
Abstract
Introduction
Clinical improvement in surgical technique and postoperative care has led distal pancreatectomy (DP) to be a safe low-mortality surgical procedure; however, formation of pancreatic fistula and abscess is still a troublesome complication. The reported morbidity rate of DP remains high, ranging from 22% to 45%,1-8 and most are related to pancreatic fistula formation with an incidence rate ranging from 5% to 33%.1-8 The reported leakage rate is variable because there was no universal definition until 2005; a strict definition and grading of postoperative pancreatic fistula was proposed by the International Study Group of Pancreatic Fistula. 9 The most acceptable methods of pancreatic stump closure are traditional hand-sewn sutures and staples, which carry almost equal leakage rate.3-8,10 In general, these 2 methods can close the pancreatic stump by external compression. We hypothesized that the technique of using external compression has the same rate of pancreatic fistula, and different methods should be applied to overcome the pancreatic intraductal pressure. Our previous study proved that inductive heat by an alternating magnetic field (AMF) system can achieve bloodless liver resection and close the bile duct and vessels with intraductal plug and perivascular fibrosis. 11 In this study, we postulated that the cut surface of the pancreas and surgical end of the pancreatic duct can be sealed by using AMF inductive heat during DP.
Materials and Methods
Needle Array
An array of 26-gauge stainless steel needles in 2 linear layouts and capped with a thermoresponsive material was designed and assembled. 11 The needles are placed 2 mm apart, and the number of needles was adjusted by surgeons simply by cutting the needle array at the desired length using regular surgical scissors. This allowed for a variety of spatial conformations when 2 or more implants with different numbers of needles were used during the same resection. The height of the entire implant was 3.5 cm, with 3 cm being the effective length of the needles in contact with the tissue. The remaining 0.5 cm was buried into the magnetic applicators (coils) with Thermolite band (New Prismatic Enterprise Co, Taipei, Taiwan), a thermoresponsive material that could reversibly change its color at a temperature below (black) and above 70°C (white). This design allowed the surgeons to adjust the operating temperature for tissue resection.
AMF Generator
The AMF generator and applicator were designed and assembled in our laboratory. The system’s physical properties and specifications had been reported in our previous work. 11 In brief, the equipment generated an alternating magnetic force and proved to be capable of heating the stainless steel implants in vitro and effectively coagulated liver tissues of porcine, ex vivo, and rat and rabbit, in vivo.12-14 A thermocouple device, set at 90°C with an error margin of ±2°C, to interrupt the magnetic force at a temperature above 90°C and to operate continuously below 90°C, was used to prevent overheating 12 and to maintain a stable operating temperature. The only current modification of the machine in this study was the attachment of an extension that allows the coils to reach 1.5 m beyond the machine. This extension weighs only 2 kg and can be easily operated by 1 assistant.
Animal Model
The animal experiments were carried out under humane conditions, with an approval from the laboratory animal center of our university and in accordance with the guidelines set forth by the Agriculture Council of Taiwan on animal care.
Twenty male Lanyu pigs weighing between 14 and 35 kg (mean of 24.5 kg), from Livestock Research Institute, Taitung, Taiwan, were divided into 2 groups: the conventional group using hand-sewn closure of the pancreatic end (n = 10), and the AMF group received thermal DP by AMF (n = 10). The mean weights of the 2 groups were not significantly different. The pigs were anesthetized by intramuscular injection of atropine 0.045 mg/kg, ketamine 15 mg/kg, and propiopromazine (Combelen, Bayer) 0.05 mL/kg, followed by thiamylal sodium 8 mL/kg intravenous and isoflurane 1% to 3% 200 mL/kg/min, after endotracheal intubation. During operation, each pig’s pulse and oxygen saturation was continuously monitored, and blood pressure was recorded every 15 minutes to ensure that a change in vital signs would not interfere with the amount of bleeding during resection.
Study Design
Distal pancreatectomy was performed through an upper midline incision. The pancreas was mobilized from retroperitoneum, and the spleen was preserved, as also the splenic artery and vein. The needle arrays were inserted into the parenchyma of the pancreas, and all metallic surgical instruments were removed from the abdominal cavity, because of the risk of being heated, and they were replaced by wooden retractors. The magnetic applicators (coils), with the Thermolite band, were applied on the top end of the needle implants for 0.5 cm length, with the long axis of the needles kept perpendicular to the rim of the magnetic applicator (coil) by an assistant (Figure 1A). A few seconds after turning on the AMF generator, the color of the Thermolite band changed from black to white (Figure 1B), and change of color in the pancreas surface was also evident. On completion, the magnetic applicator was withdrawn, and the implants were completely removed. The area where the needles were applied showed macroscopic signs of thermal ablation, and the distal pancreas was transected along the ablated line by a scalpel in an almost bloodless resection (Figure 1C).
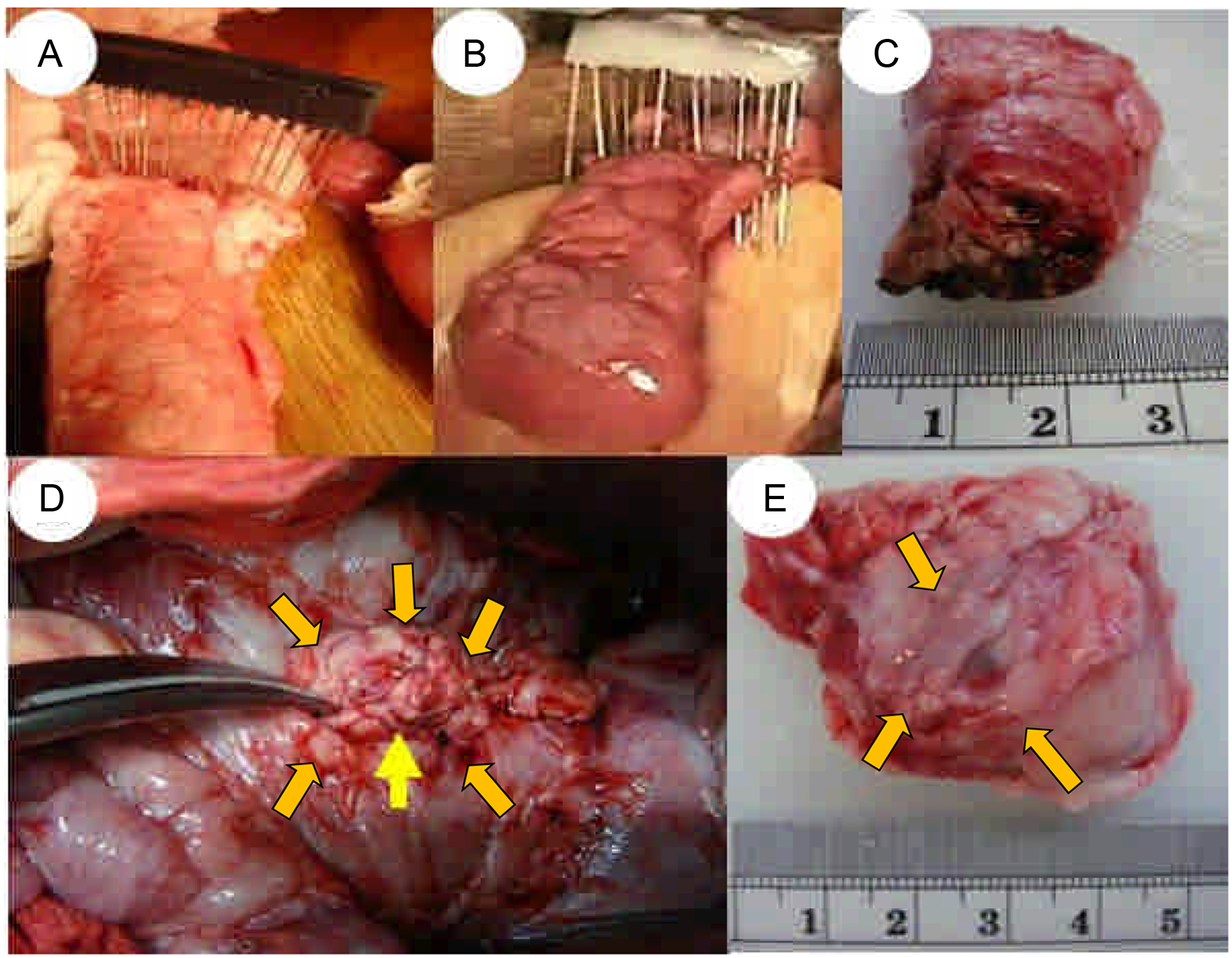
Distal pancreatectomy by AMF method.
For comparison, conventional DP using the hand-sewn method was performed. The pancreas was transected by a scalpel after mobilization, and the pancreatic stump was closed using 3-0 silk by a row of horizontal mattress sutures just proximal to the stump. The main pancreatic duct was not identified and ligated in both groups.
Degree of Postoperative Abscess
The animals in both group received relaparotomy on the 14th postoperative day (POD), and the degree of postoperative abscess was recorded according to abscess score: grade 0, well-healed pancreatic stump without abscess; grade 1, minimal amount of abscess within the pancreatic stump following the opening of the fibrotic pancreas end; grade 2, minimal amount of abscess around and within the pancreatic stump; and grade 3, presence of abscess around and within the pancreatic stump with extension to the surrounding bowels (Figure 2). The abscess score was scored by another senior surgeon staff blinded to the group. The difference in body weight after operation was also recorded. Abscess is defined as a gross collection of purelent materials. Culture, to prove the presence of bacterial infection, or drain fluid analysis was not performed.
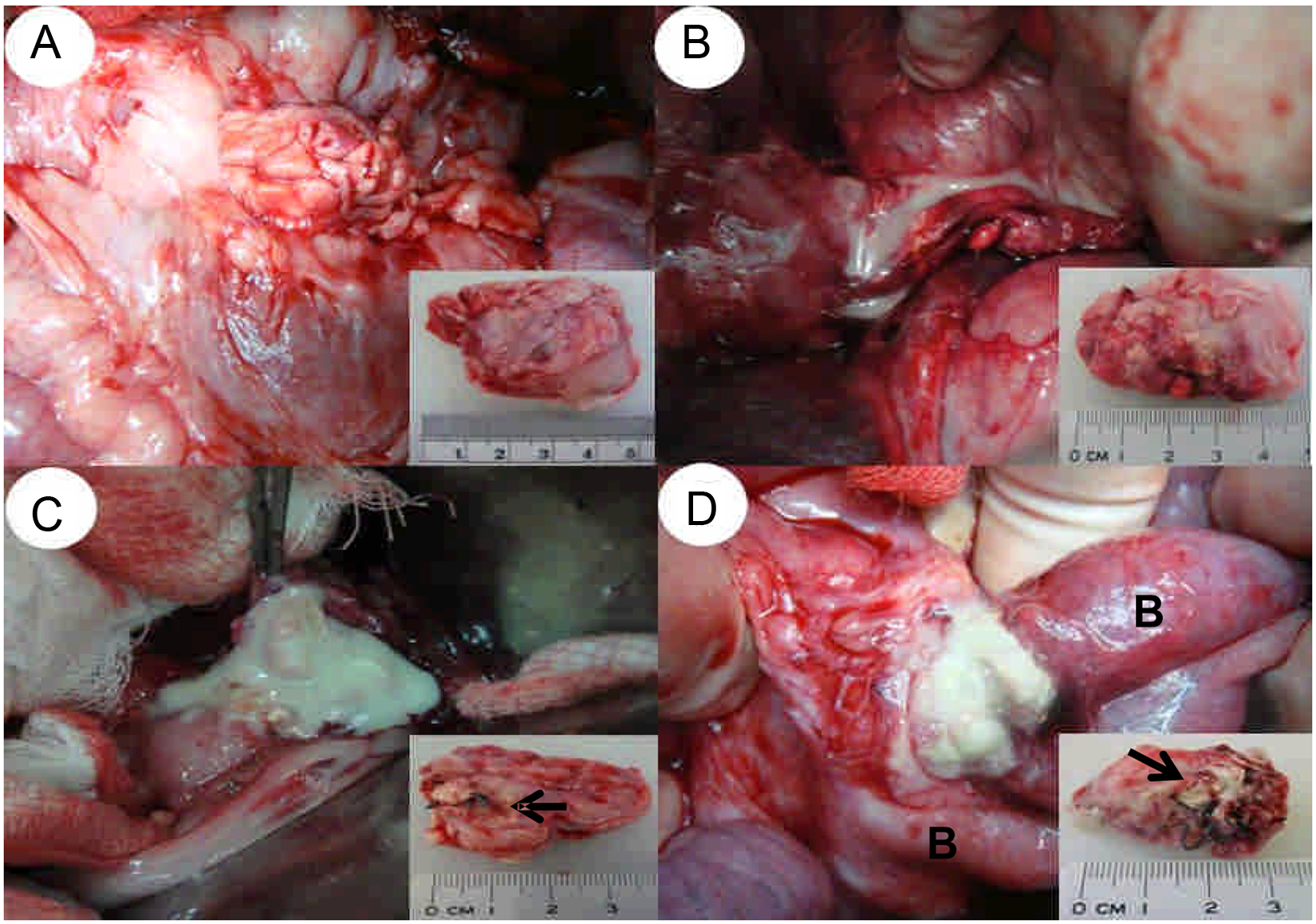
Definition of degree of postoperative abscess after DP.
Histological Examinations
The immediate effect of electromagnetic thermoablation was examined. One half of the resected pancreas was fixed in 10% formalin, sectioned, and stained with hematoxylin–eosin and tunnel test for apoptosis. To assess tissue viability with nicotinamide-adenine dinucleotide phosphate (NADPH)-diaphorase staining, the other half was frozen in optimal cutting temperature by using liquid nitrogen. The frozen samples were sectioned, mounted on glass slides, and washed in water. The samples were then allowed to react for 20 minutes at room temperature with NADPH-diaphorase reaction solution (10 mL of 10 mmol/L PBS, pH 7.4, containing 10 mg NADPH and 5 mg nitroblue tetrazolium). The remnant pancreas was removed on the day of sacrifice, and the same study was used to evaluate the reparative processes of the remnant of pancreas. The histopathologic examination was done by a blinded pathologist.
Statistical Analysis
The postoperative abscess score and postoperative body weight change were compared using the Mann–Whitney U test, and postoperative body weight change ratio was analyzed using Student’s t test. Values of P < .05 were considered statistically significant. The data were analyzed using STATA 10 software (Stata Corp, College Station, TX).
Results
Our method created a uniform ablation area equivalent to the entire length of the needles for doing DP easily. There was no animal death in each group before sacrifice on the 14th POD. The severity of abscess score after DP was significantly decreased in the AMF group compared with the conventional group: grade 0 (n = 7) and grade 1 (n = 3) versus grade 0 (n = 2), grade 1 (n = 3), grade 2 (n = 3), and grade 3 (n = 2; P = .009), respectively (Figure 3). Microscopically, there were prominent coagulative necrosis, loss of NADPH-diaphorase activity, and significant apoptosis in the resected pancreas in the AMF group when compared with the conventional group in the immediate postoperative period (Figure 4), suggesting that the inductive heat by AMF can achieve heat ablation of pancreas parenchyma successfully. On the 14th POD after AMF ablation, the pancreatic stump was covered with thick fibrosis, and histological study of the remnant pancreas showed that the parenchyma had well recovered with positive NADPH-diaphorase activity, absence of apoptosis, and the pancreatic duct was sealed off successfully by prominent periductal fibrosis and intraductal plug (Figure 5).
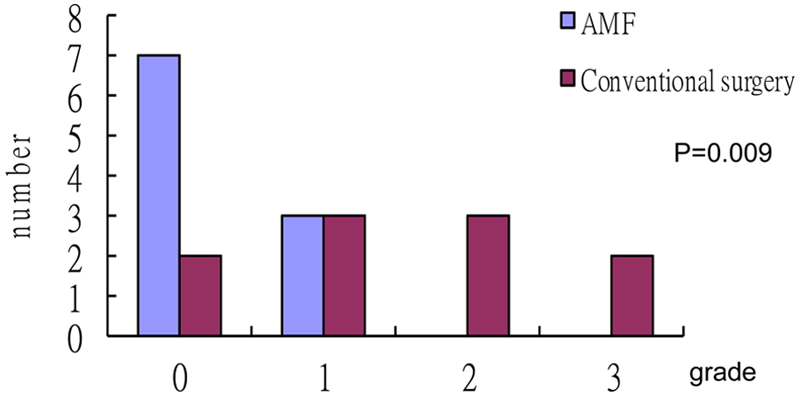
Abscess score after DP on the 14th POD.
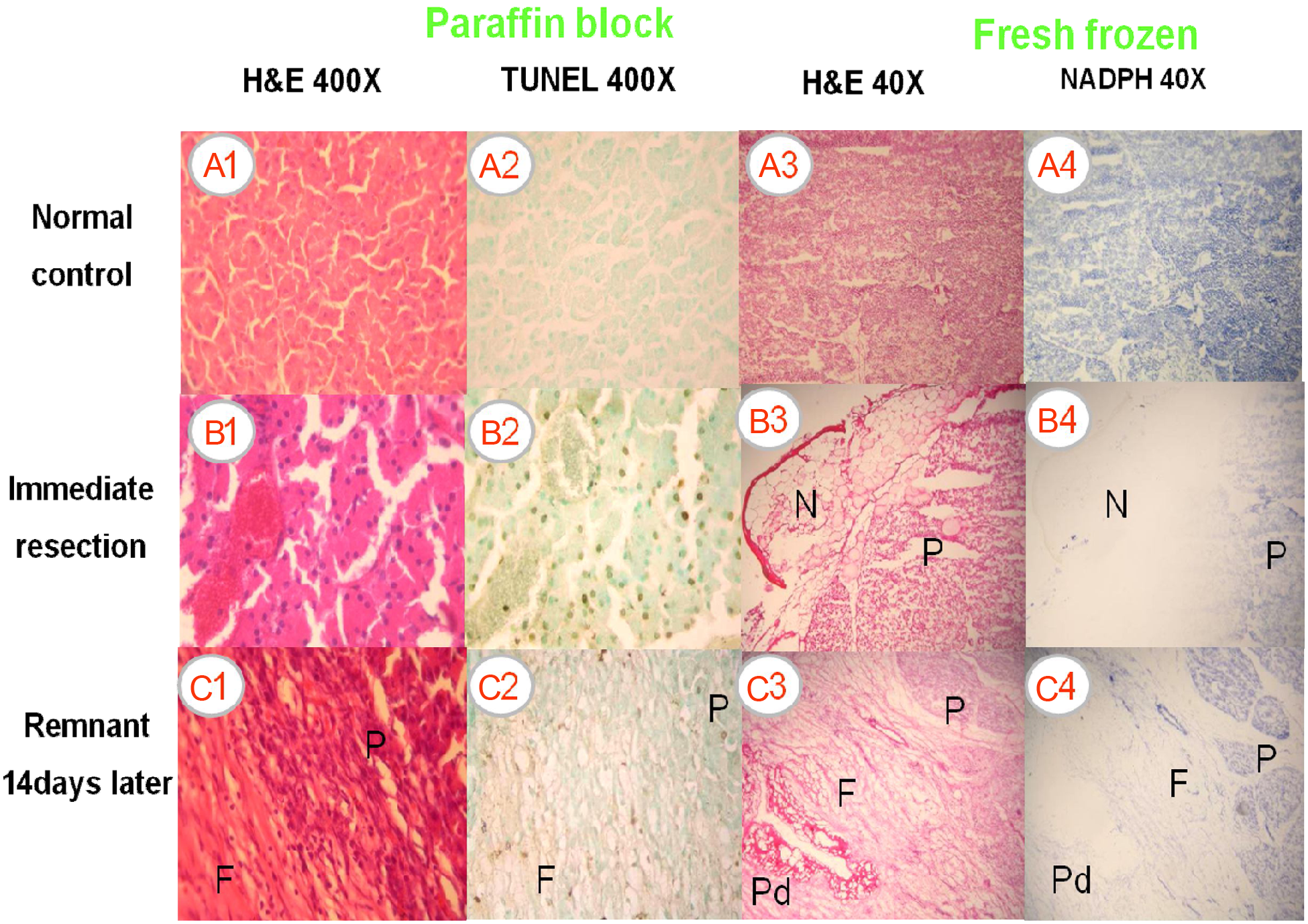
Pathological examination of the resected margin of the pancreas.
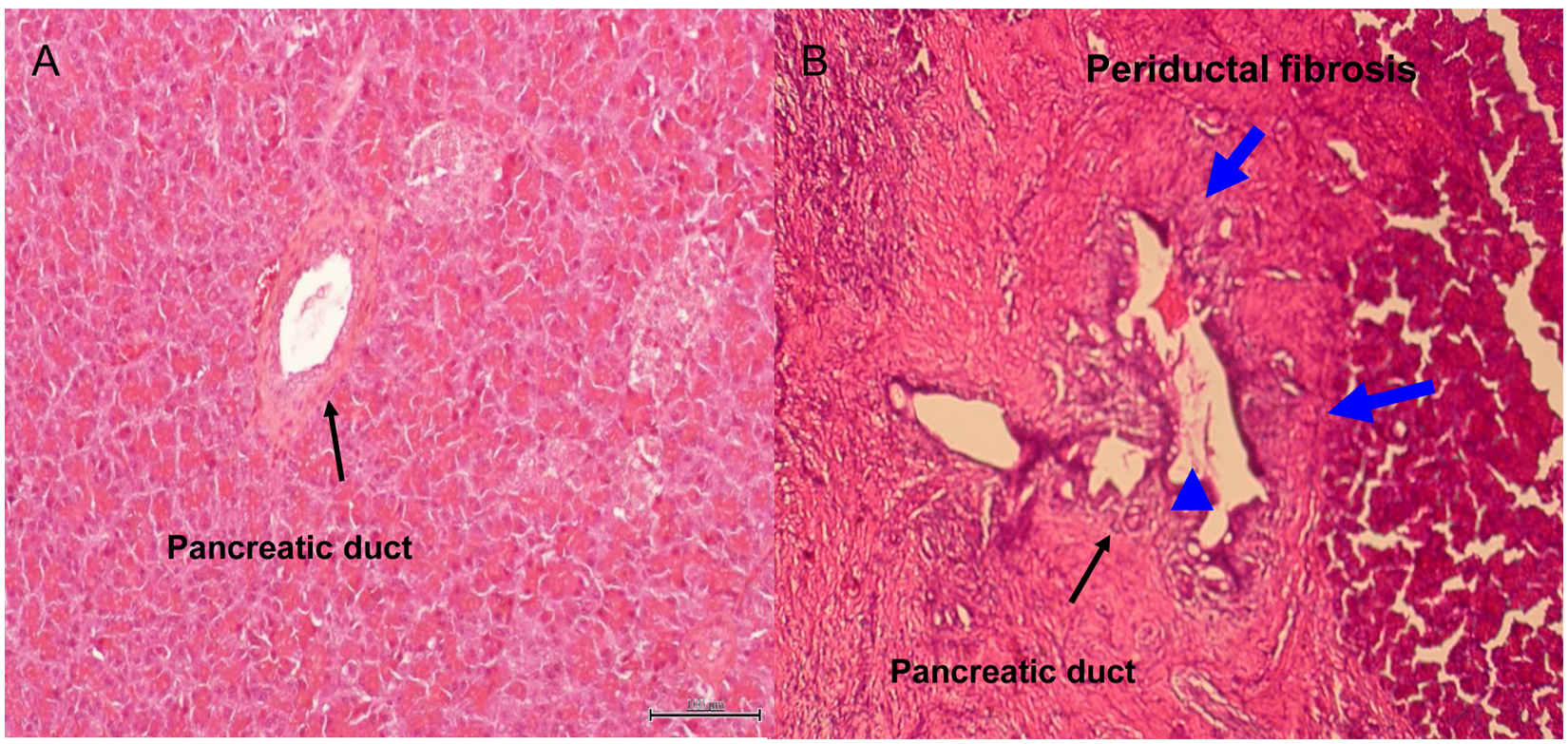
Pathology sections of resected pancreatic margin.
The body weight gain was evaluated to determine whether the intake of food was affected by DP. The averages of body weight before operation were 23.8 ± 1.8 kg in the AMF group and 25.3 ± 2.1 kg in the conventional group (P = .588). The averages of body weight on the 14th POD were 25.4 ± 5.5 kg in the AMF group and 25.4 ± 6.0 kg in the conventional group. There were 9 pigs with body weight gain before sacrifice in the AMF group compared with only 3 pigs in the conventional group and was statistically significantly increased in the AMF group (P = .003). This result correlates with lower abscess score in the AMF group compared with the conventional group.
Discussion
Pancreatic stump management is still a challenging and unresolved problem. The incidence and severity of pancreatic fistula remained unchanged though great improvement of surgical techniques and perioperative care has been achieved. There were dozens of methods in dealing with pancreatic stump during pancreatic resection, such as fibrin glue sealing, 15 occlusion of the main pancreatic duct, 16 seromuscular patch, 17 omental or free falciform patch,18,19 and Roux-en-Y drainage. 20 The most popular and acceptable methods were traditional hand-sewn sutures, staples, or both. The mechanisms of these techniques in decreasing leakage of pancreatic juice were either external compression or occlusion of the pancreatic duct and pancreatic end surface; however, the conclusive optimal surgical procedure for pancreatic stump closure cannot be drawn.15,16,19,21 The normal pancreatic parenchyma is soft in consistency and tends to have higher rates of pancreatic leak than the hard one because the soft pancreatic parenchyma is subjected to crushing. 19 Ligation of the main pancreatic duct combined with other techniques such as suture, ligation, or stapling of the pancreatic end cannot decrease leakage of pancreatic juice 22 probably because of the increase in intraductal pressure at the pancreatic end during contraction of the papillae and the presence of 0 to 5 branches of pancreatic duct on the cut surface of the pancreatic end. 21
In this study, a totally different mechanism and technique was used in contrast to previous studies. The electromagnetic force generates inductive heat uniformly via the needle arrays and generates an area of coagulative necrosis that ablates pancreatic tissue, including the vessels and pancreatic duct. It avoids unnecessary manipulation or crushing of the cut surface of normal pancreas parenchyma and is able to induce dense fibrosis formation around the main and branches of pancreatic ducts resulting in decreased leakage of pancreatic juice and abscess formation. These correlates with the findings of lower abscess score and improve body weight gain in the AMF group.
There were 2 porcine studies using LigaSure device 23 and saline-coupled radiofrequency ablation (TissueLink) 24 to seal the pancreatic stump without sutures or staples. The LigaSure device study did not show any significant difference when compared with the suture group. The TissueLink study revealed evidence of complete coagulative necrosis with obliteration of both vascular and ductal structure, with leakage rate of 5.5% versus 42% in the suture group. Recently, a small series of laparoscopic DP, using Habib 4x, which delivers high-energy radio wave, showed a 14% pancreatic leak in 14 patients. 25 Our studies have shown that the incidence of pancreatic leakage and abscess formation were significantly lower in the heat ablation method using AMF compared with the conventional method using hand-sewn or staple method, and it can be feasible in the near future.
There are some limitations in this study. First, the postoperative amylase level from the intra-abdominal fluid was not determined and the severity of pancreatic fistula was not classified according to definition by the International Study Group of Pancreatic Fistula. 9 Instead, the clinical observation of abscess formation was done and showed the AMF group had a significant lower abscess score than the conventional group (P = .009), which might indicate lower pancreatic leakage. The body weight gain was also increased with statistical significance (P = .003) on the 14th POD in the AMF group and correlates with low abscess score and less irritation of the peripancreatic organs. Second, the thickness of the pig’s pancreas is thinner than in human beings, and the main pancreatic duct is not easily identified and ligated in the conventional group. Whether the periductal fibrosis in pig’s pancreatic duct can produce the same compression effect in the larger human pancreatic duct needs further validation and experimental studies.
In conclusion, the AMF system is an alternative method of sealing of the pancreatic end when performing DP in the porcine model, and clinical trial is necessary for its use in the future.
Footnotes
Acknowledgements
We thank the veterinarian Chih-Ting Liu, Mr Chih-Hao Huang, and Mr Sheng-Chieh Huang for helping with operations in the porcine model. We also thank Ms Ming-Hwa Chen and Ms Yi-Chun Lai for their excellent coordination of this multidisciplinary team.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study is supported partly by a grant from the National Science Council of Taiwan, NSC 97-2627-B-006-007; Dr Roberto Zuchini, physician and PhD student, was supported by an international scholarship from National Cheng Kung University.