
Abstract
Lithium carbonate is a first-line psychopharmacological agent for the treatment of mood disorders, demonstrating significant therapeutic and prophylactic efficacy in the management and prevention of relapses in bipolar affective disorders characterized by manic and depressive episodes. However, chronic lithium therapy or acute overdose can lead to toxicity, with symptoms predominantly observed in individuals with a psychiatric history. Clinical manifestations of lithium toxicity are primarily neurologic and gastrointestinal. This article presents the diagnosis and treatment of a case of lithium toxicity, incorporating an analysis of the literature on the characteristics of wakeful EEG before and after treatment in relation to serum lithium levels. It was found that EEG, as an adjunctive examination in lithium-induced encephalopathy, serves as a sensitive tool for assessing lithium-related neurotoxicity, facilitating the safe management of manic disorders and other psychiatric conditions treated with lithium carbonate.
Introduction
This study focuses on lithium intoxication through a specific case report, comparing the dynamics of wakeful EEG before and after treatment of lithium intoxication. It demonstrates the significant positive correlation between EEG dynamics, dynamic changes in serum lithium concentration, and the progressive dynamics of the patient's condition. Additionally, it elaborates on the specific utility of routine wakeful EEG recordings in the diagnosis and management of patients with lithium intoxication.
Serum Lithium Concentration and Routine Awake EEG Recordings.

Lithium carbonate is a commonly used medication for the treatment of mood disorders, including mania, bipolar affective disorder, and depression. However, its therapeutic range is narrow, with serum lithium levels for clinical efficacy typically maintained between 0.60 and 1.20 mmol/L, while levels exceeding 1.4 mmol/L can result in lithium toxicity. 1 Lithium-induced neurotoxicity poses a significant risk of permanent neurological sequelae. The neurological manifestations of lithium toxicity include tremor, delirium, myoclonus, and extrapyramidal motor disturbances. 2 Early identification of lithium toxicity in high-risk patients through sensitive auxiliary diagnostic tools is critical for guiding timely treatment. Here, we report the case of a patient with mania who developed neurotoxic symptoms after long-term oral lithium therapy. Routine awake-state EEG recordings were obtained both before and after treatment. By comparing the EEG dynamics strongly associated with serum lithium levels, this study explores the feasibility of using routine awake-state EEG recordings as an auxiliary tool for the long-term management of lithium therapy in the treatment of mania and other psychiatric disorders.
Case Presentation
A 54-year-old right-handed male farmer was admitted to our hospital on the night of July 5, 2021, due to “slurred speech and slowed responses for 9 days, with worsening over the past 3 days.” Nine days prior to admission, the patient developed diarrhea, occasionally accompanied by nausea and vomiting. He sought treatment at a local clinic, where he received oral medications (specifics unknown) with partial relief of symptoms. However, he gradually felt fatigued, which did not improve with rest and progressively worsened. He then visited a local hospital for further treatment (details unknown), but his symptoms deteriorated significantly 3 days prior to admission, prompting emergency admission to our hospital.
Past Medical History: Fifteen years prior, the patient had experienced symptoms such as excitement, excessive talking, reduced sleep, and hyperactivity without clear precipitating factors. He was diagnosed with mania at a municipal psychiatric hospital and had been on long-term oral lithium carbonate therapy (specific dosage unknown; the family arbitrarily adjusted the dosage on occasion). Due to difficulties in medication adherence caused by his condition, he had discontinued lithium carbonate 7 days before admission.
On admission, vital signs were as follows: temperature 37.2 °C, pulse 84 beats/min, respiratory rate 20 breaths/min, blood pressure 145/83 mm Hg, and body weight 60 kg. The patient had normal development and moderate nutritional status. He was conscious but exhibited poor mental status, slurred speech, decreased level of consciousness, slowed behavior, and impaired executive function. He was uncooperative with questioning and unable to complete assessments of memory, orientation, and calculation. Additional findings included a blank stare, normal and coordinated eye movements, bilaterally equal and round pupils with prompt light reflexes, symmetrical facial muscles, and a midline tongue upon protrusion. Neurological examination revealed neck stiffness (two-finger width under the chin), normal muscle tone, grade 5 muscle strength in all limbs, symmetrical deep tendon reflexes, and a questionable left Babinski sign. Coordination tests (finger-nose and heel-knee-shin tests) and assessments of sensory modalities (deep, superficial, and cortical sensation) could not be performed due to poor cooperation. The patient occasionally experienced urinary incontinence.
Admission laboratory tests showed: serum sodium 139 mmol/L, serum calcium 2.47 mmol/L, serum potassium 6.21 mmol/L, urea 14.4 mmol/L, and serum creatinine 330.8 μmol/L. A consultation with the nephrology department suggested a high possibility of chronic renal insufficiency. Imaging and Other Examinations:Admission cranial CT: Lacunar infarcts in the right periventricular region and left basal ganglia; slightly lower density in the left basal ganglia compared to the contralateral side.Admission cranial MRI: 1) Multiple new infarcts suspected in the right basal ganglia and left thalamus; 2) Bilateral ethmoid sinusitis; 3) No significant abnormalities in cranial MRA or MRV.Cranial MRI 2 weeks after admission: 1) Abnormal signal in the left thalamus, consistent with a new infarct; 2) Bilateral basal ganglia lacunar infarcts; 3) Bilateral ethmoid sinusitis and bilateral mastoiditis.Abdominal ultrasound (liver, gallbladder, pancreas, spleen, and kidneys) on admission: Diffuse renal lesions; no significant abnormalities in the liver, gallbladder, pancreas, or spleen.Ultrasound of renal size, cortical thickness, and blood flow: Diffuse renal lesions; increased resistance index in the right renal artery; decreased blood flow in the left kidney; normal blood flow in the right kidney. Parathyroid hormone and serum β2-microglobulin levels were measured.
Given the patient's history of diarrhea with nausea/vomiting 9 days prior to onset, followed by progressive fatigue, slowed responses, slurred speech, and decreased consciousness, intracranial infection and autoimmune encephalitis could not be ruled out. A lumbar puncture was performed after admission, with normal results for cerebrospinal fluid (CSF) routine tests and biochemistry. High-throughput sequencing of CSF for viruses and bacteria, as well as serum and CSF tests for autoimmune encephalitis antibodies and paraneoplastic antibodies, showed no abnormalities. Considering the patient's long-term lithium carbonate use, lithium intoxication could not be excluded. After consultation with the department of psychological health, serum lithium concentration was measured at a psychiatric hospital. After admission, the patient's level of consciousness progressively declined. The serum lithium concentration was 3.93 mmol/L. Immediate interventions included fluid resuscitation, vasopressors to maintain circulatory stability, correction of metabolic acidosis, mechanical ventilation for respiratory support, sedation, anti-manic therapy, anti-infective treatment, liver protection, and albumin infusion. Concurrently, a hemofiltration catheter was placed for blood purification to reduce lithium levels. Niaoduqing (a traditional Chinese medicine) was administered to manage chronic renal insufficiency.
Electroencephalography (EEG)
EEG Recording Methodology
Serum lithium concentrations were monitored, and routine awake EEG recordings were performed both before and after treatment. Prior to the EEG examination, the purpose of the test and the need for cooperation were explained in detail to both the patient and their family, with a particular emphasis on informing the family. The EEG was conducted in a quiet room with soft lighting and a comfortable temperature to avoid artifacts caused by patient sweating or shivering. The test was performed within 3 h after a meal to prevent hypoglycemia from affecting the results.
The EEG recordings were obtained using the Nihon Kohden EEG-1200C system. Electrodes were placed according to the international 10–20 system. Before electrode placement, the patient's scalp was cleaned to minimize skin resistance caused by oil or debris. High-quality disk electrodes were used. Although routine awake EEGs are typically recorded in a seated position, the recordings were performed in a supine position in this case due to the patient's clinical condition.
The instrument parameters were adjusted prior to the examination, including sensitivity (7-10 μV/mm), high-frequency filter (70 Hz), low-frequency filter (0.53 Hz or 1 Hz), and display time (10 s per screen). After confirming the proper functioning of the equipment, EEG recordings were performed.
Serum Lithium Concentrations and EEG Features Before and After Treatment
Pre-Treatment EEG (Serum Lithium: 3.93 Mmol/L)
Background Activity:Severe background abnormalities were observed. No dominant occipital rhythm was detected. The background activity was characterized by irregular mixed waveforms dominated by low-to-moderate amplitude delta slow waves. High-to-moderate amplitude delta slow waves were predominantly observed in the bilateral frontal poles and anterior temporal regions, with widespread involvement. Paroxysmal Abnormalities:Irregular paroxysms of low-amplitude atypical spike-wave complexes were noted, primarily in the bilateral frontal poles, frontal, and anterior temporal regions (Figure 1).
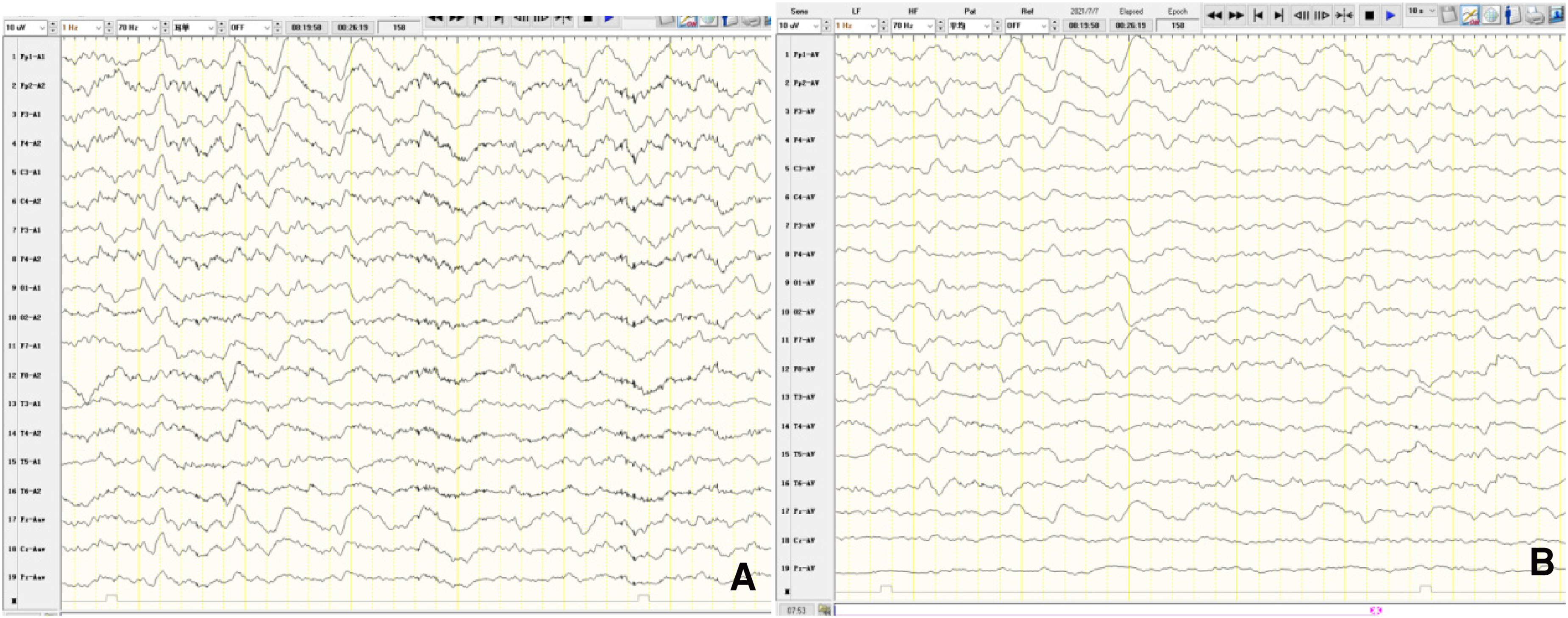
Awake EEG before treatment for lithium toxicity (serum lithium concentration: 3.93 mmol/L). A: EEG recording with ear lobe reference montage. B: EEG recording with average reference montage.
EEG After 2 Weeks of Treatment (Serum Lithium: 1.8 Mmol/L)
Background Activity: Mild background abnormalities were observed. Occipital dominant rhythm was less prominent, with low-amplitude alpha activity (8-10 Hz) showing poor modulation and amplitude variability. Moderate amounts of low-to-moderate amplitude theta slow waves were observed paroxysmally in the frontal regions, with widespread involvement. Paroxysmal Abnormalities: No relevant abnormalities were detected (Figure 2A).
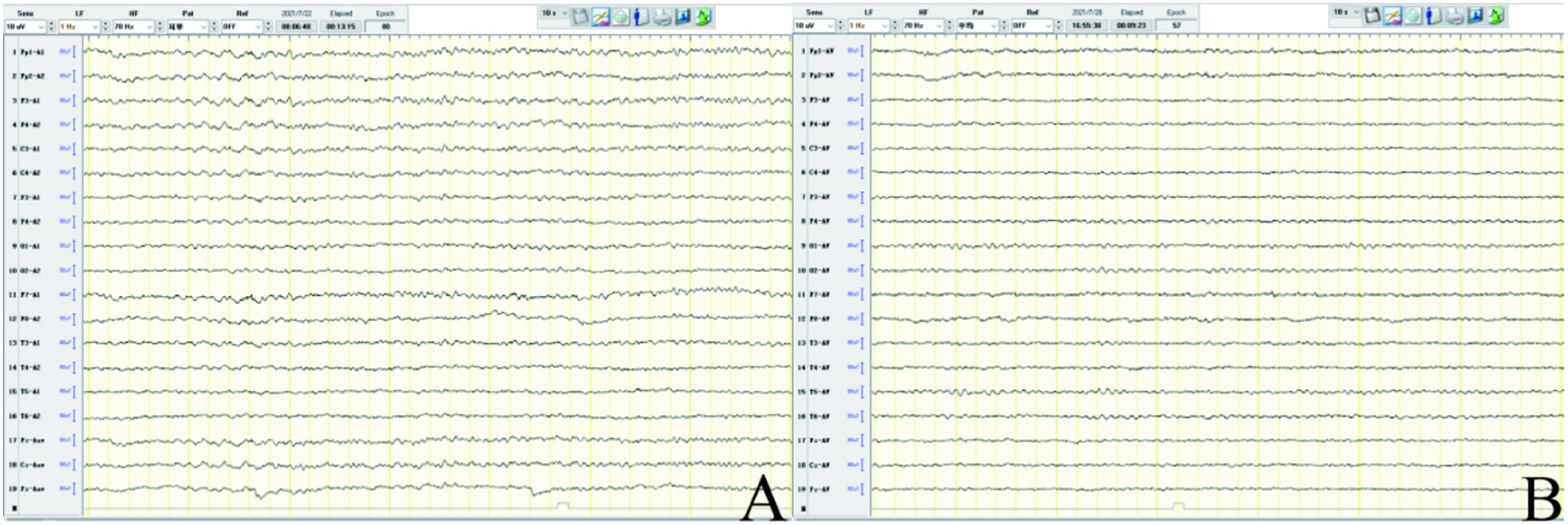
Awake EEG after treatment for lithium toxicity. A: EEG after 2 weeks of treatment (serum lithium concentration: 1.8 mmol/L). B: EEG after 3 weeks of treatment (serum lithium concentration: 0.57 mmol/L).
EEG After 3 Weeks of Treatment (Serum Lithium: 0.57 Mmol/L)
Background Activity: Normal background activity was observed. A clear occipital dominant rhythm was present, with low-amplitude alpha activity (9-12 Hz) and rhythm, though modulation and amplitude variability remained suboptimal. Scattered low-amplitude theta slow waves were occasionally observed. Paroxysmal Abnormalities: No relevant abnormalities were detected (Figure 2B).
Discussion
The recording and analysis of electroencephalography (EEG) represent an essential, sensitive, and non-invasive approach for evaluating brain function in clinical practice. EEG is widely used to assess dysfunction associated with various neurological disorders.
In this case of lithium carbonate toxicity, we performed wakeful EEG recordings at three time points: before treatment, 2 weeks after treatment, and 3 weeks after treatment. These time points allowed direct comparison among serum lithium concentration, EEG dynamics, and clinical status (Table 1): Before treatment: Serum lithium was markedly elevated. EEG showed dominant slow (delta) activity, consistent with severe brain dysfunction, and the patient could only cooperate passively. Two weeks after treatment: Serum lithium decreased to near normal. EEG showed a dominant alpha pattern with intermixed theta waves. The patient's clinical status improved significantly, with active but incomplete relaxation. Three weeks after treatment: Serum lithium normalized. EEG showed a normal waking alpha pattern, and the patient was fully alert, relaxed, and cooperative. These results demonstrate that EEG changes induced by lithium toxicity are reversible and closely correlated with serum lithium levels. As serum lithium decreased to normal, EEG slowing resolved gradually, and clinical status improved in parallel. This highlights a tight relationship among serum lithium dynamics, EEG changes, and clinical neurological state. Previous experimental studies in mice have demonstrated that lithium-induced encephalopathy correlates with brain lithium accumulation, 3 supporting EEG as a sensitive biomarker for lithium neurotoxicity. Scalp EEG in lithium intoxication typically presents with extremely slow waves (including delta waves), spikes, sharp waves, irregular discharges, or periodic discharges—with increased diffuse slow waves as the most prominent feature.4,5 EEG abnormalities caused by lithium neurotoxicity, along with clinical symptoms, can be reversed by hemodialysis. Hemodialysis is also effective in removing lithium and reversing EEG abnormalities in severe lithium intoxication (especially cases with obvious EEG abnormalities or renal insufficiency).4,6Additionally, lithium intoxication symptoms may be confused with those of cerebral infarction in some elderly patients; however, their EEG patterns differ. Two weeks after admission, the patient developed a new cerebral infarction. This infarction was insufficient to explain the clinical symptoms and showed a weak correlation with EEG dynamics before and after hemodialysis-based treatment. For patients with cerebral infarction, EEG can reflect the location and extent of brain damage: larger and more superficial infarcts result in more pronounced EEG abnormalities, typically manifesting as focal or regional irregular delta slow waves corresponding to the infarcted areas identified on imaging.7,8 Studies have reported that in the early stage of acute ischemic stroke (AIS), slow wave elevation (δ↑, θ↑) and alpha/beta wave reduction (α/β↓) are common, and these changes correlate with infarct size (especially cortical involvement).9,10 Epileptiform discharges are also not uncommon in AIS and are associated with cortical involvement. 11 A comparative study of CT and EEG found that unilateral theta/delta slow waves have high value in indicating cortical infarction; hemispheric asymmetry is associated with cortical ischemia, whereas lacunar infarctions rarely present with such abnormalities.7,12In summary, although both lithium intoxication and cerebral infarction can cause EEG background slowing and epileptiform discharges, they differ in key aspects:
Lithium intoxication: Often associated with a history of lithium use and renal dysfunction; EEG abnormalities are characterized by relatively diffuse slow wave distribution, and rapid improvement occurs after hemodialysis and lithium discontinuation.Cerebral infarction: Often presents with sudden focal neurological deficits; EEG abnormalities are characterized by relatively unilateral, focal, or hemispherically asymmetric slow waves, which are consistent with imaging findings and clinical signs. Asymmetry may improve after reperfusion therapy.
To date, lithium carbonate remains a first-line medication for the long-term treatment and prevention of manic episodes in bipolar disorder. 1 However, lithium has a relatively narrow therapeutic window, with therapeutic doses close to toxic doses. Early symptoms of lithium intoxication are often non-specific and easily overlooked in clinical practice. Therefore, strict and regular monitoring of serum lithium concentrations during treatment is crucial to ensure medication safety. Psychiatrists must consider individual patient factors, pay close attention to the specific toxic side effects of drugs like lithium, closely monitor clinical manifestations, and perform regular EEG examinations. This allows for flexible adjustment of treatment plans and reduction in the incidence of lithium intoxication.
Given the delicate balance between the efficacy and safety of lithium, there is an urgent need to explore safer and more effective alternative treatment options in the future. Currently, the key to long-term patient management lies in collaborative efforts between medical professionals and patients. During lithium treatment, it is essential to provide multi-channel, comprehensive education and guidance to patients and their families—with a particular focus on family members. Due to the specificity and chronicity of psychiatric disorders, family members should take the lead in medication management, supervise and assist patients in safe medication use, and ensure regular follow-ups for serum lithium concentration monitoring and EEG re-evaluations.
EEG examination combined with serum lithium concentration measurement helps support the diagnosis of lithium carbonate intoxication through a more comprehensive evidence chain and aids in differentiating lithium toxicity-related clinical syndromes (including those associated with other psychiatric medications). 13 In contrast to serum lithium concentration measurement— which aims to obtain a specific, objective value to determine whether levels are within the normal range—EEG examination is intended to more accurately and dynamically assess the disease progression, treatment efficacy, and recovery status of patients with lithium intoxication.
Relevant literature and case reports indicate that6,14,15: In lithium intoxication, EEG changes are relatively consistent and more strongly correlated with neurotoxic symptoms than with serum lithium levels.Lithium encephalopathy may occur even when serum lithium levels are within the therapeutic range, suggesting that serum lithium levels do not always reflect brain lithium levels.
Improvements in EEG often synchronize with the alleviation of clinical symptoms and are more aligned with clinical status than serum lithium levels alone. EEG is an indispensable tool for evaluating acute and chronic lithium toxicity; it is suitable for monitoring treatment efficacy and disease progression and is superior to serum lithium levels alone as an indicator of toxicity activity and recovery. Furthermore, unlike serum lithium concentration—which typically requires measurement at psychiatric hospitals and cannot provide immediate results—EEG examinations can be performed at the patient's bedside quickly and yield real-time results. A case report 6 showed that simplified EEG was used in the emergency department to quickly detect EEG abnormalities at the bedside and perform dynamic monitoring. In that case, the patient had a serum lithium level of 3.88 mmol/L and acute kidney injury; after hemodialysis and sedation, the patient recovered without neurological sequelae. 6 This highlights the usability and value of simplified EEG in emergency settings. Given that routine wakeful EEG recordings offer advantages such as immediacy, sensitivity, continuity, painlessness, and low cost—and considering that EEG changes in lithium carbonate intoxication primarily involve background activity abnormalities (which can be observed via wakeful recordings)—routine wakeful EEG is relatively suitable for the long-term management of such patients. It enables phased assessment of patient conditions through dynamic EEG monitoring and is therefore practically necessary and feasible.
Footnotes
Acknowledgements
The authors thank the patient and family for their cooperation in this case report.
Ethical Statement
This case report was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from the patient and family for publication of this case report and accompanying images. Patient confidentiality has been maintained throughout.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Academician Workstation of The Second Hospital & Clinical Medical School, Lanzhou University,
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current case report are available from the corresponding author on reasonable request, subject to patient privacy considerations.
Registered Clinical Trials (RCTs)
Not applicable (this is a case report, not a clinical trial).
Pre-Print Hosting
Not applicable / This manuscript has not been published as a pre-print.