
Abstract
Adhesions are a formidable challenge in patients undergoing reoperative cardiac surgery, particularly in those supported by an intracorporeal left ventricular assist device (LVAD) and undergoing heart transplantation. This report describes the pathological findings following the clinical use of a surgical sealant (CoSeal, Baxter Healthcare, Fremont, CA), in a patient who underwent LVAD implantation. On the treated surfaces, a minimal amount of adhesions were observed, whereas in untreated surfaces adhesions were present.
Clinical Summary
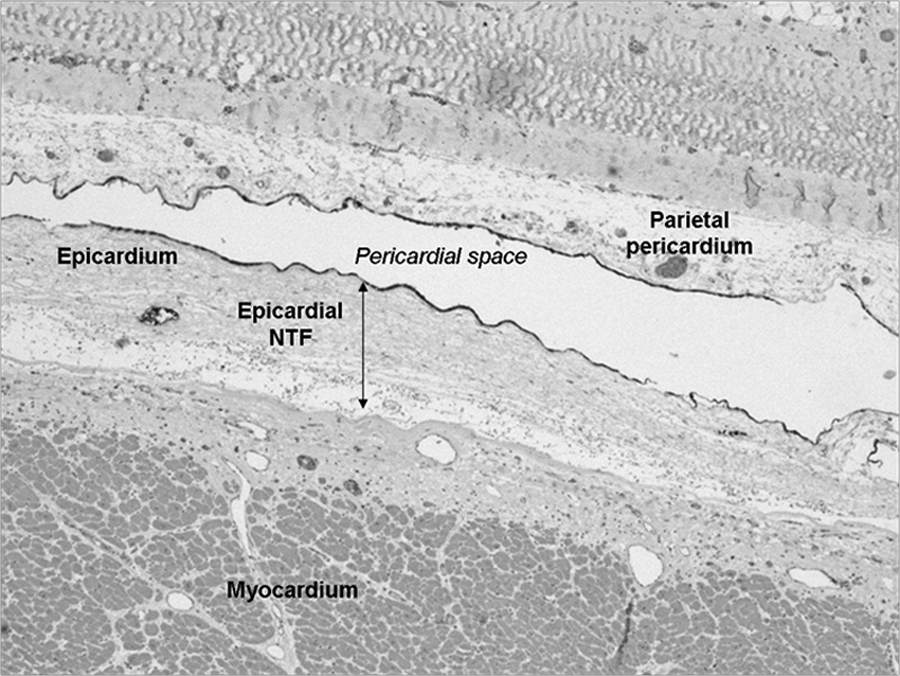
In April 2010, a 50-year-old man affected by end-stage heart failure secondary to dilated cardiomyopathy underwent intracorporeal left ventricular assist device (LVAD) implantation as a bridge to transplantation, at our hospital. At the end of the operation, as previously described, 1 8 mL of CoSeal (Baxter Healthcare, Fremont, CA) was sprayed over the anterior epicardium of both the ventricles and over the great vessels. An expanded polytetrafluoroethylene membrane was stitched along the borders of pericardiotomy to protect the outflow cannula, the great vessels, and the right ventricle. The postoperative course was uneventful, and he recovered very well. Six months later, an aggressive lymphoma was diagnosed. In March 2011, the pump stopped working. Because of the dismal prognosis of the cancer, we decided not to replace the LVAD. One year following the implantation, the patient died because of cardiogenic shock and multiorgan failure. Autopsy revealed intrapericardial adhesions around the left ventricle to be very scanty, filmy, and avascular and amenable to easy blunt dissection. Along the inferior surface of left ventricle, adhesions were found to be denser but still amenable to blunt dissection. Full-thickness intact specimens, including specimens from both the parietal and visceral pericardium, were obtained from the anterior wall (sprayed with CoSeal) and the inferoposterior wall (control) of the left ventricle. Histological sections were stained with hematoxylin and eosin and examined at low magnification. Moreover, immunohistochemical stain for calretinin was performed to detect mesothelial cells. The specimen from the anterior wall, treated with CoSeal, showed no connective tissue between serosa layers (Figure 1A), whereas it was clearly visible in the inferior wall specimen (Figure 1B). A layer of neotissue fibrosis was present in both the specimens (Figures 1 and 2) just beneath the epicardium. Immunohistochemistry showed the integrity of the mesothelial cells along both the sides of pericardium treated with CoSeal (Figure 2).
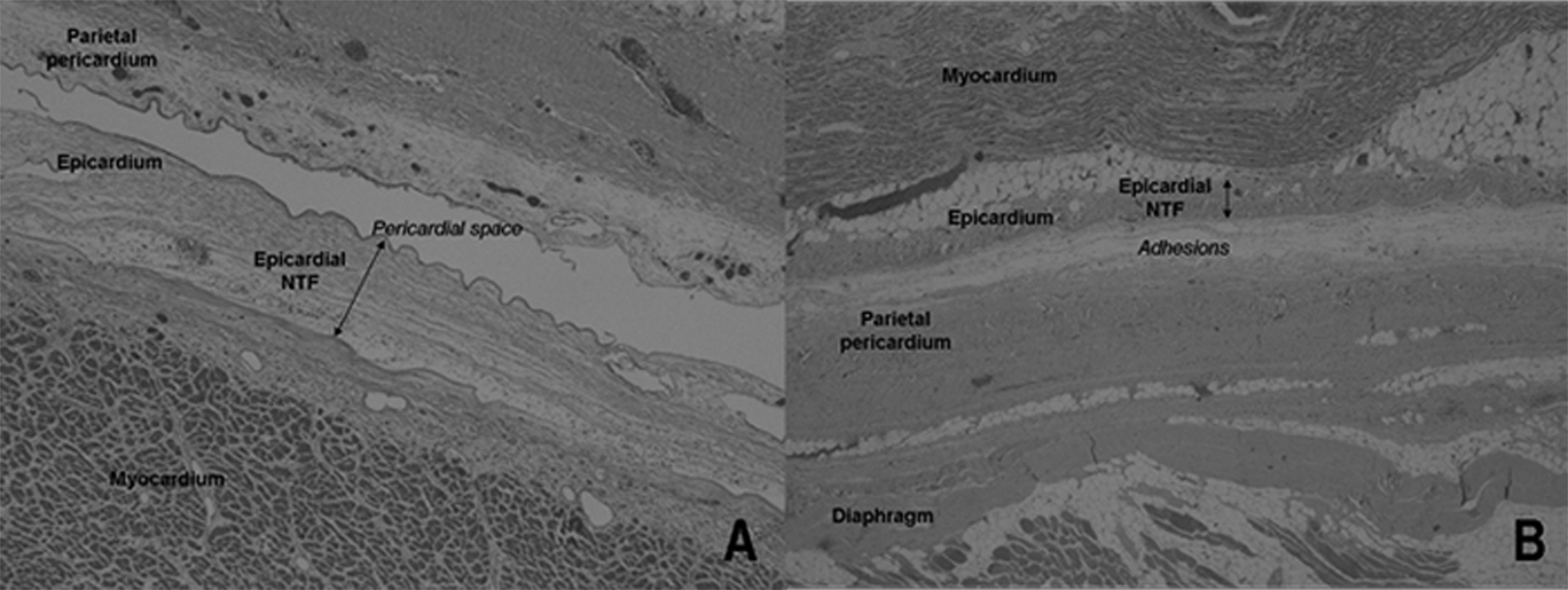
A, Photomicrograph of histology specimen (hematoxylin–eosin) from the anterior wall of the left ventricle, treated with CoSeal. No connective tissue is present between the pericardial layers. No residuals of sealant product are visible. Neotissue fibrosis (NTF) is evident just beneath the epicardium. B, Photomicrograph of histology specimen (hematoxylin–eosin) from the inferior wall of the left ventricle, not treated with CoSeal. Loose connective tissue fills the space between the pericardial layers. NTF is evident just beneath the epicardium.
Photomicrography of histology specimen from the anterior wall of the left ventricle, treated with CoSeal. Calretinin antibody staining shows the integrity of the mesothelial cells along both the layers of the pericardium.
Discussion
Adhesions are a formidable challenge in patients supported by an intracorporeal LVAD and undergoing heart transplantation. In most cases, such patients are transplanted within 12 months from LVAD implantation and during this time lapse postsurgical adhesions become dense and vascularized. 2 Dissection of the adhesions prolongs the operative time and ischemic time of the donor heart significantly and increases perioperative bleeding and the need for blood transfusions.
To limit the formation of adhesions, we adopted CoSeal, an in situ–forming surgical sealant, applied on the heart surface during LVAD implantation in patients bridged to heart transplantation. 1 CoSeal is a sprayable polymeric matrix composed of 2 synthetic polyethylene glycols. In a multicenter European study, 3 the use of CoSeal was consistently associated to filmy and avascular adhesions at reoperation. Polyethylene glycol–based sealants cover the epicardial surface and acting as a protective barrier—by limiting the aggregation of inflammatory cells and fibrin, and later collagen fibers, in the injured mesothelium, 2 —they prevent the subsequent formation of dense and vascular adhesion. Within 4 months from application, the sealant is completely reabsorbed by macrophage through phagocytosis.
To the best of our knowledge, this is the first histopathological study on human tissues about the clinical use of CoSeal in cardiac surgery. The unfortunate death of our patient did give us the unique chance to evaluate in a human being the histopathology of both the pericardial layers, on full-thickness intact specimens. It could be very difficult to obtain similar samples during a heart transplant without the risk of injury to the surrounding organs, such as lung and diaphragm. In previous experimental studies on surgical sealants and membranes to prevent intrapericardial adhesions, apparently only the epicardial side was evaluated.4,5 The inferoposterior left ventricular wall was investigated as a control, because it was not treated with CoSeal at operation. The anterior right ventricular wall was not evaluated because of the potentially confounding effects produced by the expanded polytetrafluoroethylene membrane.
In this case, intrapericardial adhesions were macroscopically filmy and avascular, and amenable even to blunt dissection. Microscopy showed an intact layer of mesothelial cells on both the sides of the pericardium (Figure 2), without connective tissue filling of the space between them (Figure 1A). On the anterior wall of the left ventricle, intrapericardial adhesions were virtually absent. Residuals of the sealant were not detected. However, some degree of inflammatory reaction produced a subepicardial layer of neotissue fibrosis in both the anterior and inferior walls (Figure 1A and B).
In conclusion, macroscopic and histopathological evidence showed that, in our patient, CoSeal use was associated with very scanty, filmy, and avascular intrapericardial postsurgical adhesions. Such finding confirms the favorable outcomes emerging from the available literature.1,3 However, there is a compelling need for prospective randomized studies to evaluate clinical efficacy of CoSeal thoroughly.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.