
Abstract
The objective was to introduce a new system for transvaginal removal of ovarian cyst and to evaluate its feasibility. With a new transvaginal system, ultrasound-assisted culdotomy, and laparoscopy supported cystectomy if vaginal procedure failed. The authors conducted a retrospective review in which 35 cases using new vaginal ovarian cystectomy were compared with 40 cases of laparoscopic cystectomy for the treatment of dermoid cyst. All cystectomies were completed without conversion to laparotomy and complications. In a case from vaginal group, laparoscopy was required. No differences existed in operating time, hemoglobin decrease, and C-reactive protein value between groups. Laparoscopically supported vaginal ovarian cystectomy with ultrasound-guided culdotomy was equivalent to laparoscopic cystectomy as to invasiveness and preserved the option of a completely vaginal approach. When a presumed benign dermoid cyst is located in cul-de-sac, this operation may represent a preferable alternative to an exclusively laparoscopic or exclusively vaginal ovarian cystectomy.
Introduction
Abdominal surgery has traditionally required an abdominal wall incision and this dermal incision is one of the most important determinants of invasiveness. Pain, scarring, and complications, including hernia formation and adhesions are associated with the incision size. 1 Although the use of laparoscopy has contributed significantly to an improvement in these shortcomings by reducing the size of the incisions, laparoscopy still possesses similar complications as laparotomy.2-4
Recently, natural orifice translumenal endoscopic surgery (NOTES) has become an area of great interest.1,5-9 In NOTES, natural orifices such as the mouth, anus, urethra, and vagina are used as ports of entry into the peritoneal cavity through which flexible or rigid endoscopic devices are passed. NOTES is still in the early stages of development but is expected to prove superior to laparoscopic surgery with regard to invasiveness, as incisions in the abdominal wall are eliminated. Among natural orifices, the transvaginal route is considered to be the most promising for peritoneal cavity access.10-13
The vagina is a unique organ, directly abutting the peritoneal cavity, but showing no visible scars after incision of the vaginal wall.14,15 For more than a century, gynecological surgeons have used the vagina as a route for the removal of intraperitoneal organs. 16 Vaginal hysterectomy is commonly performed by gynecologists and has many advantages over both abdominal hysterectomy and laparoscopically assisted vaginal hysterectomy.17,18 Theoretically, benign ovarian cysts can also be removed vaginally.19,20
Vaginal ovarian cystectomy, however, has failed to gain wide acceptance among gynecologists. In developed countries, most benign ovarian cysts are managed laparoscopically. Vaginal ovarian cystectomy consists of culdotomy and ovarian cystectomy, and each step carries technical difficulties. 21 In culdotomy, the peritoneal cavity cannot be opened without an accurate incision of the vaginal wall toward the cul-de-sac, and a blind incision can sometimes injure the rectum. 22 Even if the culdotomy is performed successfully, intrapelvic adhesions among cysts and uterus sometimes preclude completion of the cystectomy. In such cases, the surgeon must convert to laparotomy. The risk of rectal injury and the uncertainty of success have thus dissuaded most gynecologists from adopting this procedure.
To resolve these problems, we recently proposed new techniques for culdotomy and cystectomy that do not default to laparotomy when unsuccessful. Transvaginal ultrasound was used to identify a safe route into the cul-de-sac and this culdotomy procedure showed a high success rate.10,23,24 In addition, to remove the dependence on laparotomy if the vaginal approach failed, we adopted a system in which a laparoscopic system was available if needed. 25
The less-invasive surgery must be pursued continuously after the establishment of minimally invasive surgery by laparoscopy. Vaginal surgery has the benefit of no incisions in the abdominal wall, compared with laparoscopy. In this study, vaginal ovarian cystectomy using a new culdotomy approach and laparoscopic backup was compared with standard laparoscopic cystectomy in women with a dermoid cyst. The purpose of this study was to evaluate the feasibility of the newly presented vaginal ovarian cystectomy.
Materials and Methods
The diagnosis of dermoid cyst was determined by preoperative transvaginal ultrasonography.26,27 The indications for cystectomy were that the dermoid cysts were presumed benign and the premenopausal women wished to preserve the ovaries. In the majority of cases, magnetic resonance imaging was used to distinguish benign dermoid cyst from dermoid cyst with malignant transformation or other ovarian tumors, including malignancies. Dermoid cysts with serum squamous cell carcinoma antigen levels outside the normal range were excluded from the indications for cystectomy, due to the possibility of malignant transformation.28-30 Dermoid cysts with α-fetoprotein levels outside the normal range were also excluded because of the possibility of being immature. 31
For the treatment of presumed benign dermoid cysts, 93 women had undergone ovarian cystectomy between January 2004 and September 2009 at Kanazawa University Hospital or at Sagawa Clinic. Of these 93 women, we identified 75 women with a unilateral cyst located in the cul-de-sac. The remaining 18 women had either bilateral cysts or unilateral cyst located in the vesico-uterine fossa. A transvaginal approach using culdotomy was applied in 35 of these women, and a standard laparoscopic method was used in the remaining 40 women.
The vaginal approach for cystectomy was explained to the women by 2 gynecological surgeons. During the study period, 42 women with unilateral dermoid cyst in the cul-de-sac were introduced to these 2 surgeons. After excluding 3 women who were still virgins, 39 women received explanations of not only the laparoscopic method but also the transvaginal approach to removing the cyst. In total, 35 of the 39 women wished to undergo transvaginal cystectomy and 4 women elected for laparoscopic cystectomy. As the 3 virgins were treated by laparoscopic cystectomy, 7 of the 42 women were treated using the laparoscopic method. During the same period, 33 women were introduced to another 4 surgeons who were specialists in the laparoscopic surgery and were all treated using the laparoscopic method. In total, 35 women were treated using the transvaginal approach and 40 women were treated using the laparoscopic method.
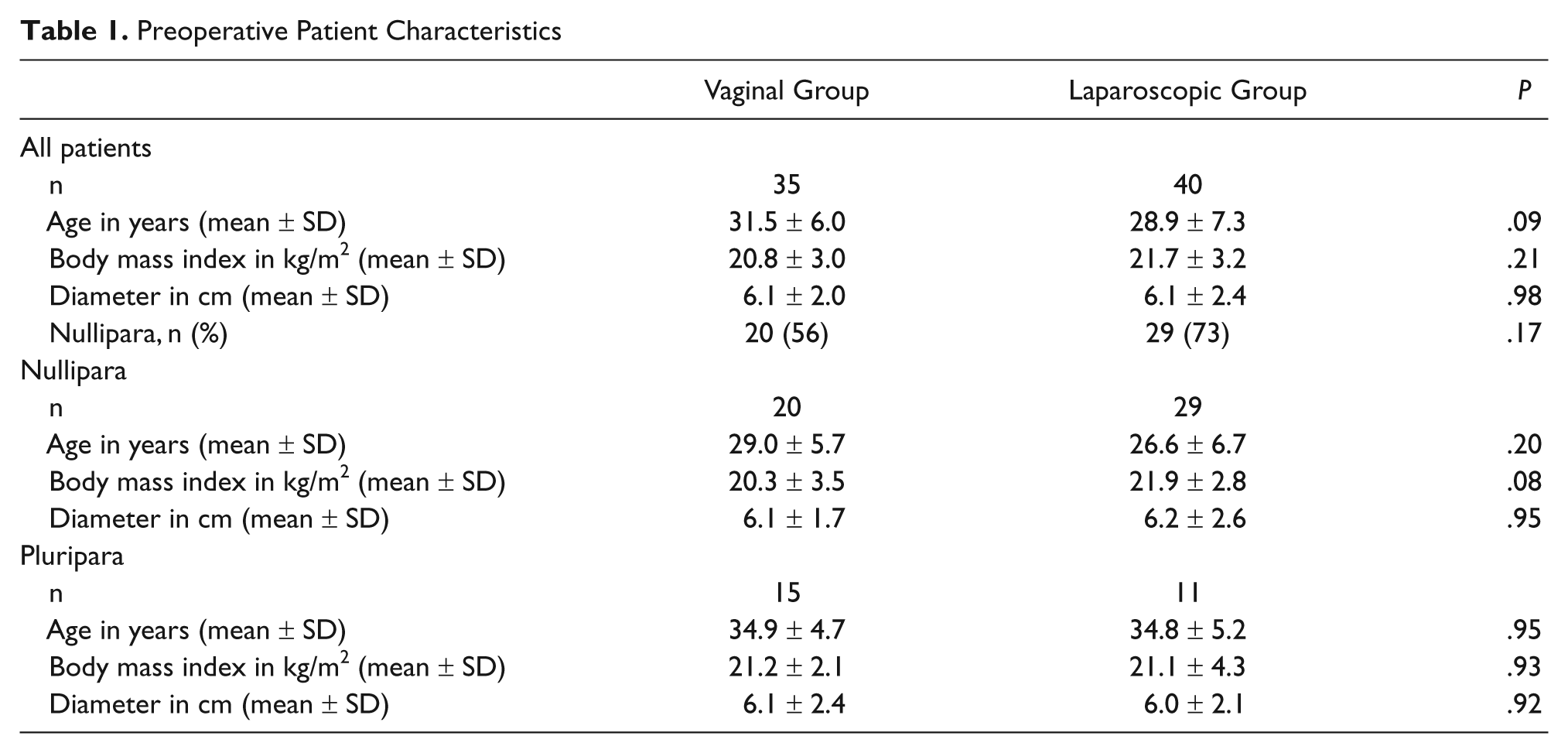
Age, body mass index, parity, and maximum cyst diameter were determined in both vaginal and laparoscopic groups as preoperative characteristics (Table 1). Completion rate, rate of conversion to laparoscopy or laparotomy, intraoperative complications, operating time, hemoglobin decrease on postoperative day 1, C-reactive protein (CRP) level on postoperative day 3, and postoperative complications were examined as intra- and postoperative outcomes and compared between groups (Tables 2 and 3). Estimated blood loss could not be calculated in half of the laparoscopy cases, since the blood was combined with aspirated cyst contents and irrigation. Hemoglobin decrease was therefore used to evaluate blood loss. Hemoglobin value was examined preoperatively and on postoperative day 1, and the decrease was calculated as the difference between these 2 values. CRP increases when infection or inflammation occurs, so we used the CRP level as an indicator of infection, inflammation, and the invasiveness of surgery. Preoperative CRP levels were all below the limit of detection.
Preoperative Patient Characteristics
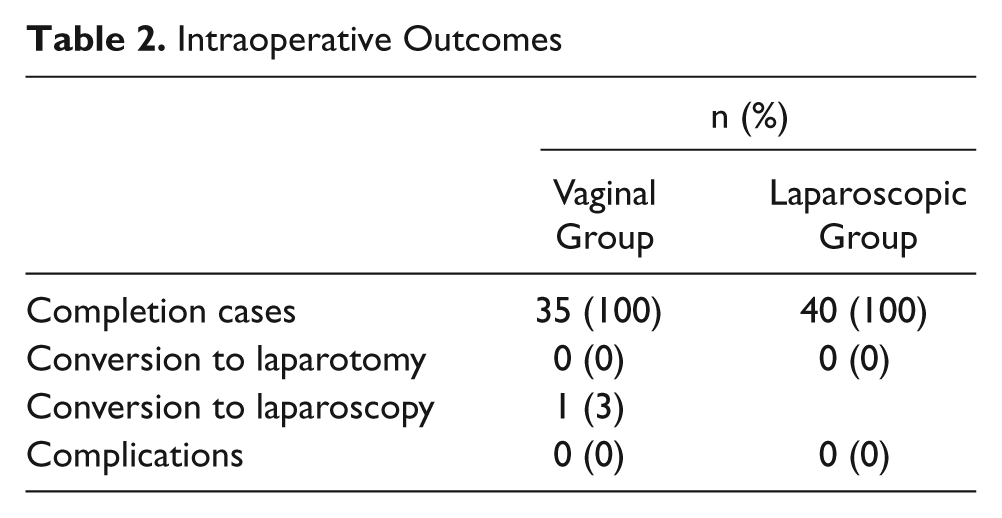
Intraoperative Outcomes
Intra- or Postoperative Outcomes in the Nulliparous and Pluriparous Classes
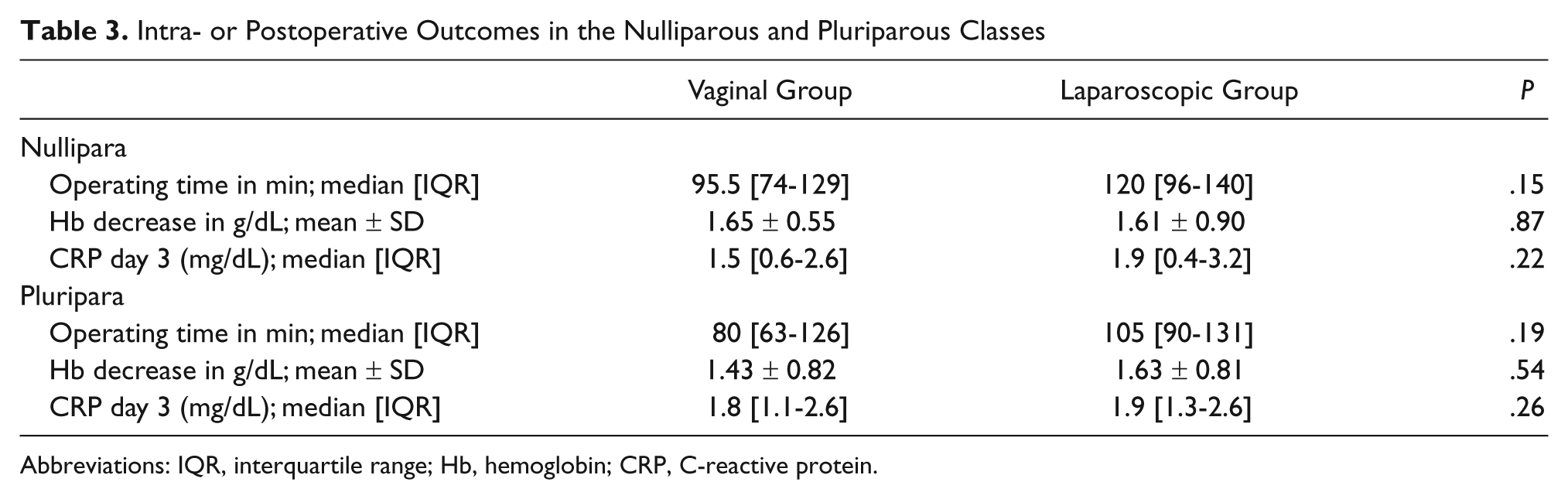
Abbreviations: IQR, interquartile range; Hb, hemoglobin; CRP, C-reactive protein.
Normally distributed data were reported as the mean ± standard deviation, whereas skewed data were reported as the median with interquartile range. To test differences, Student’s t test was used for normally distributed data, whereas Mann–Whitney U test was used for skewed data. Values of P < .05 were considered statistically significant.
Operative Procedure for the Vaginal Approach
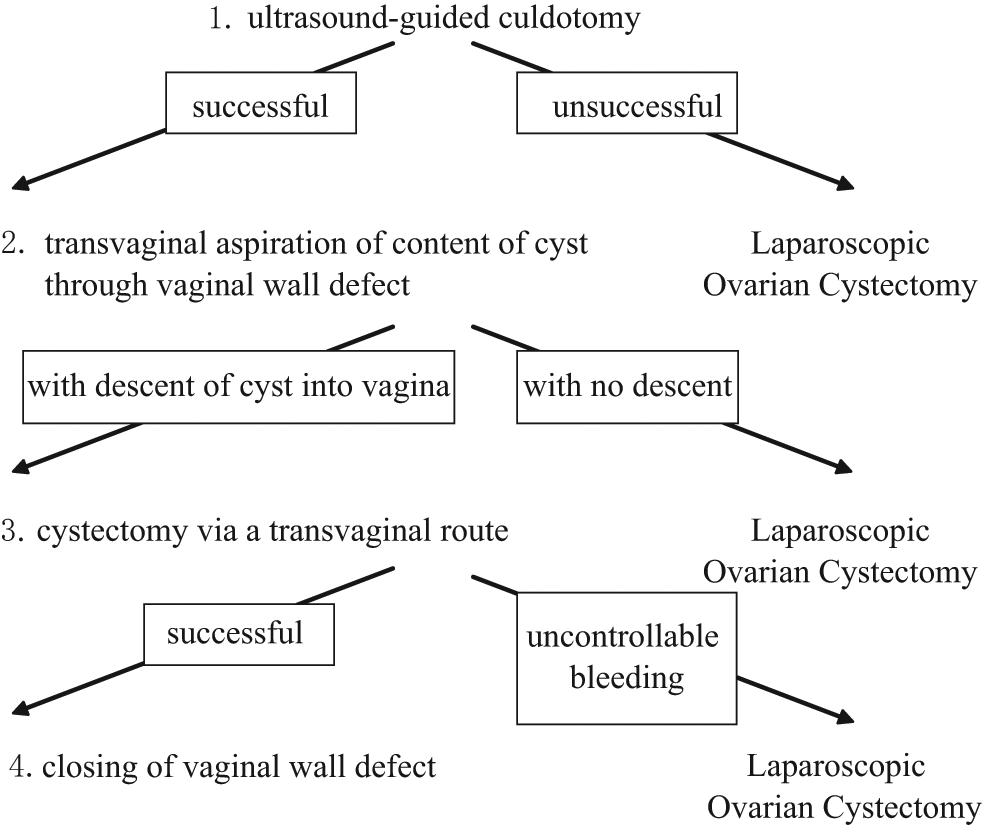
Women were administered enemas on both the day prior to and the day of surgery. Antibiotic prophylaxis was intravenously used on the day of surgery and subsequent 2 days. The operation began transvaginally with the woman in the dorsal lithotomy position on the operating table under general or spinal anaesthesia. Disinfection of vagina was achieved by povidone iodine. Culdotomy was completed first, followed by ovarian cystectomy, which was performed through the defect in the vaginal wall (Figure 1).
Procedure of laparoscopically supported vaginal ovarian cystectomy with ultrasound-guided culdotomy
Each culdotomy was assisted by transvaginal ultrasonography. In the first 8 cases, ultrasound and a renal balloon dilator catheter were used for culdotomy. 23 In the last 27 cases, ultrasound and an umbrella Hakko needle was used for culdotomy.10,24 With both methods, transvaginal ultrasonography visualized the safe vaginal area for entry into the cul-de-sac.
In the former group, following centesis to the vaginal wall by the needle under ultrasound guidance, a balloon catheter dilated the route toward the cul-de-sac. 23
In the latter group, an umbrella Hakko needle was a guide for the entry into intraperitoneal cavity.10,24 After a vaginal ultrasound probe with a needle guide was inserted into the vagina, the ovarian cyst was directly punctured under ultrasound guidance with an umbrella Hakko needle via the center of the posterior vaginal fornix (Figures 2A and 2C). Following ultrasonographic confirmation of the placement of the top of the umbrella needle into the cyst, the umbrella portion of the needle was opened (Figure 2B). Following the extraction of the ultrasound probe from the vagina, the needle remained, penetrating the center of the posterior vaginal fornix. While the needle was gently retracted toward the operator’s side, the vaginal walls on both sides of the needle were incised with an electric scalpel (Figure 2D). Following an adequate incision of the vaginal wall, the ovarian cyst wall was visible in the cul-de-sac through the vaginal defect. By enlarging the defect in the vaginal wall with forceps, the culdotomy was completed (Figure 2E). The final size of incision was about 3 cm. This culdotomy procedure was named Culdotomy 2U. 24 In cases in which the ovarian cyst was a short distance from the cul-de-sac, we adopted the Culdotomy 4S2U procedure. 10 In this procedure, saline solution was infused into the intrapelvic cavity from a balloon catheter inserted into the uterus via the fallopian tubes and an artificially developed saline solution space in the cul-de-sac was punctured by the umbrella needle under the guidance of transvaginal ultrasound (Figure 2C). After successful culdotomy, the ovarian cyst wall was visible in the cul-de-sac.
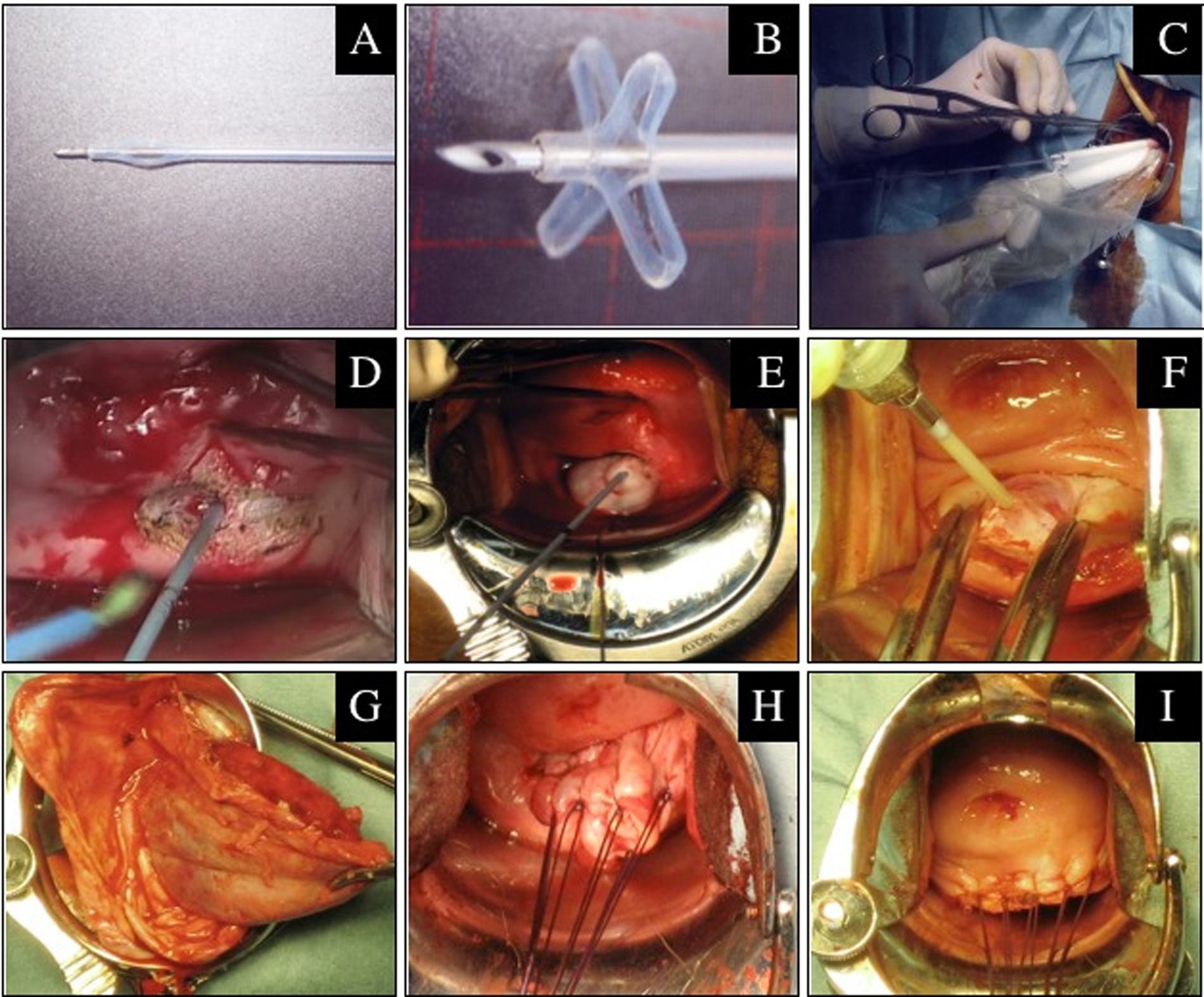
The procedure of vaginal ovarian cystectomy
The ovarian cyst was then partially exteriorized through the vaginal wall defect toward the side of the operator. The cyst contents were then aspirated with another needle to reduce the volume and permit further exteriorization (Figure 2F). If the dermoid cyst had too many solid components or the cyst fluid was too viscous for drainage, cyst contents were removed by enlarging the culdotomy. Any cyst contents that spilled into the peritoneum were carefully aspirated and wiped away. After the partial descent of the cyst into the vagina, transvaginal ovarian cystectomy was performed in a manner similar to that of the procedure for laparotomy (Figure 2G). Perfect resection of cyst wall was confirmed by no rupture and round shape of the removed cyst wall bottom. Following hemostasis and repair of the remaining ovarian tissue (Figure 2H), the defect in the vaginal wall was closed with sutures transvaginally (Figure 2I).
If vaginal ovarian cystectomy was impossible because of failed culdotomy or no descent of cyst into the vagina secondary to intrapelvic adhesions or in the event of uncontrolled bleeding, cystectomy was completed by laparoscopy (Figure 1). 25 Laparoscopic ovarian cystectomy was performed using a standard laparoscopic procedure. After removal of the resected surgical specimen via the vagina, the vaginal defect was closed transvaginally.
The umbrella Hakko needle is a newly developed device that has not yet been approved for medical use.10,24 The Kanazawa University Hospital Ethics Committee and Institutional Review Board authorized experimental use of this device in vaginal ovarian cystectomy. A full explanation of the device was provided to the women, all of whom provided informed consent prior to participating in the study.
Laparoscopy Operative Procedure
Gas laparoscopy was performed in all laparoscopic cases. The woman was placed in the dorsal lithotomy position on the operating table under general anesthesia and the first trocar was inserted from below the umbilicus into the intraperitoneal cavity using the open method. Following visualization of the intraperitoneal cavity with the scope, 2 additional ports were inserted. A uterine manipulating device was used to move the uterus in all women except those who were virgins. In most cases, cystectomy was completed intra-abdominally. In some cases, the cyst contents were aspirated intra-abdominally and the cyst was removed extra-abdominally. Following hemostasis with bipolar forceps and irrigation of the intraperitoneal cavity, the laparoscopic procedure was finished with suturing of the port wounds.
Results
Age, body mass index, parity, and cyst diameter were compared between the vaginal and laparoscopic groups as preoperative patient characteristics (Table 1). No significant differences were noted between groups, although the vaginal group tended to show higher mean age and fewer nulliparous women compared with the laparoscopic group.
All cases were divided into nulliparous and pluriparous classes. In each class, age, body mass index, and cyst diameter were compared between vaginal and laparoscopic groups (Table 1). In the nulliparous class, mean age tended to be higher and body mass index tended to be lower in the vaginal group, but these differences were not significant. In the pluriparous class, no differences were apparent between groups.
All cystectomies in both vaginal and laparoscopic groups were completed without conversion to laparotomy. Laparoscopy was required to complete the cystectomy in a case from the vaginal group because of uncontrolled bleeding. No major intraoperative complications, including rectal injury, were encountered in either group (Table 2).
Operating time, hemoglobin decrease on postoperative day 1, and CRP level on postoperative day 3 were compared between groups, in the nulliparous and pluriparous classes. Hemoglobin decrease is shown as mean ± standard deviation because of the normal distribution, whereas data for operating time and CRP level are shown as median with interquartile range because of the skewed distribution.
Operating time and hemoglobin decrease were compared between groups as intraoperative outcomes (Table 3). Operating time tended to be shorter in the vaginal group than in the laparoscopic group in both nulliparous and pluriparous classes, but the differences were not significant. No significant difference existed between the 2 groups with regard to hemoglobin decrease.
CRP level was compared between groups as postoperative outcomes (Table 3). No difference between groups was identified about CRP level. No severe postoperative complications or cases of malignancy were identified in either group.
Discussion
Vaginal ovarian cystectomy requires no incisions into the abdomen. If completed successfully, the procedure may be less invasive than laparoscopy. 32 The conventional transvaginal approach, however, is not always successful and is often difficult. 21 A restrictive surgical field, lack of confidence in performing the culdotomy, difficulty in observing and irrigating intraperitoneal cavity, and a reluctance to convert to laparotomy in unsuccessful cases are factors that have dissuaded most gynecologists from adopting this procedure. We have proposed 2 solutions to overcome some of these shortcomings.10,23-25 The first is a new culdotomy technique and the other is support by laparoscopy. Our modifications have evolved into laparoscopically supported vaginal ovarian cystectomy with ultrasound-guided culdotomy. We therefore compared this new system of vaginal ovarian cystectomy with standard laparoscopic cystectomy.
To avoid sampling bias between the 2 groups, we gave thought to the following points. The histological type of ovarian cysts was limited to dermoid cysts. Operative procedure was limited to cystectomy only. Bilateral cysts were excluded and the object of surgery was restricted to unilateral cyst located in the cul-de-sac. Eligible cases were selected from the same facilities within the same period.
Analysis of preoperative patient characteristics revealed fewer nulliparous women in the vaginal group, compared to the laparoscopic group (Table 1). Women were required to be nonvirginal for employment of the transvaginal route. As a result, 3 women who were virgins were intentionally assigned to the laparoscopic group. Of the 4 women who desired laparoscopic operation after explanation of the transvaginal method, 3 were nulliparous by chance. If they had been included in the vaginal group, there would have been more nulliparous women in the vaginal group. Bias of parity may have influenced operative outcomes, as the transvaginal procedure may be easier in pluriparous women compared with nulliparous women. We thus divided cases into nulliparous and pluriparous classes for analysis.
Analysis of preoperative patient characteristics in the nulliparous class showed a tendency toward older age and lower body mass index in the vaginal group, although these differences were not significant (Table 1). The absence of virgins seems likely to have increased the mean age in the vaginal group. We do not know why body mass index was lower in the vaginal group.
All culdotomies were achieved successfully with ultrasound-guided methods in the vaginal group. In the last 27 of the 35 cases, the latest culdotomy procedures were adopted.10,24 Transvaginal ultrasonography visualized the safe vaginal area for entry into the cul-de-sac and a newly developed umbrella Hakko needle guided the correct incision of the vaginal wall. This method was simple and the operating time for culdotomy was short. We believe that each successful culdotomy was because of this technique.
No cases showed poor descent of the cyst to the vagina and resultant conversion to laparoscopy. This finding suggests that adhesions are rare and removal of a cyst wall through the vaginal wound is possible in the majority of cases of dermoid cyst. In one case, laparoscopy was required because of uncontrolled bleeding from remaining ovarian tissue. In our system, laparoscopy guarantees completion of the operation whenever the transvaginal procedure fails, thus sparing the woman a highly invasive procedure. In this sense, our system worked well. 25
Some gynecologists may claim that laparoscopically supported vaginal ovarian cystectomy is not an operative method, as the laparoscopy is not always used and the procedure differs among cases. Allowing for this point, we consider our method as a system. There is merit to recognizing transvaginal cystectomy with backup laparoscopy as a definite operation system. Traditional vaginal cystectomy without laparoscopic support must sometimes be converted to laparotomy and has thus failed to gain wide support from both surgeons and patients. Recognition of our method as an operative system could lead to a dramatic effect on vaginal ovarian cystectomy. Gynecologists would be able to confidently recommend a vaginal approach to women. Women would be more likely to accept a vaginal approach if a minimally invasive procedure is more certain. Vaginal ovarian cystectomy combined with laparoscopic support should be recognized as a new operative system.
In terms of operating time, hemoglobin decrease, and CRP level, no differences existed between groups. These findings suggest that cystectomy via a vaginal route is comparable to laparoscopic cystectomy in terms of invasiveness.
Although no intra- or postoperative complications were apparent in the vaginal group, infertility and dyspareunia over the long term must be evaluated. According to a questionnaire about transvaginal NOTES to gynecologists, infertility and dyspareunia after the operation remain matters of concern. 33 We are now addressing these questions with a questionnaire to women undergoing vaginal ovarian cystectomy.
We must take into consideration the influences of intraperitoneal spillage of cyst contents. When performing ovarian cystectomy, either laparoscopically or transvaginally, avoiding intraperitoneal spillage in all cases is not feasible.34,35 Preoperative minimization of the possibility of ovarian malignancy is thus imperative.26,27,36 Meticulous preoperative studies, including ultrasound, magnetic resonance imaging, and tumor marker levels are essential to exclude all cases of possible malignancy.26-31 In some cases in which preoperative examinations do not perfectly rule out the possibility of malignancy, laparoscopy should be selected because laparoscopic inspection may be useful to find stage I-c ovarian malignancy.
Chemical inflammation after intraperitoneal spillage must also be avoided. CRP level of the vaginal group was statistically equal to that of the laparoscopic group. This result suggests that intraperitoneal spillage in the vaginal group was minimal and chemical inflammation did not occur. However, the degree of intraperitoneal spillage should be estimated using a different method. Currently, we perform intraperitoneal observation with a flexible endoscope via a vaginal wound during vaginal ovarian cystectomy. Using this scope, the pelvic cavity can not only be observed but also irrigated. This method may thus become useful as a routine procedure for vaginal ovarian cystectomy.
We named the new vaginal ovarian cystectomy using ultrasound and an umbrella needle, as applied in the last 27 cases, “laparoscopically supported vaginal ovarian cystectomy with the assistance of ultrasound and an umbrella needle “ (LSVOC2U). Our system showed a reliable profile comparable to conventional laparoscopy for the treatment of dermoid cyst located in the cul-de-sac. If the woman desires a minimally invasive, scarless surgery, this method may be the preferred alternative to an exclusively laparoscopic or exclusively vaginal ovarian cystectomy.
Footnotes
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author received no financial support for the research, authorship, and/or publication of this article.