
Abstract
Purpose
This study aimed to systematically assess ictal scalp electroencephalography (EEG) evolution by examining both ictal onset characteristics and late significant patterns (LSPs) in adults with focal epilepsy. We aimed to investigate their individual and collective descriptive roles in seizure lateralization and localization, as well as their correlation with seizure semiology, interictal EEG findings, and structural magnetic resonance imaging (MRI) within a multimodal presurgical assessment framework.
Methods
We retrospectively analyzed 67 adults with drug-resistant focal epilepsy who underwent extended video-EEG monitoring, during which 242 seizures were documented. The ictal EEG findings were categorized based on the morphology of the onset and subsequent rhythmic patterns. The yields of lateralization and localization were evaluated independently for ictal onset patterns, LSPs, and combined ictal interpretations. Cohen's κ statistics were used to look at multimodal concordance between ictal EEG, seizure semiology, interictal EEG, and MRI findings.
Results
The most common types of ictal onset were non-rhythmic or unclassifiable activity (29.3%) and low-voltage fast activity (28.5%). Late significant patterns were detected in 36.8% of seizures, predominantly manifesting as rhythmic theta–alpha activity, followed by repetitive spikes or sharp waves. The integration of LSPs resulted in enhanced lateralization and localization yields, in contrast to the analysis of onset patterns in isolation. At the individual patient level, combined ictal interpretation lateralized seizures in 68.6% of cases and localized seizure-onset regions in 70.1% of cases. There was a high degree of agreement between ictal and interictal EEG (κ = 0.775, strict right-left), a high degree of agreement between ictal EEG and MRI (κ = 0.710), and moderate-to-high agreement between ictal EEG and seizure semiology (κ = 0.647).
Conclusion
A systematic evaluation of ictal EEG evolution, including the identification of LSPs, provides additional descriptive data that augments conventional ictal-onset analysis in focal epilepsy. The integration of ictal evolution findings with semiology, interictal EEG, and MRI validates a multimodal interpretative framework for presurgical evaluation. These results highlight the possible clinical importance of incorporating seizure evolution analysis into conventional scalp EEG interpretation, although further validation with surgical outcome data is required.
Keywords
Introduction
Epilepsy is one of the most common neurological disorders worldwide and a major cause of neurological disability and economic burden. 1 Focal epilepsy constitutes the principal subgroup in adult populations; notwithstanding considerable therapeutic progress, approximately one-third of patients continue to experience drug-resistant seizures. Epilepsy surgery is the best long-term option for some individuals to be free of seizures and have an improved quality of life. 2
To effectively treat epilepsy surgically, it is essential to precisely identify the epileptogenic zone, the specific region of the brain responsible for seizures. A comprehensive presurgical assessment is required to precisely delineate this zone. This typically encompasses long-term video electroencephalography (vEEG), high-resolution magnetic resonance imaging (MRI), neuropsychological assessment, and, when necessary, functional imaging modalities or invasive intracranial electroencephalography (EEG) monitoring to enhance localization precision.
Among these diagnostic modalities, prolonged vEEG monitoring is essential for presurgical assessment, as it enables the simultaneous evaluation of ictal electrophysiological activity and seizure semiology. 3 Ictal scalp EEG patterns vary widely according to seizure type and underlying pathology. Early ictal onset may manifest as attenuation or low-voltage fast activity (LVFA), rhythmic discharges, repetitive spikes, electrodecremental responses, or nonspecific/unclassifiable activity. In addition to onset characteristics, late significant patterns (LSPs)—reproducible rhythmic or focal discharges emerging seconds after seizure onset—may provide additional lateralizing and localizing value.
Previous studies have explored the localizing value of ictal scalp EEG patterns, particularly in temporal lobe epilepsy where rhythmic 5–9 Hz theta activity at or near onset is well established as a marker of mesial temporal pathology.4-6 Outside the temporal lobe, the ictal scalp EEG repertoire is broader and frequently less specific, with non-rhythmic or low-voltage fast onsets that propagate rapidly and complicate visual interpretation.7,8 Comparatively few studies have examined the post-onset evolution of ictal EEG in a structured way, and even fewer have evaluated whether the addition of late significant patterns improves lateralization beyond onset analysis alone, particularly in extratemporal cases or in cohorts with mixed pathologies.9,10 The clinical implications of such an extension are potentially relevant: in centers with limited or delayed access to invasive monitoring, maximizing the noninvasive yield of scalp EEG can refine the working presurgical hypothesis and rationalize the indication for stereo-EEG.
On this background, the present study was designed to systematically analyse ictal onset and LSP features in adults with focal epilepsy and to assess their individual and combined contributions to scalp EEG localization and lateralization. By integrating these electrophysiological findings with seizure semiology and MRI data, we sought to evaluate multimodal concordance and explore whether ictal EEG evolution within the first 30 s could provide additional descriptive value during the presurgical evaluation.
We hypothesized that
Incorporating LSPs alongside ictal onset patterns enhances localization and lateralization concordance compared with onset analysis alone. A high concordance between scalp EEG (onset + LSP) and MRI/semiology identifies patients with well-defined epileptogenic zones, who may be potential candidates in whom invasive EEG could be avoided in carefully selected cases. Non-lateralized or discordant scalp EEG patterns indicate cases that are likely to require invasive evaluation.
Methods
Study Design and Participants
This retrospective study included adult patients (>15 years) with a diagnosis of focal epilepsy who were monitored at a tertiary epilepsy outpatient clinic. vEEG recordings were obtained over an 18-month period at the Sleep Disorders and Epilepsy Monitoring Unit, where patients underwent monitoring for diagnostic purposes, follow-up, or presurgical evaluation.
Patients were included if at least one ictal event was captured during vEEG monitoring.
Exclusion criteria were findings consistent with primary generalized epilepsy, non-epileptic events, a history of neurodegenerative disease, alcohol or drug abuse, and seizures occurring outside the camera field.
Ethics
The study was approved by the Dokuz Eylul University Non-Interventional Research Ethics Committee (approval number: 2016/14-32, file no: 926-GOA; date: 26 May 2016). Given the retrospective nature of the study, the requirement for informed consent was waived. All procedures were conducted in accordance with the Declaration of Helsinki.
Video-EEG Monitoring and Analysis
Video-electroencephalography monitoring was performed using the Grass-Telefactor digital system over 3–5 consecutive days, with continuous synchronized video recordings obtained using a dual-camera setup. Scalp EEG was recorded using a standard 21-channel configuration in accordance with the international 10–20 system (including Fpz and Oz). Both referential (linked ears) and bipolar longitudinal montages were systematically reviewed for ictal and interictal analyses. Additional polygraphic channels, such as electro-oculography (EOG), submental electromyography (EMG), and electrocardiography (ECG), were included to assist in distinguishing artifacts and accurately characterizing seizure-related physiological changes. All recorded seizures were independently evaluated by two experienced neurophysiologists (ND and BB). During EEG pattern classification, the readers were aware that the recordings belonged to patients with focal epilepsy under presurgical evaluation but remained blinded to detailed clinical, semiological, and neuroimaging information, including lesion localization and seizure subtype. Each seizure was classified according to predefined operational EEG criteria. Multimodal concordance with semiology, interictal EEG, and MRI was assessed only after all ictal classifications were locked. Discrepancies between readers were resolved through consensus review.
Definition of Ictal EEG Patterns
Ictal Onset Patterns (IOPs)
Ictal onset was defined as the first sustained (≥3 s) electrographic change distinct from the background, occurring no later than 10 s after the electroclinical seizure onset. Morphological classification was performed using only the first 3 s of this sustained activity, in line with previously published scalp EEG methodologies.11,12 The 10-s window referred to the maximum allowable interval between the behavioral onset on video and the first sustained scalp EEG correlate, not the duration over which morphology was judged. A wider window for the clinico-electrographic interval was chosen because a substantial proportion of focal seizures, particularly those of mesial or extratemporal origin, show a brief delay between behavioral onset and a recognizable scalp EEG correlate; restricting that interval to 3 s would have systematically excluded such seizures and biased the cohort towards events with synchronous clinico-electrographic onset.
Ictal onset morphologies were classified into seven categories:
attenuation or low-voltage fast activity (LVFA); repetitive spikes or rhythmic sharp waves; rhythmic delta activity; rhythmic theta/alpha activity; rhythmic beta activity; non-rhythmic/unclassified activity; and artifact-dominated onset.
Representative examples of the principal morphological onset patterns used for classification are shown in Figure 1(A–F) to illustrate the operational definitions applied during the visual EEG analysis. Artifact-dominated onsets, although defined as a separate category, were not illustrated because these events were excluded from the localization and lateralization analyses.

Representative scalp ictal EEG onset patterns observed in adults with focal epilepsy. (A) Attenuation or low-voltage fast activity (LVFA); (B) repetitive spikes or rhythmic sharp waves; (C) rhythmic delta activity; (D) rhythmic theta/alpha activity; (E) rhythmic beta activity; (F) non-rhythmic / unclassified activity. All traces are displayed in a bipolar longitudinal (double-banana) montage with concurrent polygraphic channels. Recording parameters: sweep speed 30 mm/s (10 s per page), sensitivity 7 µV/mm, low-frequency filter 1 Hz, high-frequency filter 70 Hz, notch filter 50 Hz. The L-shaped calibration bar in the lower-right corner of each panel indicates 100 µV (vertical) and 1 s (horizontal). The ellipses indicate the regions of interest discussed in the text.
Late Significant Patterns (LSPs)
Late significant patterns were defined as reproducible localizing or lateralizing discharges emerging within 30 s (after the first 10 s) of seizure onset and lasting >10 s.Patterns appearing later than 30 s or dominated by propagation-related activity were excluded. Interpretation of LSPs was performed considering their temporal evolution and spatial concordance with early ictal EEG changes.
Lateralization and Localization Criteria
Ictal discharges were categorized according to their spatial distribution, based on both referential and bipolar montages, into five groups consistent with the study protocol and prior scalp EEG literature:
Regional: onset confined to a single lobe or contiguous lobar regions. Hemispheric: involvement of multiple areas within one hemisphere. Bilateral with dominant side: asynchronous or amplitude-asymmetric discharges affecting both hemispheres but with clear lateral predominance. Bilateral non-lateralized: synchronous, symmetrical discharges involving both hemispheres simultaneously. Non-localizable: diffuse or artifact-obscured activity precludes localization.
In this study, localization was defined as regional localization. Only seizures classified as regional were considered localized. Hemispheric and bilateral patterns were regarded as lateralizing but not localizing, whereas non-localizable patterns were excluded from the localization analyses. This definition was adopted to ensure stricter spatial specificity in the localization analyses.
An amplitude ratio >2:1 between hemispheres (referential montage) was accepted as lateralization, and a frequency difference ≥1 Hz was defined as bilateral asynchrony.
Each seizure was documented with respect to its onset morphology, LSP characteristics, lateralization, and localization.
Clinical Semiology
Video recordings were analyzed concurrently with EEG data, and seizure types were classified according to the ILAE 2017 operational criteria as
13
:
Focal aware seizures (FAS) Focal impaired awareness seizures (FIAS), Focal to bilateral tonic–clonic seizures (FBTCS)
Lateralizing signs (version, dystonic posturing, automatisms, speech arrest, etc) were systematically recorded. Semiological localization hypotheses were assigned according to the ILAE 2017 operational seizure classification and established presurgical semiology principles.13,14
Magnetic Resonance Imaging Evaluation
All patients underwent cranial MRI on a 1.5 Tesla scanner using standard epilepsy protocols (T1-weighted, T2-weighted, and FLAIR), and the imaging findings were reviewed by the epilepsy team as part of the routine presurgical assessment. MRI findings were categorized as follows:
Mesial temporal sclerosis (MTS): hippocampal atrophy and T2/FLAIR hyperintensity. Other epilepsy-related structural lesions: cortical dysplasia, post-encephalitic or post-traumatic gliosis, vascular malformations, cortical/subcortical atrophy, hippocampal asymmetry, arachnoid cysts, and developmental venous anomalies, which are considered potentially epileptogenic. Normal MRI: no epileptogenic lesion or findings deemed unrelated to epilepsy, such as nonspecific gliotic changes, chronic ischemic foci, or diffuse mild cortical atrophy.
For statistical analysis, patients were grouped into the MTS, other epilepsy-related lesion, and normal MRI categories.
This comparison evaluated the concordance between scalp vEEG findings and structural imaging during the presurgical assessment.
Statistical Analysis
All data were analyzed using SPSS version 15.0 (SPSS Inc., Chicago, IL, USA).
Continuous variables were reported as mean ± SD or median (IQR) according to distribution. Normality of distribution was assessed using standard normality tests. Categorical variables were presented as n.
Comparisons between groups were performed using the χ2 or Fisher's exact test for categorical data and the independent-samples t-test or Mann–Whitney U test for continuous data, as appropriate.
Localization/lateralization yields were compared between onset-only and onset + LSP analyses using McNemar's test for paired proportions at the seizure level.Agreement between ictal EEG, semiology, and MRI was assessed using Cohen's κ (κ < 0.20 poor; 0.21-0.40 fair; 0.41-0.60 moderate; 0.61-0.80 substantial; > 0.80 almost perfect). Multimodal concordance analyses (κ statistics with semiology, interictal EEG and MRI) were computed using the combined ictal interpretation (onset + LSP) at the patient level, since this represents the working clinical product of complete ictal review. A p value < 0.05 was considered statistically significant.
Results
Patient Characteristics and Seizure Distribution
A total of 67 patients with focal epilepsy were evaluated, contributing to 242 seizures captured during long-term video EEG monitoring (median: 3 seizures/patient, range: 1-9). Among the documented seizures, 143 (59.1%) occurred during wakefulness, and 99 (40.9%) occurred during sleep. At the individual patient level, 32 (47.8%) experienced seizures solely during wakefulness, 21 (31.3%) exclusively during sleep, and 14 (20.9%) had seizures in both states.
Ictal Scalp EEG Findings
Ictal Onset Patterns (IOPs)
The predominant IOP observed was non-rhythmic/unclassifiable activity in 71 seizures (29.3%) and attenuation/low-voltage fast activity in 69 seizures (28.5%). In 14.9% of the seizures, artifacts rendered the onset pattern indeterminable. Repetitive spikes/sharp waves, rhythmic delta activity, and rhythmic beta activity were the least prevalent onset patterns, occurring in 5.4%, 2.1%, and 2.1% of the seizures, respectively (Figure 2).
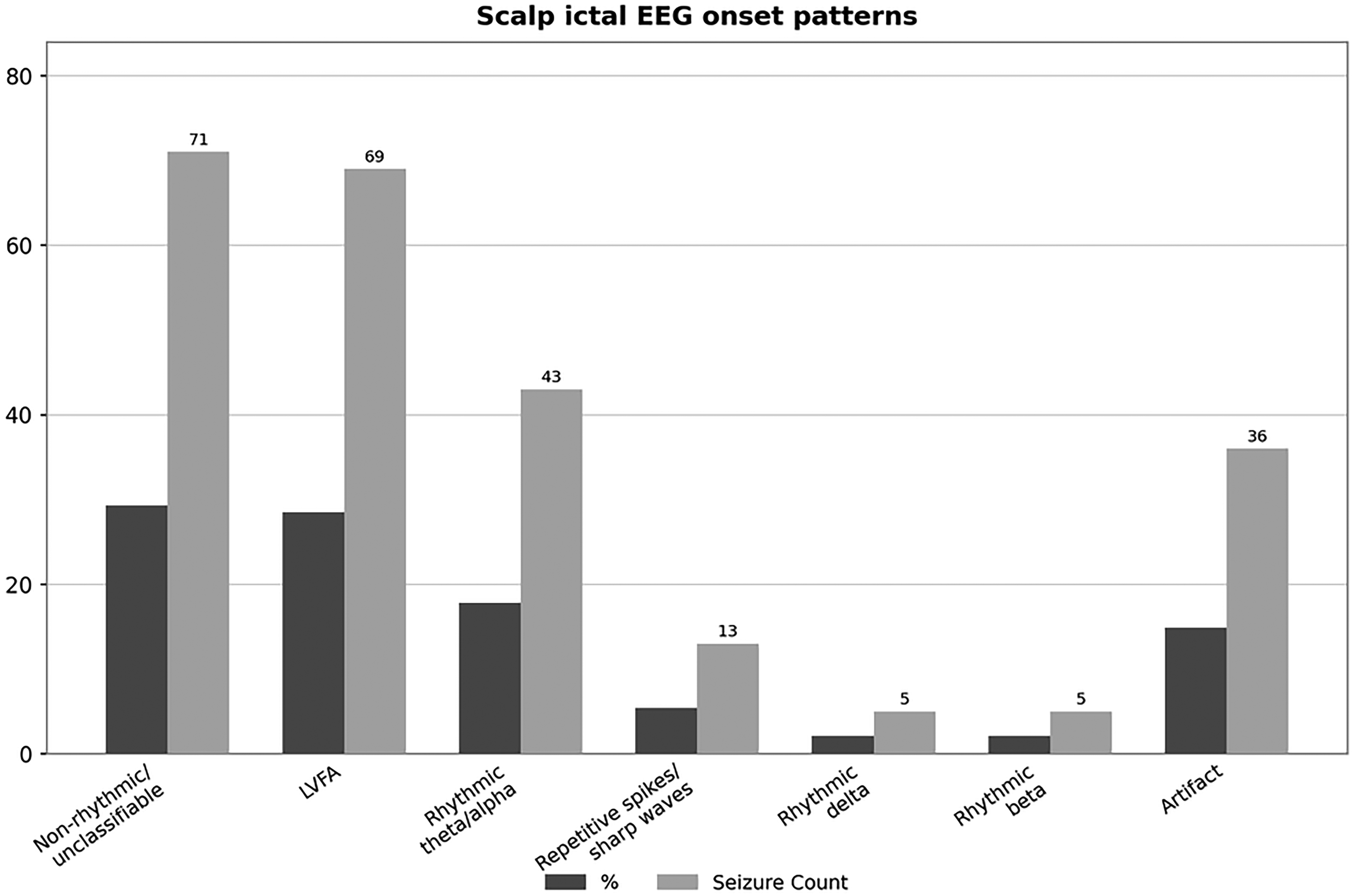
Distribution of scalp ictal EEG onset patterns in 242 seizures. LVFA, low-voltage fast activity.
Among seizures with identifiable IOPs, attenuation/LVFA was more frequently associated with temporal lobe seizures, whereas non-rhythmic/unclassifiable activity was predominantly observed in frontal lobe seizures. Repetitive spikes or sharp waves were also more common in frontal lobe lesions; however, this onset pattern constituted a small proportion of all recorded seizures.
Based solely on the onset characteristics, hemispheric lateralization was achieved in 61 seizures (25.2%), with 44 (72.1%) originating in the right hemisphere and 17 (27.9%) in the left hemisphere. Localization to a candidate lobe was feasible in 64 seizures (26.4% of all seizures). At the patient level, IOPs facilitated the lateralization of the epileptogenic hemisphere in 21 (31.3%) patients and localization of the onset zone in 23 (34.3%) patients.
Late Significant Patterns (LSPs)
A late significant pattern was identified in 89 seizures, which emerged after a mean latency of 12.8 ± 6.5 s. Rhythmic theta–alpha activity was the most prevalent LSP subtype, observed in 61 seizures (68.5%). Repetitive spikes or rhythmic sharp waves constituted the second most common pattern, occurring in 20 seizures (22.5%), followed by rhythmic delta activity in seven seizures (7.9%). Artifacts precluded late-pattern analysis in only one seizure (1.1%). When present, LSPs enabled hemispheric lateralization in 79 seizures (78.4%) and localization in 69 seizures (77.5%). At the patient level, LSPs facilitated lateralization of the epileptogenic hemisphere in 30 (44.8%) and localization of the onset zone in 31 (46.3%) patients.
Combined Analysis of Ictal Patterns
The integration of IOPs with LSPs yielded higher localization and lateralization yields than IOPs alone. At the seizure level, 130 (53.7%) seizures were successfully lateralized, and 133 (54.9%) were localized (Figure 3). At the patient level, combined ictal analysis facilitated the lateralization of the epileptogenic hemisphere in 46 (68.6%) and the localization of the onset region in 47 (70.1%) patients, demonstrating the strongest yield among all scalp EEG parameters (Figure 4). The discrepancy between seizure- and patient-level yields reflects the within-patient heterogeneity of seizure onsets: many patients contributed multiple seizures with variable electrographic features, and a single confidently lateralizedevent was sufficient to assign hemispheric concordance at the patient level, even when other seizures from the same patient were non-lateralized or artifact-dominated. This is a recognized property of scalp EEG cohorts and underscores the value of capturing multiple seizures during prolonged monitoring.
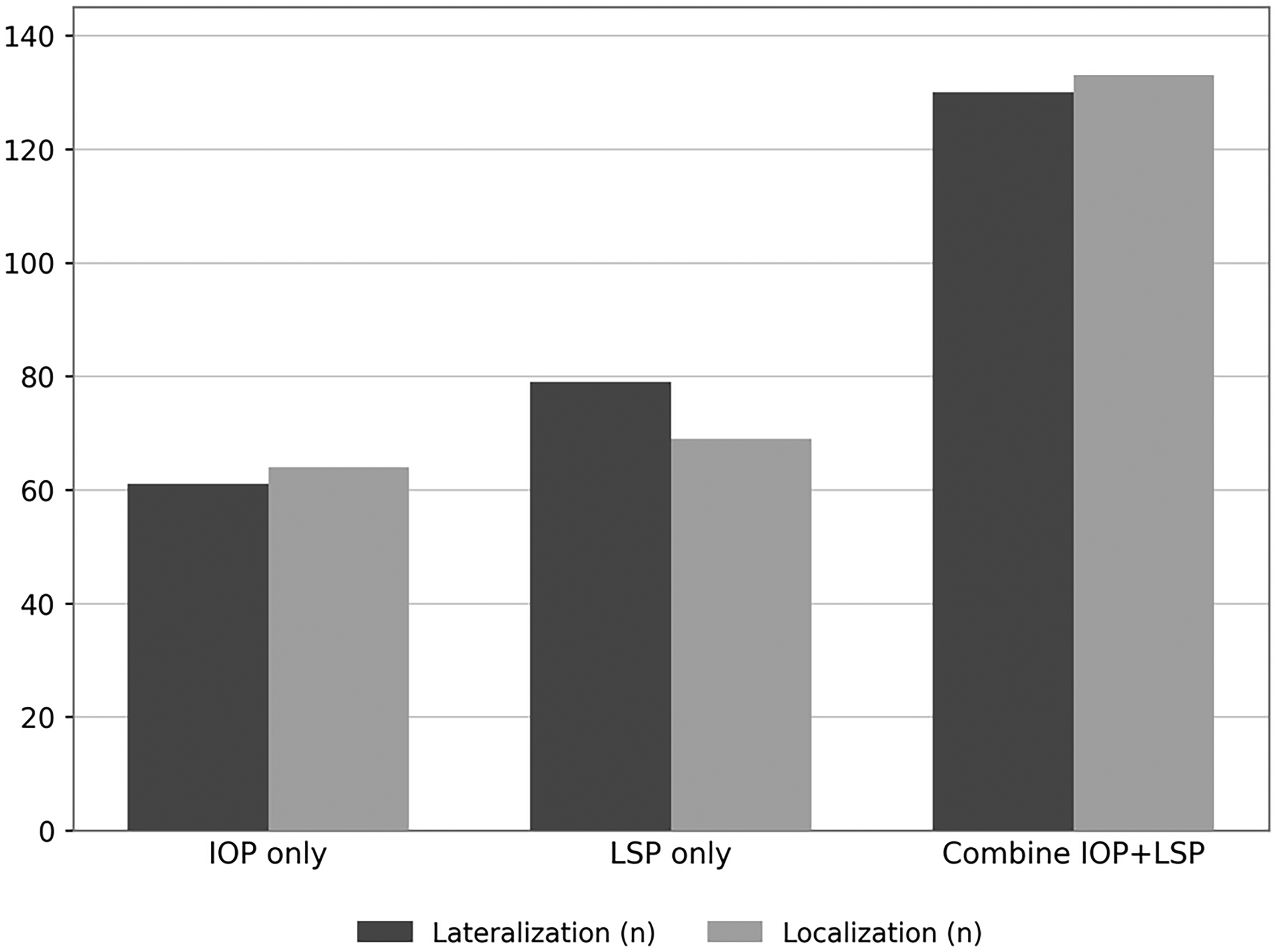
Comparative yield of ictal onset patterns, late significant patterns and combined analysis at the seizure level. IOP, ictal onset pattern; LSP, late significant pattern.
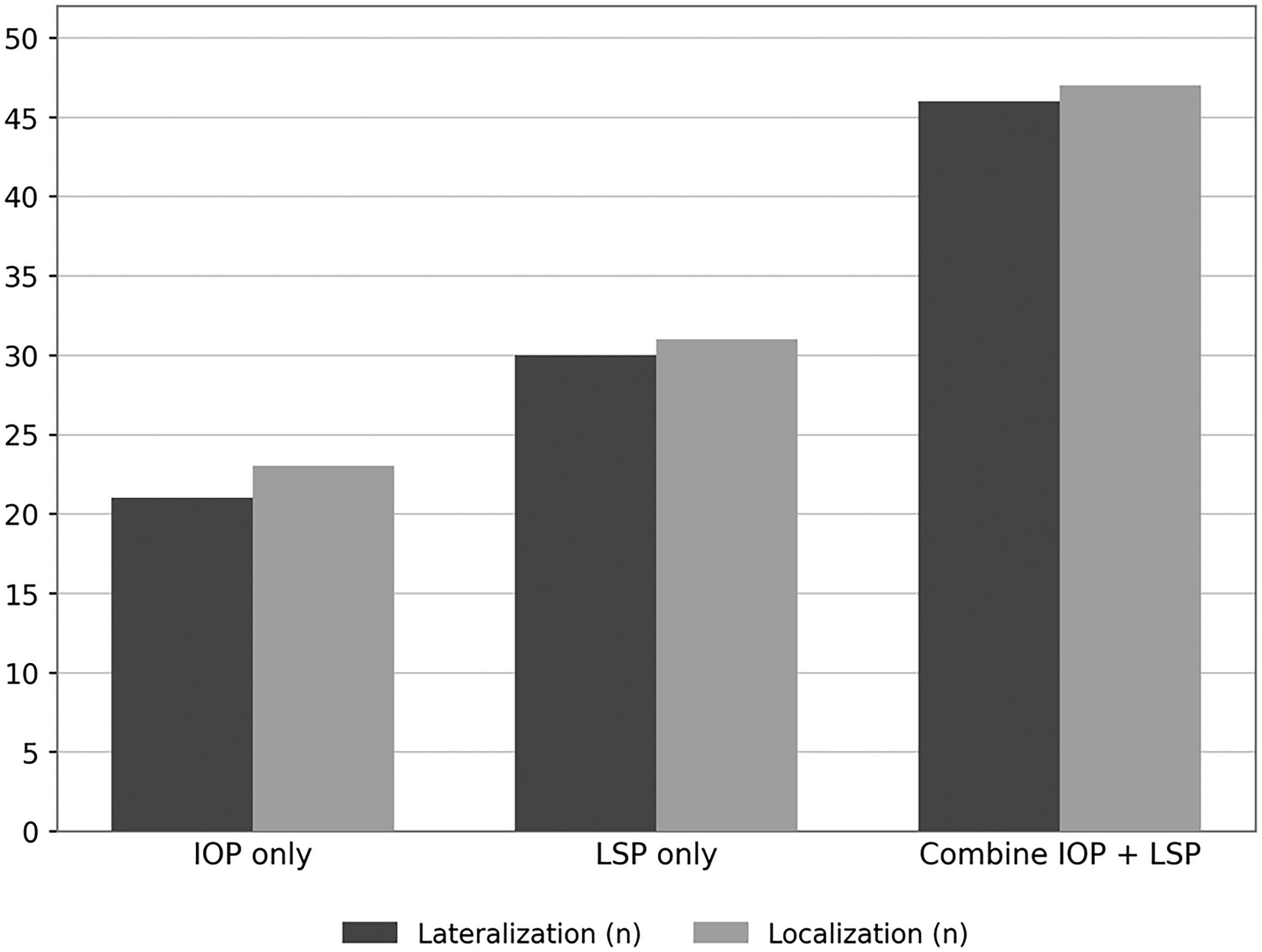
Comparative yield of ictal onset, late significant and combined patterns in scalp EEG at the patient level. IOP, ictal onset pattern; LSP, late significant pattern.
Inter-Rater Reliability
Inter-rater agreement before consensus adjudication was substantial for both the morphological classification of ictal onset patterns and LSP morphology, and almost perfect for hemispheric lateralization. The most frequent points of disagreement involved the distinction between non-rhythmic activity and artifact-dominated onsets, which were resolved by joint review.
Interictal EEG and Seizure Semiology
Interictal EEG Findings
Interictal epileptiform discharges were observed in 56 patients (83.6%) and were absent in 11 patients (16.4%). At the patient level, interictal abnormalities were regional in 28 patients (41.8%), hemispheric in 15 patients (22.4%), bilateral with side predominance in four patients (6.0%), bilateral without side predominance in nine patients (13.4%), and absent in 11 patients (16.4%).
Seizure Semiology
Seizure semiology analysis revealed temporal lobe onset in 154 seizures (63.6%), frontal onset in 60 seizures (24.8%), and non-localizable onset in 28 seizures (11.6%). Lateralizing semiological signs were identified in 170 seizures (70.2%), with a right hemisphere preference in 100 seizures (41.3%) and a left hemisphere preference in 70 seizures (28.9%). At the patient level, semiology indicated a temporal onset in 41 patients (61.6%), frontal onset in 17 patients (25.0%), and indeterminate onset in 9 patients (13.4%). Semiologic lateralization was achieved in 52 patients (77.6%).
Magnetic Resonance Imaging Findings
Magnetic resonance imaging findings indicated structural abnormalities in 28 patients, accounting for 41.8% of the cohort. Mesial temporal sclerosis (MTS) was the most prevalent lesion, identified in 20 patients, with 13 right-sided and seven left-sided cases. Additional abnormalities, such as cortical dysplasia, focal atrophy, hippocampal asymmetry, arachnoid cysts, and developmental venous anomalies, were observed in eight patients. MRI-facilitated hemispheric lateralization in all 65 structurally abnormal seizure events was used as a reference comparator for concordance analyses.
Multimodal Concordance
Multimodal comparisons revealed variable, yet clinically meaningful, alignment across diagnostic modalities. The agreement between ictal and interictal EEG was fair when all categories were considered (κ = 0.354), improving to substantial under strict right-left classification (κ = 0.775). Ictal EEG demonstrated substantial concordance with seizure semiology (κ = 0.647), with patient-level agreement observed in 41 of 67 patients (61.3%). Concordance between ictal EEG and MRI in patients with structural abnormalities was strong (κ = 0.710). Interictal EEG exhibited moderate agreement with seizure semiology (κ = 0.431), whereas interictal EEG–MRI agreement showed the strongest cross-modal alignment, achieving almost perfect concordance (κ = 0.859). These multimodal κ values were derived using the combined ictal interpretation (onset + LSP) at the patient level. The lower lateralization yields obtained from onset patterns or LSPs in isolation, evident in Figures 3 and 4, imply correspondingly lower agreement when either component is used alone.
Discussion
Ictal scalp EEG is an essential tool in the presurgical evaluation of focal epilepsy, complementing imaging and clinical data analysis. Although invasive intracranial recordings are the gold standard for pinpointing the true seizure focus,11,12 their limited availability and higher risk make it imperative to extract the maximum information from noninvasive EEG.
In our series, we found that focusing on the entire seizure evolution, rather than only the earliest EEG change, was associated with higher localization yields. In particular, the addition of LSPs increased the proportion of seizures and patients in whom lateralizing or localizing information could be identified compared to the analysis of ictal onset patterns alone. This highlights that many of the most informative EEG features emerge seconds after seizure onset; if one examines only the initial transient, critical localizing clues may be overlooked.
These results align with those of previous studies, showing wide variability in scalp ictal patterns across epilepsy types. Temporal lobe seizures are classically associated with organized, rhythmic 5–9 Hz theta activity at or near the onset,4-6 whereas extratemporal epilepsies often begin with low-amplitude, disorganized, or unclassifiable discharges. 7 In our cohort, attenuation or low-voltage fast activity (LVFA) was among the most frequent early patterns across all lobes, consistent with prior reports.8,9 However, its lateralizing value was modest, except in well-circumscribed temporal cases.
Frontal lobe seizures often begin with nonspecific fast or mixed activity, reflecting rapid spread; such “pseudotemporal” patterns (in which frontal onset mimics a temporal rhythm on scalp EEG) have been described previously.15,16 These misleading early features limit the localizing power of the onset alone in patients with frontal epilepsy.
In contrast, once seizures evolved into a stable rhythmic discharge, the scalp EEG became much more localized. We observed that late theta/alpha rhythms and repetitive spike–sharp wave complexes frequently indicated the point at which the epileptogenic region could be identified. This is in agreement with earlier studies, which indicated that organized rhythmic ictal discharges carry stronger lateralizing and localizing information than the very first EEG change.8,9
For example, temporal lobe seizures in our patients reliably progressed to 5–9 Hz theta/alpha waves, particularly in those with mesial temporal sclerosis; this late rhythmic pattern is a well-known marker of temporal onset and is associated with favorable surgical outcomes.4-6,17 Conversely, frontal seizures tend to develop late repetitive spikes or sharp waves, 10 which provide the main clues for lateralization. In addition to localization, emerging evidence suggests that ictal scalp EEG patterns may also reflect the underlying epileptogenic etiology.
In surgical temporal lobe epilepsy cohorts, hippocampal sclerosis has been associated with longer-lasting theta-dominant ictal activity, whereas tumor-related epilepsies more frequently exhibit shorter ictal durations and alpha/beta-dominant onset patterns. 18 Such etiology-dependent differences in ictal frequency profiles may offer a pathophysiological explanation for the higher diagnostic value of late-ictal patterns observed in specific patient groups in our cohort. Taken together, these findings underscore that a systematic evaluation of the evolving ictal EEG, not only the spike at onset, is critical for accurate noninvasive localization.
The improvement observed in the combined analysis is unlikely to reflect a single mechanism. Different generators contribute to different temporal phases of the seizure: ictal onset is dominated by activity from the seizure-onset zone, but on the scalp, it is frequently obscured by deep generators, low signal-to-noise, or rapid propagation. The late significant pattern emerges once the seizure has recruited a sufficient cortical volume to produce a synchronized, organized discharge and is therefore more likely to generate a lateralized scalp signature, even when the onset is non-lateralized. The two patterns thus carry partially independent information; when both are informative, the assignment is reinforced, and when only one is informative, the combined analysis ‘rescues’ seizures that would otherwise be classified as non-lateralized.11,12
Our multimodal concordance analysis further emphasizes the benefits of integrating scalp EEG with other diagnostic data. Across the cohort, ictal EEG lateralization substantially agreed with imaging and semiology. In particular, patients with clear structural lesions showed excellent alignment between EEG, MRI, and clinical features. Those with unilateral mesial temporal sclerosis almost always had ipsilateral interictal spikes and ictal onsets, mirroring classic reports.19,20
In such well-defined cases, some authors have argued that ictal EEG recording may not be necessary if the interictal EEG and MRI findings are concordant. 19 Our findings are consistent with this observation in that patients with concordant EEG and MRI findings demonstrated clear lateralization on scalp recordings; however, these results should be interpreted cautiously and do not replace outcome-based validation.
In contrast, patients without a clear lesion or with extratemporal epilepsy often have more discordant results, highlighting the need for a comprehensive approach. In several cases, our ictal EEG was equivocal or non-lateralized; however, other modalities offered clarity. This situation has been noted in prior studies of MRI-negative or extratemporal cases21,22: neither EEG nor imaging alone may reliably localize, so a combined analysis of interictal spikes, seizure semiology, and EEG evolution becomes essential.
Indeed, we found that even when the earliest ictal pattern was nonspecific, integrating late ictal features with lateralizing signs (such as head deviation or dystonia) and interictal EEG markedly improved accuracy. This mirrors earlier observations that combining scalp EEG with clinical lateralizing signs significantly boosts lateralization precision. 23
Particular caution is required in patients with discordant imaging, dual pathology, or multifocal or shifting seizure foci. In these complex cases, LSP analysis should not be interpreted in isolation from other diagnostic tools. However, recurrent late rhythmic activity consistently converging on the same hemisphere across multiple seizures may still provide supportive lateralizing information, particularly when ictal onset patterns are unclear. Conversely, persistent discordance between onset, LSP, and imaging findings may indicate the need for invasive evaluation rather than direct surgical decision-making. Therefore, we consider LSP analysis a complementary noninvasive tool rather than a substitute for intracranial EEG.
The diagnostic yield of scalp EEG also varies according to seizure type. Unsurprisingly, no focal aware seizures (FAS) in our series produced clear ictal scalp discharges, consistent with the notion that seizures originating deep in the cortex or medial temporal structures can remain “scalp negative”. 11 In contrast, most focal impaired awareness seizures (FIAS) and focal-to-bilateral tonic–clonic seizures (FBTCS) in our patients showed lateralized patterns; approximately 62% of FIAS and 70% of FBTCS were lateralized on EEG. This reinforces that more intense and widespread seizures tend to generate detectable scalp signals and supports the practice of capturing multiple seizures of various types during monitoring.
Practical Implications
Several practical points emerge for routine presurgical EEG interpretation. First, interpreters should avoid over-reliance on the earliest EEG changes; the most informative features in our cohort, particularly well-formed rhythmic discharges, often appeared several seconds after seizure onset, and the emergence of a sustained 5–9 Hz theta rhythm should carry substantial weight as an indicator of temporal lobe onset. Second, no single modality is foolproof; convergence between EEG, MRI and semiology generally predicts a well-defined epileptogenic zone, while patients with concordant scalp EEG and MRI findings (such as MTS or focal cortical dysplasia) can in selected cases proceed to surgery without invasive monitoring. Third, routine reporting should explicitly note any late significant patterns. As shown here, documenting the evolution of ictal rhythms increased the localization yield in our cohort; this simple, no-cost addition to standard EEG interpretation may be particularly valuable in MRI-negative cases where subtle EEG clues guide surgical planning. Finally, vigilance is warranted in extratemporal epilepsy, where frontal and occipital seizures frequently produce diffuse or misleading scalp patterns; non-lateralised or discordant EEG in these contexts should not be considered reassuring, and invasive intracranial monitoring should be considered to avoid the risk of incorrect localization.
Limitations
This study has several limitations. Most importantly, postoperative surgical outcomes were not available for any patient in this cohort; therefore, the true accuracy of ictal onset patterns and LSPs in identifying the epileptogenic zone could not be validated against postsurgical seizure freedom, which remains the definitive benchmark for localization. Formal inter-rater reliability statistics (Cohen's κ) were not pre-specified or calculated as part of the original study design. Although every seizure was independently reviewed by two experienced neurophysiologists with consensus adjudication, the absence of a quantitative agreement estimate is acknowledged as a limitation of this study. Future prospective studies incorporating reproducibility analyses would strengthen the reliability of ictal pattern classification and LSP interpretation. Although standardized, the visual classification of ictal patterns retains an unavoidable degree of subjectivity. Future computational EEG approaches (quantitative time-frequency analysis, independent-component decomposition) may improve reproducibility and reduce observer dependency of the results. We also did not perform a formal sensitivity analysis using a stricter 3-s clinical-onset window, and the cohort size in either subgroup was insufficient to support reliable separate κ estimates for temporal and extratemporal epilepsy. Formal subgroup analyses in larger cohorts would be a valuable next step in this research. The cohort included a heterogeneous group of MRI-negative and extratemporal cases in whom the true onset zone often remains uncertain without invasive recordings or postoperative confirmation. As a retrospective single-centre analysis, the distribution of seizure types and the proportion of temporal versus extratemporal epilepsies may not fully reflect larger surgical populations, underscoring the need for prospective multicentre studies incorporating invasive EEG and postoperative outcomes. Our findings should therefore be regarded as hypothesis-generating: they motivate, rather than replace, the validation of LSP analysis against surgical outcomes in prospective, surgically operated cohorts.
Conclusion
Systematic evaluation of the full ictal evolution on scalp EEG, particularly the incorporation of late significant patterns, enhances noninvasive localization and lateralization in adults with focal epilepsy. While ictal onset patterns alone often lack sufficient discriminatory power, the emergence of late rhythmic theta/alpha activity or repetitive spike–sharp wave complexes provides additional localizing information, particularly in temporal and frontal lobe epilepsies. The strong concordance observed between ictal EEG, interictal findings, MRI and semiology supports the value of a multimodal approach in presurgical assessment. The absence of postoperative outcome data precludes the definitive validation of these electrophysiological markers, and our findings should be regarded as hypothesis-generating. Prospective studies incorporating both scalp and invasive EEG with postsurgical outcome data are required to establish the diagnostic utility of LSP-guided localization, particularly in MRI-negative cases or settings in which invasive monitoring is limited.
Footnotes
Acknowledgements
The authors would like to thank all clinicians and EEG technicians who contributed to the acquisition and interpretation of the video-EEG recordings.
Ethics Statement
The study was approved by the Dokuz Eylul University Non-Interventional Research Ethics Committee (approval number: 2016/14-32, file no: 926-GOA; date: 26 May 2016). Given the retrospective nature of the study, the requirement for informed consent was waived. All procedures were conducted in accordance with the Declaration of Helsinki.
Consent for Publication
Not applicable. No identifiable individual participant data are presented in this manuscript.
Author Contributions
DAM contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. ND contributed to conception and design; contributed to acquisition, analysis, and interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. İÖ contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy. BB contributed to conception and design; contributed to interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to ethical and privacy restrictions but are available from the corresponding author on reasonable request.