
Abstract
Objective
To describe demographics, semiology, etiology, and clinical features in individuals with insulo-opercular and pure insular onset presenting with hyperkinetic seizures (HKS).
Methods
Under PRISMA guidelines, Embase, PubMed, Medline, and Cochrane were searched for articles between 1969 and January 10, 2025, using terms for hyperkinetic/hypermotor seizures, insular epilepsy, sleep-related hypermotor epilepsy, nocturnal paroxysmal dyskinesia/dystonia, nocturnal frontal lobe epilepsy, and complex motor behavior. Eligible studies were reports or retrospective series of patients with pure insular or insulo-opercular epilepsy and HKS, documented with SEEG or subdural recordings, with at least 6 months of postsurgical follow-up and Engels class I. Of 271 studies, 14 met inclusion criteria.
Results
Fourteen studies including 34 patients were analyzed; 61.8% had pure insular onset. Focal cortical dysplasia was the most common etiology, present in two-thirds of cases. Most HKS began with non-motor semiology (76.5%). Hyperkinetic automatisms type 3, defined by integrated/natural hyperkinetic behaviors, manipulation/utilization behaviors, and distal stereotypies, were reported in 49.9% of patients with pure insular onset. Compared with insulo-opercular onset, pure insular onset was associated with a higher frequency of these behaviors, along with agitation, vocalization, and breathing difficulties (p < 0.05). These findings are based on small, heterogeneous samples and should be interpreted cautiously.
Conclusion
HKS were more frequently associated with pure insular onset. Focal cortical dysplasia was the most common etiology, and integrated/natural hyperkinetic behavior was more frequent with pure insular onset. Given limited sample size, heterogeneity, and study design constraints, these findings should be considered exploratory rather than definitive.
This is a visual representation of the abstract.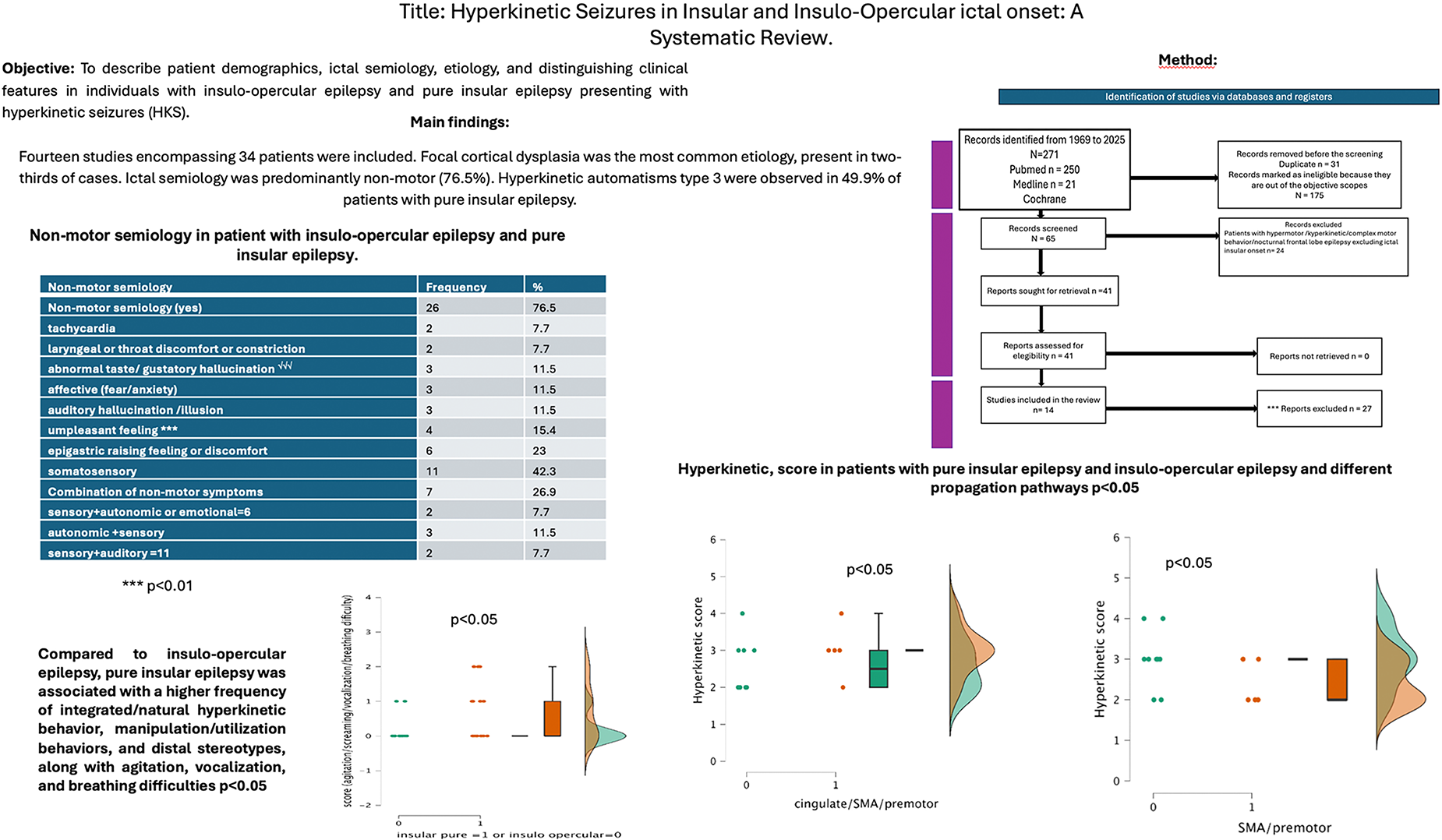
Keywords
Introduction
According to the ILAE, hyperkinetic seizures (HKS) refer mainly to the quantitative dimension of ictal motor activity, characterized by an excessive amount, rate, and acceleration of movement. The resulting motor behavior may appear integrated with physiological movement patterns, although it is usually exaggerated and may, in some cases, become non-integrated or unnatural, sometimes accompanied by facial expression or vocalization. In this context, integrated behavior denotes semipurposeful, naturalistic motor activity forming a recognizable behavioral sequence, such as singing, clapping, object manipulation, or marked emotional expression, even when exaggerated or socially incongruent. By contrast, fragmented behavior refers to disorganized, non-naturalistic motor activity lacking a coherent sequential structure. Similarly, stereotyped behavior refers to excessive repetition of the same motor act, including rhythmic repetitive movements of the trunk and proximal limbs or of the hands and feet, whereas non-stereotyped behavior describes more variable motor patterns without fixed repetitive recurrence. In contrast, the term hypermotor is broader and encompasses not only the excess of movement but also its qualitative organization. It typically describes large-amplitude, vigorous, and often bizarre movements involving the proximal limbs and trunk, such as rocking, jumping, thrashing, pelvic thrusting, or kicking. Thus, whereas hyperkinetic emphasizes the quantity and speed of movement, hypermotor also incorporates the complexity, organization, and anatomical distribution of the ictal motor pattern. Although these terms are often used interchangeably in the epilepsy literature to describe complex motor behaviors distinct from simple motor signs, they should not be regarded as strictly synonymous
This distinction allows for a more nuanced characterization of motor phenomena within gestural motor behavior.1–4
HKS including hyperkinetic and hypermotor behavior have been observed in epilepsy arising from a range of cortical regions, including the prefrontal, orbitofrontal, cingulate, dorsolateral frontal, temporal, parietotemporal, parietal, occipital, and insulo-opercular areas. While the insulo-opercular network is highly relevant, it is important to note that hyperkinetic semiology is not exclusive to insular or frontal epilepsy, as demonstrated by Tinuper et al (2016).1–4
Insular and insulo-opercular seizures are often underdiagnosed, primarily due to incomplete intracranial exploration. However, a significant additional challenge lies in the inherent difficulty of recognizing insular semiology. The clinical presentation of insulo-opercular seizures frequently mimics frontal, temporal, or parietal lobe epilepsy, which can lead to misclassification even before invasive evaluation is undertaken. This semiological limitation warrants greater emphasis, as underdiagnosis is not solely a technical issue.5,6 Given that premises ictal semiology plays a critical role in guiding electrode implantation. However, insular implantation is technically challenging due to vascular risks and anatomical constraints, and improper implantation may adversely affect surgical outcomes. 7
This review aims to delineate the demographics, semiology, and etiology of HKS in insulo-opercular and pure insular epilepsy, and to identify possible distinguishing clinical features. Accurately distinguishing between insular and insulo-opercular seizure onset zones is essential for planning stereo-electroencephalography (SEEG) electrode implantation during the presurgical evaluation of patients with drug-resistant focal epilepsy. This distinction is not only important because the opercular regions should not be explored in isolation from the insular cortex, but also because seizures originating from these areas can closely mimic other types of epilepsy. A thorough understanding of the ictal semiology associated with insular and insulo-opercular regions is therefore critical to ensure these zones are appropriately considered when formulating the implantation hypothesis and to minimize the risk of mislocalization during presurgical planning.
Methods
Search Strategy
A systematic review was conducted in accordance with PRISMA guidelines.
8
Searches were performed in Embase, PubMed, Medline, and Cochrane databases for articles in English published up to January 10, 2025. Keywords included:
Hyperkinetic seizures Hypermotor epilepsy Sleep-related hypermotor epilepsy ictal hyperkinesia nocturnal paroxysmal dyskinesia/dystonia nocturnal frontal lobe epilepsy complex motor behavior Insular epilepsy Insulo-opercular epilepsy
The reviewers (RAM, NA, and TH) independently screened abstracts, reviewed full texts, and extracted data (Figure 1).
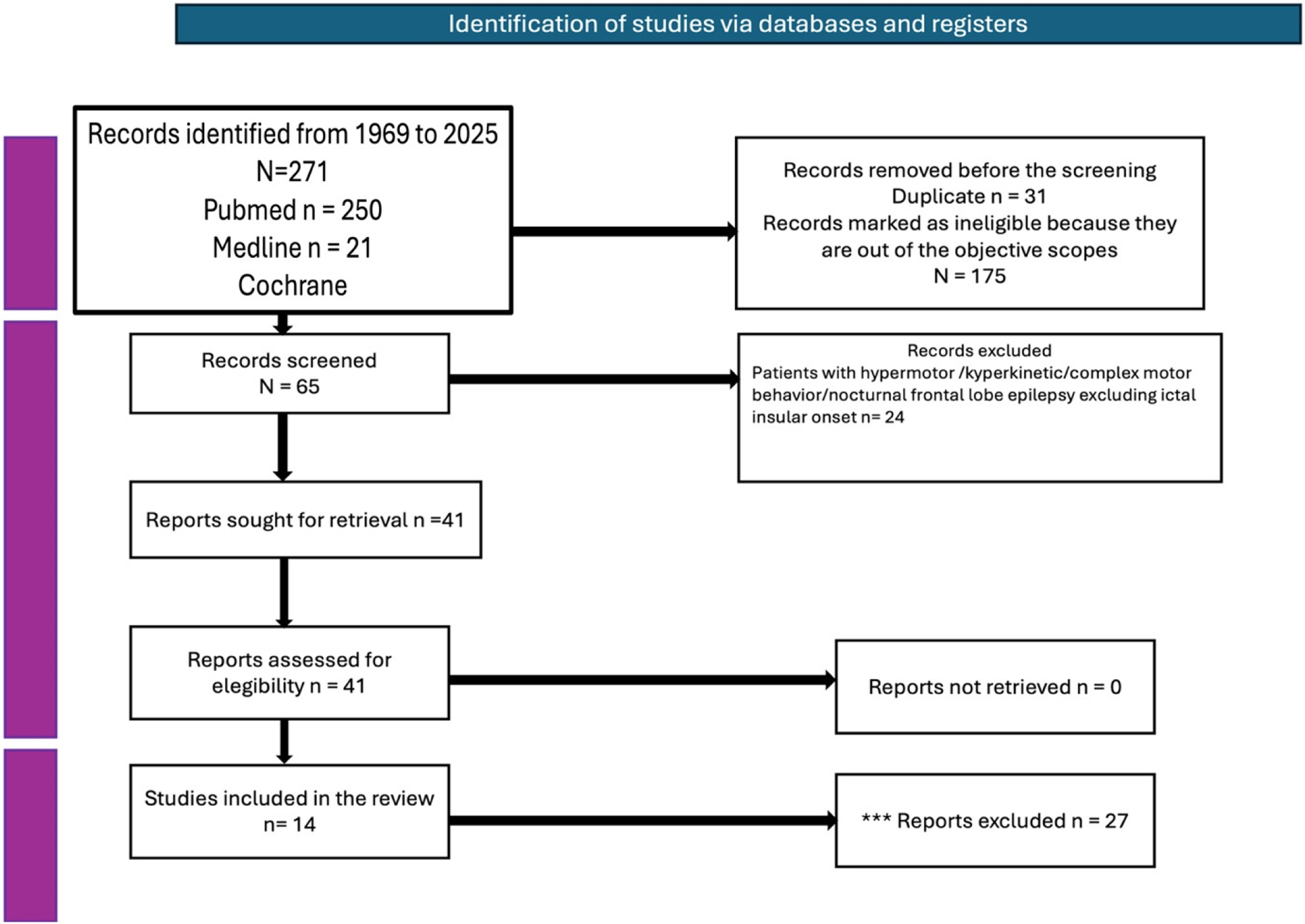
Shows a Modified PRISMA Flow Diagram Depicting the Studies’ Selection Process.
Inclusion Criteria
Patients with pure insular or insulo-opercular epilepsy presenting with HKS
SEEG and/or subdural recordings with contacts in the insular opercular cortex with or without electrocorticography (ECoG) confirming ictal onset zone.
If a subdural grid was used, at least the insular cortex was sampled with SEEG or resected during surgery to render the patient seizure-free.
Case reports, case series, and retrospective studies
Clear description of ictal semiology and surgical outcomes (Engel Class I)
Minimum 6-month postoperative follow-up
Exclusion Criteria
Incomplete data on ictal semiology, ictal onset zone, MRI findings, or surgical outcomes
Articles not published in English.
Participants
Included studies evaluated both pediatric and adult populations.
Quality Assessment
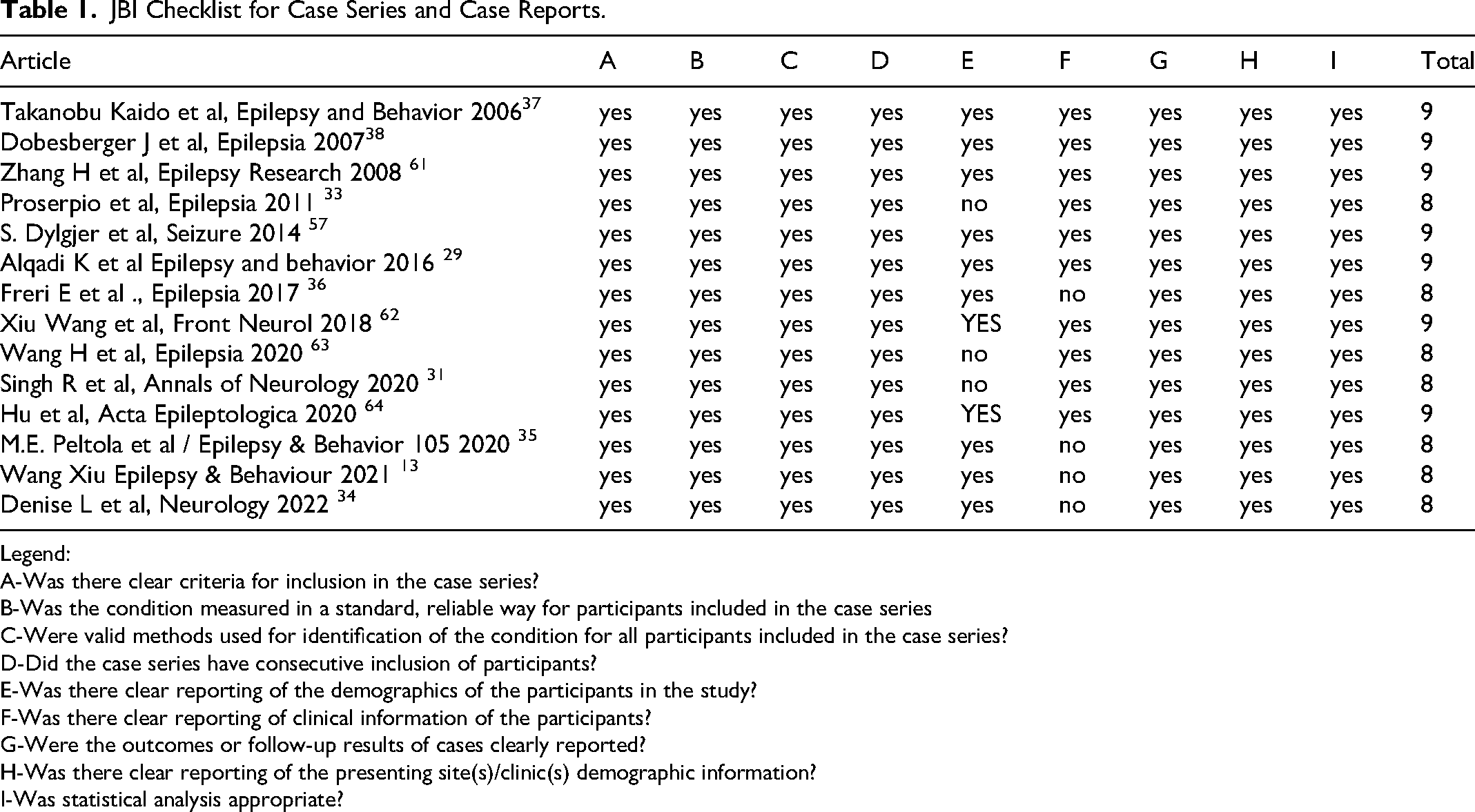
Risk of bias was assessed using the JBI checklist (Joanna Briggs Institute Model of Evidence-Based Healthcare questionnaire) 9 for case series and case reports. Seven studies scored 9, and seven scored 8, indicating high methodological quality. The author's interrater reliability scoring the risk of bias was (Cohen's κ = 0.93) (Table 1).
JBI Checklist for Case Series and Case Reports.
Legend:
A-Was there clear criteria for inclusion in the case series?
B-Was the condition measured in a standard, reliable way for participants included in the case series
C-Were valid methods used for identification of the condition for all participants included in the case series?
D-Did the case series have consecutive inclusion of participants?
E-Was there clear reporting of the demographics of the participants in the study?
F-Was there clear reporting of clinical information of the participants?
G-Were the outcomes or follow-up results of cases clearly reported?
H-Was there clear reporting of the presenting site(s)/clinic(s) demographic information?
I-Was statistical analysis appropriate?
Data Management
For each study meeting the inclusion criteria, the following variables were extracted and compiled into a dataset for further analysis: age at epilepsy onset and at time of surgery, gender, etiology, surgical topography (eg, anterior/posterior insular, insulo-opercular frontal/parietal/central/temporal), anatomical localization of ictal onset; type of intracranial evaluation (SEEG, subdural grid, or both), duration of follow-up, histopathology; and ictal semiology.
These variables were systematically organized for statistical analysis and anatomo-clinical correlation.
Data Extraction and Definitions of Variables
Data Extraction
From each selected publication, the number of patients with relevant data was recorded, with emphasis on semiology, epileptogenic zone, surgical type, and anatomo-clinical correlations.
Semiology-Based Scoring Systems
To enable consistent statistical analysis across diverse clinical descriptions, three semiology-driven scoring systems were developed: 1.-Hyperkinetic Seizure Scale; 2.- Non-Motor Semiology Scale; 3.-Agitation/Vocalization/Grimacing/Breathing Difficulty (AVGB) Scale. These systems capture features most consistently reported across studies and reflect known relationships between seizure semiology and symptomatogenic brain regions.
Hyperkinetic Seizure Scale
This scale models the expected progression of seizure semiology across distinct cortical networks. For instance, early clonic activity (primary motor cortex) is distinguished from axial tonic/dystonic posturing (premotor regions). More complex, naturalistic hyperkinetic behaviors (eg, kicking, pedaling, rocking) are categorized separately, reflecting prefrontal and medial frontal involvement.10–15 The highest score captures integrated gestural or negative affective behaviors (fear, rage, wandering), commonly linked to mesial temporal, orbitofrontal, and ventromedial prefrontal networks.16–23
Non-Motor Semiology Scale
This parallel framework considers the absence of aura as consistent with non-eloquent cortical onset. Single or multiple non-affective auras indicate involvement of eloquent or multimodal regions. Affective auras, often tied to mesial temporal or orbitofrontal networks, receive higher scores for their specific localization value.
AVGB Scale
A four-item behavioral scale was created to capture agitation, vocalization, grimacing, and breathing difficulty—features associated with activation of the insular cortex, mesial frontal regions,24–26 cingulate cortex, and temporal lobe structures.27,28 These symptoms are scored independently due to variable reporting and cannot be reliably integrated into a composite hyperkinetic scale.
Comparison with Fayerstein et al (Epilepsia 2016) 14
The validated Fayerstein hyperkinetic seizure scoring system 14 was not applied because required elements (speed/intensity of movements, latency, presence of rhythmic/repetitive movements) were inconsistently described in the available datasets. The new scoring systems rely only on semiologic details consistently extractable from all included studies, minimizing missing data and ensuring broad applicability.
Hyperkinetic Seizure Scale (1-4):
Early clonic signs + hyperkinetic automatisms No early clonic signs + unnatural hyperkinetic behaviors, proximal/axial tonic/dystonic posturing, trunk rotation No early clonic signs + natural/integrated hyperkinetic behaviors (kicking, rocking, pedaling), manipulation/utilization behaviors, distal stereotypies No early clonic signs + integrated gestural behaviors with negative emotional expression (fear, anxiety, rage), speech production, epileptic wandering
Non-Motor Semiology Scale (0-4)
0 – No aura 1 – One non-affective aura 2 – Two or more non-affective auras 3 – Affective aura 4 – Two or more auras plus affective aura
AVGB Scale (0-4)
0 – None 1 – One symptom 2 – Two symptoms 3 – Three symptoms 4 – All four symptoms
Insular seizures produce complex autonomic, sensory, affective, respiratory, and motor manifestations due to the insula's deep location and extensive connections with limbic, frontal, temporal, parietal, and brainstem networks. The AVGB components align closely with documented insular ictal features and activation of different insular regions24–26:
Agitation
Reflects activation of insular networks involved in viscerosensation, pain, emotional processing, and autonomic arousal. May also indicate rapid spread to motor/behavioral networks.24–26
Vocalization
Common due to strong insular connections with laryngeal, respiratory, and limbic pathways. Symptoms include laryngeal constriction, throat discomfort, dysarthria, groaning, and unpleasant throat sensations.27,28
Grimacing
Indicates activation of affective, somatosensory, and pain-processing regions. Manifests as facial discomfort, pain-like expressions, and distorted facial movements.27,28
Breathing Difficulty
The insula's role in autonomic regulation makes breathing discomfort, dyspnea, chest/throat tightness, and altered respiratory patterns characteristic of insular ictal onset.27,28
Each author reviewed the ictal semiology of each patient and scored every patient with this proposed score system, and the interrater reliability was high (Cohen's κ = 0.72).
Ictal Seizure Onset Zone (SOZ) Classification
To clarify insular semiology comparisons across intra-insular localization and network-extent frameworks these regions were explicitly divided in two orthogonal axes: “anterior versus posterior insula” (this clinical-anatomic dichotomies define anterior vs posterior insula relative to the central insular sulcus, a key landmark demarcating anterior and posterior divisions (with different gyral patterns and cytoarchitecture gradients). Anterior/posterior is a within-insula topography label not a claim about whether the epileptogenic zone is confined to the insula. “Pure insular” versus “insulo-opercular” categorization addresses epileptogenic network extent: whether the ictal onset zone is restricted to the insula/peri-insular sulcus versus insula plus adjacent opercular cortex at onset and/or as an essential component of the epileptogenic network.
The distinction between “pure insular” and “insulo-opercular” localizations is based exclusively on SEEG-defined seizure onset zones. Specifically, “pure insular seizure onset” refers to cases where the ictal onset is confined to the insular cortex and peri-insular sulcus, as determined by SEEG findings, while “insulo-opercular epilepsy” includes cases where the ictal onset extends into adjacent opercular regions.
SOZ data were extracted from tables and figures in each study and grouped into:
Pure insular ictal onset. Insulo-opercular ictal onset. Anterior Onset: Insular cortex + precentral areas. Central Onset: Insular cortex + central region. Posterior Onset: Insular cortex + temporoparietal regions.
Note: Ventral/dorsal axial regions were excluded due to inconsistent reporting.
Assessment of Seizures Propagation Pathway
Propagation pathways were systematically evaluated by extracting descriptions of the brain structures involved during hyperkinetic seizure behaviors from each included study. The analysis focused on identifying which cortical regions were recruited during the evolution of hyperkinetic seizures, as reported in the anatomo-clinical and electrographic correlation data.
The studies were reviewed for explicit mention of propagation patterns, including the onset zone and subsequent spread to adjacent regions. SEEG (stereo-electroencephalography) findings were used to determine the sequence of regional involvement during seizures. Three out of fourteen studies did not assess or report the structures involved in the generation of hyperkinetic seizures (Alqadi et al, Wang H et al, and Singh et al).29–31 Only consistently reported pathways were included in the final analysis
Statistical Analysis
Statistical analysis was performed using JASP, a cross-platform software supporting both frequentist and Bayesian methods. We first analyzed the agreement between the examiners’ scoring of the risk of bias, HKS scale, non-motor semiology scale, and Agitation/Vocalization/Grimacing /Breathing Difficulty Scale by calculating Cohen's kappa.
32
Bayesian Model Averaging was used to pool quantitative variables (eg, age), assuming no variance in actual effect sizes (τ = 0) under the random-effects model. Descriptive Statistics: Frequencies and percentages were reported for ictal symptoms and signs. Inferential Statistics:
Chi-square tests were used for qualitative variable comparisons.
Mann-Whitney U tests (non-parametric t-test analog) were applied to compare semiology scores across anatomical locations.
Bonferroni correction was used to adjust the alpha risk for multiple comparisons.
Raincloud plots were employed to visualize raw data, distributions, and summary statistics, combining violin plots, box plots, and scatter plots.
Statistical significance was set at p < 0.05. Areas with n < 3 were excluded from analysis.
Results
Summary of Included Studies
Fourteen studies met the inclusion criteria, encompassing a total of 34 patients with hyperkinetic seizures (HKS) who underwent epilepsy surgery and achieved seizure freedom at the time of publication (Engel I). Follow-up durations ranged from 6 months to 19.3 years. Intracranial recordings were performed using stereo-electroencephalography (SEEG) in 11 studies, subdural grid (SDG) in 1 study, and combined SEEG and SDG in 2 studies (see Table 2). Supplemental Material Table 1 lists excluded studies focused on insulo-opercular epilepsy, with reasons for exclusion provided (Table 2).
General Characteristics of Studies.
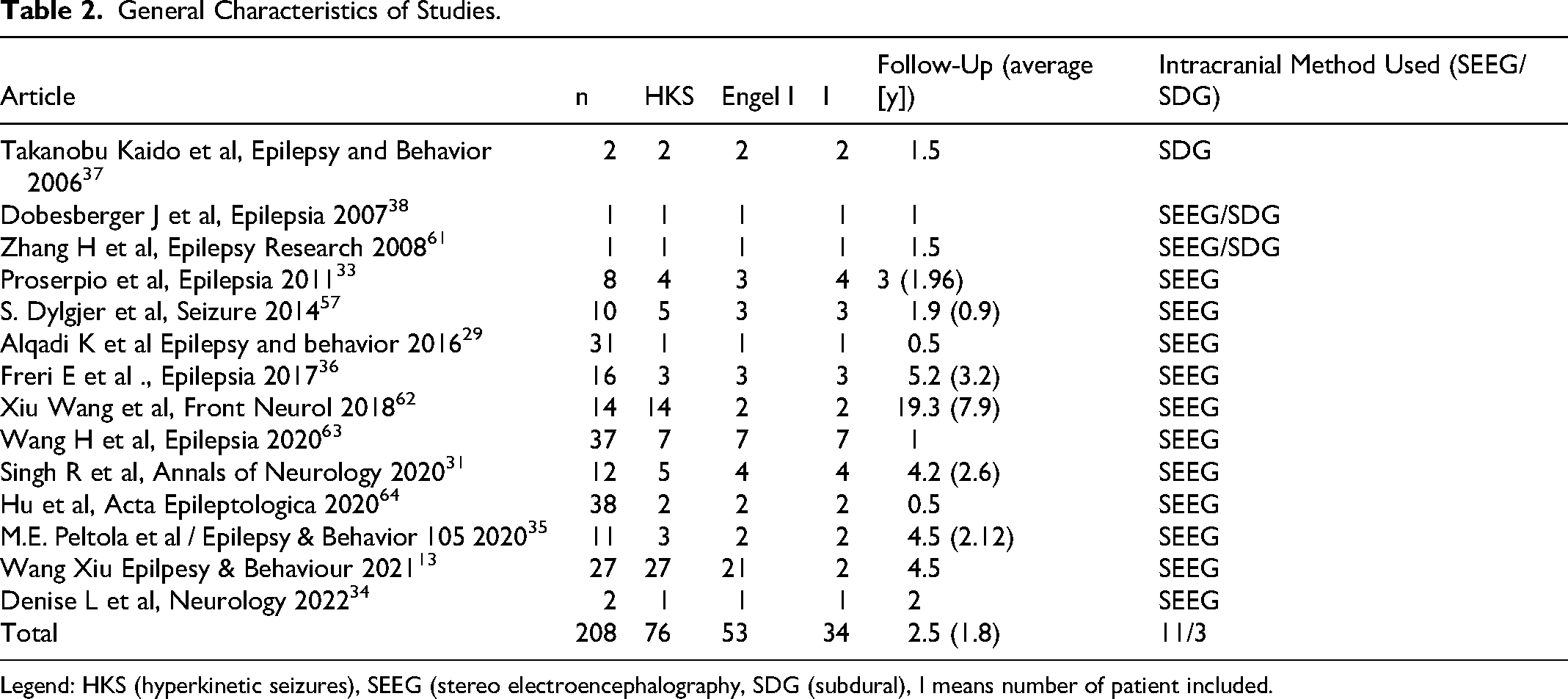
Legend: HKS (hyperkinetic seizures), SEEG (stereo electroencephalography, SDG (subdural), I means number of patient included.
Bias in Reporting
Several limitations and inconsistencies were noted across studies:
Proserpio et al and Wang et al did not report individual ages at epilepsy onset or surgery; only averages were provided. 33
Freri et al, Peltola et al, and Denise et al did not specify the type of HKS in four patients34–36
Alqadi et al, Wang H et al, and Singh et al did not describe the anatomical structures involved during HKS29–31
Wang H et al did not report histopathological findings. 30
We found that presurgical evaluation data were inconsistently reported across the studies, which limited our ability to perform a structured analysis (see Supplementary Material Table 1). This variability and incomplete reporting of non-invasive presurgical data precluded a comprehensive analysis.
Age at Seizure Onset, Surgery, Engel Score and Follow-Up
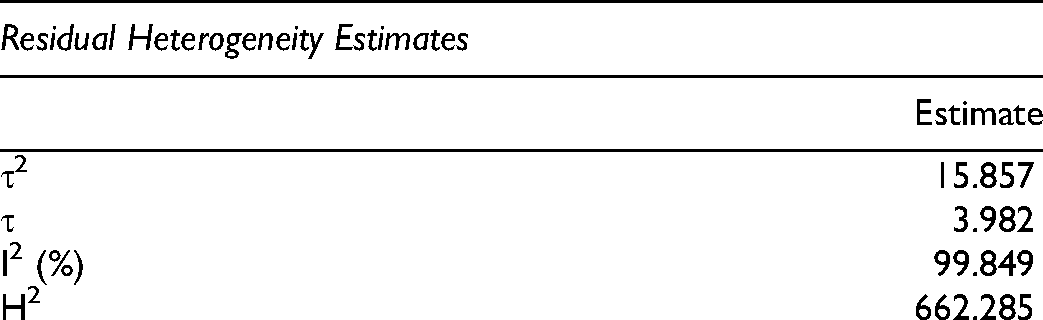
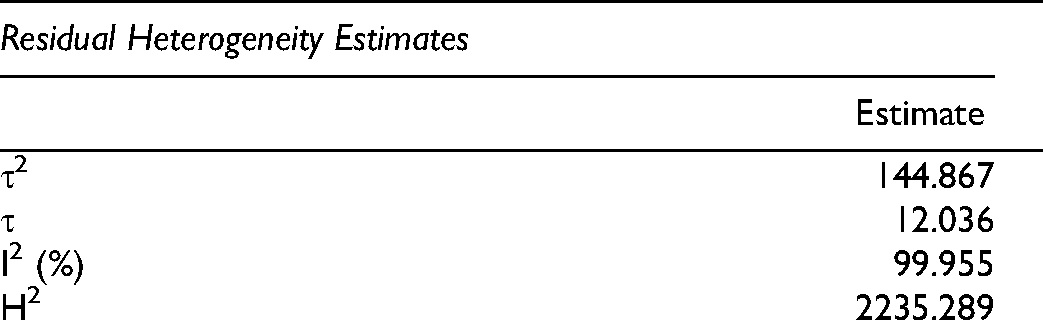
The mean age at seizure onset among patients was 7.67 years, with a range spanning from 5.14 to 10.2 years. This measure demonstrated considerable variability (T2 = 15.6; I2 = 99.8%) (Figure 2). The average age at the time of surgery was 21.6 years (range: 14.31-29.02 years), again reflecting substantial heterogeneity (I2 = 99.9%). The mean follow-up period after surgery was 3.84 years, ranging from 1.08 to 6.61 years, and this too showed high variability (T2 = 24.9; I2 = 99.87%). Notably, all patients included in the study achieved seizure freedom, corresponding to an Engel class I outcome (100%) (Figure 3).
Average Age at Seizure Onset by Study.
Average Age at the Time of Surgery by Study.
3.4 Ictal onset zone and areas involved in hyperkinetic seizure semiology:
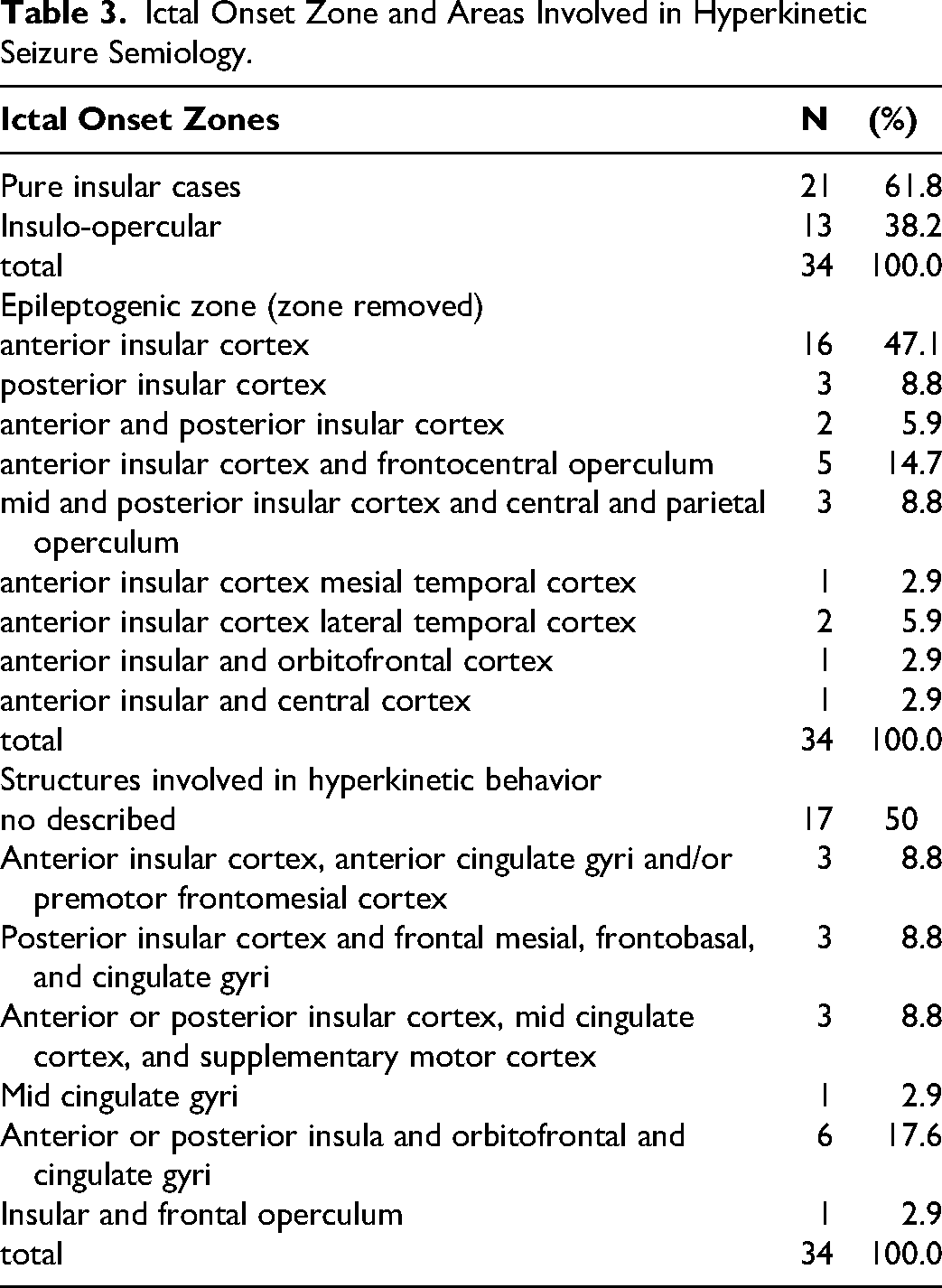
Twenty-one (61.8%) of reported patients had pure insular onset, whereas thirteen (38.2%) of patients had the operculum as part of the ictal onset (insulo-opercular). Most patients with HKS have an onset in the anterior insular cortex (47.1%). The most common opercular region involved in the ictal onset was the frontocentral operculum, seen in five patients (14.7%) (Table 3).
Ictal Onset Zone and Areas Involved in Hyperkinetic Seizure Semiology.
Etiology of Insular and Insulo-Opercular Ictal Onset with Hyperkinetic Seizures
Nineteen patients (73.1%) had a focal cortical dysplasia, including six with FCD type 1 (23.1%), three with no further classified FCD (11.5%), and ten patients (38.5%) with FCD type 2. Other etiologies can be revised in Table 4. The histology was not reported in eight of 34 patients (see study by Wang H et al, Epilepsia 2020). 30
Etiology of Epilepsy with Insulo-Opercular Seizure Onset and Hyperkinetic Seizures.
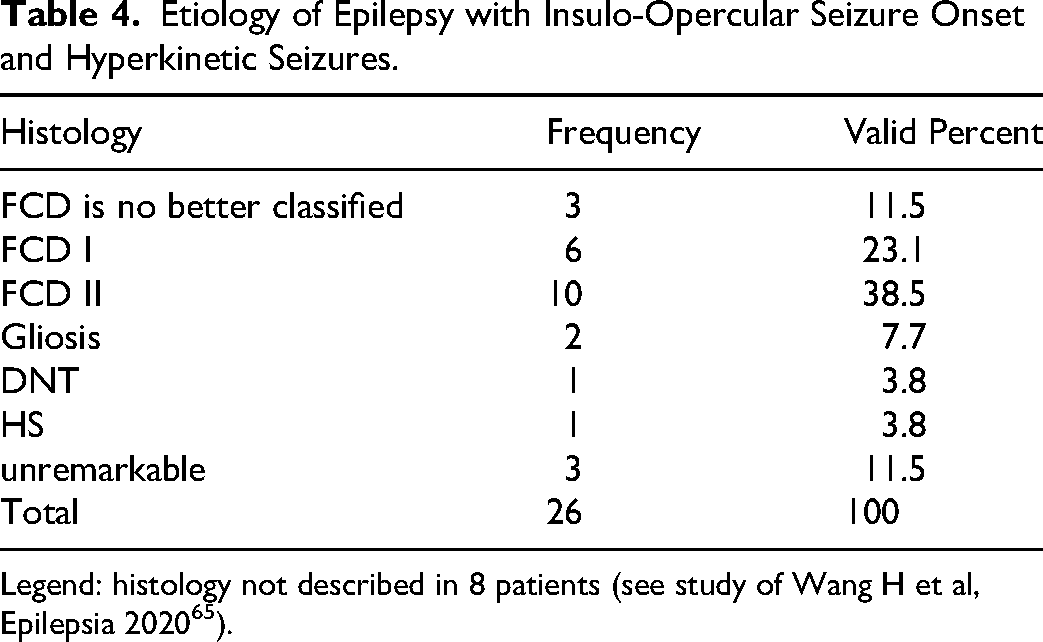
Legend: histology not described in 8 patients (see study of Wang H et al, Epilepsia 2020 65 ).
Ictal Semiology
Non-motor semiology is presented in 26 patients out of thirty-four (76.5%). The most common non-motor symptoms were somatosensory symptoms, observed in 11 patients (42.3%). Tachycardia and laryngeal or throat discomfort or constriction were seen in two patients (7.7%) (Table 5). A complete description of non-motor symptoms can be found in Supplemental Material (Table 2).
Non-Motor Semiology in a Patient with Insulo-Opercular and Pure Insular Ictal Onset.
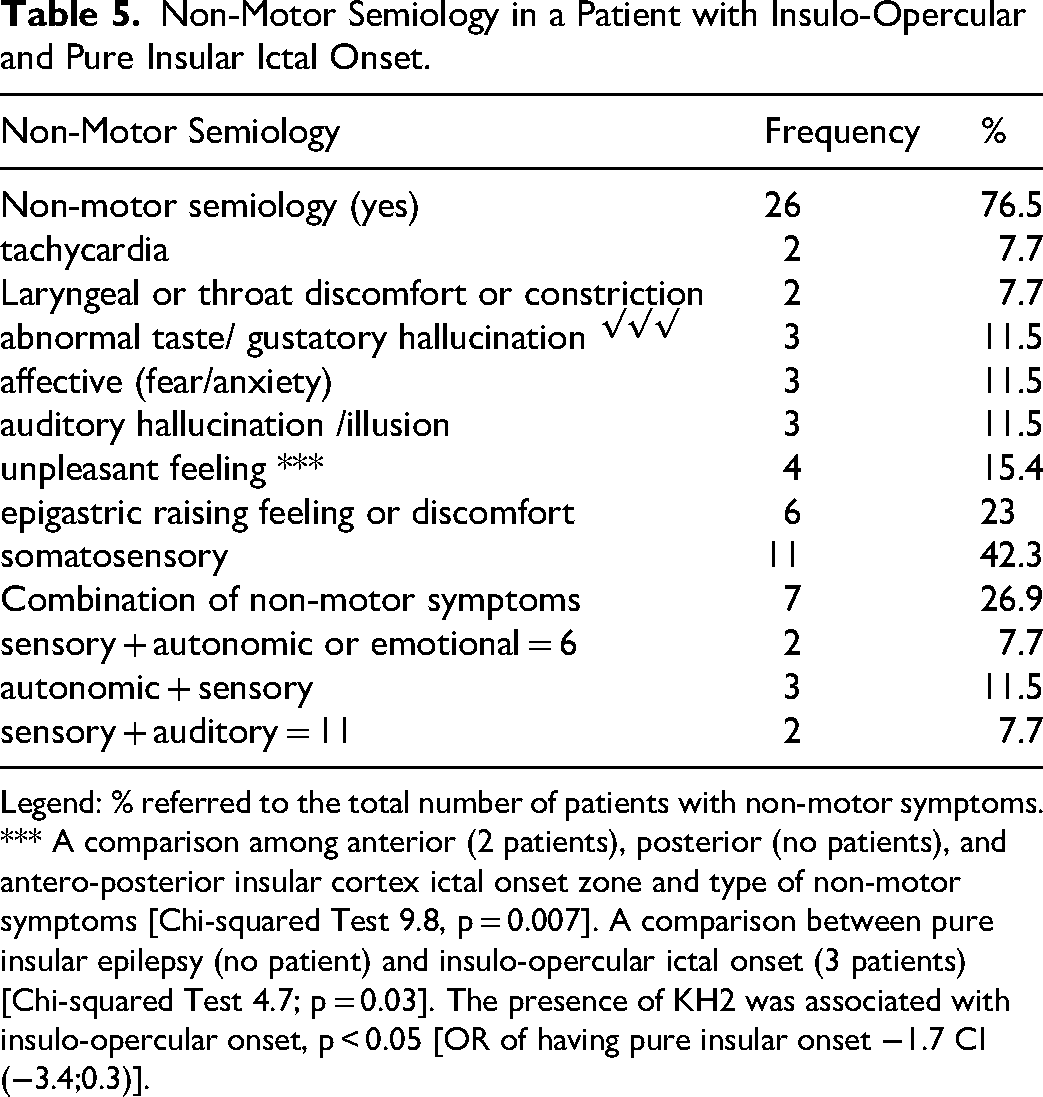
Legend: % referred to the total number of patients with non-motor symptoms. *** A comparison among anterior (2 patients), posterior (no patients), and antero-posterior insular cortex ictal onset zone and type of non-motor symptoms [Chi-squared Test 9.8, p = 0.007]. A comparison between pure insular epilepsy (no patient) and insulo-opercular ictal onset (3 patients) [Chi-squared Test 4.7; p = 0.03]. The presence of KH2 was associated with insulo-opercular onset, p < 0.05 [OR of having pure insular onset −1.7 CI (−3.4;0.3)].
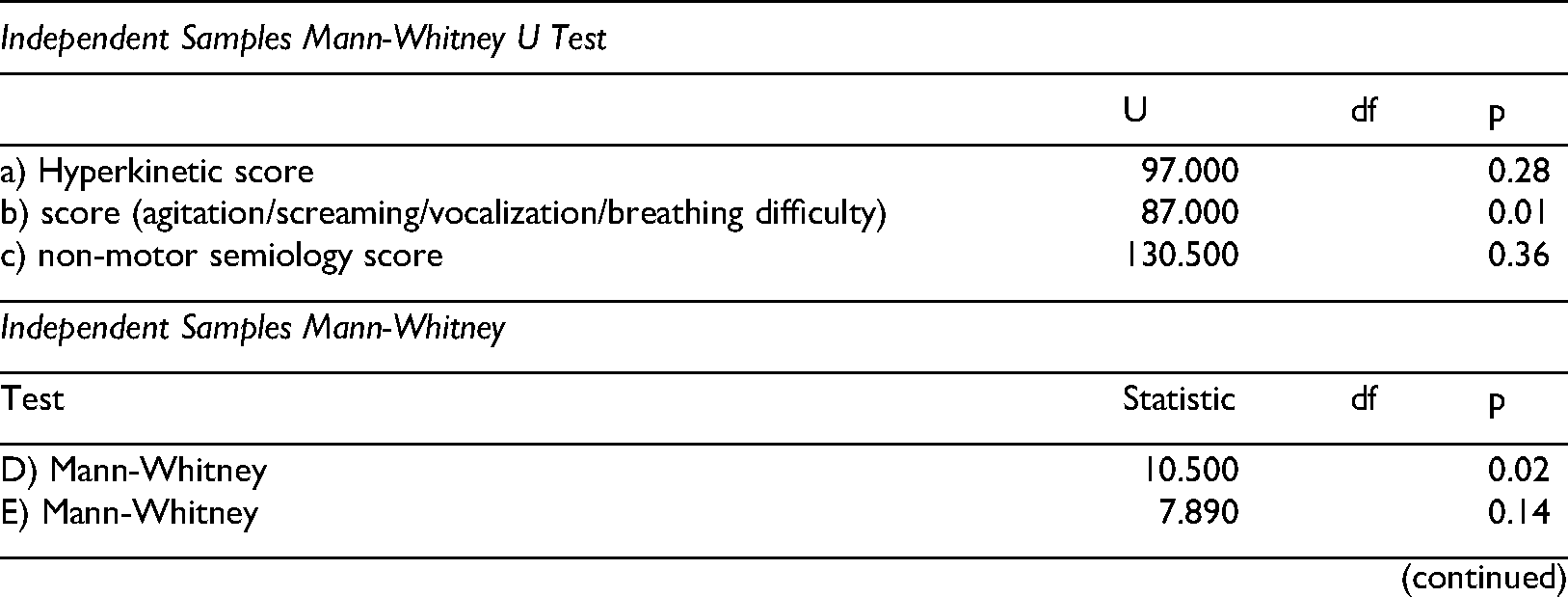
Only thirty out of thirty-four patients with HKS, had a clear description of their HKS type (see bias in reporting 3). The HKS types of these 30 patients are shown in (Table 6). Most patients with insulo-opercular and pure insular ictal onset presented with HKS classified as HK2 (26.6%) or HK3 (49.9%) (Table 6). A complete description of hyperkinetic behavior can be reviewed in Supplementary Material Table 3. Patients with insulo-opercular ictal onset had HK2 more frequently than patients with pure insular ictal onset (p < 0.05) OR – 1.7 CI (−3.4 −0.3). No significant statistical differences were found comparing anterior versus posterior insular ictal onset (Chi-squared p > 0.05). There were no differences in the hyperkinetic score between patients with pure insular ictal onset and patients with insulo-opercular ictal onset (p > 0.05) (Figure 5a). Regarding the agitation/screaming/vocalization/breathing difficulty score, patients with pure insular seizure onset have one or two of these symptoms. In contrast, patients with insulo-opercular ictal onset do not (p < 0.05) (see graphic 5b, 1.5* IQR, and the upper Hinge (Interquartile Range) reach 1 to 2. There is no difference between insulo-opercular and pure insular seizure onset regarding non-motor semiology score (median is 0 in both), p > 0.05 (Figure 5c).
Hyperkinetic Semiology in a Patient with Insulo-Opercular and Pure Insular Ictal Onset.
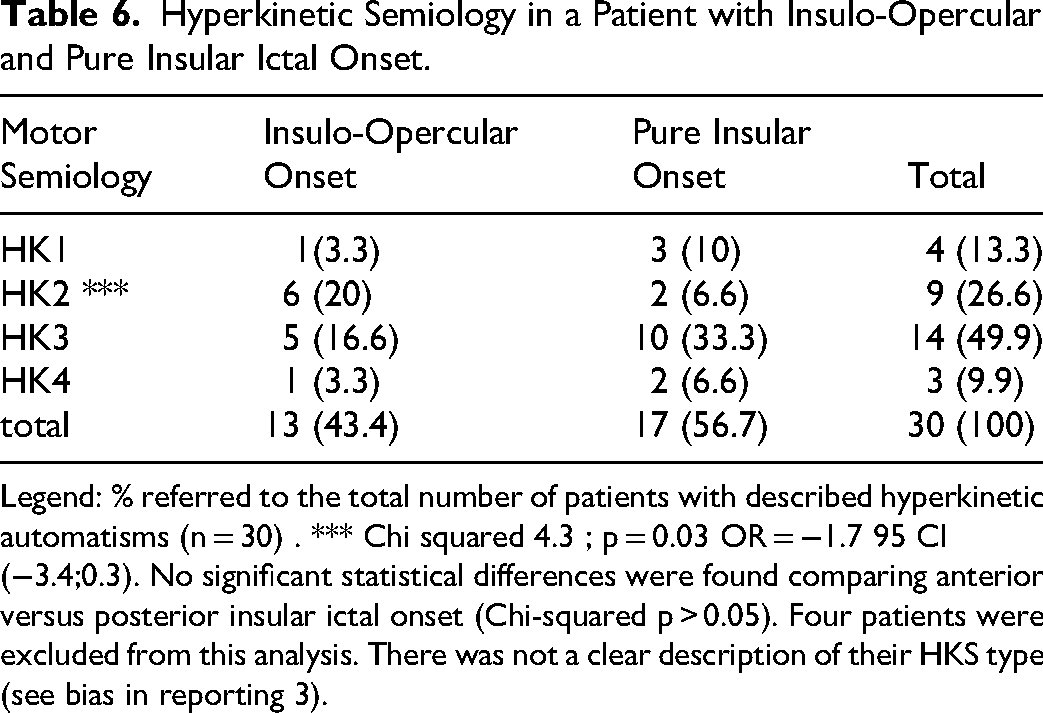
Legend: % referred to the total number of patients with described hyperkinetic automatisms (n = 30) . *** Chi squared 4.3 ; p = 0.03 OR = −1.7 95 CI (−3.4;0.3). No significant statistical differences were found comparing anterior versus posterior insular ictal onset (Chi-squared p > 0.05). Four patients were excluded from this analysis. There was not a clear description of their HKS type (see bias in reporting 3).
Propagation analysis was available for 17 of 34 patients. Within this subset, certain propagation pathways appeared to be associated with specific hyperkinetic seizure types; however, given the limited sample size and heterogeneity of the subgroup, these findings should be interpreted cautiously. For example patients with a propagation pathway to the premotor and SMA areas had a median hyperkinetic score of 2, which was statistically significant compared to patients with HKS via a different pathway (p < 0.05). A patient with a propagation pattern to fronto-basal structures and cingulate cortex had a median hyperkinetic score of 3 and an upper whisker of 4, which was statistically significant compared to other pathways during HKS (p < 0.05) see (Figure 5 d, e, f).
Discussion
In this systematic review consisted exclusively of Engel I patients, selected from 14 articles and totaling 34 individuals with insulo-opercular or pure insular ictal onset who remained seizure free during follow-up. This is, to our knowledge, the first systematic review on hyperkinetic seizures in insulo-opercular epilepsy. This review primarily offers a descriptive synthesis of the available evidence, and any analytical inferences should therefore be interpreted cautiously. A clearer distinction between the reporting of observed patterns and the drawing of broader conclusions is warranted, particularly given the several methodological limitations of the underlying studies: first, we fully acknowledge that the sample size in our review is small, and as such, the comparative statistical analyses should be interpreted with caution. We emphasize that these findings are exploratory and intended to generate hypotheses rather than provide definitive conclusions. The sample size also limites generalizability of our results and the need for larger, prospective studies to validate these observations; Second, patient selection could introduce a bias since several articles included in this review investigated insulo-opercular ictal onset but were not explicitly designed to address epilepsy with hyperkinetic seizures; third, there was a heterogeneity among studies regarding the method to explore the insulo-opercular region intracranially (11 studies used SEEG, one used SDG, and two studies combined both modalities (Table 2). However, since all patients underwent insulo-opercular resection and were seizure-free after a long period of time, the assumption that the insular cortex was involved in the generation of HKS could be assumed with a high level of confidence. There is significant heterogeneity among the data in each included study, depending on its purpose. For example, the semiology was described in detail when the focus was on anatomo-clinical correlation, or it was brief when the objective was postsurgical seizure outcome. Fourth, the age at onset of epilepsy, at the time of epilepsy surgery, and follow-up time are heterogeneous and not reported by all authors for each patient. As such, for some studies, the average of reported ages and follow-up time was used instead. Fifth, there were four patients in whom the hyperkinetic automatism was not described; Sixth, the intracranial structure involved during the hyperkinetic semiology was not reported in all studies included in the review; seventh; the histopathology was not reported in 8 patients; eighth because the terms “hypermotor” and “hyperkinetic seizures” have only recently entered common usage, we may have inadvertently excluded relevant older studies. Earlier literature frequently used terms such as “ictal hyperkinesia,” “complex motor seizures,” “nocturnal frontal lobe epilepsy,” and “nocturnal paroxysmal dyskinesia/dystonia.” This is especially important given recent evidence indicating that many cases previously classified as nocturnal frontal lobe epilepsy may originate outside the frontal lobe, including the insular region. We recognize this as a limitation; nineth the three semiology-based scoring scales are currently unvalidated externally and were applied to the same dataset from which they were derived. This introduces circularity and likely inflates apparent performance, so the findings should be considered preliminary until confirmed in an independent cohort. A key limitation is that all three semiology-based scores were derived and tested in the same dataset, without external or independent validation. This creates a circular evaluation framework, increasing the risk of overfitting and optimistic estimates of diagnostic performance. Because a model or score usually performs best in the dataset that created it. When derivation and testing happen in the same sample, the score may look more accurate, discriminative, or clinically useful than it really is. That means the reported performance may not generalize to new patients, new centers, or routine practice.
The inclusion of both SEEG and subdural studies in this systematic review is problematic, as these two methodologies do not allow the same degree of precision in anatomic localization. In one of the papers cited, for example, using subdural grid exploration (reference 10 in the paper), the insular involvement was suspected because of abnormal MRI signal rather than electrophysiological data. The patient in question had resection of both insula and temporal cortex, such that the true SOZ and relation to hyperkinetic semiology are difficult to confirm. However, in this review, we included not only pure insular ictal onset but also insulo-opercular ictal onset, including insulo-temporal operculum. Besides, these patients had a lesion in the insular cortex, and the resection, including the insular cortex, rendered the patient seizure-free. 37 It would have been informative to consider the timing of hyperkinetic semiology appearance regarding other features, since the latency until onset of hyperkinetic behavior has been described as a feature distinguishing frontal from extra-frontal onset. However, since this is not reported in all studies, it was not possible to do this analysis. Another possible limitation is that the score system used here has not been previously validated.
Nevertheless, in the method section, we explained why that was necessary. Furthermore, each author reviewed the ictal semiology of each patient and scored every patient with this proposed score system, and the interrater reliability was high (Cohen's κ = 0.72). This indicates a good inter-rater reproducibility of the score.
Notably high prevalence of focal cortical dysplasia (FCD) type I (23.5%) [Table 4] was observed in this review. This finding likely underscores inherent limitations in current diagnostic methodologies, particularly in cortical regions that are not comprehensively sampled by intracranial electrode placement. The possibility exists that subtle dysplastic lesions within frontal or opercular areas may evade detection, thereby complicating the accurate delineation of seizure onset and propagation pathways. Consequently, these observations highlight the imperative for thorough intracranial exploration and the integration of advanced neuroimaging techniques to mitigate the risk of undiagnosed pathology in adjacent cortical territories.
Lastly but not less important we acknowledge that presurgical evaluation data were inconsistently reported across the studies, which limited our ability to perform a structured analysis (see Supplemental Material Table 1).
Despite these limitations, the assessment of risk of bias using the quality score [JBI checklist for case series and case reports] showed that the JBI score was 8 to 9 in 100% of studies included in this systematic review. This means that the data gathered from the included studies had good quality. Moreover, all included patients remained seizure-free during the follow-up period, with a mean follow-up time of 3.84 years, ranging from 1.08 to 6.61 years (Figure 4). This warrants that the epileptogenic zone was correctly removed.
Average of Postsurgical Follow-up in Years by Study.
Hyperkinetic, Non-motor Symptoms and Agitation/Screaming/Vocalization/Breathing Difficulty Score in Patients with Pure Insular Epilepsy and Insulo-opercular Epilepsy and Different Propagation Pathways.
Significant Findings
This systematic review reveals several important insights into hyperkinetic seizures (HKS) in insular and insulo-opercular ictal onset: 1.- More than half of the patients (61.8%) had a pure insular ictal onset zone, with the anterior insular cortex being the most frequent site of ictal onset (47.1% pure anterior, 5.9% antero-posterior); 2.- during HKS, seizure activity often propagated to extra-insular structures, including the anterior/mid-cingulate cortex, basal frontal cortex, frontomesial cortex, and supplementary motor area (SMA). Only one patient (2.9%) lacked involvement of these regions during HKS. 38 The interpretation of the propagation analysis warrants caution. Because propagation data were available for only half of the cohort (17/34 patients), the analysis was performed in a reduced and heterogeneous subset, which limits both statistical robustness and clinical generalizability. Therefore, the observed relationships between propagation pathways and hyperkinetic seizure types should be considered hypothesis-generating rather than conclusive anatomoclinical associations ; 3.- FCD was the most common etiology, found in 73.1% of patients with reported histopathology; 4.- non-motor symptoms were present in 76.5% of cases, with somatosensory symptoms being the most common (42.3%); 5.- most patients exhibited either (HK2: Unnatural hyperkinetic behaviors, proximal/axial tonic or dystonic posturing, trunk rotation (26.6%) or HK3: Integrated/natural hyperkinetic behaviors (eg, kicking, rocking, pedaling), manipulation/utilization behaviors, distal stereotypes (49.9%); 6.- semiology differences by ictal onset zone (patients with pure insular ictal onset more frequently exhibited HK3 behaviors and agitation/screaming/vocalization/breathing difficulty (p < 0.05).
Seizure Symptoms
Our findings align with prior studies on insular epilepsy, confirming that non-motor symptoms—particularly somatosensory, epigastric, laryngeal, and autonomic—are common in pure insular-onset seizures.
Somatosensory Symptoms: These were the most frequently reported, including paresthesia and anesthesia in regions such as the head, neck, chest, perioral area, and upper limbs. Notably, these symptoms did not follow a Jacksonian march or somatotopic distribution typical of primary somatosensory cortex seizures5,39 Anterior versus Posterior Insular Onset: Contrary to previous hypotheses,
40
we did not find a significant association between somatosensory symptoms and posterior insular onset. However, unpleasant sensations were significantly associated with anterior insular onset (Chi-squared = 9.8, p = 0.007). Painful Seizures: Only three patients reported pain (abdominal or shoulder), with no correlation to insular subregions. This challenges prior assumptions linking painful seizures to posterior insular or secondary somatosensory cortex involvement41,42 Laryngeal and Throat Constriction: These symptoms, often considered hallmark signs of insular epilepsy,43,44were rare in our cohort (7.7%). This contrasts with other reviews reporting rates as high as 90%.
44
No significant association was found between these symptoms and ictal onset localization, likely due to the small sample size. Autonomic Symptoms: Independent autonomic features (eg, epigastric sensation, tachycardia, hypersalivation, apnea) were present in 34.6% of patients with non-motor symptoms. This is lower than previously reported rates (eg, 73% in Peltola et al35,45). While autonomic symptoms are known to arise from insular pole and middle short gyrus stimulation,
46
we found no significant localization correlation in our cohort.
Gustatory, Auditory, and Emotional Symptoms
Gustatory hallucinations were reported in three patients, all of whom had insulo-opercular ictal onset. No patients with pure insular onset described gustatory symptoms (p < 0.05, Table 5). This finding aligns with previous literature suggesting that gustatory hallucinations are more frequently associated with insulo-opercular epilepsy than pure insular epilepsy.44,47 However, it is known that insular cortex epilepsy can occasionally produce gustatory hallucinations,44,47 the low incidence in our cohort may reflect sample bias or limitations in electrode coverage.
Auditory symptoms were reported in three patients (11.5%), consistent with previous reports of auditory disturbances in insular epilepsy. 47 Patients described high-pitched voices or distorted sounds, suggesting involvement of the temporal operculum and posterior long gyrus of the insula. These findings support the insula's role in auditory processing and modulation, particularly during late-stage sound perception
Emotional symptoms, such as anxiety and fear, were reported in three patients (11.5%). These symptoms are consistent with the insula's known connections to the amygdala and caudate nucleus, which are involved in emotional regulation and fear processing.48,49 This supports the hypothesis that ventral insular involvement may contribute to emotional disturbances during seizures.
Motor Semiology in Hyperkinetic Seizures
Most patients in this review exhibited HK2 (26.6%) or HK3 (49.9%) hyperkinetic automatisms (Table 6), consistent with prior studies on insulo-opercular epilepsy:
HK2: Characterized by unnatural hyperkinetic behaviors, proximal/axial tonic or dystonic posturing, and trunk rotation. HK3: Defined by integrated/natural hyperkinetic behaviors (eg, kicking, rocking, pedaling), manipulation/utilization behaviors, and distal stereotypes.
These motor patterns were associated with distinct propagation pathways:
HK2: Linked to propagation to the premotor cortex and SMA. HK3: Associated with propagation to the fronto-basal cortex and cingulate gyrus.
These results emphasize that motor manifestation in seizure of insular onset are most likely attributable to early involvement of connected motor networks rather than the insular cortex alone.
Wang Xiu et al found significant hypometabolism in the cingulate motor area, SMA, and cingulate sulcus in patients with HKS, supporting early involvement of frontal motor structures. Their study also showed elevated epileptogenicity index (EI) values in these regions, reinforcing their role in complex motor behaviors. 50
Freri et al 36 and others have shown that complex motor signs typically emerge when ictal discharges spread to mesiofrontal regions. Pure insular onset is less frequently associated with these signs. The insulo-opercular network, with its extensive anatomical and functional connections, likely contributes to the hypometabolic patterns observed in these patients.
While pure insular cortectomy is rarely reported29,33,36 our review found that 61.8% of patients had pure insular epilepsy, suggesting that in the context of HKS, the insular cortex alone may be sufficient to generate these behaviors.
Rheims et al
49
further support this distinction, noting that:
Seizures from the anterosuperior insular cortex resemble nocturnal frontal lobe epilepsy, with dystonic, asymmetric posturing and less integrated motor behavior. Seizures from the posterior or anteroinferior insular cortex mimic temporal lobe epilepsy, with more integrated motor features.
This aligns with our findings that HK2 and asymmetric tonic posturing were more common in insulo-opercular ictal onset (p < 0.05, OR = –1.7, CI: −3.4 to −0.3), and that asymmetric tonic posturing was significantly more frequent in insulo-opercular onset than pure insular ictla onset.
Seizure Propagation and Motor Patterns (see Figure 6)
Seizure propagation pathways were strongly associated with specific hyperkinetic seizure types:
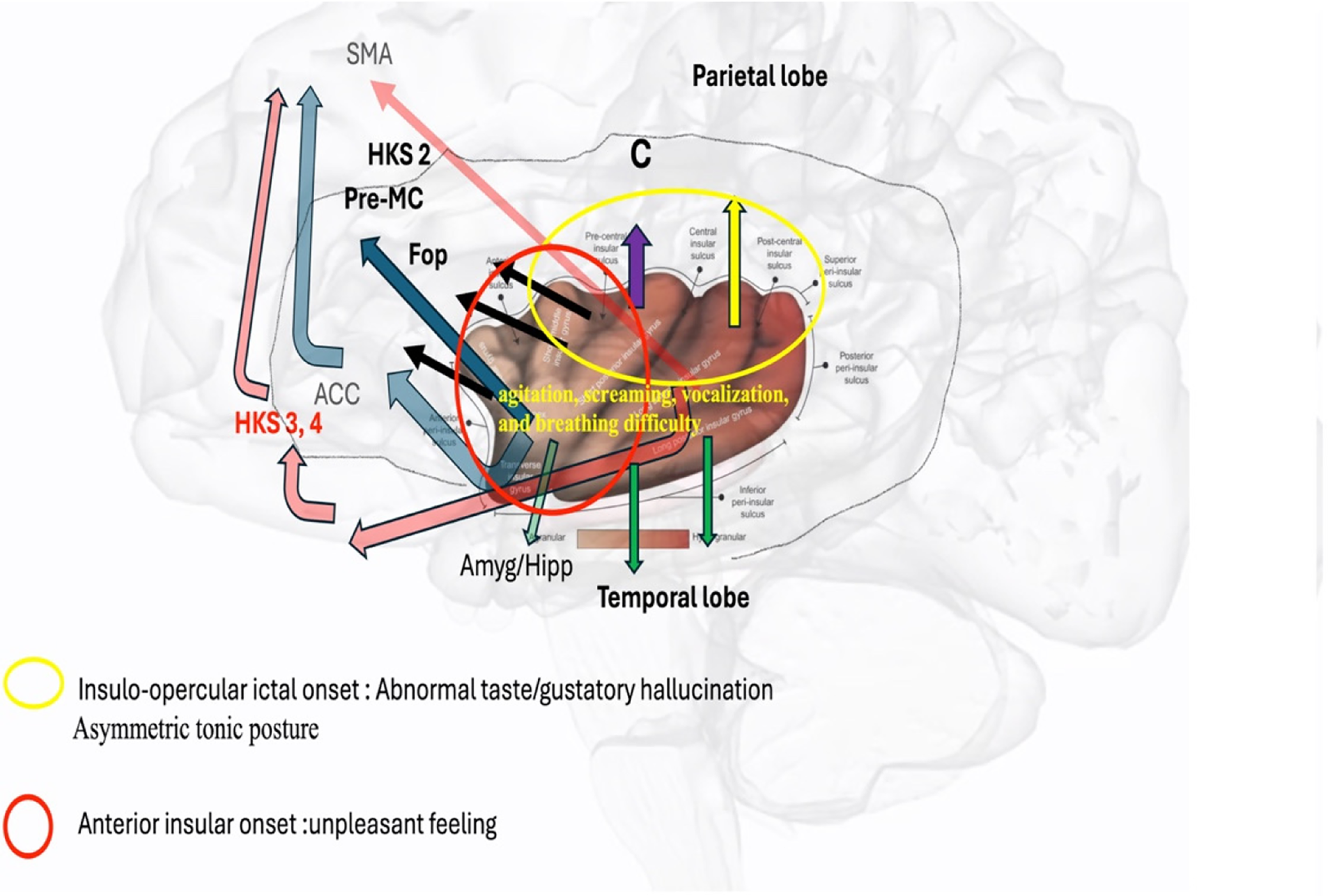
Ictal Semiology Association with Insular and Insulo-opercular Ictal Onset and Spreading Pathways.
No significant association was found between anterior versus posterior insular ictal onset and the type of hyperkinetic seizure. This may be due to the limited number of patients with pure insular onset in the cohort.
However, motor symptoms did help differentiate pure insular versus insulo-opercular ictal onset. Asymmetric tonic posturing was observed associated to seizures with insulo-opercular seizure onset zone (Table 7), consistent with findings from Hagiwara et al
51
Their SEEG analysis revealed:
The middle and posterior insula had strong functional coupling with the pre-SMA in patients with tonic posturing. The anterior short gyrus showed significant connectivity with anteromesial frontal regions in patients with hyperkinetic signs.
Other Motor Signs Associated with Hyperkinetic Seizures in the Study.
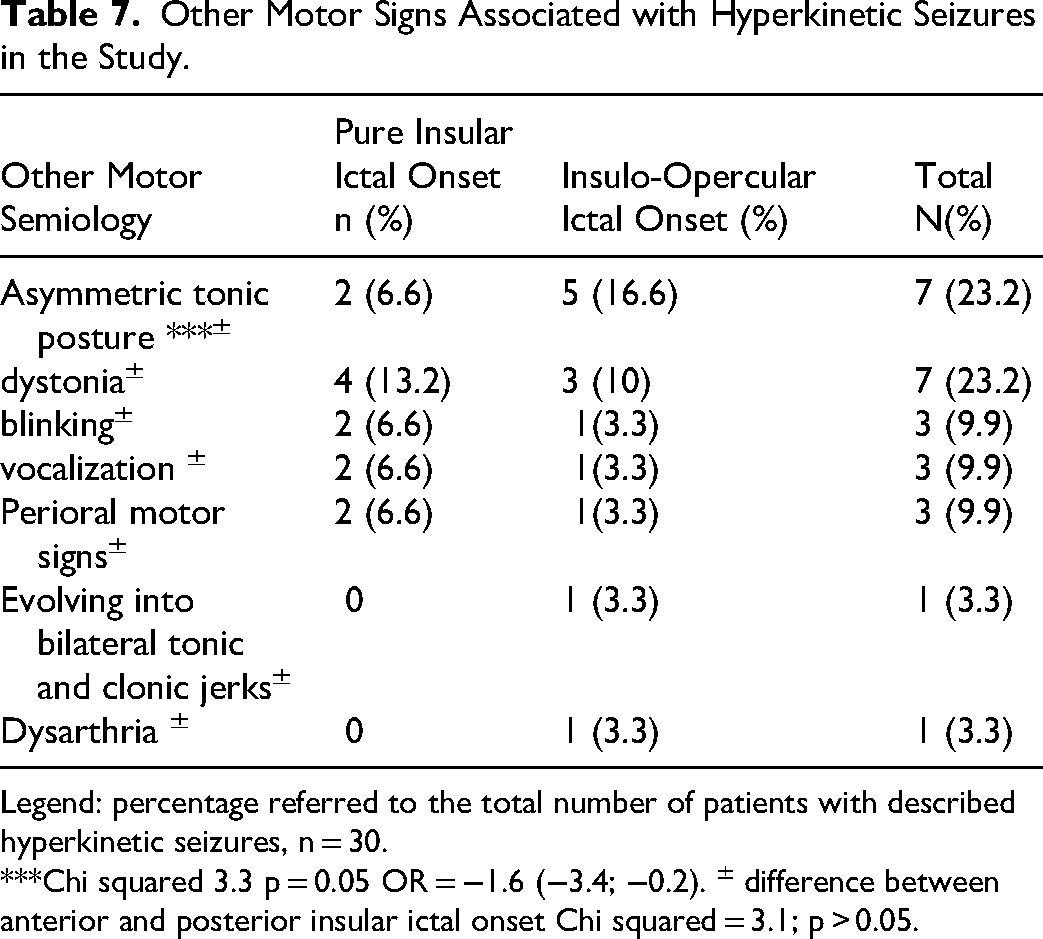
Legend: percentage referred to the total number of patients with described hyperkinetic seizures, n = 30.
***Chi squared 3.3 p = 0.05 OR = −1.6 (−3.4; −0.2). ± difference between anterior and posterior insular ictal onset Chi squared = 3.1; p > 0.05.
Functional MRI studies further support these findings:
When the seizure onset zone spans the central insular sulcus or extends to the suprasylvian operculum, the relationship between onset and motor pattern may become obscured. 54 In our cohort, we observed a mix of hyperkinetic and dystonic/tonic symptoms originating from the anterior bank of the central insular sulcus. In the paper published by Fayerstein J et al, the authors assessed seizures from 37 patients with HK, 2 of them with insular onset, and they did not find any correlation between the hyperkinetic scale and seizure onset in the insular cortex. 14 We excluded these two patients from the present review since their seizure characteristics were not described in the paper. The authors used a multicriteria scale (hyperkinetic seizure scale [HSS]) with 10 semiology features. In this study, dystonia, integrated behavior, and bilateral or unilateral hyperkinetic movements were statistically significant according to localization. Patients with seizures characterized by asymmetric hyperkinetic movements associated with marked dystonia and vocalization mainly included parietal seizures.
In contrast, bilateral and symmetrical stereotyped hyperkinetic movements without dystonia were represented by temporal seizures and one-third of prefrontal seizures (dorsolateral). Patients with intense emotionality and vocalization with bilateral and symmetrical hyperkinetic movements and integrated behavior have an ictal onset zone involving half of the temporal seizures and a majority of the prefrontal (ventromedial) seizures.55,56 These results are not comparable to ours because we use different scales and we only study insulo-opercular epilepsy.
Additional Motor, Vocal Emotional and Autonomic Features (see Figure 6)
Our findings (Table 7) confirm the frequent presence of ipsilateral eye blinking in insular seizures, 57 though its mechanism remains unclear56,58
Regarding agitation, screaming, vocalization, and breathing difficulty, patients with pure insular ictal onset were more likely to exhibit one or two of these symptoms. In contrast, patients with insulo-opercular seizure onset tended not to (p < 0.05, Figure 5b). These findings are supported by:
Jennifer Yip et al
59
found that affective sensations (eg, anxiety, chest tightness) were evoked during insular stimulation. Laure Mazzola et al41,60 reported viscero-sensitive symptoms—including throat constriction, dyspnea, and visceral anxiety—arising from stimulation of anterior insular regions.
These symptoms ranged from mild discomfort to panic-like anxiety, often associated with thoracic or abdominal constriction. This supports our observation of affective symptoms, breathing difficulty, and vocalization in patients with pure insular epilepsy.
Conclusion
This review suggests that hyperkinetic seizures in pure insular onset or insulo-opercular onset are associated with heterogeneous, semiological and anatomo-clinical patterns. The strength of these observations is limited by substantial interstudy heterogeneity, which constrains statistical power and limits generalizability. Nevertheless, the available data indicate that most patients with hyperkinetic seizures had a pure insular onset, predominantly involving the anterior insular cortex, with focal cortical dysplasia representing the most common etiology. Reported semiology included unnatural hyperkinetic behaviors, proximal or axial tonic or dystonic posturing, and more naturalistic automatisms such as kicking, rocking, pedaling, and manipulation or utilization behaviors, frequently without prominent early motor signs. Taken together, these findings raise the possibility that hyperkinetic manifestations reflect the engagement of distinct insulo-opercular-frontal connections. Patients with pure insular ictal onset also appeared more likely to present with HK3 behaviors, agitation, vocalization, and breathing difficulty, and less likely to demonstrate asymmetric tonic posturing than those with insulo-opercular onset. Given the exploratory nature of the evidence, however, these patterns should be interpreted cautiously and require confirmation in larger and methodologically more consistent studies.
Supplemental Material
sj-docx-1-eeg-10.1177_15500594261455108 - Supplemental material for Hyperkinetic Seizures in Insular and Insulo-Opercular Seizure Onset: A Systematic Review
Supplemental material, sj-docx-1-eeg-10.1177_15500594261455108 for Hyperkinetic Seizures in Insular and Insulo-Opercular Seizure Onset: A Systematic Review by Rene Andrade Machado, Natasha Acosta Diaz and Satyanarayana Gedela in Clinical EEG and Neuroscience
Supplemental Material
sj-docx-2-eeg-10.1177_15500594261455108 - Supplemental material for Hyperkinetic Seizures in Insular and Insulo-Opercular Seizure Onset: A Systematic Review
Supplemental material, sj-docx-2-eeg-10.1177_15500594261455108 for Hyperkinetic Seizures in Insular and Insulo-Opercular Seizure Onset: A Systematic Review by Rene Andrade Machado, Natasha Acosta Diaz and Satyanarayana Gedela in Clinical EEG and Neuroscience
Supplemental Material
sj-docx-3-eeg-10.1177_15500594261455108 - Supplemental material for Hyperkinetic Seizures in Insular and Insulo-Opercular Seizure Onset: A Systematic Review
Supplemental material, sj-docx-3-eeg-10.1177_15500594261455108 for Hyperkinetic Seizures in Insular and Insulo-Opercular Seizure Onset: A Systematic Review by Rene Andrade Machado, Natasha Acosta Diaz and Satyanarayana Gedela in Clinical EEG and Neuroscience
Supplemental Material
sj-docx-4-eeg-10.1177_15500594261455108 - Supplemental material for Hyperkinetic Seizures in Insular and Insulo-Opercular Seizure Onset: A Systematic Review
Supplemental material, sj-docx-4-eeg-10.1177_15500594261455108 for Hyperkinetic Seizures in Insular and Insulo-Opercular Seizure Onset: A Systematic Review by Rene Andrade Machado, Natasha Acosta Diaz and Satyanarayana Gedela in Clinical EEG and Neuroscience
Footnotes
Ethical Approval and Informed Consent Statements
N/A
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Available upon request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.