
Abstract
Objective:
To identify factors associated with White matter hyperintensities burden in adults with focal epilepsy.
Methods:
We conducted a retrospective review of 60 patients with focal epilepsy treated at the Second Affiliated Hospital of Xinjiang Medical University between October 2024 and October 2025. Patients were selected according to predefined inclusion and exclusion criteria. All patients underwent 17-h scalp video electroencephalography and 3 T brain magnetic resonance imaging (3D T1 and 3D FLAIR sequences, 1.0-mm slices). Clinical features were documented from caregiver-reported symptoms, video recordings, seizure frequency and duration during the preceding two months, and medical history. Seizure type and epilepsy classification were determined in a multidisciplinary conference in accordance with the 2017 International League Against Epilepsy guidelines. White matter hyperintensities (WMH) in the frontal, temporal, parietal, and occipital lobes and the periventricular region were scored using the modified Scheltens scale, and a total WMH score was calculated. Non-parametric tests were used to compare regional WMH scores. The total WMH score was categorized into four levels: 0 (score ≤1), 1 (score >1-5), 2 (score >5-10), and 3 (score ≥10). Univariate and multivariate ordinal logistic regression analyses were performed to identify risk factors associated with WMH burden.
Results:
White matter hyperintensities were observed in 71.7% of patients. Lesions were predominantly located in the subcortical U-fibers and deep white matter, with fewer in the white matter adjacent to the cortex and in the corpus callosum. Frontal lobe WMH scores were significantly higher than temporal and occipital scores (P < 0.05). Most WMH were smaller than 3 mm in diameter(58%), whereas larger lesions were uncommon(42%). In multivariate analysis, age (OR = 1.60, 95% CI 1.01-1.10), seizure duration (OR = 1.06, 95% CI 1.13-2.24), and the presence of interictal epileptiform discharges (OR = 5.83, 95% CI 1.71-19.87) were independently associated with greater WMH burden. After adjustment for age, seizure duration, interictal epileptiform discharges, and a seizure frequency exceeding once per day were identified as independent risk factors for WMH burden.
Conclusion:
WMH are common in adults with focal epilepsy, and the frontal lobe is the most frequently affected region. Age, interictal epileptiform discharges, and seizure duration are independent risk factors for greater WMH burden. WMH may serve as an imaging marker for clinical seizure severity.
Keywords
Introduction
Focal epilepsy has traditionally been considered a disorder originating from a localized epileptogenic focus, but growing evidence now suggests that it is fundamentally a large-scale brain network disorder. 1 White matter tracts serve as the anatomical substrate for transmitting neural signals in the brain; thus, their structural integrity and functional status are essential for maintaining normal brain function. Neuroimaging studies consistently reveal widespread white matter changes in epilepsy patients, manifesting at the microstructural level as increased diffusivity and reduced fractional anisotropy (FA) and at the macroscopic network level as decreased global and local efficiency.2,3 Notably, these changes are not limited to the epileptogenic focus; they are also observed in white and gray matter regions distant from it, reflecting the widespread nature of the epileptic network. 4 Animal models further confirm that recurrent focal seizures can cause widespread structural damage to major white matter tracts in both hemispheres. 5
Among these white matter changes, white matter hyperintensities (WMH) are among the most visible and easily quantifiable markers on conventional magnetic resonance imaging (MRI). The prevalence of WMH is higher in patients with focal epilepsy than in healthy individuals, with a complex and varied pathological basis. In specific etiologies, such as focal cortical dysplasia (FCD), WMH is directly associated with developmental pathological changes, including poor myelination and axonal fiber loss.4,6 For most patients, the reduction in FA, which indicates myelin loss or axonal injury, may result from secondary Wallerian degeneration triggered by recurrent seizures.7,8 Furthermore, Antiseizure Medications(ASMs) may contribute to this process. Studies have shown that patients treated with enzyme-inducing ASMs carry a significantly higher burden of WMH. 9 These findings suggest that both the epilepsy itself and its treatment contribute to the formation and progression of WMH, with epilepsy-related white matter microstructural damage potentially developing into visible WMH over time. 10
There is a bidirectional interaction between white matter networks and epilepsy. On the one hand, white matter serves as a key pathway for the conduction of epileptic discharges, and changes in its diffusion parameters can assist in localizing the epileptogenic focus, especially in MRI-negative patients. 11 Conversely, lesions in white matter can serve as an initiating factor for epilepsy. WMH, a marker of cerebral small vessel disease, may increase the risk of late-onset epilepsy by affecting cortical microstructure or causing microinfarcts. 12 This bidirectional relationship underscores that WMH is not only a consequence of epilepsy but also a potential causal and modifying factor, with its burden likely closely tied to disease severity and clinical outcomes. 2
Although the importance of WMH in epilepsy is increasingly recognized, current research primarily addresses descriptive phenomena. There remains a lack of systematic, multivariable analyses identifying which factors—such as epilepsy duration, seizure frequency, seizure duration, antiseizure medication types, and vascular risk factors—are independent risk factors for increased WMH burden and of assessing their relative importance. This knowledge gap limits our ability to identify high-risk patients and develop targeted management strategies.
Accordingly, this cross-sectional study aims to systematically investigate the clinical risk factors associated with WMH burden in patients with focal epilepsy. The findings are expected to elucidate key drivers of epilepsy-related white matter injury, to provide a theoretical foundation for future research on the adjunctive localization of epileptogenic foci and on interventions aimed at mitigating white matter damage, and to offer insights into the involvement and disruption of white matter tracts within the epileptic brain network. 5
Materials and Methods
Research Participants
This retrospective analysis included 60 adults with focal epilepsy who met the inclusion and exclusion criteria between October 2024 and October 2025. Patients aged 14 to 18 years were included because their brain development was considered to have largely reached maturity. The screening flowchart is shown in Figure 1.
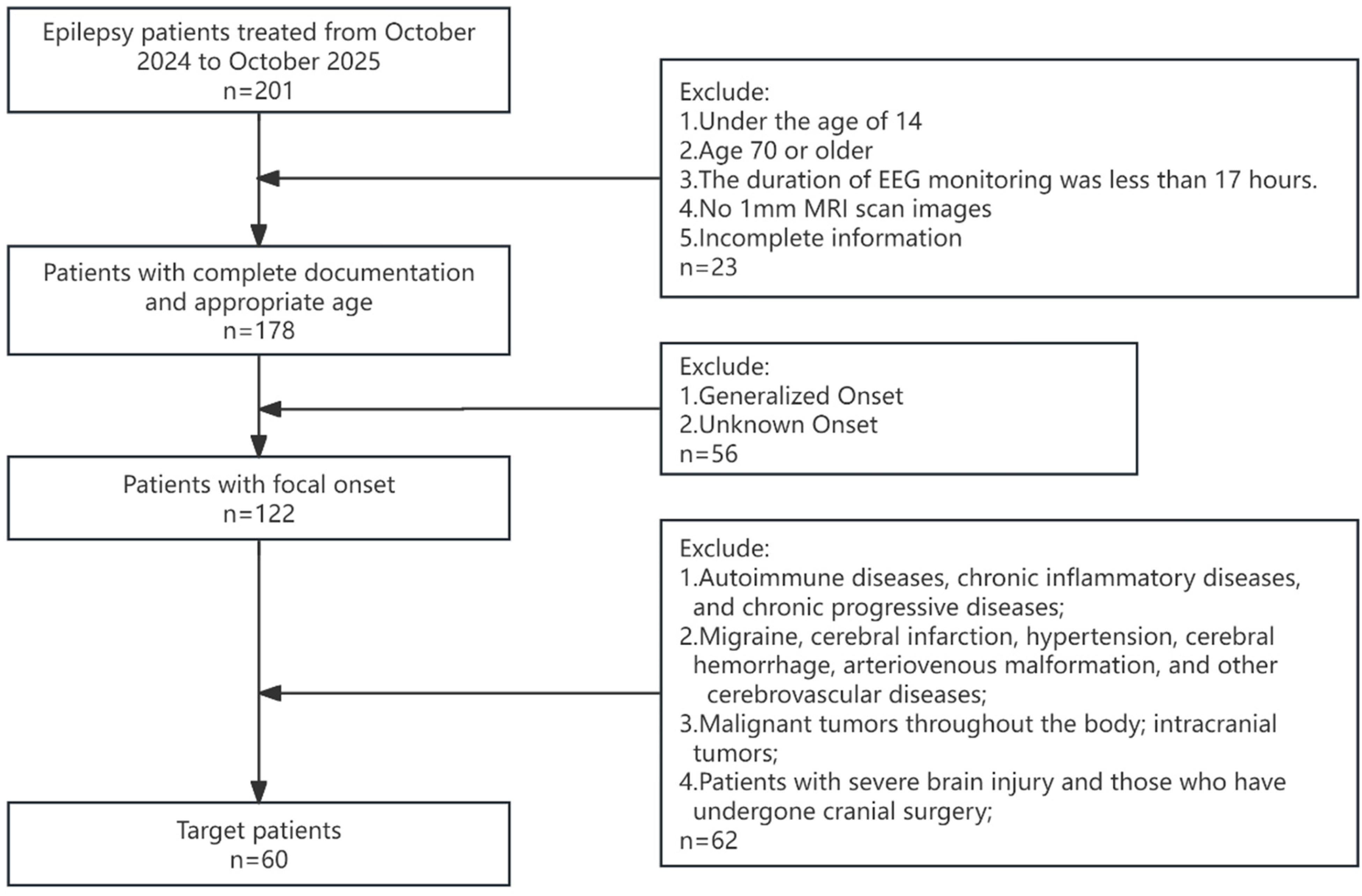
Flow diagram of the enrollment process.
Inclusion criteria were as follows: (1) age 14–70 years, with a diagnosis of focal epilepsy confirmed by a multidisciplinary team according to the 2017 International League Against Epilepsy guidelines; (2) completion of a 3 T epilepsy-protocol MRI and 17-h video electroencephalography (EEG) monitoring that included at least one full sleep cycle; and (3) availability of detailed seizure semiology, including seizure videos provided by patients or caregivers, seizure frequency before the visit, and complete long-term video EEG and 3 T MRI data.
Exclusion criteria were as follows: (1) autoimmune diseases, chronic inflammatory disorders, or other chronic progressive systemic conditions; (2) cerebrovascular and related disorders, including migraine, ischemic stroke, hypertension, intracerebral hemorrhage, and arteriovenous malformations; (3) systemic malignancies or intracranial tumors; and (4) a history of severe traumatic brain injury or previous neurosurgical procedures; (5) multifocal epilepsy.
MRI, EEG Data Acquisition, and Analysis
All patients underwent 3 T MRI on a Philips Ingenia scanner (Koninklijke Philips N.V., Amsterdam, Netherlands). The imaging protocol included a 3D T1-weighted sequence (TR/TE, 8.2/3.7 ms; matrix, 240 × 240; number of signal averages [NSA], 1; isotropic voxel size, 1 mm3; no gap), a 3D FLAIR sequence (TR/TE/TI, 6000/340/1800 ms; matrix, 240 × 241; NSA, 1; isotropic voxel size, 1 mm3; no gap), and a high-resolution in-plane 2D coronal T2-weighted sequence (TR/TE, 3000/120 ms; matrix, 376 × 374; NSA, 1; slice thickness, 2 mm).
Target sequences were registered to the Montreal Neurological Institute (MNI) 152 brain template for spatial normalization. Brain regions were parcellated using the normalized space, and WMH were rated using the modified Scheltens scale, with separate scores assigned to periventricular and lobar regions according to the following rules. Periventricular hyperintensities (score range 0-6) were rated according to three items: (1) occipital caps (0-2); (2) frontal caps (0-2); (3) periventricular bands (0-2). For each item: 0 = no lesion; 1 = lesion <5 mm; 2 = lesion 6–10 mm. Lobar WMH (score range 0-24) were rated for the frontal (0-6), parietal (0-6), occipital (0-6), and temporal (0-6) lobes as follows: 0 = no abnormality; 1 = lesions ≤3 mm and ≤5 in number; 2 = lesions ≤3 mm and ≥6 in number; 3 = lesions 4–10 mm and ≤5 in number; 4 = lesions 4–10 mm and ≥6 in number; 5 = lesions ≥11 mm and ≥1 in number; 6 = confluent lesions. Other MRI abnormalities were excluded from scoring. Regional subscores and a total score were calculated. The diameter of each WMH was manually delineated.
EEG was recorded continuously with a Nihon Kohden EEG-1200c system (Japan) equipped with a 32-channel JE-921A amplifier and Neuroworkbench 0510 recording software. Electrode placement followed the international 10–20 system, with Cz as the default reference. The sampling rate was 250 Hz, and electrode impedance was maintained below 50 kΩ. Epileptiform discharges were defined as sharp waves, spikes, spike–slow wave complexes, polyspike–slow wave complexes, or generalized paroxysmal discharges. Recording parameters were a sensitivity of 7–10 μV/mm, a time constant of 0.1–0.3 s, and a paper speed of 30 mm/s (equivalent display speed in the digital system).
Quality Control
Brain MRI scans were reviewed independently by two senior radiologists in a single-blind manner. Data were cross-checked for consistency, and any discrepancies were resolved by consensus. Video-EEG recordings were interpreted jointly by two physicians with intermediate-level certification in electroencephalography, as accredited by the China Association Against Epilepsy.
Clinical data were analyzed using SPSS (version 24) and R software (version 4.5.1). Inter-rater reliability was assessed using Cohen's kappa with quadratic weights, with 95% confidence intervals, and was interpreted according to the criteria of Landis and Koch; this analysis was performed using the irr package in R. Normality of continuous variables was tested using the Shapiro–Wilk test. Variables approximating a normal distribution were presented as mean ± standard deviation. Comparisons of continuous variables across multiple groups were conducted using the Kruskal–Wallis test for independent samples. Multivariate ordinal logistic regression was used to assess associations. A two-sided p value of <0.05 was considered statistically significant.
Results
Baseline Characteristics and Variables
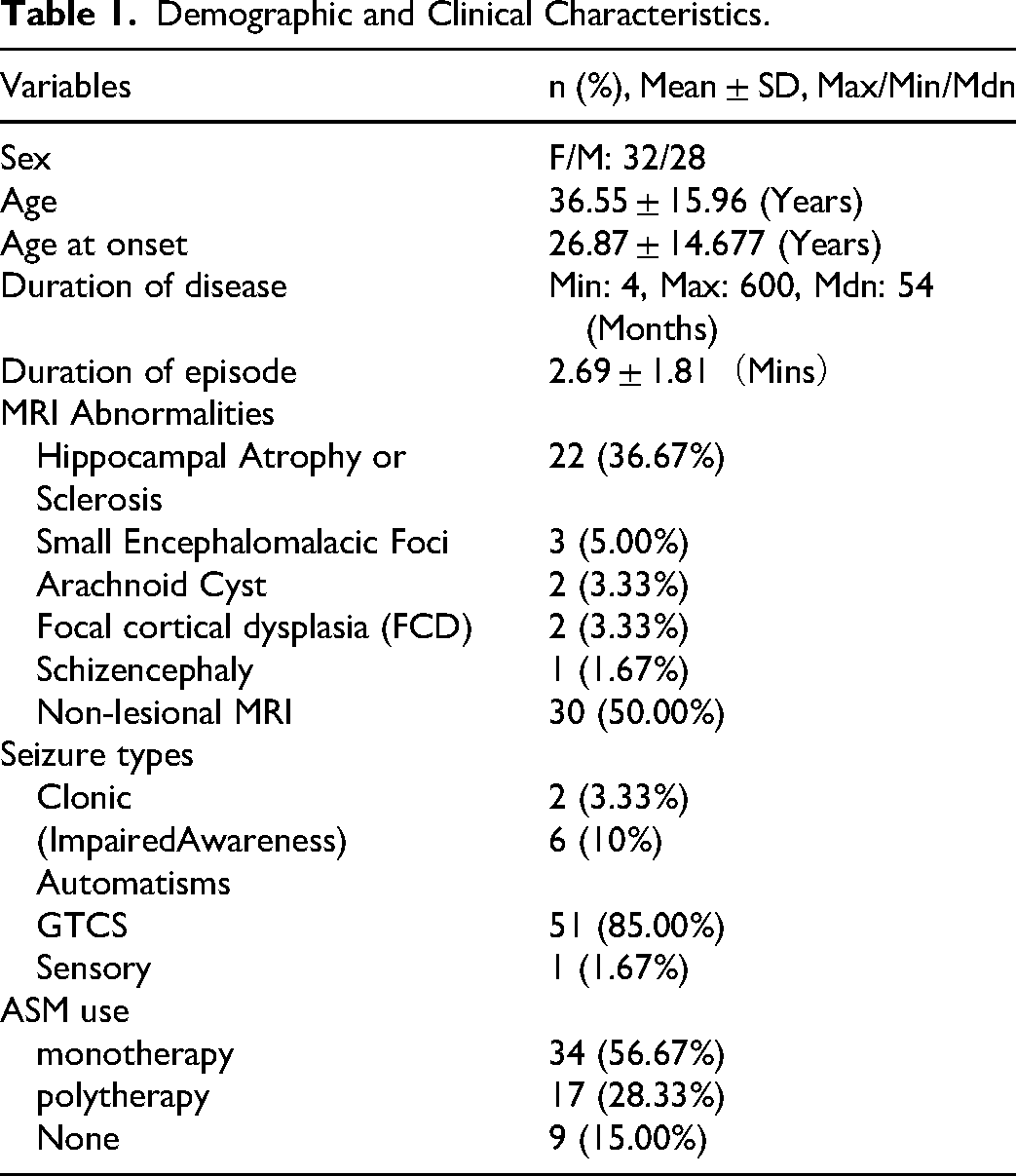
The clinical characteristics of the 60 enrolled patients are summarized in Table 1. The mean age of the cohort was 36.55 ± 15.96 years, and 53.33% of the patients were female. MRI abnormalities were absent in 30 patients, and 85.00% of patients had generalized tonic-clonic seizures among their seizure types.
To identify risk factors for WMH, multivariate logistic regression analysis was performed using clinical features coded according to the system described in Table 2. The “Score” column denotes the numerical values assigned to each categorical variable for inclusion in the model.
Risk Factors Associated with WMH Burden
Univariable ordinal logistic regression analysis revealed that age (p = 0.006), seizure duration (p = 0.024), seizure frequency of at least once per day (p = 0.011), and interictal epileptiform discharges (IEDs) (p < 0.001) were significantly associated with WMH severity. Sex, disease duration, seizure frequency of ≤1 per week, symptomatology, presence of MRI abnormalities, and antiseizure medication use showed no significant associations (all p > 0.05). Variables with p < 0.05 in univariable analysis were entered into a multivariable ordinal logistic regression model. Multivariable analysis identified age (OR = 1.06, 95% CI: 1.01-1.10, p = 0.012), seizure duration (OR = 1.60, 95% CI: 1.13-2.24, p = 0.007), and the presence of IEDs (OR = 5.83, 95% CI: 1.71-19.87, p = 0.005) as independent predictors of WMH severity. Detailed results of the univariable and multivariable analyses are presented in Table 3
Demographic and Clinical Characteristics.
Participants’ Demographic Characteristics and the Variables are Categorized as Follows.
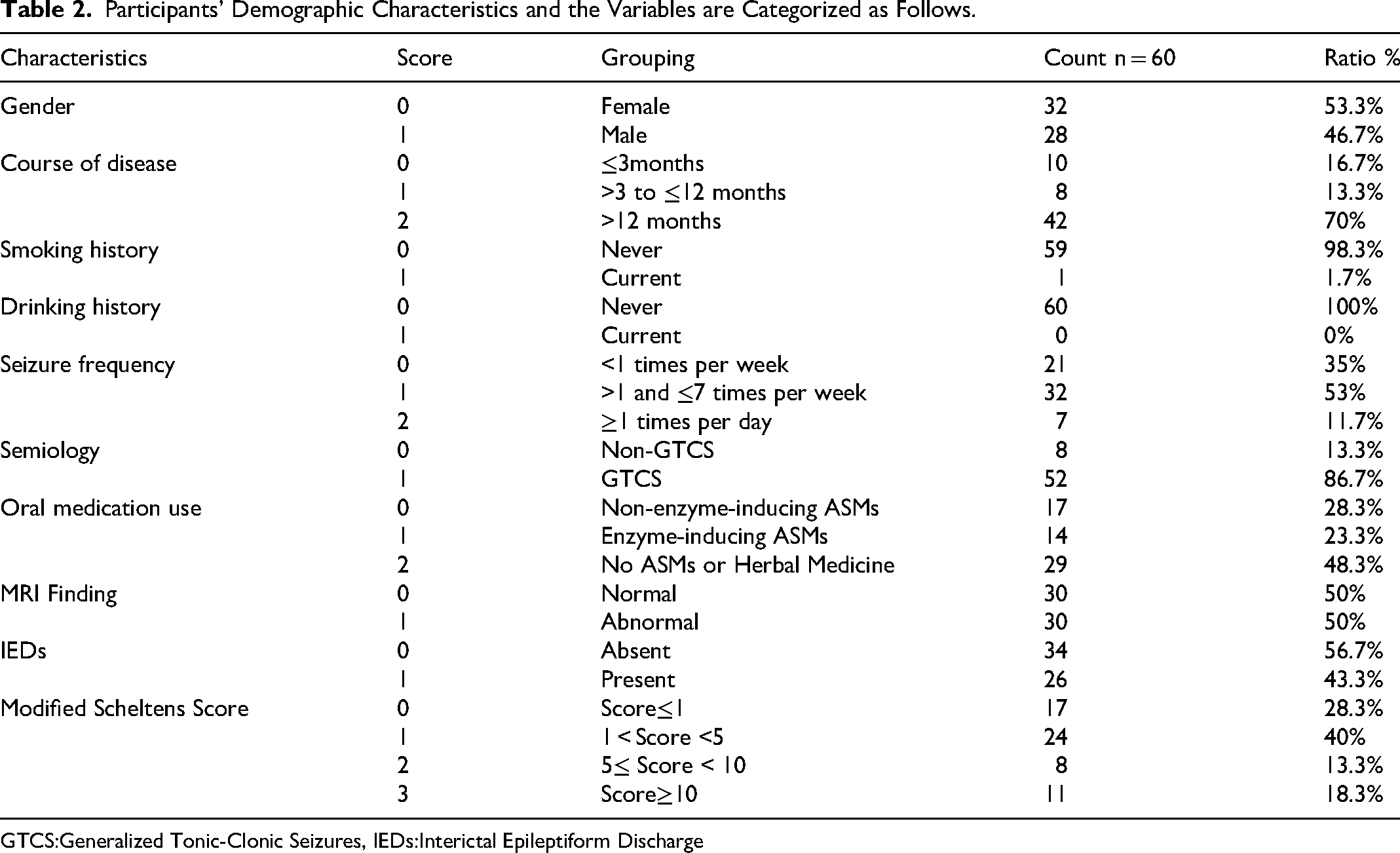
GTCS:Generalized Tonic-Clonic Seizures, IEDs:Interictal Epileptiform Discharge
Factors Associated with White Matter Hyperintensities in Univariate and Multivariate Analyses.
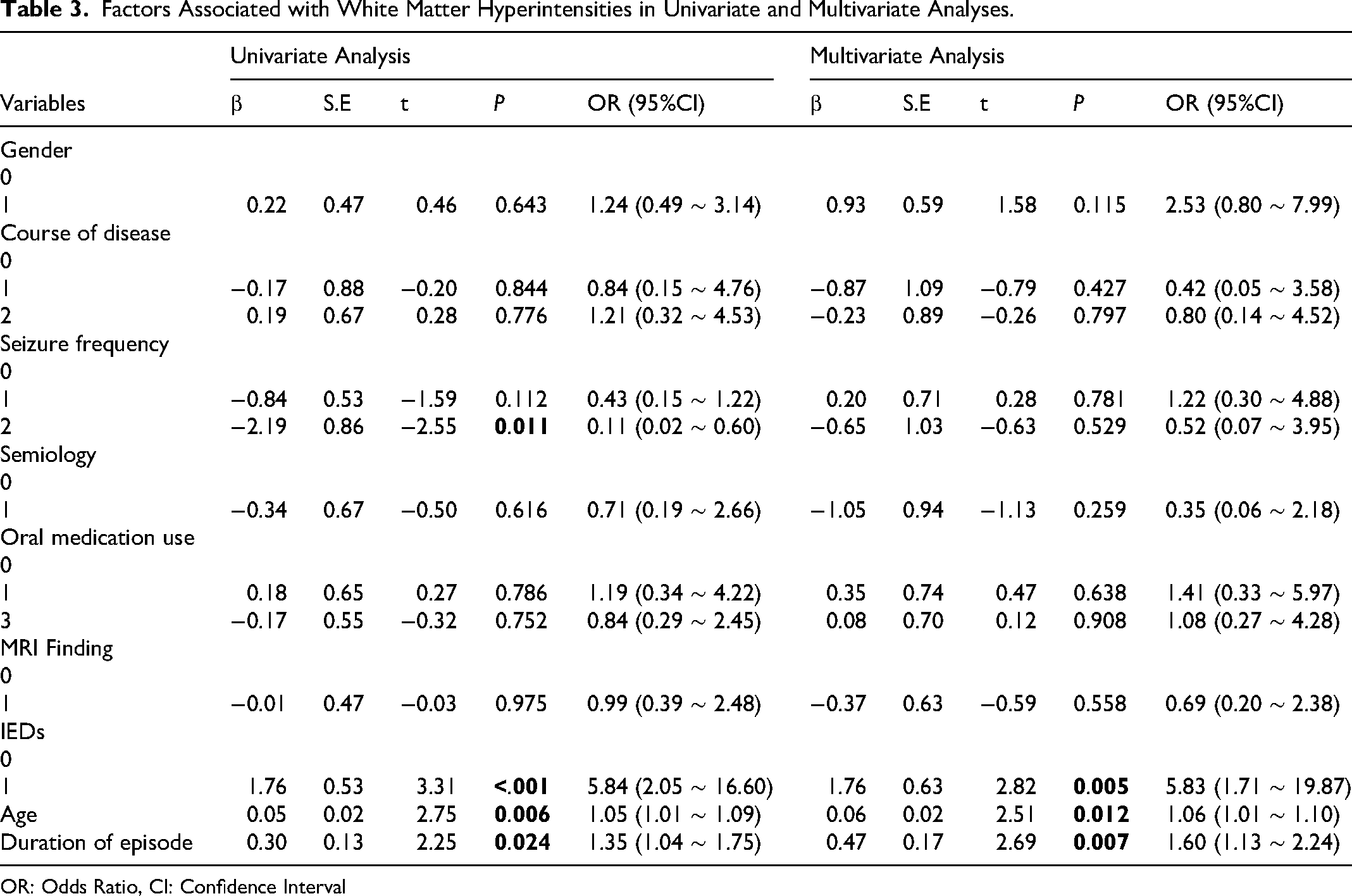
OR: Odds Ratio, CI: Confidence Interval
The forest plot from the multivariable logistic regression analysis is presented in Figure 2
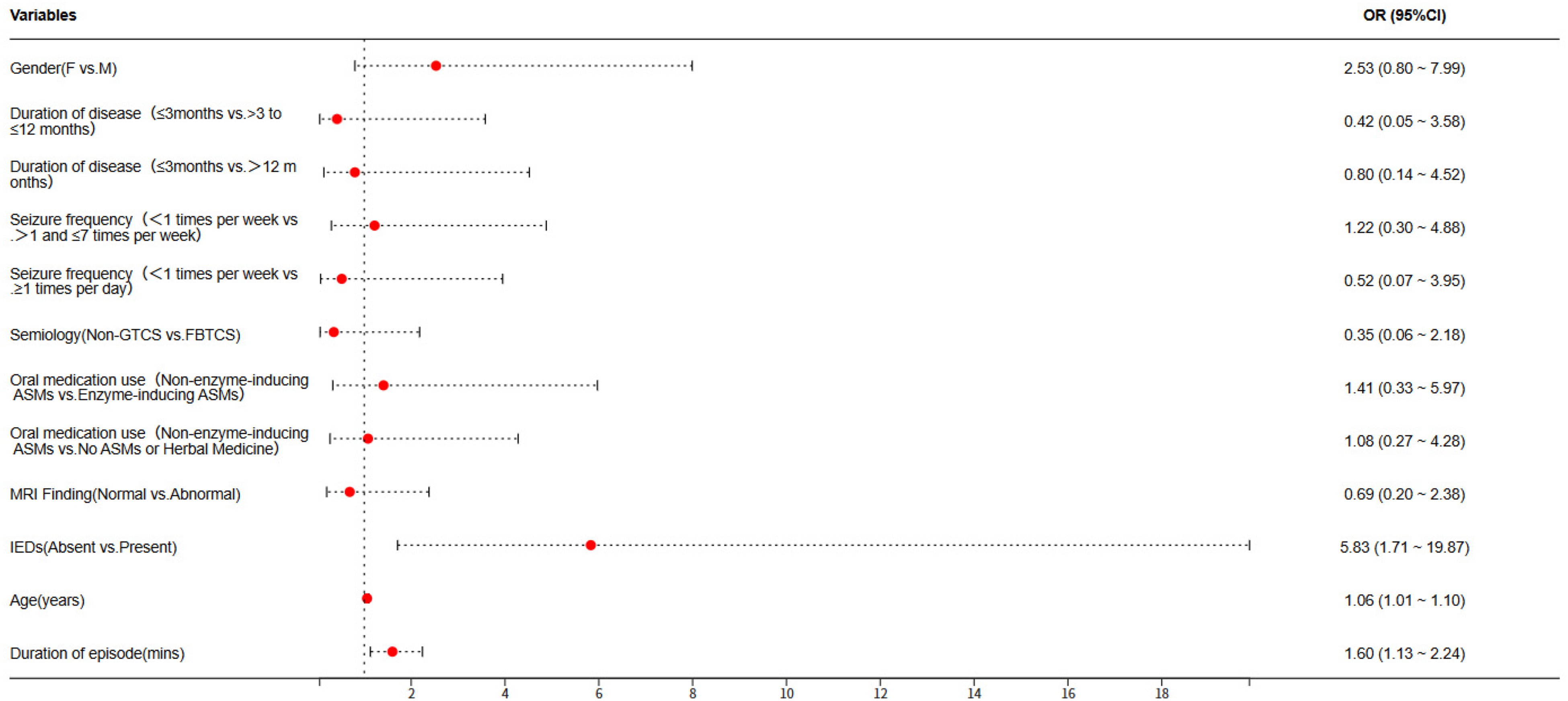
Forest plot of risk associations for white matter hyperintensities.
Regional Differences in WMH Scores
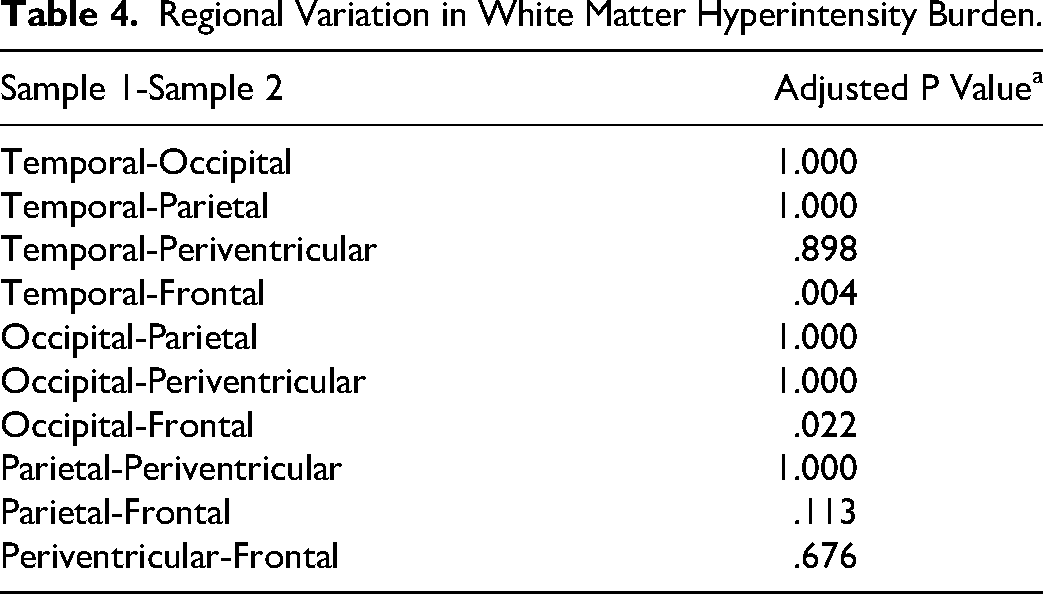
Regional differences in WMH burden were assessed using the modified Scheltens scale. Inter-rater reliability, assessed using Cohen's kappa with quadratic weights, was substantial (κ = 0.82, 95% CI: 0.74-0.89). As WMH scores did not follow a normal distribution (Shapiro–Wilk test, p < 0.05), regional differences in WMH burden were compared using the Kruskal–Wallis test. Post hoc pairwise comparisons with the Bonferroni correction revealed that frontal lobe WMH burden was significantly higher than that in the temporal lobe (adjusted p = 0.004) and the occipital lobe (adjusted p = 0.022). No other significant differences were observed among regions (adjusted p > 0.05). Detailed pairwise comparison results are presented in Table 4. The absolute counts and percentages of WMH lesions for each brain region are presented in Table 5.
Regional Variation in White Matter Hyperintensity Burden.
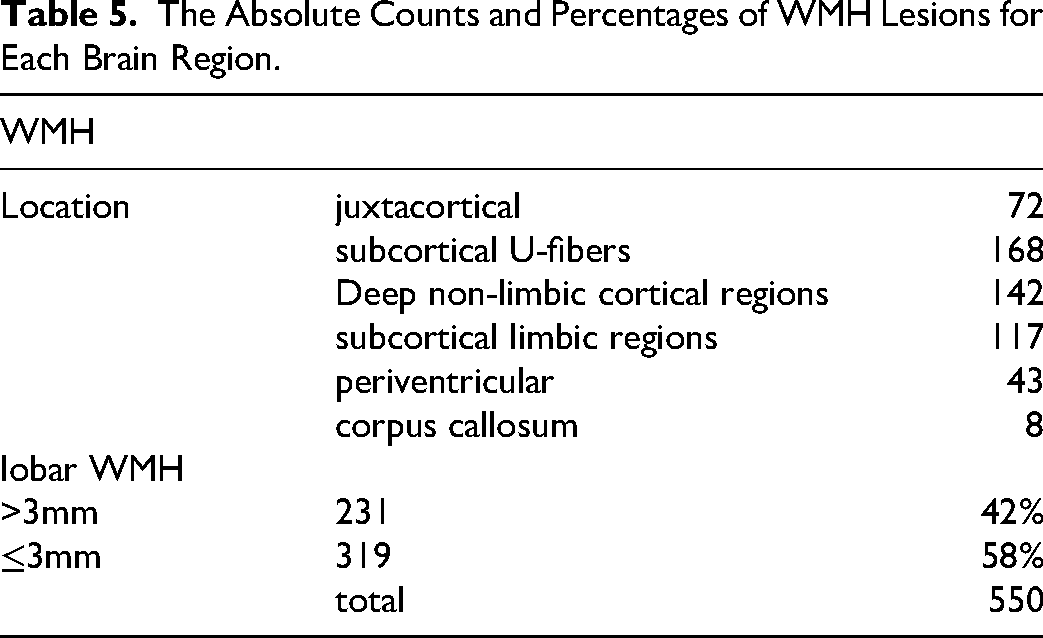
The Absolute Counts and Percentages of WMH Lesions for Each Brain Region.
Case Presentation
MRI images from two patients with WMH, together with their clinical information, are shown in Figure 3.
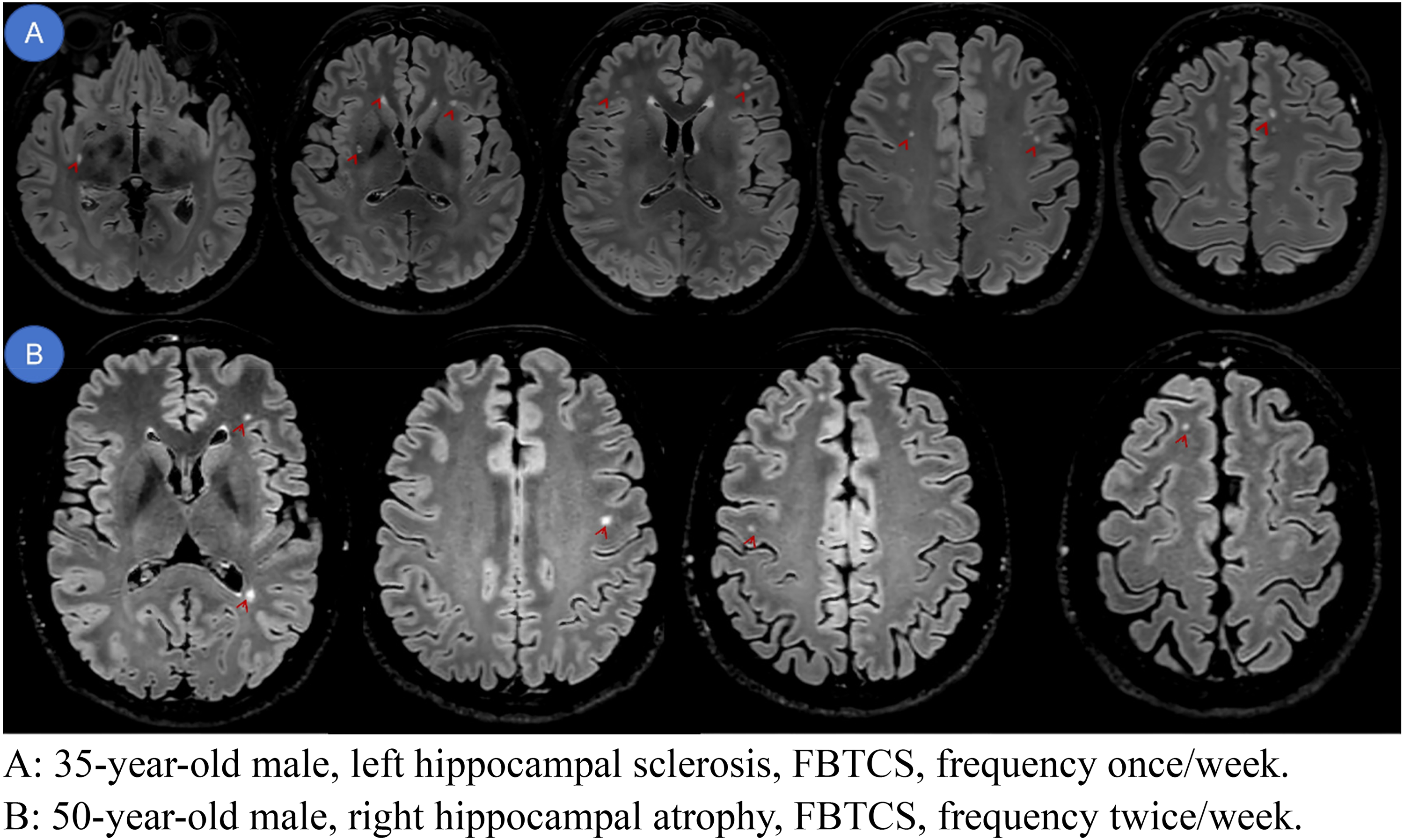
A: 35-year-old male, left hippocampal sclerosis, FBTCS, frequency once/week. B: 50-year-old male, right hippocampal atrophy, FBTCS, frequency twice/week.
Discussion
Research on WMH has predominantly focused on dementia, with relatively few studies conducted in the context of epilepsy. WMH are closely associated with disruption of white matter structural integrity and reduced interhemispheric functional connectivity, with the latter linked to declines in processing speed and executive function. 13 Aging is an independent factor influencing both the prevalence and severity of WMH, with age-related risk factors contributing to its development.14,15 A greater baseline WMH volume increases the risk of cognitive impairment and dementia. 16 WMH volume has also been associated with essential tremor. 17 The location and severity of WMH affect cognitive deficits and may provide clues to the underlying etiology; frontal and parietal WMH have been linked to impairments in executive function and memory.18–21
Evidence suggests that patients with epilepsy are more likely to exhibit WMH, particularly those treated with enzyme-inducing antiseizure medications. 9 White matter tract damage has been observed in patients with temporal lobe epilepsy and hippocampal sclerosis. 11 In children and adolescents with temporal lobe epilepsy, bilateral white matter involvement may reflect developmental brain plasticity and the widespread nature of epileptic networks. 3 The extent of WMH in early to middle adulthood may predict the subsequent development of late-onset epilepsy 12 and is also associated with antiseizure medication use. 9
In the present study, no association was found between enzyme-inducing antiseizure medications and WMH. The frontal lobe was the most common site of WMH in our cohort; whether this spatial distribution relates to seizure propagation remains uncertain and warrants further investigation. Age, IEDs, and seizure duration were identified as independent risk factors for WMH. Based on current evidence, a spatial correlation between IEDs and WMH cannot be established, primarily because the sites of white matter pathology do not correspond predictably to IED localization and because IEDs are limited by poor spatial resolution, making it difficult to accurately reflect specific anatomical locations.
Further investigation of spatial associations will require more advanced technical approaches, representing a direction for our ongoing research. Notably, the presence of generalized tonic-clonic seizures was not identified as a risk factor for WMH in this study—a finding that diverges from conventional understanding and warrants validation in larger cohorts. In the present study, 42% of WMH were >3 mm in diameter, whereas 58% were round or oval lesions measuring <3 mm. The lesions were predominantly located in subcortical U-fibers, deep non-limbic cortical regions, and deep limbic cortical regions, whereas periventricular and juxtacortical areas were also relatively frequently involved, and the corpus callosum was rarely affected. This distribution pattern differs markedly from that of WMH attributed to other etiologies, suggesting an underlying mechanism distinct from that of cerebrovascular disease. This may also explain the low detection rate on conventional slice-thickness MRI, as WMH in this cohort were relatively small in volume, posing challenges for automated detection; consequently, manual counting was employed rather than volumetric analysis.
Our findings support the view that clinical investigations should consider not only the size but also the location of WMH. 22 A meta-analysis of studies on temporal lobe epilepsy suggested that WMH are predominantly confined to unilateral subcortical regions, particularly the posterior cerebral cortex or areas surrounding preexisting lesions. 4 Recurrent seizures may induce axonal injury in ipsilateral fiber tracts and cause associated secondary Wallerian degeneration. 4 In patients with refractory temporal lobe epilepsy, secondary white matter degeneration may occur in the corpus callosum, with pathological changes extending beyond the temporal lobe to involve the contralateral limbic system, thalamus, and remote extratemporal structures.7,8
WMH observed on MRI can be considered indicative of white matter tract injury. Whether the spatial distribution of these lesions corresponds to critical nodes within the electrical conduction network remains unexplored, and the underlying biological mechanisms of such injury have not been elucidated. The relationship between white matter damage and seizure activity also remains unclear—whether the injury is caused by epileptic electrical activity, ischemia, hypoxia, or immune-mediated processes remains to be determined. Moreover, whether white matter injury can recover following seizure control is unknown. Additionally, no studies have investigated whether the distribution of white matter damage may aid in localizing epileptogenic foci. The present study provides only a preliminary exploration of the association between IEDs and WMH burden; further in-depth investigation is needed to clarify the risk factors for WMH and their relationship with epileptic electrical conduction pathways. Strict inclusion and exclusion criteria were applied in this study to minimize confounding factors and ensure the reliability of the findings. Nevertheless, WMH remained associated with age, and after adjusting for age, a significant correlation between WMH and seizure duration persisted.
This study has several limitations. First, its retrospective design and relatively small sample size may limit statistical power to detect differences between groups. Although some studies have suggested that deep learning methods do not outperform conventional approaches for WMH identification and segmentation, 23 this was not examined in the present study. The modified Scheltens scale was used, which demonstrates good reliability and validity; it enables assessment of both lesion size and location as well as the number of deep white matter lesions and shows good correlation with WMH volume. This scale may be particularly sensitive in longitudinal observation of WMH progression and its relationship with clinical manifestations.
Future studies may consider using machine learning for automated segmentation and volumetric analysis, combined with fiber tractography to localize affected tracts and map them to standard space. 24 However, some have suggested that spatial normalization may introduce inaccuracies in volumetric measurement. Future work should also incorporate source localization analysis using scalp EEG to enhance study quality and reproducibility. Scalp EEG abnormalities show some degree of spatial deviation from their underlying anatomical structures; increasing electrode density may improve spatial correspondence. Future studies with larger sample sizes could employ spatial overlap analysis using radiomics and source localization techniques to further investigate the mechanisms underlying WMH formation in patients with epilepsy and its relationship to the epileptic network.
Footnotes
Acknowledgment
During the preparation process, the authors checked all texts for spelling and grammar using translation software tools such as Chatgpt 4. The authors took full responsibility for the content of the publication. We thank Bullet Edits Limited for the language editing assistance.
Ethics Statement
The study protocol was reviewed and approved by the Ethics Committee of The Second Affiliated Hospital of Xinjiang Medical University (Approval No. 2023TSYCLJ0030). Due to the retrospective nature of the study, the requirement for written informed consent was waived by the IRB.
Author Contributions
X.Z. and W.J.Z. contributed equally to this work. They were responsible for conceptualizing the research direction, designing the study, collecting and curating the data, and drafting the original manuscript. CG, MBH, RL was responsible for reviewing the literature and organizing the references. K.L. (the corresponding author) oversaw the entire project, including supervision, project administration, and validation of the findings. He also provided the collaborative vision, secured funding, and was responsible for reviewing and editing the final manuscript. All authors read and approved the final manuscript. All authors have participated sufficiently in the work and agreed to be accountable for all aspects of the work.
Funding
This research was funded by the Leading Talents in Science and Technology Innovation Program, Urumqi, China [2023TSYCLJO030].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All inquiries should be directed to the corresponding author. The data are available upon reasonable request.
Registered Clinical Trial (RCTs)
Not Applicable