
Abstract
Brain activity can be assessed using electroencephalography (EEG) through measures such as power spectral density (PSD), functional connectivity, the brain symmetry index (BSI), and event-related brain responses. Transcranial direct current stimulation (tDCS) is an adjunctive intervention for post-stroke motor rehabilitation using different montages, including ipsilesional anodal, contralesional cathodal, and bilateral M1 stimulation. However, EEG-derived neurophysiological responses associated with motor recovery following tDCS have not been comprehensively reviewed. A PubMed search from 2000 to 2025 identified 12 studies investigating the effects of tDCS on oscillatory activity and 3 studies examining event-related brain responses. Five studies evaluated tDCS alone (without rehabilitation), whereas 10 investigated tDCS combined with rehabilitation. For tDCS alone, ipsilesional anodal stimulation (anode over the ipsilesional M1 and cathode over the contralateral supraorbital area) and bilateral M1 stimulation (anode over the ipsilesional M1 and cathode over the contralesional M1) showed similar trends toward enhancing high-frequency power and functional connectivity, whereas contralesional cathodal stimulation tended to reduce beta band connectivity. For tDCS combined with rehabilitation, PSD findings were inconsistent; however, BSI and event-related desynchronization (ERD) following ipsilesional anodal stimulation consistently showed increased high-frequency activity associated with motor improvement. ERD enhancements were also observed following bilateral M1 stimulation. Overall, heterogeneity in EEG analytical methods likely contributes to inconsistent findings. Nevertheless, current evidence suggests that ipsilesional anodal and bilateral M1 stimulation may upregulate high-frequency activity in individual with stroke. Future systematic studies integrating standardized EEG analyses with clinical outcomes across different tDCS montages are needed to establish EEG-based guidelines for post-stroke motor rehabilitation.
Keywords
Introduction
Brain activity reflects the physiological response of cortical neurons and can be evaluated using electroencephalography (EEG), which records the summed postsynaptic activity of cortical pyramidal neurons in the cerebral cortex during both unconscious and conscious stages, including rest, movement preparation, and movement execution. 1 EEG signals are typically classified into delta (1–3 Hz), theta (4–7 Hz), alpha (8–12 Hz), beta (12–30 Hz), and gamma (30–80 Hz). 2 EEG indices have been shown to reflect motor recovery after stroke from the acute to chronic phases.3,4 In the human cortex, modulation of high-frequency oscillations is involved in cortical activity during motor preparation.5,6 These oscillatory activities are altered following stroke onset. 2 Numerous studies have investigated stroke-related changes in cortical activity and their relationship with motor impairment using various EEG analytical approaches across different stages of recovery, highlighting the potential of EEG indices as biomarkers for monitoring motor rehabilitation outcomes. Following stroke, increased low-frequency oscillations (i.e., delta power) in both hemispheres have been reported in individuals with acute stroke. 7 In the early subacute phase, low-frequency activity persists, with its spatial distribution depending on lesion characteristics. 8 Increased low-frequency oscillations (i.e., delta band) and decreased high-frequency oscillations (i.e., alpha band) in the ipsilesional hemisphere have also been reported. 9 Additionally, lower delta power and higher alpha and beta power are generally observed in patients with better clinical recovery. 8 In individuals with chronic stroke, network reorganization tends to stabilized, often in a maladaptive manner. 10 This state is frequently characterized by persistent interhemispheric imbalance, whereby excessive inhibition from the contralesional hemisphere further suppresses the ipsilesional hemisphere, thereby limiting functional recovery.10,11 Spectral analyses have demonstrated reduction in high-frequency power and connectivity (particularly in the alpha and beta power) in the ipsilesional hemisphere of individuals with chronic stroke compared with healthy controls, and these changes are associated with poorer motor outcomes. 12 In contrast, increased ipsilesional beta power and beta power coherence within the ipsilesional hemisphere has been associated with better motor recovery.12–14 Moreover, an increased brain symmetry index (BSI), reflecting greater interhemispheric asymmetry, has been reported from the acute to chronic stages of stroke, and is correlated with severity and functional recovery.15–17 Furthermore, event-related brain responses are altered after stroke, with reduced alpha event-related desynchronization (alpha-ERD) observed in the ipsilesional hemisphere during movement preparation and execution of the affected limb.18,19
Over the past two decades, transcranial direct current stimulation (tDCS), a non-invasive brain stimulation (NIBS) technique, has been extensively investigated as an adjunctive intervention in stroke rehabilitation, demonstrating positive effects on motor recovery across multiple phases of stroke.20–23 tDCS modulates cortical excitability in a polarity-dependent manner within a limited dose range. Anodal stimulation increases cortical excitability by inducing depolarization of the resting membrane potential, whereas cathodal stimulation decreases excitability by inducing hyperpolarization.24–26 In healthy population, the after-effects of tDCS are thought to be mediated by a N-methyl-D-aspartate (NMDA) receptor-dependent synaptic plasticity. 27 In addition, modulation of brain-derived neurotrophic factor (BDNF) contributes to tDCS-induced neural plasticity.28,29 These effects are commonly associated with long-term potentiation (LTP)-, and long-term depression (LTD)-like plasticity.26,30 Another proposed mechanism underlying the after-effect of tDCS is the modulation of neurotransmitters in the human brain, particularly gamma-aminobutyric acid (GABA). Additionally, GABA plays an important role in synaptic plasticity and cortical activity, including the generation and modulation of brain oscillation in the human cortex.6,31 Recent studies in healthy population have reported conflicting results of tDCS on GABA level across different stimulation sites.32–37 While anodal stimulation over M1 consistently reduces GABA concentration in both healthy32–35,38 and elderly populations. 39 In contrast, no changes in GABA concentration are observed following either anodal or cathodal stimulation over the auditory cortex 36 or anodal stimulation over cerebellar cortex. 37 Whereas cathodal stimulation over M1 has been reported no change in GABA concentration over stimulated hemisphere, Bachtiar et al (2018) study demonstrated a reduction of GABA concentration over non-stimulated hemisphere.26,40,41 These discrepancies of the results may cause by differences of intensity or timing effects.26,40,41 Additionally, Nandi et al (2022) have been reported that reduction of GABA concentration at M1 region is correlated with higher amount of grey matter volumes. 32 These factors may underlie the inconsistent results of anodal and cathodal stimulation across studies. Collectively, these mechanisms may be reflected in tDCS-induced changes in EEG oscillations.
Common tDCS montages in stroke can be categorized as unilateral and bilateral approaches. The selection of electrode placement is guided by the ipsilesional hemisphere and the interhemispheric imbalance model. 42 In a unilateral montage, an active electrode (anode or cathode) is applied over a targeted area, such as the primary motor cortex (M1; e.g., C3/C4), while the reference electrode is placed over the contralateral supraorbital area (Fp1 or Fp2). 43 Anodal stimulation is typically applied over the ipsilesional hemisphere to enhance cortical excitability, whereas cathodal stimulation is applied over the contralesional hemisphere to reduce hyperexcitability and excessive inhibition exerted on the ipsilesional hemisphere. In bilateral montage, both electrodes are positioned over homologous cortical areas, with the anode over the ipsilesional hemisphere and the cathode over the contralesional hemisphere. This approach aims to rebalance interhemispheric inhibition (IHI). The most common target site of bilateral stimulation is the primary motor cortex of both hemispheres.
Numerous studies have employed both physiological and functional outcome measures to evaluate the therapeutic efficacy of tDCS during post-stroke recovery.20–23,44,45 More recently, EEG indices have increasingly been used as outcome measures to assess the effects of tDCS. However, no comprehensive review has systematically examined the effects of tDCS on EEG outcomes, particularly in relation to motor recovery in individuals with stroke. Therefore, this narrative review aims to summarize the current evidence regarding the effects of tDCS alone and in combination with motor rehabilitation on brain oscillations and motor performance in individuals with stroke.
Methods
Literature Search and Strategy
A targeted literature search was conducted using PubMed to identify studies published between 2000 and 2025 that investigated the effect of tDCS, with or without rehabilitation interventions, and reported EEG, event-related potentials (ERPs), and motor outcome measures. The search employed a combination of Medical Subject headings (MeSH) terms and keywords, including “stroke”, “transcranial direct current stimulation”, “tDCS”, “electroencephalography”, “EEG”, “brain oscillations”, “event-related potentials”, and “motor recovery”. To ensure a comprehensive narrative synthesis, the reference lists of identified articles and relevant reviews were manually screened to identify additional studies.
Study Selection and Inclusion Criteria
Studies were included if they met the following criteria: (1) involved adult with ischemic or hemorrhagic stroke; (2) utilized tDCS as a primary intervention (either using tDCS alone or in combination with motor rehabilitation); and (3) reported EEG indices as outcome measures alongside motor outcomes. The included EEG indices were as follows: (1) power spectral density (PSD), which quantifies changes in brain oscillations within specific frequency bands; (2) relative power, which represents the proportion of power within a given frequency band relative to the total EEG power across all frequencies; (3) functional connectivity, which characterizes brain network interactions; (4) BSI, which quantifies interhemispheric spectral asymmetry46,47; and (5) event-related brain responses, which provide complementary information on both phase-locked and non-phase-locked neural activity. Event-related brain responses included: i) ERPs, which represent stimulus- or phase-locked neural responses; ii) ERD and event-related synchronization (ERS), which reflect non-phase-locked modulation of spectral power within specific frequency bands associated with motor preparation, execution, or attentional processes. 1 Studies investigating non-motor outcomes (e.g., aphasia or neglect), targeting brain regions other than motor-related areas, or those using other forms of brain stimulation were excluded.
Data Synthesis and Analysis
The initial search yielded 148 publications. After screening, 12 studies investigating the effects of tDCS on EEG oscillations and 3 studies examining event-related brain responses in individuals with stroke were included. Among these, five studies targeted M1 evaluated the effects of tDCS alone (without rehabilitation) on EEG oscillations, whereas 10 studies (10 studies targeted M1 with 3 studies additionally targeted premotor cortex (PMC)) examined tDCS combined with rehabilitation interventions on EEG oscillations and event-related brain responses. Given the heterogeneity in tDCS parameters (e.g., intensity and duration) and the diversity of EEG analytical approached across studies, a formal meta-analysis was not feasible. Therefore, this narrative review synthesized the findings quantitatively according to the tDCS montage (e.g., ipsilesional anodal, contralesional cathodal, and bilateral M1 stimulation) used in each stroke recovery phase. Details of tDCS parameters, study designs, and EEG indices are summarized for studies examining tDCS alone (Table 1) and tDCS combined with rehabilitation interventions (Table 2).
Summarized tDCS Parameters and EEG Analytical Methods for tDCS Alone.
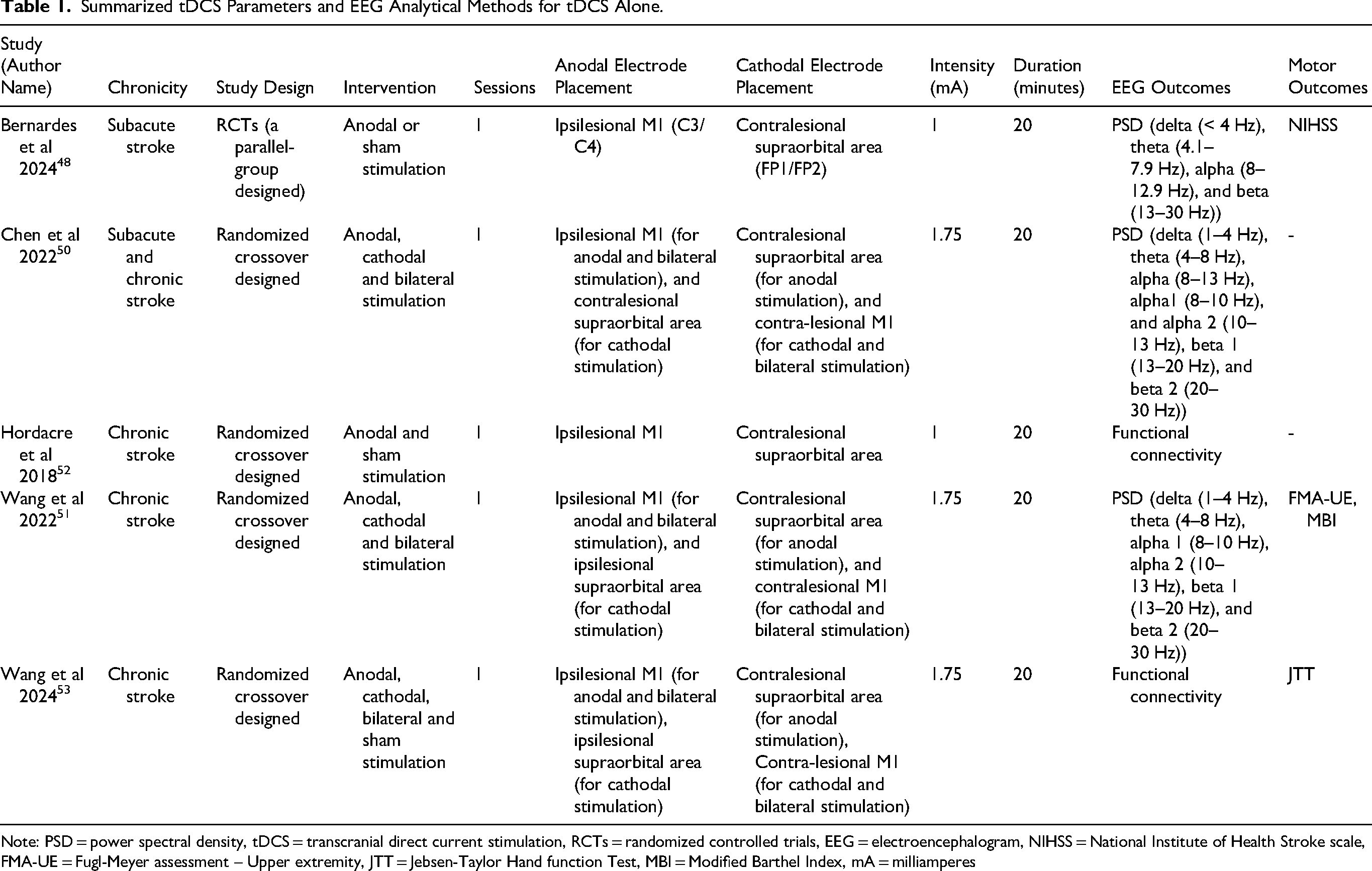
Note: PSD = power spectral density, tDCS = transcranial direct current stimulation, RCTs = randomized controlled trials, EEG = electroencephalogram, NIHSS = National Institute of Health Stroke scale, FMA-UE = Fugl-Meyer assessment – Upper extremity, JTT = Jebsen-Taylor Hand function Test, MBI = Modified Barthel Index, mA = milliamperes
Summarized tDCS Parameters and EEG Analytical Methods for tDCS with Rehabilitation.
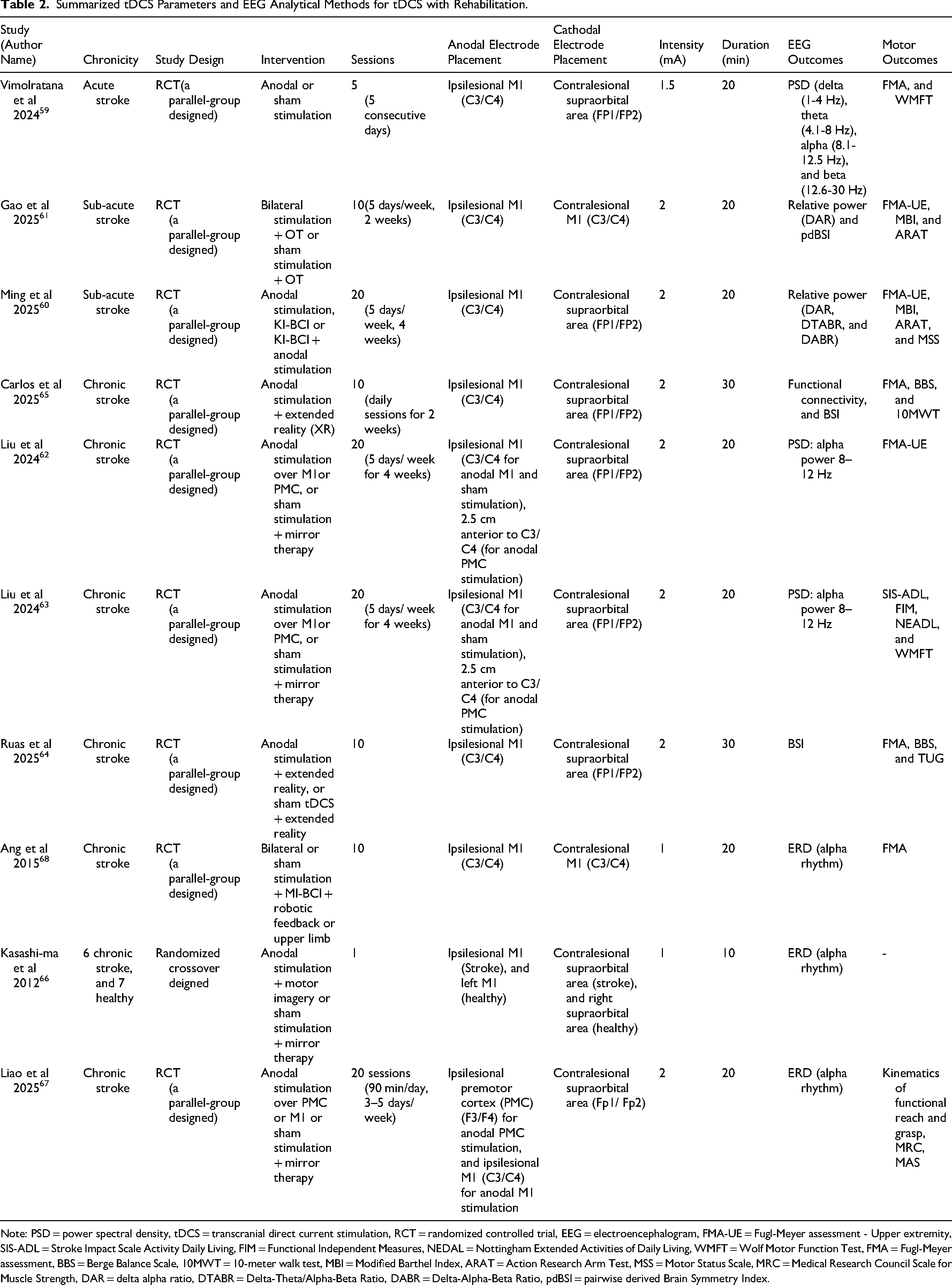
Note: PSD = power spectral density, tDCS = transcranial direct current stimulation, RCT = randomized controlled trial, EEG = electroencephalogram, FMA-UE = Fugl-Meyer assessment - Upper extremity, SIS-ADL = Stroke Impact Scale Activity Daily Living, FIM = Functional Independent Measures, NEDAL = Nottingham Extended Activities of Daily Living, WMFT = Wolf Motor Function Test, FMA = Fugl-Meyer assessment, BBS = Berge Balance Scale, 10MWT = 10-meter walk test, MBI = Modified Barthel Index, ARAT = Action Research Arm Test, MSS = Motor Status Scale, MRC = Medical Research Council Scale for Muscle Strength, DAR = delta alpha ratio, DTABR = Delta-Theta/Alpha-Beta Ratio, DABR = Delta-Alpha-Beta Ratio, pdBSI = pairwise derived Brain Symmetry Index.
Results
Changes in EEG Indices Following tDCS Alone in Stroke
At present, there is no evidence regarding the effects of tDCS alone in individuals with acute stroke. Only one study using ipsilesional anodal stimulation was identified in the subacute phase. A parallel-group randomized controlled trials (RCTs) by Bernardes et al (2024) reported increased alpha and beta power at P4 and reduced delta power at C3 following a single session of 1 mA anodal stimulation (25 cm2) over the ipsilesional M1, compared with sham stimulation. 48 The sham condition used an identical electrode montage, with current applied only for the first minute to mimic cutaneous sensation. 49
In the chronic phase, four randomized crossover studies have investigated the neurophysiological effects of unilateral anodal, unilateral cathodal and bilateral stimulation. Similar effects of ipsilesional anodal stimulation to those observed in the subacute phase have also been reported in individuals with chronic ischemic stroke. Chen et al (2022) and Wang et al (2022) reported increased alpha power over the ipsilesional hemisphere following a single session of 1.75 mA anodal stimulation (35 cm2) over the ipsilesional M1 for 20 min.50,51 Specifically, Chen et al (2022) observed increased alpha power (8–10 Hz) across prefrontal, frontal, central, and parietal areas of the ipsilesional hemisphere, along with increases in frontal and fronto-central areas of the contralesional hemisphere. Higher-frequency alpha power (10–13 Hz) also increased bilaterally in frontal and fronto-central areas. 50 When analyses were stratified by lesion side, Wang et al (2022) reported that in individuals with left-hemisphere lesions, alpha power (8–10 Hz) increased in frontal and fronto-central areas, along with increased beta power (13–30 Hz) in fronto-central and parietal areas. In contrast, in individuals with right-hemisphere lesions, only alpha power (10-13 Hz) increased in prefrontal, central, and parietal areas, with no significant changes in beta power. 51 These findings support the effects of ipsilesional anodal stimulation in enhancing both alpha and beta power in the ipsilesional hemisphere, with greater responsiveness observed in individuals with left-hemisphere lesions. 51 Functional connectivity analyses using partial least squares (PLS), which identify connectivity patterns between a seed electrode (e.g., C4) and other electrodes, further support the role of ipsilesional anodal stimulation in modulating high-frequency oscillations associated with motor recovery. Increased alpha power (8–13 Hz) in the temporal area of the ipsilesional hemisphere has been reported following a single session of 1 mA anodal stimulation (35 cm2) over the ipsilesional M1 for 20 min, and this change was associated with enhanced cortical excitability measured by single-pulse transcranial magnetic stimulation (TMS). 52 Furthermore, changes in beta-band functional connectivity were significantly associated with improvements in upper extremity function, as assessed by the Jebsen-Taylor Hand Function Test (JTT), following a single session of ipsilesional anodal stimulation. 53 For contralesional cathodal stimulation in chronic stroke, previous studies reported no significant changes in PSD following a single session of 1.75 mA cathodal stimulation (35 cm2) over the contralesional M1 (C3/C4) for 20 min.50,51 However, functional connectivity analyses demonstrated a reduction in beta-band connectivity over the contralesional frontal-central motor areas following cathodal stimulation, which was associated with improvements in upper extremity function. 53 For bilateral stimulation in chronic stroke, previous studies have demonstrated its potential to modulate high-frequency oscillations. Significant increases in alpha power within the ipsilesional hemispheres have been reported.50,51 Chen et al (2022) reported that a single session of 1.75 mA bilateral stimulation (35 cm2) over the M1 for 20 min increased alpha power (10–13 Hz) in fronto-central, central, and centro-parietal areas of the ipsilesional hemisphere, as well as in central and temporal areas of the contralesional hemisphere. In contrast, Wang et al (2022) observed alpha power enhancement limited to the ipsilesional hemisphere using a similar protocol. 51 These discrepancies may be attributed to differences in analytical approaches: Chen et al (2022) analyzed pooled data without stratifying by lesion side, whereas Wang et al (2022) compared individuals with right- versus left-hemisphere lesions. However, inconsistent findings were reported regarding beta-band functional connectivity and upper extremity function following bilateral stimulation. 53
Collectively, only a limited number of EEG indices have been reported in the context of tDCS alone in subacute and chronic stroke. To date, no studies have investigated event-related brain response (i.e., ERPs or ERD/ERS) following tDCS alone in these populations. Nevertheless, both PSD and functional connectivity appear to be useful for characterizing the effect of tDCS in the subacute and chronic phases.15,54 While PSD reflects overall oscillatory activity within specific frequency bands, functional connectivity captures inter- and intrahemispheric network dynamics and may be more sensitive to tDCS-induced neurophysiological changes.55,56 Ipsilesional anodal and bilateral stimulation highlight potential physiological mechanisms underlying tDCS-induced motor recovery, possibly mediated by enhanced intrahemispheric connectivity and increased high-frequency oscillatory activity within the ipsilesional hemisphere. Notably, the effects of ipsilesional anodal stimulation may extend to the contralesional hemisphere. 50 In addition, contralesional cathodal stimulation may facilitate motor recovery through reductions in beta-band connectivity in the contralesional hemisphere. This effect may be explained by the overactive contralesional hemisphere decreases inhibitory influence on the ipsilesional hemisphere, 57 thereby restoring interhemispheric balance. Furthermore, reducing contralesional cortical activity may help prevent maladaptive motor recovery in chronic stroke. 58
Changes in EEG Indices Following tDCS Combined with Rehabilitation in Stroke
Only one study using ipsilesional anodal stimulation was identified in the acute phase. In a parallel-group RCTs, Vimolratana et al (2024) reported increases in alpha and beta power in both hemispheres following 5 sessions of 1.5 mA anodal stimulation (25 cm2) over the ipsilesional M1 for 20 min, combined with conventional physical therapy in individuals with acute stroke. However, no significant between-group differences were observed between the anodal and sham stimulation groups. A significant correlation between increased beta power in the ipsilesional hemisphere and Fugl-Meyer Assessment (FMA) scores was observed in participants with mild motor impairment. 59 Currently, there is no evidence regarding other tDCS montages in individuals with acute stroke.
In the subacute phase, two parallel-group RCTs were identified employing ipsilesional anodal and bilateral stimulation over the M1. These studies reported inconsistent findings regarding relative power, although improvements in BSI were observed. Ming et al (2025) reported that 20 sessions of 2 mA anodal stimulation (25 cm2) over the ipsilesional M1 for 20 min significantly improved the delta–alpha–beta ratio (DABR). However, no significant differences in DABR were observed among kinesthetic motor imagery-based brain computer interface (KI-BCI) alone, ipsilesional anodal stimulation alone, and the combined intervention. Nevertheless, both the KI-BCI alone group and the combined group demonstrated significant improvements in upper extremity function, as assessed by Fugl-Mayer Assessment – upper extremity (FMA-UE), whereas ipsilesional anodal stimulation alone did not. 60 In contrast, Gao et al (2025) reported parallel improvements in EEG indices and motor performance following 10 sessions of 2 mA bilateral stimulation (25 cm2) over the M1 for 20 min combined with occupational therapy. Improvements were observed in delta-alpha ratio (DAR), BSI, and FMA-UE scores compared with the occupational therapy alone group. 61 These discrepant findings may be attributed to difference in electrode montage, rehabilitation modalities, and intervention protocols. Ming et al (2025) also noted potential limitations related to upper-limb ergometer training, including reliance on EEG-driven activation and a limited number of EEG channels, which may restrict precise localization and interpretation of brain activity. 60 Currently, there is no evidence regarding cathodal stimulation on brain oscillatory activity in subacute stroke.
In the chronic phase, most included studies employed ipsilesional anodal stimulation, while only one study used bilateral stimulation. The majority of study adopted a parallel-group RCTs design, with the exception of Kasashima et al (2012), who used a randomized crossover design. For ipsilesional anodal stimulation, inconsistent findings were reported for both high-frequency power and motor outcomes. Liu et al (2024) reported significant increases in alpha power following 20 sessions of 2 mA anodal stimulation applied over the ipsilesional premotor cortex (PMC; approximately 2.5 cm anterior to M1 at C3/C4) using small electrodes (3.14 cm2) for 20 min. No significant between-group differences were observed among anodal stimulation over the ipsilesional M1, ipsilesional PMC, and sham stimulation, with all groups receiving mirror therapy. However, improvements in FMA scores were observed across all groups, with the PMC stimulation group demonstrating sustained improvements up to three months post-intervention. Notably, only changes in the PMC stimulation group were correlated with FMA improvements, and regression analysis suggested that alpha power may predict motor recovery. 62 Similar findings were reported in a study using larger electrodes. Liu et al (2024) demonstrated improvement in activities of daily living (ADLs) accompanied by increased alpha power following 20 sessions of 2 mA anodal stimulation (35 cm2) over the ipsilesional PMC for 20 min. 63 Regarding BSI, improvements in alpha and gamma symmetry, motor function, and balance have been reported following 10 sessions of 2 mA ipsilesional anodal stimulation (35 cm2) for 30 min combined with extended reality interventions. 64 Similarly, Carlos et al (2025) reported improvements in beta and gamma symmetry following comparable stimulation parameters. Improvements in FMA, Berg Balance Scale and 10-meter walked test (10 MWT) were correlated with improvements in high-frequency power, brain symmetry and network connectivity using lagged coherence in each frequency bands. 65 For event-related brain response, two studies reported consistent increases in alpha-ERD in the ipsilesional hemisphere following ipsilesional anodal stimulation combined with training. A single session of 1 mA anodal stimulation (35 cm2) over the ipsilesional M1 for 10 min combined with motor imagery increased alpha-ERD. 66 Similar findings were observed following 20 sessions of 2 mA anodal stimulation (3.14 cm2) over the ipsilesional M1 and PMC for 20 min combined with mirror therapy. 67 These findings suggest that ipsilesional anodal stimulation may enhance cortical activation during movement execution. For bilateral stimulation, Ang et al (2015) reported comparable improvements in alpha-ERD following 10 sessions of 1 mA bilateral stimulation (35 cm2) over the M1 for 20 min combined with MI-BCI or motor imagery alone. However, motor performance, as evaluated by FMA, did not differ between the bilateral and sham stimulation groups. 68
Overall, evidence regarding EEG outcomes following tDCS combined with rehabilitation remains limited. In the acute phase, only one study is available, suggesting that the addition of ipsilesional anodal stimulation to conventional rehabilitation may modulate cortical activity. No evidence is currently available regarding other tDCS montages combined with rehabilitation in acute stroke. In the subacute stroke, findings on relative power remains inconsistent across studies, likely reflecting differences in electrode montage and rehabilitation protocols. In contrast, in chronic stroke, ipsilesional anodal stimulation demonstrates more consistent improvements in BSI and ERD, with positive associations with motor recovery. Improvement in high-frequency oscillations have also been observed; however, their relationship with motor recovery remains inconclusive. Furthermore, bilateral stimulation has been reported to improve ERD, with effects on motor recovery comparable to ipsilesional anodal stimulation.
Conclusions
Existing evidence suggests that tDCS has the potential to modulate EEG oscillatory activity in individuals with stroke in a montage-, phase-, and analysis-dependent manner. When applied tDCS alone in the subacute and chronic phases, different tDCS montages induce distinct patterns of changes across EEG indices. Both ipsilesional anodal and bilateral stimulation show similar trends toward enhancing high-frequency oscillations and intrahemispheric connectivity within the ipsilesional hemisphere, with effects that may extend to the contralesional hemisphere. Contralesional cathodal stimulation may additionally support motor recovery through modulation of beta-band connectivity in the contralesional hemisphere.
For tDCS combined with rehabilitation, evidence is available across all stroke phases but is predominantly limited to ipsilesional anodal stimulation, with only a few studies investigating bilateral stimulation in the subacute and chronic phases. Although PSD is the most frequently used EEG measure, findings remain inconsistent across studies. In contrast, studies using BSI and ERD have demonstrated more consistent results, generally indicating that ipsilesional anodal stimulation enhances high-frequency activity associated with improvements in motor outcomes. Similar ERD enhancements have also been observed following bilateral stimulation. However, the use of diverse analytical methods contributes to heterogeneity in findings across studies. Based on current evidence, both ipsilesional anodal and bilateral stimulation, with or without rehabilitation, appear to upregulate high-frequency activity, which is typically reduced after stroke. Nevertheless, the limited evidence makes it difficult to determine the most appropriate EEG indices for characterizing neurophysiological changes following tDCS. Therefore, the development of EEG-based guidelines integrating standardized analytical approaches with clinical outcomes is essential to advance both research and clinical practice in stroke rehabilitation. Further systematic investigations examining the effects of different tDCS montages, with or without rehabilitation, on both EEG measures and clinical outcomes are highly recommended.
Footnotes
Acknowledgements
We thank the authors of the included studies. We also would like to extend our gratitude to Assoc.Prof.DrVorasith Siripornpanich for his advice.
Ethical Approval and Informed Consent Statements
Ethical approval was noted for all published papers included in the review. No further ethics approval was sought for this review for existing literature.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data will be made available on request. The request should be directed to the corresponding author.