
Abstract
Purpose. To assess the safety of anastomosis ring (EndoCAR) following chemoradiation. Methods. A total of 10 pigs received radiation to a bioequivalent dose of 4500 cGy with 4 doses of 5-fluorouracil 400 mg/m2 and leucovorin 20 mg/m2 intravenous bolus. On day 21, each animal underwent 2 rectal anastomoses, 10 cm apart, using a 27-mm EndoCAR device and a 29-mm circular stapler. Burst pressures, desmosine and hydroxyproline levels and radiographic leaks were assessed at 2 weeks. Results. In all, 8 pigs were included in the analysis (1 pig died, 1 specimen damaged at harvest). Leaks occurred in 6 (170-300 mm Hg) stapled and 2 ring anastomoses (150-200 mm Hg; P = .13). Internal circumferences were similar (5.5 vs 5.2 cm; P = .5). Desmosine and hydroxyproline levels were similar between groups. Conclusion. Rectal anastomosis, after chemoradiation to the pig rectum using a ring (EndoCAR), is similar to stapled anastomosis. Further trials are needed in humans to determine any clinical advantage associated with these findings.
Introduction
Colorectal cancer is the fourth most common malignancy in the United States, making colorectal resections and the subsequent colorectal anastomoses one of the most commonly performed operations in the world. Previous work from this institution has suggested that a colorectal anastomosis using the NiTi Endoluminal Compression Anastomosis Ring (EndoCAR) may be equivalent to—and in regards to burst strength and adhesion formation—superior to, the traditional circular stapled anastomosis. The costs, according to the manufacturer (NiTi Surgical Solutions, Netanya, Israel) are equivalent to the circular stapler (~$350-$400). 1
Of the estimated 157 000 new cases of colorectal cancer that were diagnosed in 2007, more than 25% of these will be rectal malignancies. Neoadjuvant chemoradiation has been associated with better local recurrence and disease-free survival rates after resection. Preoperative chemoradiation, however, has been implicated as a risk factor in developing anastomotic complications and pelvic sepsis.2,3 Quoted leak rates with the traditional circular stapled anastomosis in low anterior resection range from 3% to 10% for colorectal anastomoses and even higher for coloanal anastomoses.4-6 At this institution, the leak rate following low anterior resection after neoadjuvant chemoradiation is approximately 10%. 7 For the EndoCAR to be truly considered safe and effective for use in rectal cancer surgery, its safety must be proven in patients who have undergone preoperative chemoradiation.
Methods
This investigator-initiated study was performed with approval from the Washington University Animals Studies Committee, Department of Comparative Medicine, and the Office of Biological and Chemical Safety/Environmental Health and Safety. A total of 10 female domestic pigs, weighing an average of 41.3 kg (range 35.4-50.9 kg), were used to determine whether a compression anastomosis in the rectum would heal as well as a stapled anastomosis after chemoradiation.
The sample size was calculated using burst pressure measurements as the primary endpoint. The study was designed to demonstrate that the EndoCAR was equivalent in this regard to the traditional circular stapler, with a difference of 30% or more being considered statistically significant. To evaluate a continuous parameter such as burst pressure, while maintaining a type I error of 5% and a power of 80%, the minimum sample size was 6 procedures per arm. To account for a 10% to 20% drop-out rate because of technical issues, a sample size of 10 animals was chosen, with 1 of each type of anastomosis per animal.
On arrival to the animal facility, each of the animals was allowed at least 72 hours to acclimate to their new environment before any procedures were performed. The chemotherapy regimen was based on the National Comprehensive Cancer Network (NCCN) Practice Guidelines for neoadjuvant therapy for rectal cancer. We chose a regimen of 5-fluorouracil (5-FU) 400 mg/m2 intravenous (IV) bolus and leucovorin 20 mg/m2 IV bolus for 4 days, through an ear vein, starting on the same day as the radiation. The body surface area of the pigs was calculated using the formula from Kelley et al 8 : (surface area in cm2) = 734 (body weight in kg)0.656. The average daily dose of 5-FU for these pigs was 337 mg. The average daily dose of leucovorin was 16.8 mg. Modern radiation therapy methods were used in this study. Because of the practical considerations involved in transporting the animals to the radiation facility and delivering radiation under repeated general anesthesia, we opted for a single dose of radiation to achieve a bioequivalent dose in the range of 4500 cGy. Though it is not possible to completely reproduce a standard course of 4500 cGy in 25 fractions with a single fraction of radiation, doses from 920 to 1362 rads had been used previously and been found to cause histologic changes in the small bowel of mongrel dogs in previous studies.9,10 Given that these pigs were also to receive 5-FU, a known radiosensitizer, the dose used in this study was 1000 cGy calculated to the midplane.
A deceased pig of the planned weight underwent a computed tomography simulation in the supine position. Images were transferred to the treatment planning system (Philips Pinnacle 7.0, Madison, WI). The rectum was contoured and equally weighted opposed lateral 6 MV photons were planned to treat the rectum to a dose of 1000 cGy in a single fraction. Each pig was aligned using external landmarks and positioning was confirmed with portal imaging before the treatment fraction. An Elekta Precise linear accelerator (Elekta AB, Stockholm, Sweden) was used to deliver the therapy.
On the first day of treatment, the pigs were sedated with an intramuscular cocktail (TKX) of 2 mL of telazol (Wyeth, Madison, NJ), 250 mg of ketamine, and 250 mg of xylazine (Bayer, Munich, Germany). They were then placed under general anesthesia by a licensed veterinary technician and placed on a portable ventilator. Intravenous access was obtained via an ear vein and secured in order to prevent dislodgment over the next 4 days. 5-FU and leucovorin were administered as determined by the previously noted formula, and the pigs were then transported to the radiation facility.
After wrapping the pigs’ hindquarters to guard against any possible contamination of the radiation facility, the pigs underwent radiation as described above. They were then transported back to the animal facility, recovered, and extubated. The pigs then received 3 more days of 5-FU and leucovorin. Although this was usually able to be accomplished without sedating them, they occasionally required sedation to receive their medication, or to get a replacement IV catheter. This was accomplished by either intramuscular TKX or ketamine at the discretion of the supervising veterinarian.
Following the fourth day of chemotherapy, the IV catheters were removed, and the pigs were allowed to rest for 3 weeks. During this entire period, they were closely monitored on a regular pig chow diet, under the supervision of a licensed veterinarian, for any signs of toxicity, especially fever or lethargy.
After the 3-week rest period, the animals were given a 48-hour bowel preparation. This consisted of 0.5 gallon of NuLytely (Braintree Laboratories, Inc, Braintree, MA) supplemented with electrolyte-rich water 3 times a day. On the day of surgery, each pig was given only water. Each pig received antibiotic prophylaxis with 20 mg/kg of intramuscular cefazolin preoperatively. Oral cefazolin was continued postoperatively for 5 days in accordance with veterinary policy. All surgeries were accomplished via laparotomy through a 6-cm low midline incision under the supervision of a licensed veterinary technician. Each animal underwent 2 anastomoses in the rectum, one stapled and one compression, randomized to proximal and distal positions. Thus, each animal acted as its own internal control.
The proximal anastomosis was formed first using a 75-mm linear stapler to transect the rectum without disturbing the local or distal blood supply. The staple line was excised and a full-thickness purse-string suture was placed in the proximal rectum component using 2-0 monofilament nonabsorbable synthetic suture to secure the anvil of either the circular stapler or the EndoCAR, depending on the randomized assignment. An assistant introduced the base of the device into the rectum and deployed the pin through the center of the transverse staple line of the rectal stump. Taking care to avoid any twisting, the anvil and pin were joined. After full apposition of the 2 segments of bowel, the device was fired and the partially opened instrument removed. Proximal and distal donuts were inspected to ensure full-thickness tissue presence and concentricity.
The distal anastomosis was then formed in a similar fashion 10 cm distal to the first anastomosis once again without disturbing the local or distal blood supply to the rectum. The anastomoses were not leak tested and no irrigation of the abdomen or wound was performed. The fascia was reapproximated with interrupted figure-of-eight 0-Prolene (Ethicon, Cincinnati, OH) sutures. The subcutaneous tissue was closed with a running 0-Prolene suture, and 20 mL of 1% marcaine was injected as local anesthesia. The skin edges were approximated with staples and the incision was covered with a viscous skin adhesive. The pig was recovered and extubated.
Animals were monitored for the first 24 hours in a recovery room, which served as a step-down unit. The pigs received intramuscular buprenorphine 0.02 mg/kg for analgesia during the first evening after surgery and were given 200 mg of oral carprofen (Pfizer, New York, NY) the morning of postoperative day 1. A clear liquid diet was offered for the first 48 hours after surgery, followed by balanced calorie, protein, carbohydrate, and fat shakes for the next 24 hours. The next day, mash was started. Pig chow was initiated by postoperative day 4.
At 2 weeks postoperatively, the pigs were sedated with TKX and given pentobarbital for euthanasia. Each pig rectum was excised, and the abdomen inspected for any sign of leaks or abscesses. A barium radiograph was obtained to assess for anastomotic narrowing or leaks. Each anastomosis was then tested separately to determine failure pressure by dividing the bowel between the anastomoses leaving a 5 cm section of bowel attached to each side of each anastomosis. One end of the bowel was clamped, while a plastic tube was placed in the other end and secured with a plastic zip tie. The bowel was completely submersed in a large bowl of water at room temperature, and a hand-operated mercury sphygmomanometer was used to inflate the bowel with air. One examiner observed the water bath for air bubbles while a second examiner monitored the pressure reading on the sphygmomanometer to record the pressure at the exact moment of failure. The pressure recorded was the first pressure where air bubbles were observed, regardless of whether the anastomosis or native tissue failed. In cases where the bowel did not leak, the pressure recorded was the maximal pressure reached. Note was made of the absence or presence, as well as the site of failure relative to the anastomosis.
Next, the internal diameter of each anastomosis was measured and recorded. Samples from each anastomosis were then preserved in 10% formalin and sent for paraffin sectioning and staining for collagen and elastin using trichrome and Verhoef–Van Gieson stains respectively. Radioimmunoassay techniques were used to quantify desmosine concentrations as a marker for elastin, and amino acid analysis was performed to quantify the concentration of hydroxyproline as a marker for collagen.
Results
One animal died as a result of endotracheal tube dislodgment during transport back from the radiation facility. The other 9 pigs all survived up to their surgery and tolerated their surgery without complications. One pig became febrile in the time period between chemoradiation and surgery and was placed on empiric antibiotics for 5 days. Blood cultures remained negative and temperature returned to normal. There were no sequelae to the episode.
The burst pressures and location of the failure at 2 weeks are summarized in Table 1. The first animal we operated on was noted to have extremely friable tissue, and it was torn while making the ring anastomosis. This was oversewn by interrupted 3-0 polydioxanone (PDS) Lembert sutures and the animal did well postoperatively. However, at the time of sacrifice, dense adhesions were noted at both anastomoses, requiring sharp adhesiolysis, and a hole in the ring anastomosis was made during removal of the adhesions. Subsequent burst testing and radiology were abandoned in this pig. Although there was neither purulent nor fecal contamination on exploration, the dense adhesions suggest that there may have been a contained, subclinical leak. None of the animals had any sign of anastomotic leak, and there were no leaks detected on barium imaging of the harvested specimens. The pressures at which the anastomoses leaked and the internal circumferences for stapled and compression anastomoses are given in Tables 2 and3, respectively.
Burst Pressure and Location of Failure
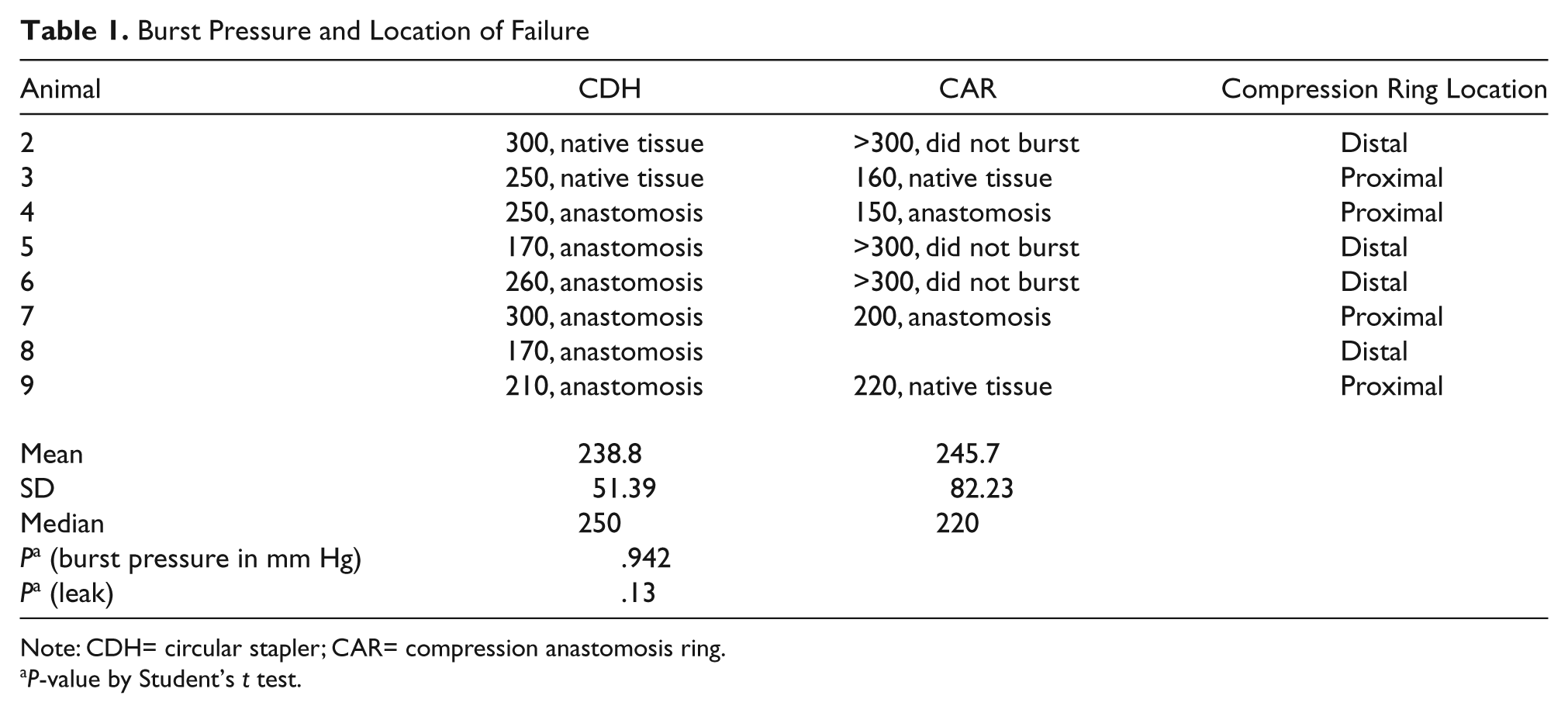
Note: CDH= circular stapler; CAR= compression anastomosis ring.
P-value by Student’s t test.
Pressure at Which Anastomoses Leaked
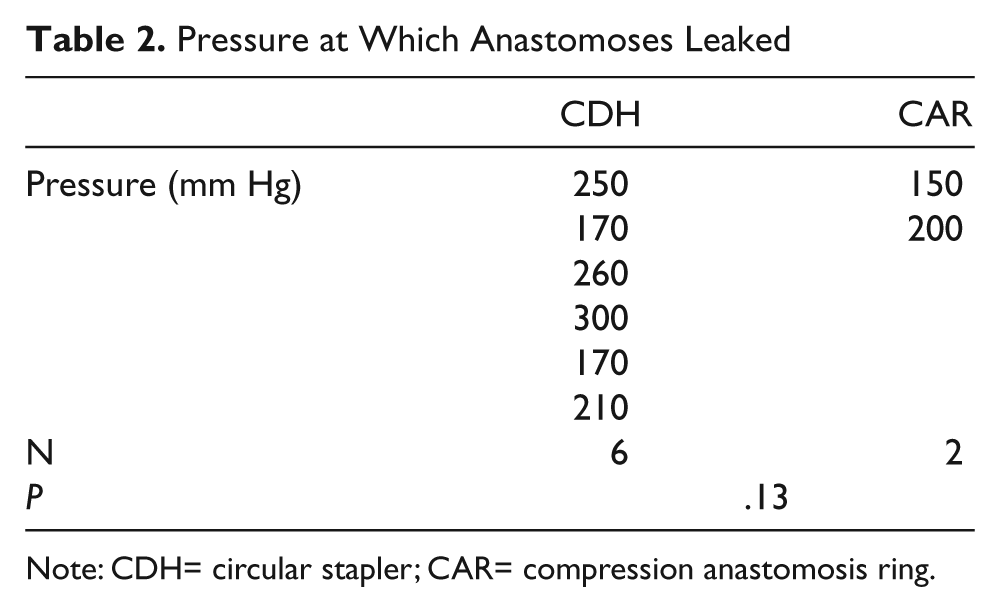
Note: CDH= circular stapler; CAR= compression anastomosis ring.
Internal Circumference (cm)
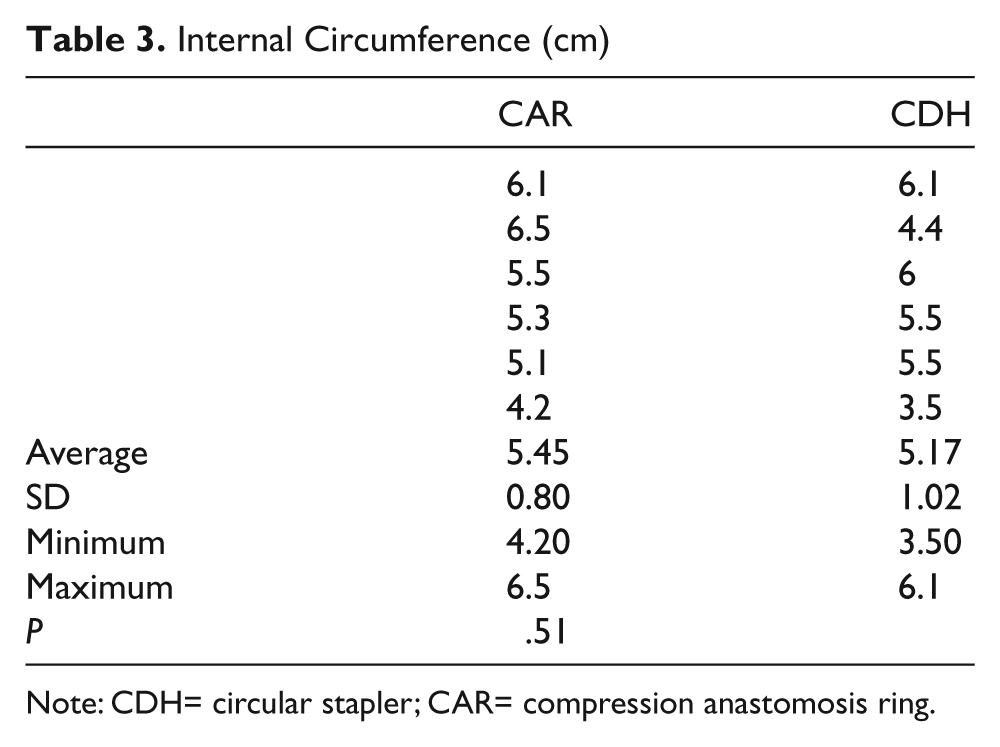
Note: CDH= circular stapler; CAR= compression anastomosis ring.
There was no significant difference in the desmosine (elastin) and hydroxyproline (collagen) levels, as seen in Table 4.
Desmosine and Hydroxyproline Levels
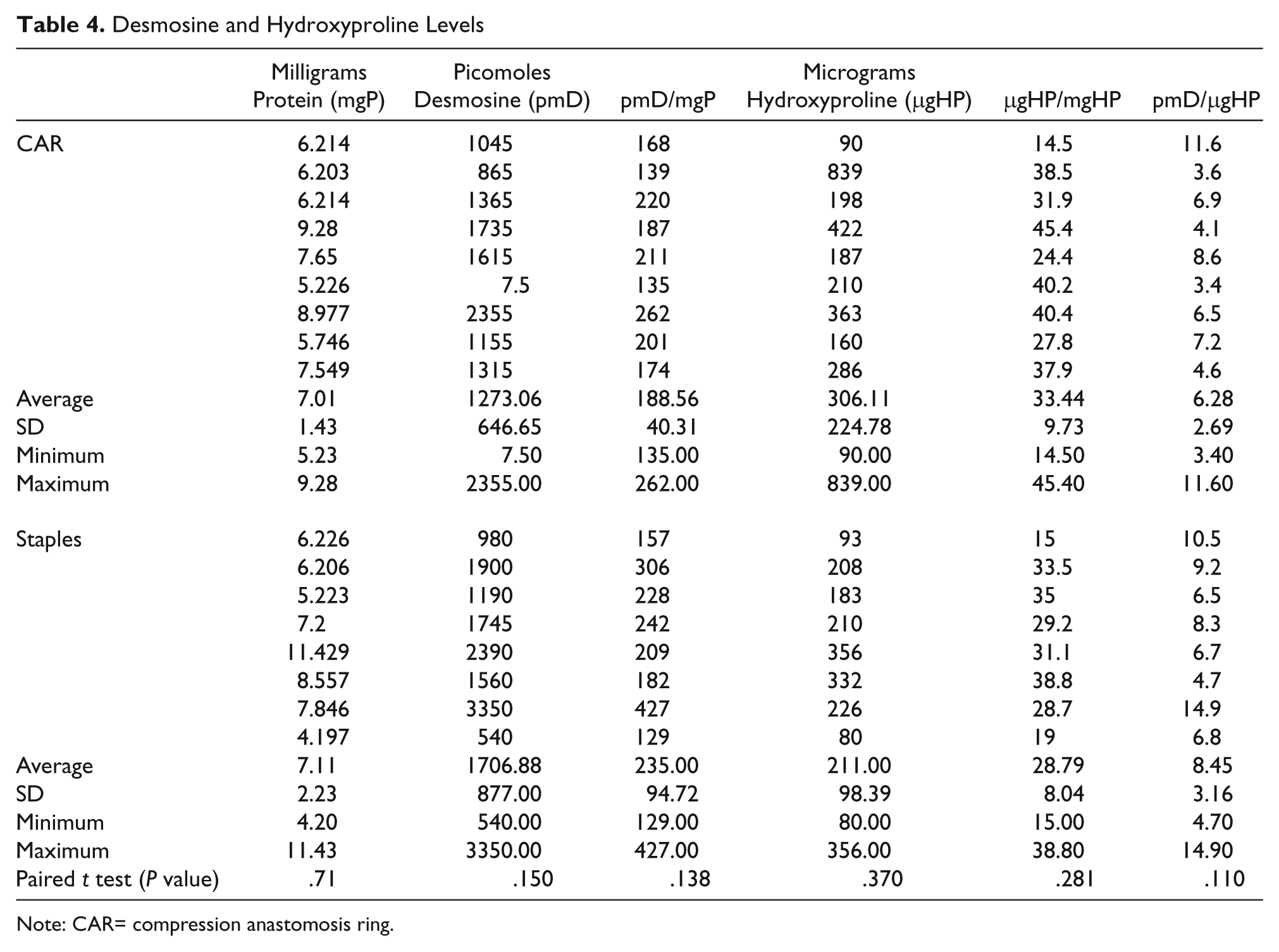
Note: CAR= compression anastomosis ring.
Discussion
Other studies have looked at colonic anastomoses in rats following neoadjuvant chemoradiation, but our search of the literature found no studies looking at its effects on rectal anastomoses in animals, let alone in a large animal model like the pig. Previous work from our institution has shown that compression rectal anastomoses with the EndoCAR in a porcine model had higher early burst strengths than stapled anastomoses, suggesting that the EndoCAR may offer an advantage over the circular stapler in preventing early anastomotic leaks. The 18-pig study by Stewart et al 1 out of our institution showed a mean anastomotic burst pressure of 256 mm Hg for the ring anastomosis versus 250 mm Hg for the stapled anastomosis at 2 weeks. The clinical applicability of this advantage in humans needs to be determined, but our previous work has shown that a trial in humans would be warranted. Failure of the ring to pass and anastomotic leak would be the most significant complications but would be considered short-term complication. Otherwise, the device works like a traditional circular stapler and should not have any different long-term complications. However, before the EndoCAR can truly be considered safe, particularly with regards to surgery for rectal cancer, it must be proven safe in patients following neoadjuvant chemoradiation. To that end, we designed the previously described model for neoadjuvant chemoradiation in a porcine model.
The main purpose of our study was to show that the EndoCAR compression anastomosis was at least as safe as the circular stapled anastomosis in our model. Given the elevated leak rate in pelvic anastomoses in general and particularly following chemoradiation, a device that could offer protection against leaks would certainly be attractive. In addition, the possibility of fewer adhesions would seem to offer the possibility of a decreased incidence of bowel obstructions and/or complications should reoperation become necessary at any point in time. Further studies in humans would be needed to see if those theoretical benefits were real ones, and delineation of those benefits was beyond the scope of this study. The results of our burst pressure testing showed no statistically significant difference between the stapled and compression anastomoses. Our analysis was further strengthened by placing a stapled and compression anastomosis in each pig, so that each animal acted as its own internal control. Furthermore, our results in this chemoradiation model were consistent with previous data from our institution which showed no statistically significant difference in burst pressures at 2 weeks. The trend toward higher burst pressures with the proximal anastomoses was likely more coincidence than anything else. It is our feeling that this trend would likely not hold up over time if there were more animals included in the study. Specifically, there should not be any devascularization of the distal colon or rectum. We performed no mobilization of the bowel, and no vessels were ligated during the course of the operation. It is unlikely that Laplace’s law applies since the porcine rectum does not vary in diameter along its intra-abdominal portion. We did not measure the diameter differences between the proximal and distal anastomotic sites.
Our data also indicates that there is no statistically significant difference in the internal circumference between the stapled and compression anastomoses, as seen in Table 3. Whereas there was some narrowing shown in the compression anastomoses seen at 2 weeks in the study by Stewart et al, 1 we did not show a difference in our model. Our smaller sample size may account for that difference. There was no difference in collagen or elastin levels. We did not have “normal” values for collagen and elastin levels, per se. We were simply using the levels on a comparative basis to see if there was any difference in the anastomoses using the 2 different techniques.
There are limitations to our model. The dosing schedule we used was based on a suggested dosing schedule from the NCCN where chemotherapy was infused for 4 days during weeks 1 and 5 of radiation therapy. Because of the practical considerations and logistics involved in transporting the animals to the radiation facility that many times, as well as the difficulties in housing them for that long a period of time, even before surgery, we opted for the previously described regimen. Although a single dose of radiation could not be completely equivalent to the dosing of the NCCN guidelines, previous studies had shown our chosen dose was within a range which had been shown to cause radiation changes in the intestines of dogs.
Conclusion
Before the compression anastomosis technique using the EndoCAR can truly gain widespread acceptance for colorectal anastomoses, it must be tested in patients who have undergone neoadjuvant chemoradiation. Previously noted potential benefits, such as protection against early anastomotic leaks, fewer adhesions, and long-term narrowing have been suggested as a result of our studies in a porcine model. Our results in a neoadjuvant chemoradiation porcine model suggest that further studies in human patients, including those being treated for rectal cancer, are warranted.
Footnotes
The authors declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The authors disclosed receipt of the following financial support for the research and/or authorship of this article:
This study was funded by research grants from NiTi and Washington University Institute of Minimally Invasive Surgery.