
Abstract
Background. Single-incision laparoscopic cholecystectomy (SILC) is a promising technique with regard to reducing postoperative pain, decreasing complications, and improving cosmesis. Many instruments have been invented to overcome the limitation brought about by the chopstick effect, most of which are inflexible. This results in a limitation when the operator wants to move the tip of the instrument to a certain angle. Recently, the authors used a new instrument, which has 2 simultaneously movable wrists, in 30 cases of SILC. Methods. From May 2010 to August 2010, 30 patients with symptomatic gallbladder disease underwent SILC through a 15- to 20-mm umbilical incision using a 3-trocar technique. A novel laparoscope instrument with adjustable and rotatable wrists (Liuyedao, Inc, Yuyao,China) was applied, combined with the use of harmonic scalpel. Results. The mean operation time was 56.4 minutes (range = 26-170 minutes). The mean estimated blood loss was 16.6 mL (range = 5-60 mL). There were no conversions of the SILC technique. No drainage was placed, and no bleeding or bile leakage occurred. The mean hospital stay was 3 days (range = 1-5 days). Conclusions. The SILC technique with the novel instrument is safe, feasible, and effective. This new instrument facilitates the SILC procedure.
Keywords
With the continued evolution of laparoscopic minimally invasive surgery, changes continue to occur in well-established laparoscopic techniques, targeting at increased facilitation for laparoscopic operations. Since the first reported cases of single-incision laparoscopic cholecystectomy (SILC) published in 1997, 1 attempts have been made to illuminate the disadvantages brought by the loss of the operative triangle and instrumental conflicts. However, instrumental development has lagged behind the innovations made in surgical techniques in SILC.
Most of the reports regarding SILC have been emphasizing on its feasibility and safety; also, several specifically designed ports were introduced, such as the application of curved laparoscopic instruments.2-6 Except for the above-mentioned innovations, specifically designed laparoscopic instruments for SILC are rarely reported. In this study, we report our initial experience of SILC using a novel laparoscopic instrument with an adjustable and rotatable wrist in 30 patients.
Patients and Methods
From May 2010 to August 2010, 30 patients underwent cholecystectomy via SILC. Most of our patients were female (female-to-male ratio = 25:5), with an average age of 29.8 years (range = 21-38 years). The mean body mass index was 19.98 (range = 15.3-27.6), and 6 of these patients had a history of abdominal surgery (appendectomy, 4; caesarean section, 2; see Table 1).
Patient Characteristics and Operative Data
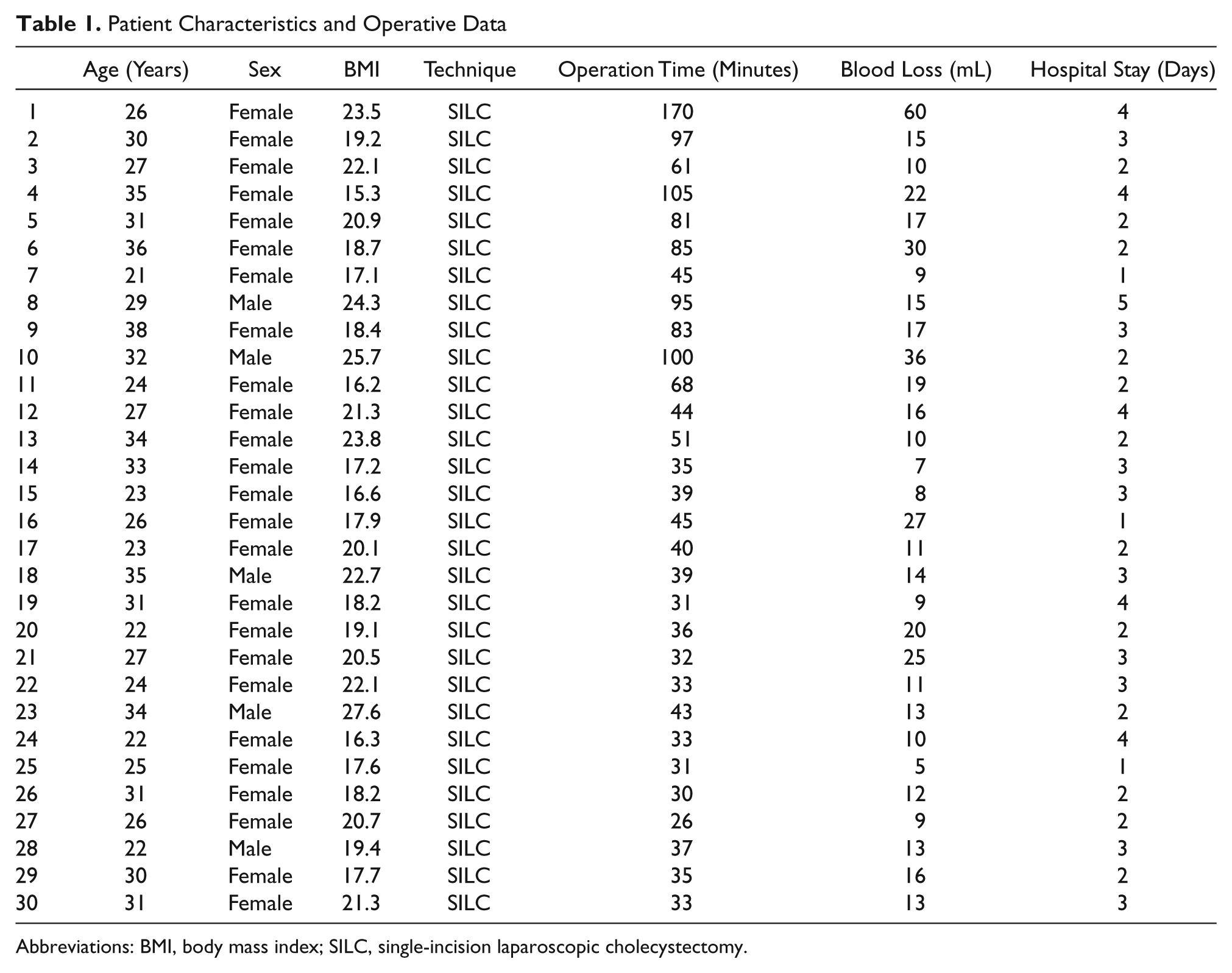
Abbreviations: BMI, body mass index; SILC, single-incision laparoscopic cholecystectomy.
The inclusion criteria were limited mainly to patients with gallbladder stone, polyp of gallbladder, and chronic cholecystitis; those without a history of recent acute onset of cholecystitis; and those with no suspected anatomic abnormality or complicated conditions such as Mirriz syndrome or serious inflammatory exudates, which were found from magnetic resonance cholangiopancreatography and ultrasonography, which were routinely performed in all the patients. Cases with a history of abdominal surgery or complex biliary disease, including biliary pancreatitis, were excluded.
Surgical Technique
Stage 1: Incision, Trocar, and Instrument Placement
A single transumbilical 10-mm incision was made. Pneumoperitoneum was induced with the Veress access needle and maintained at 14 mm Hg with carbon dioxide. A 10-mm trocar then was introduced, and the abdominal cavity was explored with a 10-mm, 30° scope, after which the incision was extended at an angle of 45° laterally and upward at both sides once the decision of SILC was made. The second and third 5-mm trocars were introduced, respectively, to the left and right of the 10-mm trocar, a 5-mm grasper with adjustable and rotatable wrist laparoscopic instrument, and a 5-mm harmonic scalpel. The grasper was placed in the left trocar, the harmonic in the right trocar, and 30° scope was placed in the middle trocar, which formed an inverted triangle.
Stage 2: Exploration, Exposure, Dissection of Calot’s Triangle
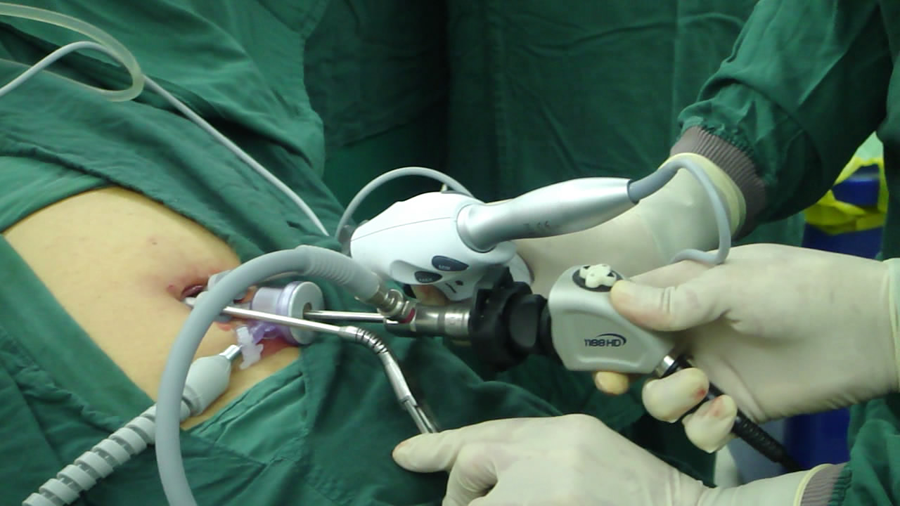
The grasper with adjustable and rotatable wrist laparoscopic instrument (Liuyedao, Inc, Yuyao, China; Figure 1) was used to grasp the bottom of the gallbladder and pull it cephalically, using the syntropic wrist. The flexible wrist was curved downwards to the extent possible manipulating from outside the abdomen, and Calot’s triangle was clearly visualized (Figure 2). Also, with the extraction, tension was formed on the surrounding peritoneum, which facilitated the dissection using a harmonic scalpel. Then Calot’s triangle was explored and cystic duct and cystic artery were exposed (Figure 3).
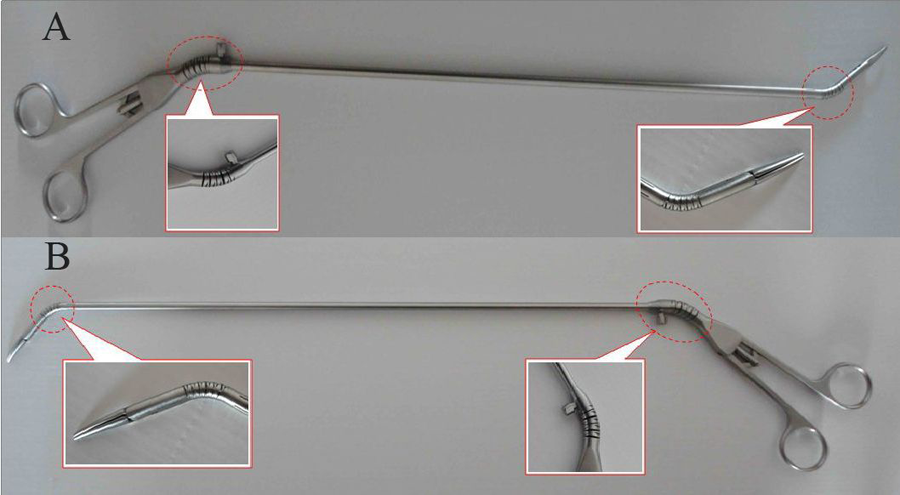
A, Instrument with the syntropic wrist. B, Instrument with the adverse wrist
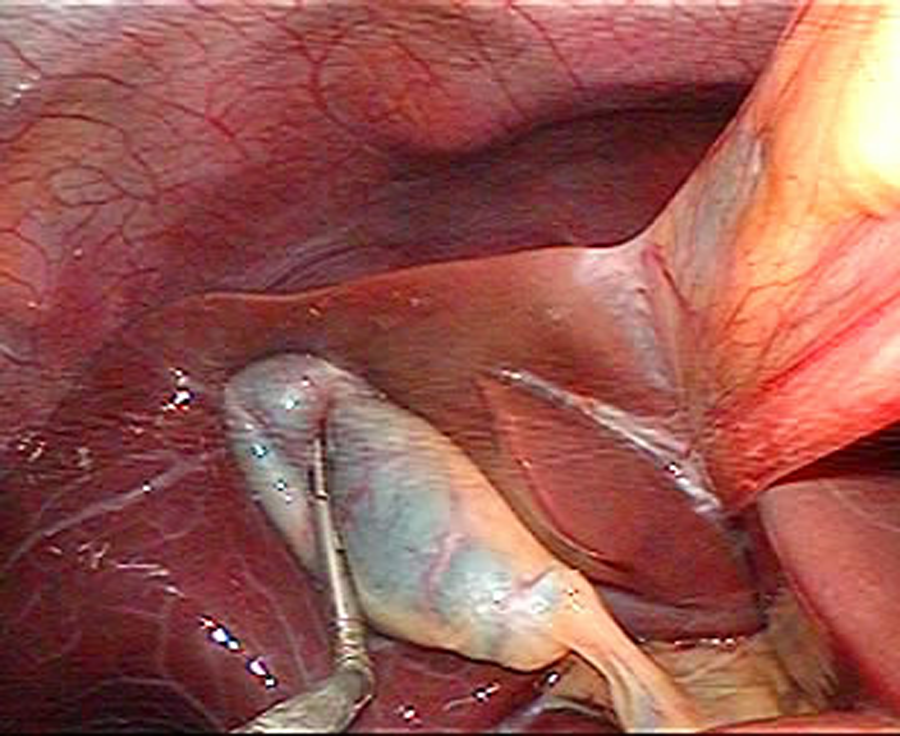
Grasping the bottom of the gallbladder
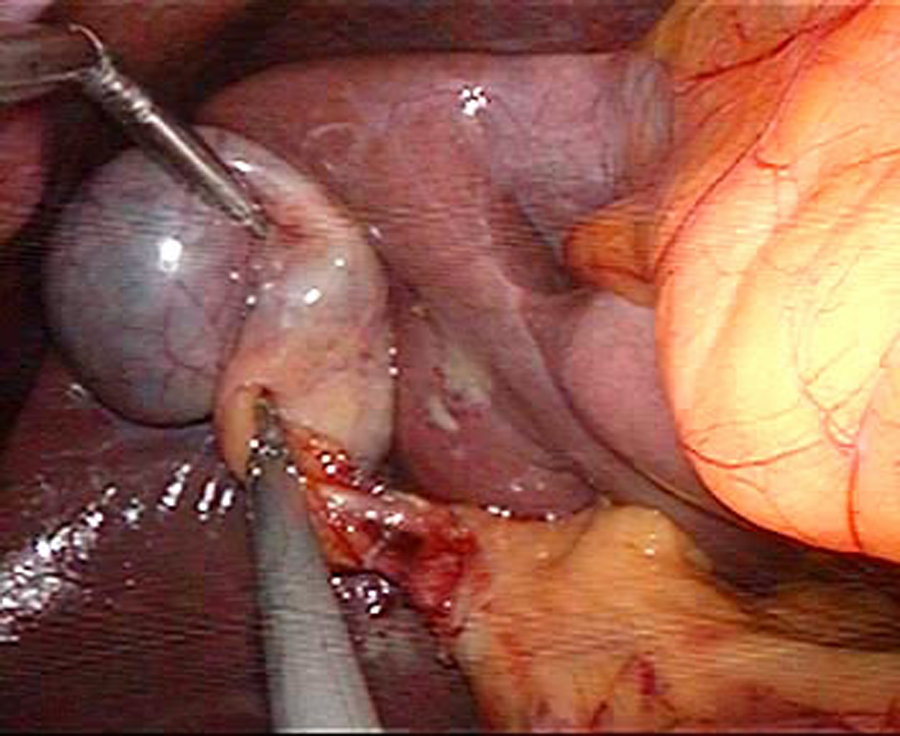
Exposure of Calot’s triangle
Stage 3: Cystic Duct Clipping and Division
Once the cystic duct has been identified and skeletonized, a clip applier was introduced from the right trocar and the cystic duct was clipped with a 10-mm ham-o-lock. Cystic duct and artery were severed using the harmonic scalpel. Dissection was continued using the harmonic scalpel to detach the gallbladder off the liver bed by pulling it laterally or cephalically as needed by manipulating the outside rotatable wrist (Figure 4).
Operation of the instrument wrist outside the abdominal cavity
Stage 4: Hemostasis and Cleanup
The instrument was then curved at its tip to form a maximum angle, to lift the liver lobe for better exposure. Meticulous hemostasis was performed, and the fundus of the gallbladder was reached. Saline irrigation was used to remove any blood or spilled bile before extracting the gallbladder. No drainage was left in place.
Stage 5: Specimen Extraction and Wound Closure
The gallbladder was then put into a plastic sample bag that was inserted and was pulled out through the 10-mm trocar site. The umbilicus incision was closed with an absorbable suture.
Results
All the SILC procedures in this group were performed successfully without conversion to conventional laparoscopic cholecystectomy or the introduction of any additional laparoscopic instruments or trocars. No intraoperative adverse events or major perioperative complications occurred. The mean operation time was 56.4 minutes (range = 26-170 minutes). The mean estimated blood loss was 16.6 mL (range = 5-60 mL). No drainage was placed, and no bleeding or bile leakage occurred. The mean hospital stay was 1-5 days, with a mean of 3 days. All the patients were followed up for 10 days to 4 months, and no complication such as bleeding, bile leakage, and wound infection occurred.
Discussion
The advantages of SILC include ideal scarless and cosmetic results, less postoperative pain, and shorter recovery time than with conventional laparoscopic cholecystectomy; it can also decrease operative trauma, incidence of portsite hernia, and infection rate of incision while maintaining patient’s safety.7-14 However, the single incision constrains the 3 instruments to only 1 axis, and the conflicts among the instruments restrict the freedom of each single instrument, which is described as “chopstick effect” or “linear effect.” Such inborn disadvantages make it difficult to create the necessary operative triangle within limited space, which is however of vital importance during the exploration of Calot’s triangle during SILC, with the rigid movements of the inflexible instruments hardly meeting the requirements when precise dissection is needed; in addition, the loss of the operative triangle extremely complicates routine procedures such as extraction during dissection. Such disadvantages of SILC account for the cumbersome procedure and excessive operative time, which have been bothering the surgeons who perform SILC.
Many attempts have been made to address the above-mentioned problems, not only on the design of specific ports and camera but also on the instruments.3-8 One typical type of existing instruments is the prebent laparoscopic instrument, which requires the use of crossed-over articulating instruments, and as a result, longer operative times are required for achieving careful and precise dissection and some adjustments in the strategy of exposure, particularly because less strength is applied to tissue than with the standard laparoscopic technique. 2 This study was to verify the validity of an innovative instrument that is different from most existing instruments for SILC. The instrument was primarily designed to overcome the limitation by introducing 2 simultaneously rotatable wrists rather than a fixed curved tip. With its adjustable and rotatable wrist, the new instrument transmits the movements of the surgeon’s wrist simultaneously, including instrument with syntropic and adverse wrist, which is illustrated in Figure 1. When the manipulator wrist (outside the abdomen during operation) curves to a curtain direction, the wrist at the tip will curve to the opposite direction simultaneously as in Figure 1A. While for the reverse direction, the wrist at the tip will be curved toward the same direction, as shown in Figure 1B. According to our initial experience, it solves the above-mentioned problems well. This is the first report on the application of this type of instrument, although it is only about SILC.
The wrist of this instrument has 7 degrees of freedom, which includes in-and-out motion, rotation of the wrist, pitch (up-down), and yaw (left-right) at the instrument’s tip, plus the grip at the tip. This simulates the movement of the human wrist inside the abdomen. The flexible wrist increases the space for movements within the limited operative field and fixed angle caused by the single port and restrains from the other 2 instruments, whereas for inflexible instruments, such disadvantages are technically not solvable. For cholecystectomy, Calot’s triangle locates at a limited space, with the vital structures such as cystic artery and cystic duct passing through; also, there are potentially various anatomic abnormalities, such as right accessory hepatic duct.15-18 A sufficient exposure of Calot’s triangle is important and this is always achieved by retracting the gallbladder more laterally, which is difficult to achieve in SILC because of the “linear effect.” In our experience, this is no longer a problem, we could curve the wrist laterally and cranially to the extent possible by manipulating from outside. Therefore, the cystic artery and cystic duct can be clearly visualized and secured safely. Moreover, the wrist can go in any direction as needed, for example, in complicated cases, when peritoneum covering the cystic artery and cystic duct is thickened due to either edema or adhesion, the wrist can be easily rotated to the left lateral and cranial direction, for the better exposure of the posterior triangle, which is a safe procedure routinely performed in conventional laparoscopic cholecystectomy. In our series, harmonic scalpel has been routinely used for dissection, although it is not considered a routine instrument for laparoscopic cholecystectomy at some centers. The tension created by extracting tissue with the tip of the instrument specifically facilitates the dissection using a harmonic scalpel; nevertheless, such tension is needed when some other instruments are applied also. The conflicts outside the abdomen among instruments are also avoided by manipulating the wrist.
In this study, the mean operation time (56 minutes, range = 26-170 minutes) was longer than that of the conventional laparoscopic cholecystectomy done by a single surgeon (30 minutes on average). Specifically, the operation time decreased considerably with experience in applying this new instrument. The first case took us as long as 170 minutes; for the next 29 cases, the mean operation time was 50 minutes (range = 26-105 minutes). For the last 10 cases, mean operation time was stabilized at an average of 34 minutes.
Despite the above-mentioned advantages for facilitating SILC, this new instrument is incomplete from our single-center experience: the absence of fine-scale maneuverability of the wrist comprising precise and steady manipulation and the lack of electric coagulation and cutting function greatly influences its efficacy.
In our study, we concluded that SILC is a feasible, safe, and reproducible technique with this new instrument. Though large-sample data and long-term follow-up are needed to verify its validity and safety, this new instrument might be potentially more helpful in SILC with further improvement.
Footnotes
Heliang Yin and Zhifei Wang contributed equally to this work and should be considered joint first author.
The author(s) declared no potential conflicts of interests with respect to the authorship and/or publication of this article.
The author(s) received no financial support for the research and/or authorship of this article.