
Abstract
Background
Persistent depressed consciousness in severe coronavirus disease 2019 (COVID-19) is commonly attributed to hypoxemia, systemic inflammation, sedative exposure, or metabolic disturbance. Non-convulsive status epilepticus (NCSE), however, may be overlooked without electroencephalography (EEG). This diagnostic principle also applies to persistent unexplained encephalopathy more broadly, particularly when impaired consciousness remains disproportionate to systemic illness.
Case
An 85-year-old woman with Parkinsonism, diabetes mellitus, and prior cerebrovascular disease developed severe COVID-19 pneumonia followed by persistent coma during intensive care. Brain computed tomography showed chronic atrophic change without acute structural lesions, and laboratory and cerebrospinal fluid findings did not identify a major alternative explanation for coma. On the day of EEG, arterial blood gas analysis showed adequate oxygenation without hypercapnia. EEG on hospital day 10 demonstrated abundant right-hemispheric rhythmic/periodic discharges at approximately 2 Hz and focal electrographic seizures arising from the right temporal region with spatiotemporal evolution, consistent with NCSE. Levetiracetam, lacosamide, and midazolam infusion were administered.
Outcome
Midazolam infusion was followed by electrographic seizure resolution but did not produce immediate clinical awakening during sedation; spontaneous eye opening emerged approximately 4 days later. Follow-up EEG on hospital day 13 showed seizure resolution with residual diffuse slowing and a sporadic right-hemispheric spike.
Conclusion
This case highlights early EEG as a practical diagnostic and treatment-monitoring tool in severe COVID-19-associated encephalopathy when depressed consciousness is persistent or disproportionate to systemic illness. More generally, EEG should be considered in persistent unexplained coma or encephalopathy after stabilization of cardiopulmonary factors.
Introduction
Neurological complications of COVID-19 include encephalopathy, cerebrovascular events, seizures, and status epilepticus. In critically ill patients, impaired consciousness is often multifactorial and may reflect hypoxemia, sepsis, systemic inflammation, metabolic derangement, or sedative exposure. EEG abnormalities are common in patients with COVID-19-associated encephalopathy, but most findings are nonspecific, including diffuse slowing, focal slowing, rhythmic activity, and periodic patterns.1,2
NCSE is a clinically important and potentially treatable cause of coma because it may occur without overt motor convulsions. EEG is therefore essential when bedside examination and systemic evaluation do not sufficiently explain persistent depressed consciousness. This principle is not limited to COVID-19; EEG should be considered in persistent unexplained encephalopathy or coma in general when impaired consciousness is disproportionate to systemic illness. We report an older patient with severe COVID-19-associated encephalopathy in whom early EEG identified treatable NCSE and serial EEG documented treatment response.
Case Report
An 85-year-old woman with Parkinsonism, type 2 diabetes mellitus, and prior cerebrovascular disease presented with severe COVID-19 pneumonia and progressive impairment of consciousness. Severe acute respiratory syndrome coronavirus 2 infection was confirmed by polymerase chain reaction, with a cycle threshold value of 17.8. Chest radiography showed right lung consolidation, and brain computed tomography demonstrated mild cerebral atrophy and periventricular lucency without acute hemorrhage, infarction, or mass effect.
She received remdesivir and dexamethasone for severe COVID-19 pneumonia. Respiratory failure progressed, and endotracheal intubation was required on hospital day 7. Tocilizumab was subsequently administered. Despite treatment of pneumonia and supportive intensive care, her neurological status deteriorated to coma.
Laboratory evaluation showed elevated inflammatory markers and mild hypomagnesemia but no major hepatic, renal, thyroid, or cerebrospinal fluid abnormality sufficient to explain the depth of coma. Cerebrospinal fluid showed no pleocytosis. Because persistent coma appeared disproportionate to systemic factors alone, EEG was obtained on hospital day 10.
On the day of EEG evaluation, arterial blood gas analysis showed pH 7.601, PaCO₂ 24.8 mm Hg, PaO₂ 212.0 mm Hg, HCO₃− 23.9 mmol/L, base excess 2.2 mmol/L, and oxygen saturation 99.6%. These findings indicated marked alkalemia with hypocapnia under ventilatory support, without persistent hypoxemia or hypercapnia sufficient to explain the depth of coma. Arterial blood gas, laboratory, and cerebrospinal fluid results relevant to systemic contributors to coma are summarized in Supplementary Table S1.
The initial EEG demonstrated abundant rhythmic/periodic discharges lateralized to the right hemisphere at approximately 2 Hz. Sequential EEG epochs then showed early right temporal ictal activity and subsequent spatiotemporal evolution in rhythmicity, amplitude, and field distribution, consistent with focal electrographic seizures and NCSE (Figure 1A–C).

Initial EEG on hospital day 10 demonstrating non-convulsive status epilepticus.
Levetiracetam and lacosamide were administered, followed by midazolam infusion under EEG monitoring. Midazolam infusion was continued for approximately 48 h. During midazolam treatment, there was no immediate improvement in consciousness, as expected in the setting of sedative infusion; however, the EEG background became suppressed and the epileptiform/electrographic seizure pattern resolved. Follow-up EEG on hospital day 13 showed resolution of NCSE, with residual diffuse background slowing at 5 to 6 Hz, superimposed 1 to 2 Hz slow waves, and a sporadic right-hemispheric spike maximal at C4 (Figure 2). Approximately 4 days after midazolam treatment, the patient developed spontaneous eye opening, with improvement from E1M1VT to E4M1VT, with verbal response not testable because of endotracheal intubation. The patient was later transferred for ventilator weaning before hospital discharge.
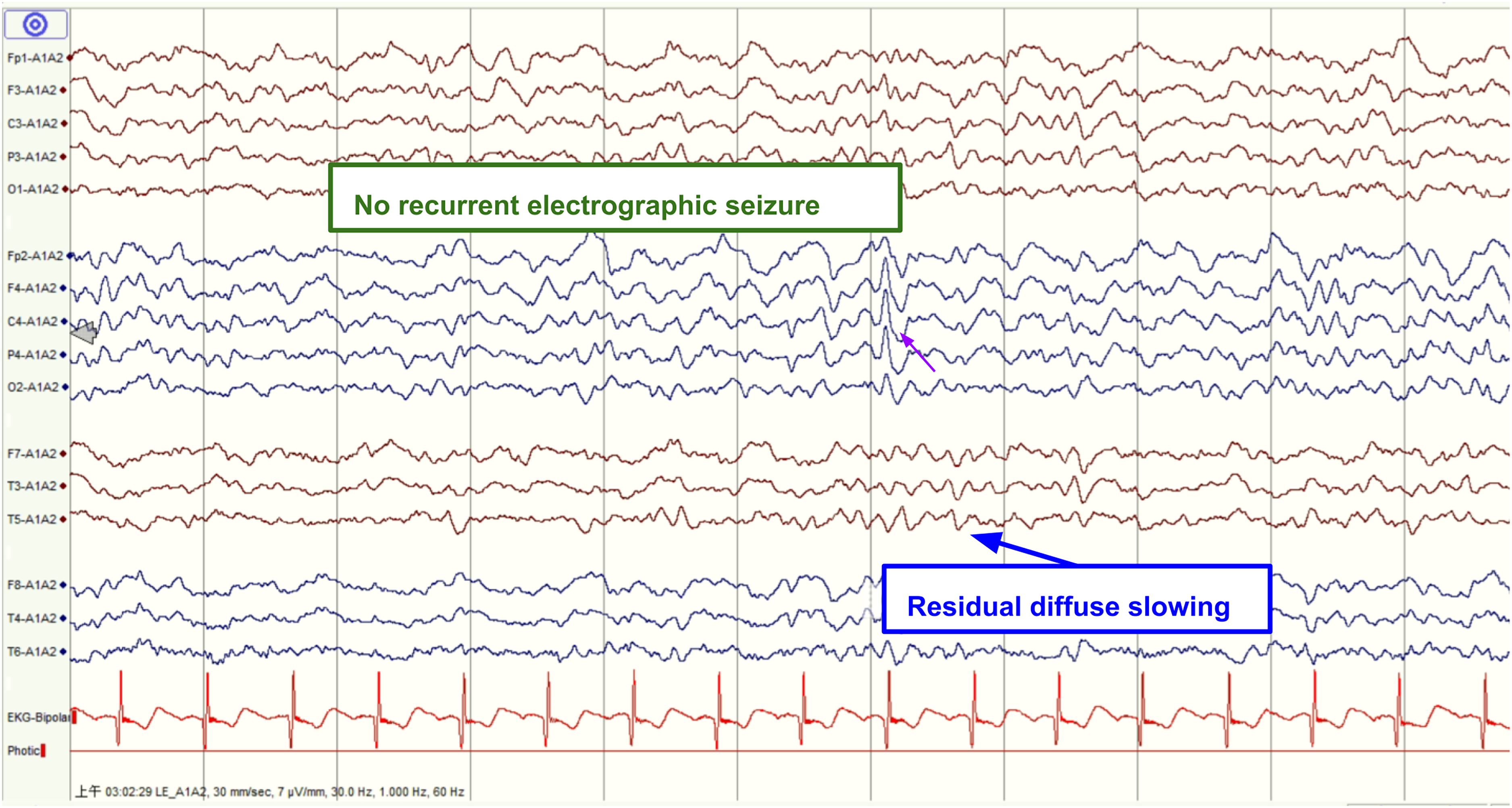
Follow-up EEG after midazolam treatment on hospital day 13.
Discussion
This case emphasizes that persistent coma in severe COVID-19 should not automatically be attributed to systemic illness alone. The clinical message is broader than COVID-19: persistent unexplained encephalopathy or coma should prompt consideration of EEG when impaired consciousness persists after stabilization of cardiopulmonary factors or remains disproportionate to systemic illness.
Published EEG studies in COVID-19 show that most abnormalities are nonspecific markers of encephalopathy, including diffuse slowing, focal slowing, rhythmic delta activity, and periodic patterns.1,2 Although acute symptomatic seizures appear uncommon among unselected hospitalized COVID-19 patients, with a pooled frequency of 0.71%, seizure risk is higher among patients selected for EEG evaluation, reaching 8.49% in one meta-analysis. 3 This supports targeted EEG use in critically ill patients with persistent unexplained coma. Status epilepticus and recurrent electrographic seizures have been reported in critically ill COVID-19 patients, but they represent a clinically important subset rather than the usual explanation for coma. 4
The clinical value of EEG in this case was twofold. First, it established a treatable diagnosis by demonstrating right temporal electrographic seizures and right-lateralized rhythmic/periodic discharges. Second, serial EEG documented treatment response, showing seizure resolution after antiseizure therapy and midazolam infusion. This before-and-after neurophysiological sequence is important because bedside examination alone could not distinguish NCSE from toxic-metabolic or inflammatory encephalopathy.
The arterial blood gas results on the day of EEG also clarify the clinical context. Although severe systemic infection and mechanical ventilation likely contributed to encephalopathy, the patient had adequate oxygenation and no hypercapnia when EEG was performed. Therefore, persistent depressed consciousness could not be fully attributed to hypoxemia or hypercapnia, and EEG was clinically justified to evaluate for an additional treatable neurological contributor.
The mechanisms linking COVID-19 and NCSE are likely multifactorial. Systemic inflammation, endothelial dysfunction, hypoxemia, metabolic stress, and blood-brain barrier disruption may lower seizure threshold.4,5 In this patient, advanced age, prior cerebrovascular disease, and Parkinsonism may have further reduced cerebral reserve.
Critical care EEG reporting should use standardized terminology. The 2021 American Clinical Neurophysiology Society terminology supports precise description of rhythmic and periodic patterns, distribution, frequency, and evolution. 6 In the present case, right temporal electrographic seizures with evolution supported NCSE rather than nonspecific encephalopathy alone. This interpretation is also consistent with consensus recommendations emphasizing prompt recognition and treatment of NCSE. 7 Similar COVID-19 presentations mimicking NCSE have also been described. 8
The absence of immediate clinical awakening during midazolam infusion does not argue against NCSE, because the sedative itself suppresses arousal. In this case, the most objective immediate treatment response was electrographic resolution, whereas clinical improvement was delayed and became evident after the sedative effect had subsided.
This report has limitations. Brain magnetic resonance imaging and long-term cognitive follow-up were unavailable, and sedative exposure and systemic inflammation may have contributed to encephalopathy. Nevertheless, the temporal relationship between EEG-confirmed NCSE, treatment, electrographic resolution, and delayed clinical improvement supports the diagnostic relevance of early EEG in this setting.
Conclusion
Early EEG should be considered when severe COVID-19-associated encephalopathy presents with persistent or disproportionate coma. Identification of NCSE can alter treatment and allow objective monitoring of neurological recovery. The same approach should be generalized to persistent unexplained encephalopathy or coma more broadly, particularly after oxygenation and ventilation have been stabilized.
Supplemental Material
sj-docx-1-eeg-10.1177_15500594261467526 - Supplemental material for Early EEG Detection of Treatable Non-Convulsive Status Epilepticus in Severe COVID-19-Associated Encephalopathy: A Case Report
Supplemental material, sj-docx-1-eeg-10.1177_15500594261467526 for Early EEG Detection of Treatable Non-Convulsive Status Epilepticus in Severe COVID-19-Associated Encephalopathy: A Case Report by Yu-Cheng Chu, Chan-Lin Chu and Shang-Yeong Kwan in Clinical EEG and Neuroscience
Footnotes
Acknowledgments
Not applicable.
Ethical Considerations
This study was approved by the Institutional Review Board of Far Eastern Memorial Hospital, Taiwan (FEMH IRB No. 111230-C).
Consent to Participate
Not applicable for this retrospective case report based on routinely collected clinical data; publication consent is stated below.
Consent for Publication
Written informed consent for publication of this case report and accompanying anonymized clinical images was obtained from the patient's legally authorized representative. The written consent is retained by the authors and is not submitted with the manuscript to protect patient confidentiality.
Author Contributions
Yu-Cheng Chu drafted the manuscript and collected clinical data. Chan-Lin Chu contributed to clinical data interpretation and manuscript revision. Shang-Yeong Kwan supervised the study and critically revised the manuscript for important intellectual content. All authors approved the final manuscript and consented to submission.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability
All data relevant to this case report are included in the article and Supplemental material. Additional de-identified clinical data are not publicly available because of patient privacy and institutional regulations.
Writing Assistance and use of Generative AI Tools
The authors used generative AI-assisted tools for language polishing, formatting support, and preparation of submission documents. The authors critically reviewed, edited, verified, and approved all scientific content and take full responsibility for the final manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.