
Abstract
Background. This study was designed to evaluate the effects of ethyl pyruvate (EP) on wound healing in primary colonic anastomoses in intraperitoneal sepsis. Methods. Standard left colon resection and end-to-end anastomosis were performed on 30 rats. They were grouped as control (C)—no further treatment; sepsis (S)—received 2 mL Escherichia coli (ATCC 25922) intraperitoneally (IP), and after 5 hours, standard resection and anastomosis were performed; or sepsis-group treated with EP (S-EP)—received 2 mL E coli IP, after 5 hours, standard resection and anastomosis were performed and treated with EP 50 mg/kg IP for 7 days. On the postoperative day 7, the animals were sacrificed. Results. The anastomosis bursting pressure in group S was significantly lower than in the other groups. There were no differences between groups C and S-EP. Tissue hydroxyproline concentrations in group C were significantly higher than in group S. Conclusions. EP administration prevented intraperitoneal sepsis-induced impaired anastomotic healing of colon.
Keywords
The presence of established intra-abdominal sepsis has been considered a contraindication to primary anastomosis. 1 However, the relationship between the intra-abdominal sepsis and colonic anastomotic wound healing would be important in some clinical situations, such as colonic perforation caused by perforated diverticulitis, colonic cancer, or abdominal penetrating trauma. It has been shown that the healing of colonic anastomoses is adversely affected by infection in the peritoneum.2,3 Currently, there is great interest in the safety and applicability of early definitive operative treatment of colonic anastomoses for patients with intra-abdominal sepsis. Strategies to prevent the systemic effects of sepsis-induced organ injury using anti-inflammatory agents have continued to be attractive subject for investigators.
Ethyl pyruvate (EP), a simple aliphatic ester derived from pyruvic acid, has been shown to be an effective anti-inflammatory agent in a variety of in vivo and in vitro model systems. 4 Acute administration of EP has been shown to improve survival and/or ameliorate organ damage or dysfunction in animal models of hemorrhagic shock,5,6 endotoxic shock,7,8 bacterial peritonitis, 9 and ethanol-induced acute liver injury. 10 This study was designed to evaluate the effects of EP on the wound healing process in primary colonic anastomoses in the presence of intra-abdominal sepsis.
Material and Methods
Animals
Wistar rats (200-250 g; n = 30) were fasted for 12 hours, but were allowed free access to water before the experimental protocol. Animals were kept in a controlled enviroment. This study was approved by Animal Use and Care Committee, School of Medicine, Marmara University. Animal care was in compliance with the current European Union regulations (O.J. of E.C.L 358/1, 12/18/1986) on protection of animals used for experimental and other scientific purposes.
Experimental Protocol
Experiments were performed on 30 male Wistar rats (Istanbul, Turkey). The animals were assigned to 3 groups at random: control (C), sepsis(S), or sepsis-group treated with EP (S-EP) at 50 mg/kg body weight intraperitoneally (IP) for 7 days. To induce intraperitoneal infection, 2 mL Eschrichia coli American Tissue Culture Collection (ATCC) number 25922 (108 E coli ATCC 25922/mL, sublethal dose); 11 was injected into the peritoneal cavity 5 hours before surgery to groups S and S-EP. To be included in the study, the animals had to survive the operation.
A standard left colon resection and end-to-end anastomosis were performed on rats. Group C rats received the anastomosis and no further treatment. Group S rats received 2 mL diluted E coli IP, and after 5 hours, a median incision and laparatomy, standard left colon resection, and end-to-end anastomosis were performed. Group S-EP rats received 2 mL diluted E. coli IP, and after 5 hours, a median incision and laparatomy, standard left colon resection, and end-to-end anastomosis were performed. Then group S-EP rats were treated with EP 50 mg/kg body weight IP for 7 days. After a postoperative interval of 7 days, the animals were sacrificed.
Preperation of Bacteria
Escherichia coli ATCC 25922 obtained from Marmara University Medical Faculty Microbiology Labarotory was used. After obtaining the bacteria, it was incubated in triptase soy broth agar. The bacteria isolated from the agar were homogenized by nefelometer as 1 McFarland, diluted with normal saline to 108 E coli/mL (sublethal dose). 11
Materials
Ethyl pyruvate was purchased from Sigma-Aldrich Chemical Co. (Steinheim, Germany).
Surgical Procedure
Intramuscular 35 mg/kg ketamine hydrochloride (Ketalar, Eczacibasi, Istanbul, Turkey) and 5 mg/kg xylazine HCl (Rompun, Bayer, Istanbul, Turkey) were injected to induce anesthesia in all groups. Animals were allowed to breath spontaneously during the surgery. The operation was performed under aseptic conditions. The abdominal wall was shaved, cleaned with 10% povidone-iodine solution and drapped with sterile drapes. Using sterile instruments, laparotomy was performed by midline incision. The distal colon was found, a 1-cm segment of left colon was resected 3 cm proximal to the peritoneal reflection in all animals. The fecal content of anastomotic ends were milked out and standardized end-to-end anastomosis was performed with a single layer interrupted inverting 6/0 polypropylene sutures. The abdomen was closed with continuous sutures of 3/0 silk sutures. All anastomoses were created by the same surgeon. After 24 hours, the animals were allowed to feed. Oral paracetamol (100 mg/kg) was added to the water of rats during the 7-day interval for analgesia before sacrifice. All animals were killed on the seventh day by intracardiac puncture while under anesthesia with high dose intraperitoneal ketamine (75 mg/kg) and xylazine HCl (16 mg/kg) and relaparotomy was done. During the postmortem examination, the anastomoses were examined macroscopically; the integrity of the anastomosis, the existence of perianastomotic abscess or peritonitis, and adhesion formation were recorded. The results were evaluated in a blinded fashion according to the scale of Van der Hamm et al, 12 as follows: 0 = no adhesions; 1 = minimal adhesions, mainly between anastomosis and the omentum; 2 = moderate adhesions, that is, between the omentum and the anastomotic site and between the anastomosis and a loop of the small bowel; and 3 = severe and extensive adhesions, including abscess formation.
Segmentery resection including 2-cm proximal and distal regions to the anastomosis place was performed. Anastomotic strength was measured in vivo by determining the bursting pressure. After bursting, the anastomotic site was resected and used for hydroxyproline measurement.
Measurement of Colonic Bursting Pressure
A 4-cm segment of colon with the anastomosis in the middle was resected. One end of this segment was closed with a ligature, and a catheter was secured to the other end. Inside a glass jar filled with water, air was pumped into the segment of colon at a rate of 2 mL/min with an infusion pump. Intraluminal pressure was monitored while the air was pumped. The intraluminal pressure at which air leakage from the anastomosis occurred, was recorded as the bursting pressure. This parameter showed the mechanical strength of the anastomoses.13-15
Tissue Hydroxyproline Measurement
Hydroxyproline levels were determined with Bergman and Loxley’s method. 16
Statistical Analysis
Descriptive statistics (mean, standard deviation [SD], confidence interval) were first calculated for all study variables. Continuous data are presented as mean ± SD. One way analysis of variance was used to examine the differences of the mean burst pressure and hydroxyproline concentrations between experiment groups. To further evaluate the significance of the differences, post hoc Tukey honestly significant difference and Tamhane analysis were used according to the homogenity of variances of the variables. Error plots were drawn to differentiate significant differences visually. Statistical significance was attributed to P < .05. All analyses were performed on SPSS version 15.0 for Windows (IBM SPSS Inc, Chicago, IL).
Results
All rats became severely ill after inoculation, as characterized by lack of movement, piloerection, and anorexia. Body weight decreased during the first 4 days after operation and stabilized thereafter. No significant differences in survival between sepsis groups were observed.
Intra-abdominal abscesses and adhesions were more frequent in group S (P < .05). Adhesion formation was also more extensive in group S. Three rats in group S developed abscesses. There were no abcess in other groups.
The mean anastomosis bursting pressures are presented in Figure 1. Group comparison showed that anastomosis bursting pressure in group S was significantly lower than in the other groups (P < .05). There were no differences between groups C and S-EP in the mean anastomosis bursting pressures (P > .05).
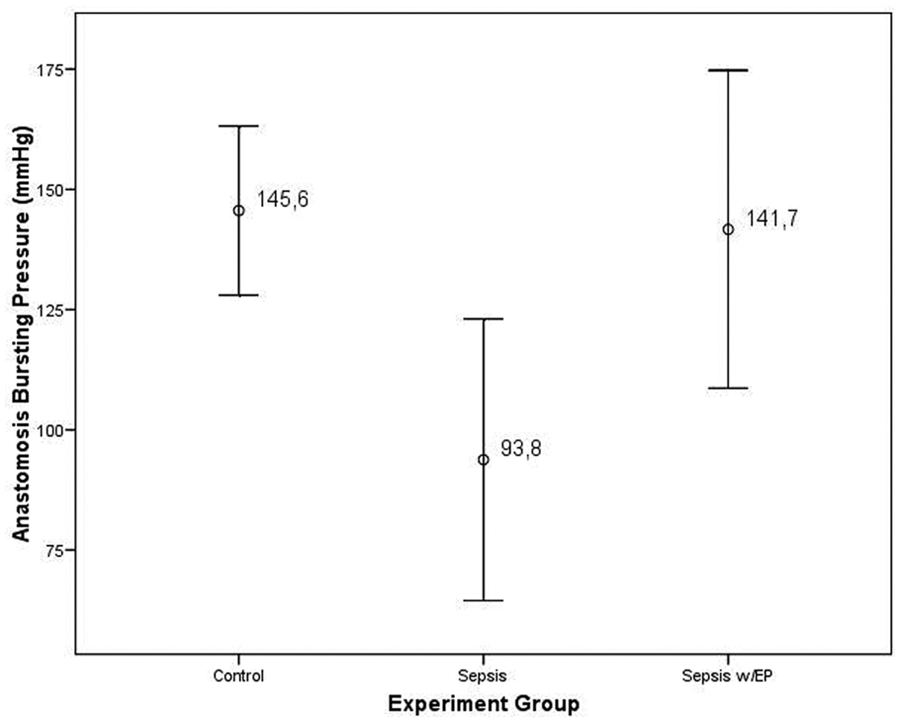
Mean anastomosis bursting pressure in the 3 groups
The mean anastomotic tissue hydroxyproline concentrations are presented in Figure 2. Group comparison showed that tissue hydroxyproline concentrations in group C were significantly higher than in group S (P < .05). There were no differences between group S-EP and other groups in the mean tissue hydroxyproline concentrations (P > .05).
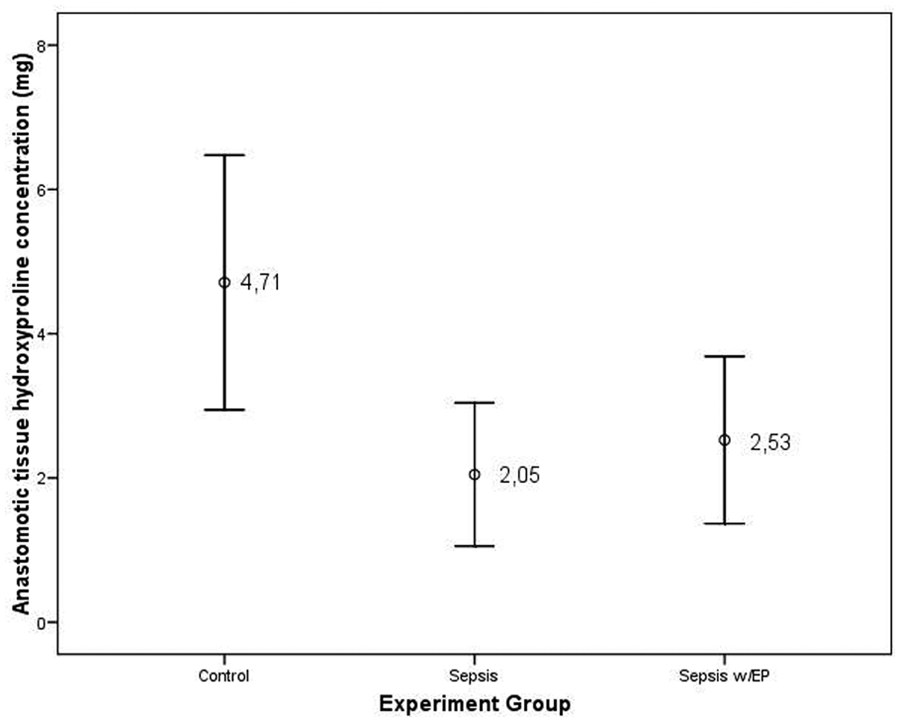
Mean anastomotic tissue hydroxyproline concentration in the 3 groups
Discussion
In the present study, although there were no differences seen among the groups in terms of hydroxyproline levels, higher anastomotic bursting pressures were observed in the S-EP group.
Despite improvements in surgical technique, anastomotic leakage after colorectal surgery continues to be a major clinical problem. Many studies have attempted to elucidate the factors contributing to colonic anastomotic dehiscence. Apart from technical errors, there are several intrinsic characteristics of the colon and regional conditions that increase the likelihood of impaired healing. The presence of established intra-abdominal sepsis has been considered a contraindication to primary anastomoses. It has been shown that the healing of colonic anastomoses is adversely affected by infection in the peritoneum.1,17 Currently, there is great interest in the safety and applicability of early definitive operative treatment of colonic anastomoses for patients with intra-abdominal sepsis.
When an anastomosis is constructed in the gastrointestinal tract, an inflammation occurs as a response to traumatic injury and foreign material such as sutures.17,18 This inflammation is a normal constituent of wound healing. If it is exaggerated, however, wound healing is delayed because of increased collagenolysis; this is why anastomotic healing is delayed in the presence of intra-abdominal infection. 19 The anastomotic area is already inflamed, and the endothelium in the perianastomotic area is already activated during the early phase of wound healing. As a result of proinflammatory and chemoattractant properties of the anastomosis, activated circulating polymorphonuclear leukocytes secondary to sepsis-induced injury may accumulate easily in the perianastomotic area, increase the inflammatory reaction, and delay healing. Together with the proteolytic enzymes, oxygen-free radicals derived from activated polymorphonuclear leukocytes and circulating xanthine oxidase may increase collagenolysis in the perianastomotic area, which delays wound healing. Strategies to prevent the systemic effects of sepsis-induced organ injury using anti-inflammatory agents, including EP, have continued to be an attractive subject for investigators. The precise mechanism of action of EP here is not clear, but is likely because of a combination of anti-inflammatory properties.
Ethyl pyruvate is a more stable aqueous form of pyruvate. Its pharmacological effects are quite diverse and include downregulation of the secretion of pro-inflammatory cytokines, amelioration of redox-mediated damage to cells and tissues, inhibition of apoptosis, and support of cellular ATP synthesis. It is possible that EP inhibits activation of nuclear factor-B (and perhaps other signaling pathways as well) by scavenging reactive oxygen species, since EP, like pyruvate, is an antioxidant. 20 More than 150 articles, which report findings from studies of EP in animal models of human disease, have appeared in the literature. Briefly, acute administration of EP has been shown to improve survival and/or ameliorate organ damage or dysfunction in animal models hemorrhagic shock, endotoxemic shock, bacterial peritonitis, necrotising pancreatitis, hepatic injury, stroke, and cutaneous burn injury.5-9,21,22 But there is no study about EP administration in colonic anastomosis in intraabdominal sepsis.
The present study is the first study that demonstrates that the colonic anastomotic wound healing process improved after administration of EP in the presence of E coli–induced intra-abdominal sepsis. We observed a higher rate of abscesses and more extensive adhesions in the rats in group S. Of course, these are negative factors for anastomotic healing. We believe that the most reliable criteria for assessing the healing of the colonic anastomosis are the macroscopic findings at postmortem examination. However, to have additional criteria, we measured the bursting pressure of the anastomoses and hydroxyproline concentrations.
It was proposed that assessment of the anastomotic healing mainly depends on mechanical parameters, and bursting pressure is particularly of great value. We have shown that EP inhibits the collagen breakdown in the colonic anastomosis and increases the colonic bursting pressure. Bursting pressure and hydroxyproline determinations are measures that offer insight into the anastomosis healing process. Bursting pressure reveals the mechanical parameters of a colonic anastomosis and reflects growing anastomotic strength. The method used in this study for measuring bursting pressure is a validated method and previous studies found that the bursting pressure increases progressively immediately after the formation of a colonic anastomosis. This indicates that it is a useful approach to measure the early changes of healing process during the first week.13-15 Biochemical parameters of anastomotic healing are reflected by the collagen content in the perianastomotic tissues, as determined by hydroxyproline levels of the perianastomotic tissue to determine healing rates. 23 We could not find any difference in terms of hydroxyproline levels, which are indicators of anastomotic healing. This may be because of inhibition of the collagen breakdown in colonic anastomosis by EP. In other studies, it was shown that the strength of anastomosis decreases markedly during the first 3 to 4 days because of the changes in the enzymatic structure of collagen bundles and collagen breakdown. After the fourth day the strength of anastomoses increases with the prominence of collagen production and accumulation. 24
Ethyl pyruvate causes improved anastomotic wound healing and increased bursting pressures in intra-abdominal sepsis. Further studies may elicit the function of EP in anastomotic wound healing in intra-abdominal sepsis.
Conclusion
In this study, although hydroxyproline levels were not affected by EP treatment, the average bursting pressures were found to be increased in anastomoses in the presence of peritonitis. This beneficial effect may be provided by anti-inflammatory effects of EP. As a result, EP treatment has positive effects on colonic anastomotic healing in case of peritonitis.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.