
Abstract
Metanephric adenoma (MA) is a rare benign tumor, diagnosis of which is often carried out after surgical treatment. In case of peripheral lesions, a partial nephrectomy (PN)—either open or laparoscopic may be preferred—and, furthermore, a radiofrequency (RF)-assisted procedure may facilitate adequate hemostasis. In November 2010, the authors performed a RF-assisted PN, according to Habib’s technique, using a 4-needle bipolar device, on a woman affected by a small exophytic MA of the right kidney. Fibrin glue was applied on the cut surface. Postoperative course was uneventful, and discharge was on postoperative day 4. MA is an extremely rare benign tumor with a favorable prognosis. In case of a preoperative cytological diagnosis, a careful follow-up has to be considered. PN represents the standard of care for small exophytic MA, and RF-assisted procedures allow an excellent hemostasis and a rapid conservative resection, with very low morbidity.
Introduction
In 1988, Mostofi et al 1 recognized metanephric adenoma (MA) as a distinct nosologic entity among renal neoplasms, featured with tubular-like epithelium cells. Metanephric adenofibroma is described as a mass constituted by “spindle cells” associated to epithelial cells, whereas the elective presence of stromal cells alone, without the epithelial component, is a typical presentation of metanephric stromal tumor. All of them belong to the common morphological spectrum of metanephric neoplasms. Currently, about 100 cases have been reported in literature, and, despite larger case series, 2 all data are mostly case reports. The widespread use of “nephron-sparing surgery” 3 allows to define partial nephrectomy (PN) as a gold standard, especially for small exophytic benign tumors. We report a case of MA in which a lower right radiofrequency (RF)-assisted PN was performed by means of a 4-needle bipolar device, which allowed for an excellent hemostasis.
Case Report
In November 2010, a 50-year-old woman affected by cholelithiasis came under our observation. An abdominal ultrasonography diagnosed cholelithiasis and hepatic angiomas. A contrast-enhanced abdominal computed tomography scan confirmed liver angiomas and detected, in preenhanced scans, a 20-mm isodense nodule in the lower pole of the right kidney, with hyperdense internal spots, irregularly enhanced in the delayed phases (Figure 1). A malignant renal neoplasm was suspected, and thus the patient underwent a right lower PN by means of a 4-needle radiofrequency electrode (Surtron SB, LED Italia Ltd, Aprilia, Italy), associated to cholecystectomy (performed by an urologist and a general surgeon). Through a ≤12-cm right subcostal incision, a lower RF-assisted PN was performed according to Habib’s technique. Once intraoperative ultrasound-guided needles were positioned at about 2 cm from the superior margin of the tumor in about 15 minutes, according to the manufacturer’s recommendations, a coagulative necrosis was created and a lower pole resection by scalpel was performed (Figure 2). No blood loss was observed and fibrin glue (Tissucol, Baxter, Deerfield, IL) was applied on the cut surface. Operative time was about 90 minutes. Postoperative course was uneventful, with discharge on postoperative day 4.
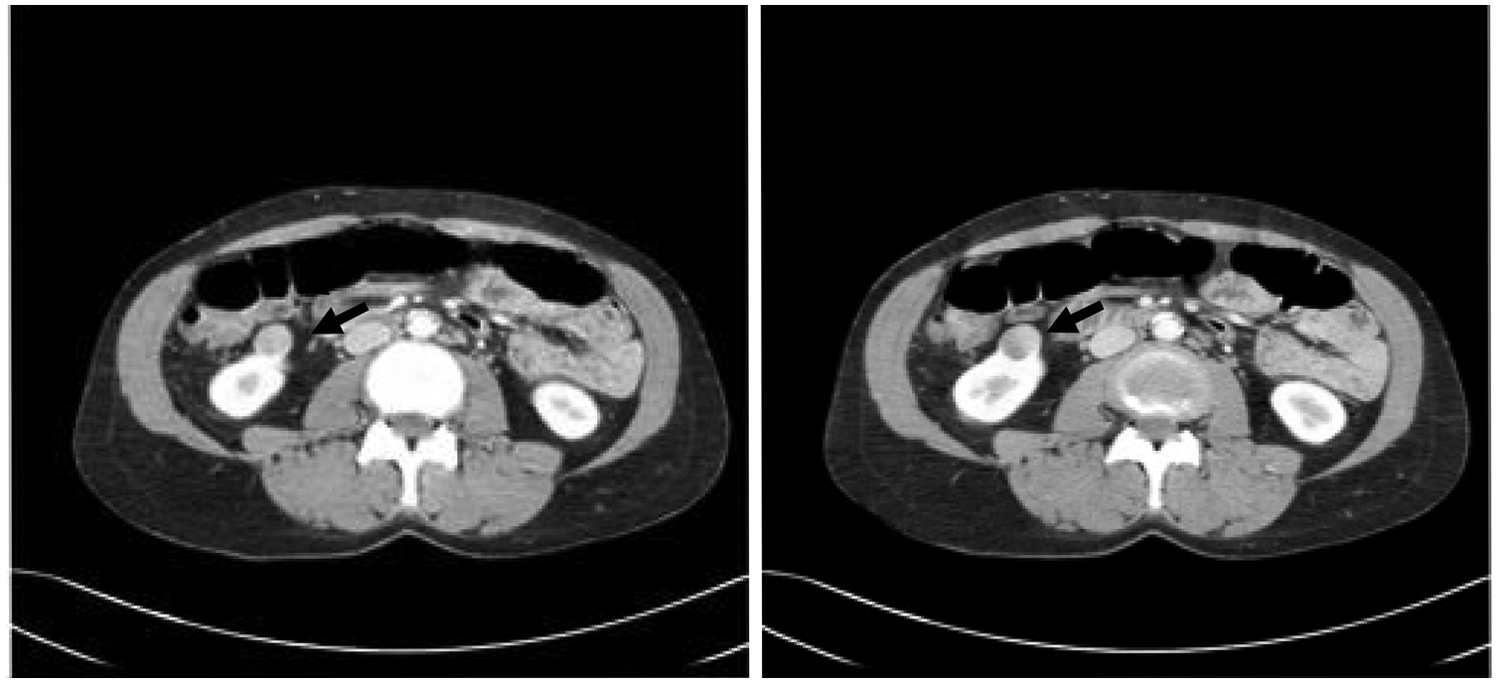
Computed tomography scan: Metanephric adenoma appears as a 20-mm isodense nodule in the lower pole of right kidney
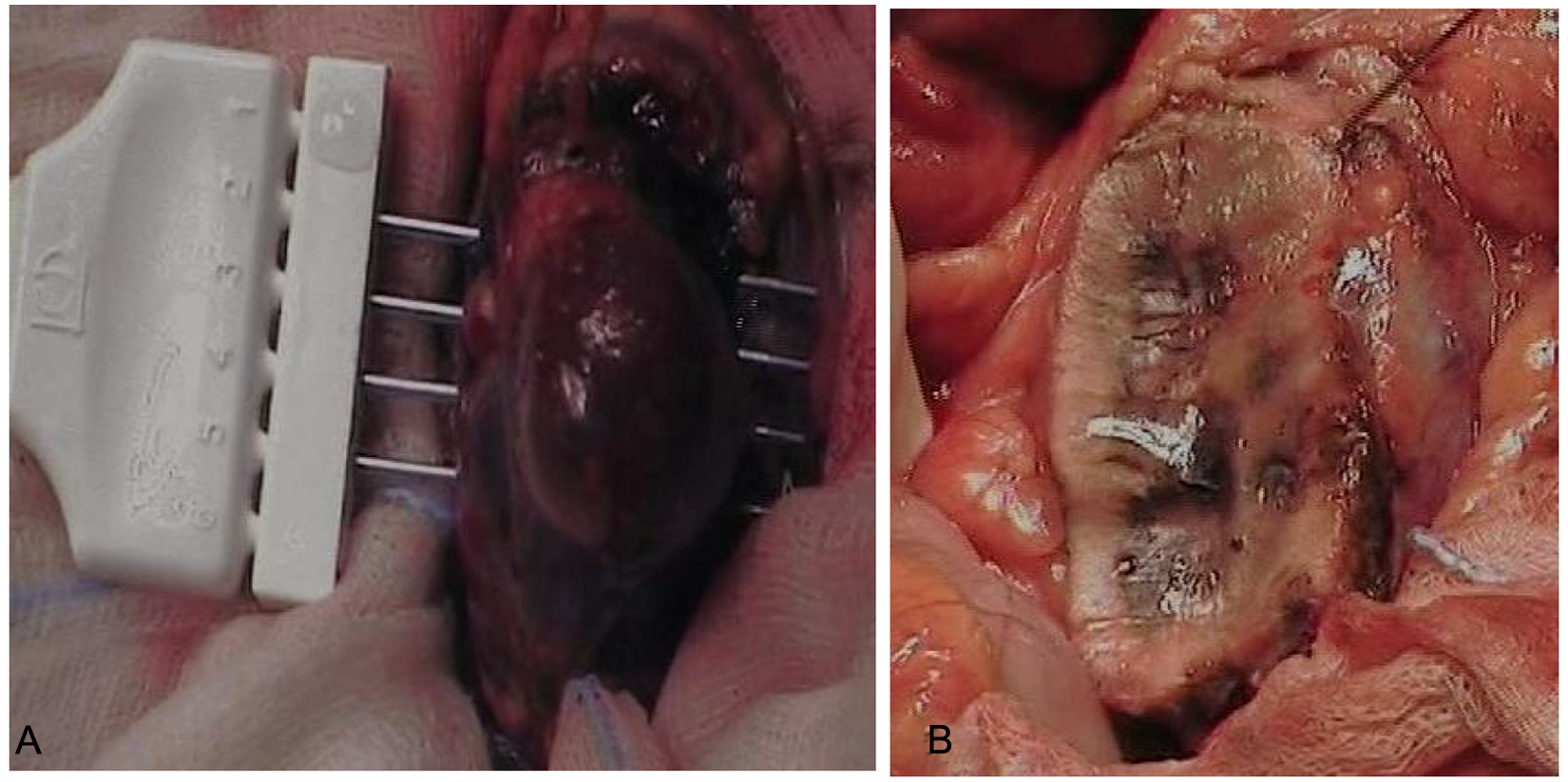
A, Intraoperative positioning of radiofrequency needles about 2 cm above the superior margin of metanephric adenoma; B, An avascular resection margin is evident after renal section by scalpel—fibrin glue was applied on the cut surface
Grossly, the specimen consisted of renal tissue measuring 4 × 3.3 × 4.5 cm in size, containing, on the cut surface, a nodule of 2 cm diameter, pink colored and soft in consistency. Microscopically, the tumor was characterized by a glandular and papillary proliferation with mild atypia and no mitotic activity, merged in a myxoid fibrous tissue. Focally, some psammoma bodies were observed. In every aspect, the tumor showed a clear-cut MA. Immunohistochemically, a focal positivity for CK7 (cytokeratin 7) and negativity for epithelial membrane antigen and racemase were observed (Figure 3).
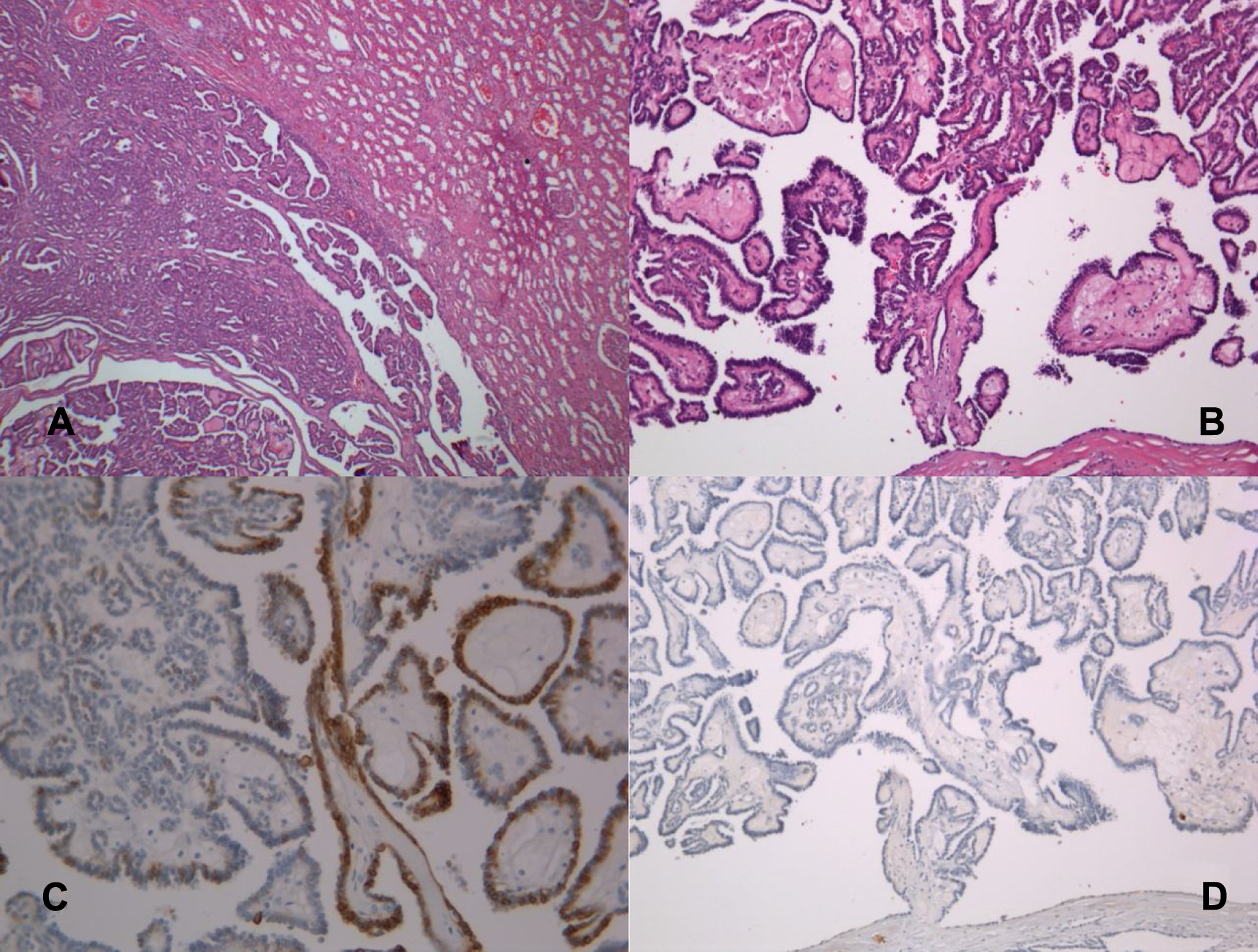
Microphotographs of the renal tumor: In every aspect the lesion shows a clear-cut metanephric adenoma.
Discussion
Metanephric adenoma is a rare renal neoplasm (constituting 0.2% of adult renal epithelial tumors), with a 2:1 female predominance and a peak age of occurrence in the fifth or sixth decade of life. 2 Grossly, MA appears as a well-defined, round, solid, and soft mass ranging from 3 to 150 mm. Histologically, MA shows small epithelial cells with a high nuclear-to-cytoplasmic ratio arranged in an acinar, tubular, glomeruloid, or papillary structure, within a paucicellular stroma, frequently showing psammomatous calcification. Mitoses are rare or absent. 2
Although MA is usually benign, some authors report metastatic forms questioning the favorable behavior of this tumor, 4,5 but in all those cases, histological diagnosis of primary tumor was doubted.
Wilms’s tumor is the main differential diagnosis of MA (age of diagnosis, presence of capsule, mitotic activity, immunohistochemical features). Main symptoms are abdominal or flank tenderness or pain, hematuria, and palpable mass, in cases of large tumors. Association with polycythemia, which varies from 1% to 6% in renal cancers, is described in up to 40% of cases. 1
Hwang and Choi, 6 after a cytological diagnosis of MA, managed conservatively a 24-year-old woman, and a 48-month follow-up did not detect either disease progression or symptoms of worsening or metastasis as well. A similar case was also described in 1997 by Zafar in a 72-year-old patient. Radiological imaging may not be specific, showing similar aspects either to Wilms’s tumor or cancer.
Radical nephrectomy may lead to the onset and/or progression of a chronic kidney disease, bringing the patient to a dialysis or transplant treatment. Hence, PN—open, laparoscopic, robotic, or hand assisted or by thermoablative procedures—once performed only on residual kidney, currently, represents the standard of care for small (<4 cm) and selected moderate (<7 cm) renal masses, according to American Urological Association Guidelines. 7 Several advantages and similar long-term oncological results, with a high survival rate (>90%) were reported, sometimes associated to a higher complication rate (bleeding, urinary fistula). 7 According to Russo, PN is rarely carried out in western countries, whereas it should be promoted through the spread of a proper training. 3
Several efficacious therapeutic alternative procedures for treating renal neoplasms, such as percutaneous or laparoscopic cryothermoablation, have been performed on selected patients, who were not eligible for surgical treatment, showing encouraging long-term oncological outcomes and very low morbidity. 8 In the last decade, referral centers have demonstrated that minimally invasive approaches, such as laparoscopic nephrectomy and laparoscopic partial nephrectomy (LPN), show comparable oncological results to traditional surgery, but with remarkable and well-known advantages. Nevertheless, LPN, currently indicated for lesions <3- to 4 cm in size, is still considered a technically difficult procedure, and sometimes a prolonged warm ischemia for hemostasis is required, especially in obese patients with large and/or central neoplasms. 9 Conversion rate in laparoscopic nephrectomy or in open surgery, operative time, blood loss, and warm renal ischemia, depend on surgeon’s experience. Since the first description of combined RF with LPN by Jacomides 10 in 2003, there has been an increasing interest in RF procedures during PN, to facilitate and improve hemostasis, creating an avascular resection margin, and avoiding hilar clamping. Such techniques showed encouraging long-term oncological and renal function outcomes, decreased operative times, and no need for hemostatic sutures, along with a low complication rate. 11 In our experience, an excellent RF-assisted hemostasis by open approach was observed, and renal parenchyma section, by scalpel, was surprisingly performed in a bloodless plane. No hilar clamping was needed.
Metanephric adenoma is an extremely rare benign tumor. After a cytological diagnosis, in selected cases, the favorable biological behavior allows an observational follow-up. PN has emerged as the standard of care for exophytic peripheral lesions <4 cm in size. RF-assisted procedures facilitate the surgical approach, allowing for an excellent hemostasis and renal resection in a bloodless plane.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.