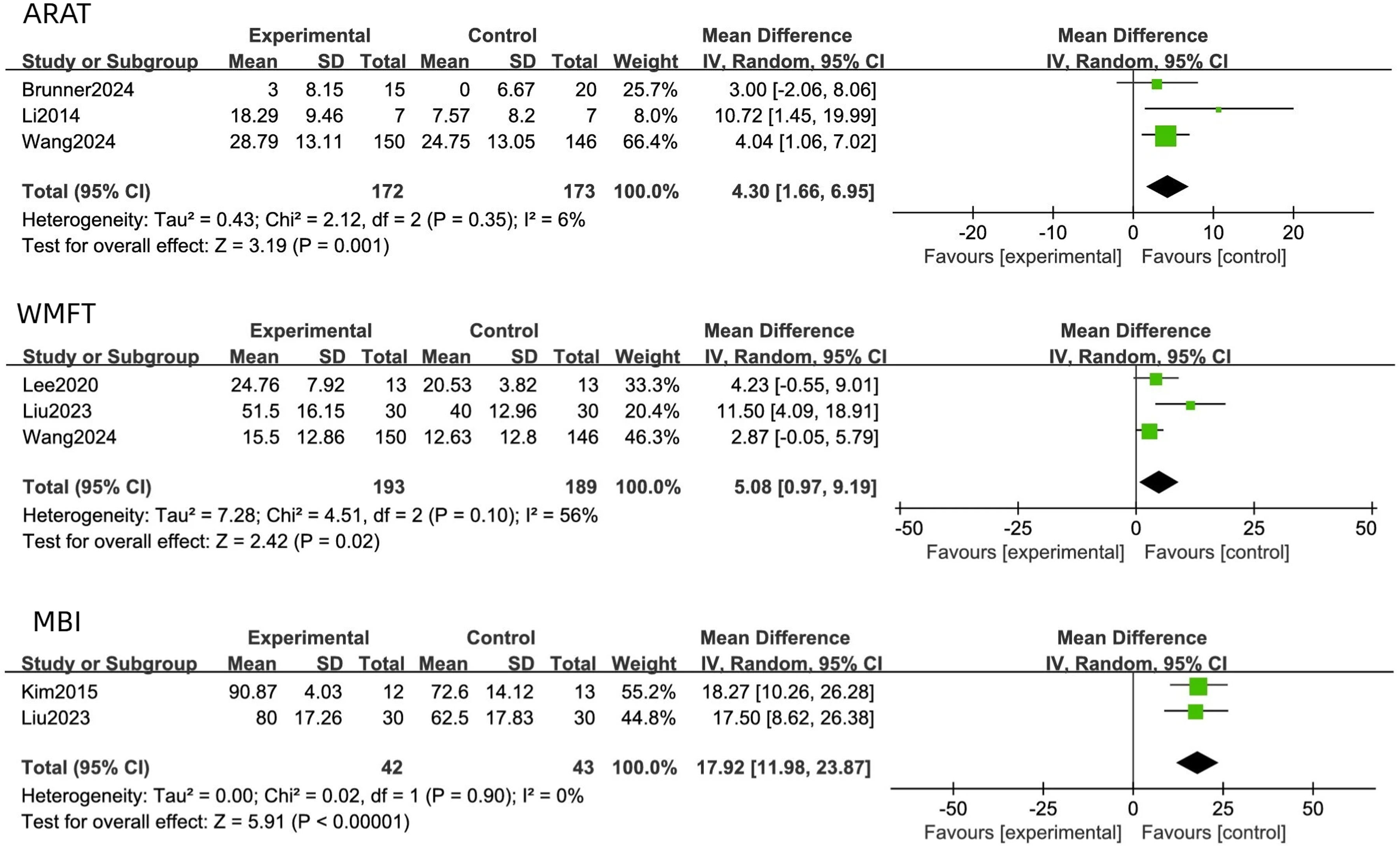
Forest plots of the effect of BCI-FES on upper limb function outcomes.
Subgroup Analysis
Subgroup Meta-Analysis Summary Table.
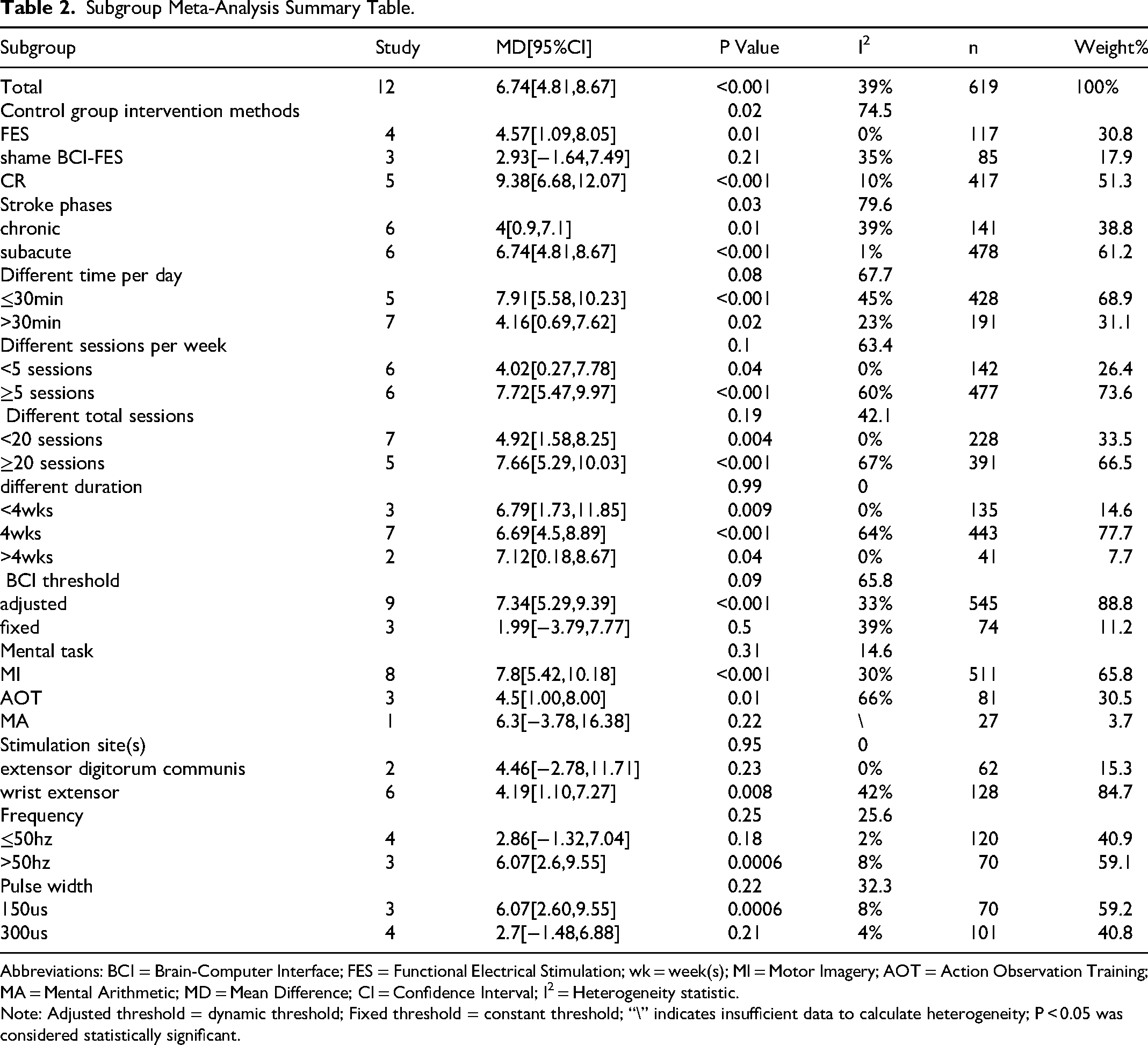
Abbreviations: BCI = Brain-Computer Interface; FES = Functional Electrical Stimulation; wk = week(s); MI = Motor Imagery; AOT = Action Observation Training; MA = Mental Arithmetic; MD = Mean Difference; CI = Confidence Interval; I2 = Heterogeneity statistic.
Note: Adjusted threshold = dynamic threshold; Fixed threshold = constant threshold; “\” indicates insufficient data to calculate heterogeneity; P < 0.05 was considered statistically significant.
Type of Control Group Training
Regarding control intervention type, studies were divided into three subgroups: FES training, sham BCI-FES, and conventional rehabilitation. The FES subgroup (4 studies, 117 participants) showed a statistically significant difference favoring BCI-FES (MD = 4.57, 95% CI 1.09–8.05, P = 0.01,I2= 0%). The sham BCI subgroup (3 studies, 85 participants) showed no significant difference (MD = 2.53, 95% CI −3.48 to 8.54, P = 0.41; I2= 35%). The conventional rehabilitation subgroup included five studies with 417 participants, in which BCI-FES was associated with greater improvement in FMA-UE scores compared with conventional rehabilitation (MD = 9.07, 95% CI 5.98–12.16, P < 0.00001), with low heterogeneity (I2= 10%). Between-subgroup comparisons suggested a trend toward differences (P = 0.06), but not statistically significant.
Stroke Phases
In the subacute phase (≤6 months), 6 trials including 478 participants showed a mean improvement of 8.45 points in FMA-UE (95% CI 5.96-10.95, P < 0.0001), reaching the threshold for clinical significance, with minimal heterogeneity (I2 = 1%). In the chronic phase (>6 months), 6 trials including 141 participants showed a mean FMA-UE improvement of 3.36 points (95% CI −1.11–7.84), which did not reach statistical significance (P = 0.14), with moderate heterogeneity (I2 = 39%). Between-subgroup comparison indicated a borderline difference between the subacute and chronic phases (P = 0.05).
Training Intensity
When stratified by training intensity, subgroup analyses were conducted according to single-session duration, weekly frequency, total number of sessions, and total intervention weeks. For session duration, sessions ≤30 min were associated with a mean FMA-UE improvement of 7.31 points (95% CI 3.82-10.23, I2 = 45%, P < 0.01), whereas sessions >30 min showed a smaller improvement of 3.99 points (95% CI −0.11-8.08, I2=23%, P = 0.06). The between-subgroup comparison was not statistically significant (P = 0.23). Regarding weekly frequency, <5 sessions per week showed a statistically significant improvement (MD = 4.02,95% CI 0.27-7.78, I2 = 0%, P = 0.04), whereas ≥5 sessions per week also showed a statistically significant improvement (MD = 6.82, 95% CI 2.83–10.82, P < 0.001). For total number of sessions, ≥20 sessions were associated with a mean improvement of 6.38 points (95% CI 1.69–11.07) with substantial heterogeneity (I2 = 67%, P < 0.001), whereas <20 sessions were associated with a mean improvement of 4.92 points (95% CI 1.58–8.25, I2 = 0%). Analysis by total intervention weeks showed that interventions <4 weeks, 4 weeks, and >4 weeks were all associated with statistically significant improvements (MD = 6.79, 95% CI 1.73–11.85, P = 0.009; MD = 4.68, 95% CI 0.44–8.92, P = 0.03; MD = 7.12, 95% CI 0.18–14.06, P = 0.04, respectively), with varying heterogeneity (I2 = 0%, 64%, and 0%, respectively).
BCI Parameters
Subgroup analyses of BCI parameters included dynamic threshold adjustment (9 studies, MD = 6.77, 95% CI 3.99–9.55, P < 0.001) and fixed-threshold settings (3 studies, MD = 1.99, CI crossing zero p = 0.61). The between-subgroup comparison did not reach statistical significance (P = 0.23).For mental task type, motor imagery (MI, 8 studies) showed a mean improvement of 6.72 points (95% CI 3.47–9.97, I2= 30%, P < 0.001), action observation training (AOT, 3 studies) showed a mean change of 3.85 points (95% CI −2.89–10.59, I2= 66%, P = 0.26), which was not statistically significant. Movement attempt (MA, 1 study) showed a mean change of 6.3 points (95% CI −3.78–16.38, P = 0.22),also not statistically significant. Between-subgroup comparison did not reach statistical significance (P = 0.75).
FES Parameters
Subgroup analyses of FES parameters are summarized in Table 2. Stimulation site showed that wrist extensors (6 studies) yielded a mean difference (MD) of 3.57 points (95% CI −0.99–8.14; I2= 42%; P = 0.12) and finger extensors (2 studies) yielded a MD of 4.46 points (95% CI −2.78–11.71; P = 0.23); neither result was statistically significant. The between-subgroup comparison was also not statistically significant (P = 0.84). High-frequency stimulation (>50 Hz, 3 studies) was associated with a significant improvement, with a mean difference (MD) of 6.20 points (95% CI 2.49–9.92; I2= 9%; P = 0.001). By contrast, low-frequency stimulation (≤50 Hz; 4 studies) resulted in a smaller change (MD = 2.83 points; 95% CI −1.42–7.08; I2= 2%; P = 0.19) that did not reach statistical significance.Similarly, narrow pulse width (150 µs, 3 studies) led to a significant gain (MD = 6.20; 95% CI 2.49–9.92; I2= 8%; P = 0.001), while the effect of wide pulse width (300 µs; 4 studies) was smaller and not statistically significant (MD = 2.65; 95% CI −1.66–6.98; I2= 4%; P = 0.23).
Publication Bias
Visual inspection of funnel plots (Supplementary Figure S1) was performed to assess potential publication bias. Egger's regression test suggested borderline funnel plot asymmetry (p = 0.046), and the fail-safe N was 62.
Discussion
This systematic review and meta-analysis included 12 studies16,17,22–31 investigating the effects of BCI-FES on upper limb motor recovery in stroke patients. The studies primarily focused on patients with ischemic or hemorrhagic stroke, with lesions commonly involving cortical and subcortical regions such as the basal ganglia and thalamus, although not all studies reported lesion location in detail. Sample sizes were generally small (range, 15–296; most n < 50), and intervention durations ranged from 3 to 8 weeks. Despite relatively wide confidence intervals, methodological quality was moderate to high (PEDro 4–9, mean 6.92), with generally reliable randomization and outcome reporting. However, unclear allocation concealment or lack of participant blinding (Figures 2 and 3) may slightly inflate effect estimates, especially in smaller studies. No serious adverse events were reported.
Meta-analysis showed that BCI-FES significantly improved FMA-UE scores, with a mean increase of 5.82 points compared with controls. These findings are consistent with previous systematic reviews.18,32 Notably, this magnitude of improvement exceeds the lower bound of commonly cited minimal clinically important difference (MCID) thresholds for the upper-extremity Fugl-Meyer Assessment (approximately 4–5 points), supporting the clinical relevance of the observed effect at the group level.33,34 In the studies included in our review, most were judged to have low risk of bias for random sequence generation, selective reporting, and other domains. However, allocation concealment and participant blinding were often rated as unclear or high risk, which may have influenced the estimated effect sizes. To address this concern, sensitivity analyses were conducted excluding three studies that did not directly report raw data or mean ± SD values for FMA-UE. The results remained significant (MD = 4.81, 95% CI 1.74-7.88, P = 0.002), supporting the robustness of the primary findings. Secondary outcomes consistently showed greater effect sizes with BCI-FES, suggesting it may contribute to improvements in upper limb function and activities of daily living, highlighting its potential clinical relevance.
Differential effects were observed across comparator types, with BCI-FES showing greater improvements relative to conventional rehabilitation and FES alone, but no statistically significant superiority over sham BCI-FES. This pattern differs from previous analyses, 35 particularly in comparisons between BCI-FES and sham BCI-FES, where inconsistent effects have been observed, likely reflecting the considerable heterogeneity in sham BCI-FES protocols, as well as variations in BCI decoding algorithms, feedback modalities, and training protocols across studies. Current evidence suggests that the observed overall benefits of BCI-FES may partially reflect the contrast between “active, high-technology” and “standard, low-attention” interventions, 36 and whether these gains are attributable to a specific “mind-driven” closed-loop neurophysiological mechanism remains to be confirmed in future sham-controlled trials with adequate sample sizes and standardized protocols.
Analysis suggested that shorter single-session durations (≤30 min) were associated with higher effect estimates than longer sessions. When considered alongside subgroup findings indicating larger effect estimates with higher weekly training frequency (≥5 sessions), these observations point to a potential association between a “short-duration, high-frequency” training pattern and improved outcomes. Although each session is brief, total weekly training intensity is high, which may contribute to the observed benefits.This pattern is conceptually consistent with the distributed practice principle in motor learning, whereby more frequent and shorter practice bouts may facilitate motor memory consolidation and transfer.37,38 In addition, shorter, more frequent sessions may improve patient compliance and reduce fatigue, enhancing their practical feasibility. Evidence on the optimal total training duration remains limited. Although longer programs (>4 weeks) were associated with larger effect estimates in some analyses, small study numbers and limited follow-up preclude firm conclusions, and intervention durations of approximately 3–4 weeks have been most commonly studied.
Subgroup analyses indicated that different BCI parameters, including BCI threshold, mental task, stimulation frequency, and pulse width may influence efficacy.However, most comparisons involved small sample sizes and showed only trend-level effects. Dynamic threshold adjustment showed a higher point estimate than fixed thresholds (MD 7.34 vs 1.99), but confidence intervals overlapped and the interaction test was not significant (p = 0.09). High-frequency stimulation (>50 Hz) and narrow pulse width (150 µs) showed numerical advantages, but between-group differences were not significant (p = 0.25 and p = 0.22, respectively). Motor imagery (MI) showed the largest and most consistent effect size across six studies(MD 7.8, I2 = 30%),suggesting it may be a relatively robust, though supporting data remain preliminary. Notably, although motor attempt tasks have been reported in only a single study by Ono et al, 39 the findings suggest that proprioceptive feedback may provide additional benefits. Pooled effects for wrist and finger extensors were similar. Wrist extensors, studied more frequently with narrower confidence intervals, may serve as a well-supported default target. Overall, current subgroup results indicate potential trends but remain insufficient to establish definitive clinical recommendations. However, studies reporting greater efficacy generally involved sessions of approximately 30 min, delivered ≥ 5 times per week for > 4 weeks.
From a neuroplasticity perspective, BCI-FES may form a closed-loop sensorimotor circuit by linking patients’ motor intentions—detected via EEG as movement-related desynchronization or motor imagery signals—with time-locked electrical stimulation of the contralateral limb. 22 The efficacy of this closed-loop circuit may be influenced by BCI parameters, where motor imagery paradigms and dynamic threshold settings help ensure temporal contingency between cortical discharge and peripheral feedback, thereby supporting Hebbian-based synaptic plasticity in cortico-spinal pathways and intracortical circuits.40–42 BCI-FES may also influence movement-related rhythms (eg, μ/β desynchronization), modulate functional connectivity, and potentially facilitate re-engagement of the affected hemisphere while reducing pathological interhemispheric inhibition, thereby contributing to motor function retention and transfer.42,43 Although most included trials did not directly assess neural outcomes, some studies suggest that long-term, repetitive, and task-specific BCI-FES training may induce lasting interhemispheric connectivity changes, potentially consolidating these neural and network-level adaptations into a framework supporting for sustained functional recovery.43, 44
It should be noted that this study has several limitations. First, some subgroups included few trials—particularly finger extensor and >4week training subgroups—limiting the precision of effect estimates and the power to detect significant differences. Second, variations in BCI decoding algorithms, feedback modalities, and training protocols across studies may introduce residual heterogeneity, despite the use of random-effects models. Third, the lack of individual patient data in some studies precluded analysis of interactions between BCI parameters and baseline impairment, stroke duration, or age. In addition, the limited number of studies available for each covariate prevented the performance of meta-regression analyses, representing an important methodological limitation of the present meta-analysis. Furthermore, although Egger's regression test suggested borderline asymmetry, the limited number of included studies means that small-study effects cannot be completely excluded. Future multicenter, large-sample RCTs, together with meta-analyses incorporating a larger number of homogeneous studies, may enable robust meta-regression analyses to examine the contribution of stimulation intensity, training density, and specific BCI parameters to clinical outcomes, thereby supporting evidence-informed optimization of BCI-assisted stimulation protocols.
Conclusion
In summary, BCI-FES interventions were associated with improvements in post-stroke upper limb motor function, with the most pronounced effects observed during the subacute phase. Exploratory analyses indicated that higher stimulation frequency, narrow pulse width, dynamic-threshold paradigms, and motor imagery tasks may be linked to larger effect sizes, and that greater session frequency and shorter session duration over multiple weeks could potentially enhance outcomes. Nevertheless, these findings are based on a limited number of studies with moderate-certainty evidence, precluding definitive conclusions regarding optimal protocols. Large-scale, multicenter trials are needed to confirm these observations and assess long-term efficacy.
Supplemental Material
sj-docx-1-eeg-10.1177_15500594261441055 - Supplemental material for Brain-Computer Interface Combined with Functional Electrical Stimulation for Post-Stroke Upper Limb Motor Recovery: A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-eeg-10.1177_15500594261441055 for Brain-Computer Interface Combined with Functional Electrical Stimulation for Post-Stroke Upper Limb Motor Recovery: A Systematic Review and Meta-Analysis by Fengjiao Liang, Xiang Chen, Baoying Li and Banghua Yang in Clinical EEG and Neuroscience
Footnotes
Acknowledgements
We extend our gratitude to the authors of the research studies included in this systematic review for their invaluable support and contributions.
Ethics Approval and Consent to Participate
Not applicable
Consent for Publication
Not applicable
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Aeronautical Science Foundation of China, National Key Research and Development Program of China, National Natural Science Foundation of China, (grant number 2024Z0710S6003,ASFC-2024Z0710S6003, 2024YFF1206500, 2024YFF1206502, No.32571279, No. 62376149).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The original contributions presented in the study are included in the article/Supplemental material, further inquiries can be directed to the corresponding author.
Supplemental Material
Supplemental material for this article is available online.