
Abstract
Introduction
Computer-enhanced surgical technology has been used to compensate the drawbacks of conventional open surgery, such as faster recovery with less pain and fewer complications after surgery. 1 This technology included master-slave telemanipulator systems that allow surgeons to control the system remotely during surgery. The intuitive design enhanced the clinical capability while maintaining the same “look and feel” of conventional surgery. The da Vinci Surgical System (dVSS; Intuitive Surgical Inc, Sunnyvale, CA) is one of the examples of computer-enhanced surgical technology that provides an intuitive translation of the telemanipulator to the robotic instrument tip and supports an internal articulated endoscopic wrist providing multiple degrees of freedom. Several studies indicated that surgeons seem to take more time to perform surgical procedures in robotic-assisted surgery because of the limited surgical space in the body. They also tend to be more cautions, which leads to increase in operating time.2,3 The prolonged average operating time increases the amount of blood loss. 4 To reduce the operating time in robotic surgery, development of an efficient training protocol for robotic surgery became an inevitable mission. 5
Since William Halsted introduced surgical training based on the apprenticeship model more than 90 years ago, “See one, do one, teach one” became the gold standard for conventional surgical training. 6 However, this gold standard training protocol might be inappropriate for modern surgical skills training because of the rising cost and complexity of medical technology, the resident work hour restriction, and an increasingly hostile malpractice scenario. 7 For instance, practice on live animals or cadavers was often incorporated in the training protocol for robot-assisted laparoscopy. However, live animals provide an inexact replication of the human anatomy. In addition, although cadaver training provides true anatomical depiction, trainees might only have one opportunity to learn, and the cadaver was usually expensive. 8 Because novices had fewer opportunities to be trained either in animal practice or using cadavers, the National Academy of Science’s Institute of Medicine reported that approximately 44 000 to 98 000 deaths occurred every year as a result of medical errors. Many of these errors could be avoided if surgeons were trained appropriately. Unfortunately, most novice surgeons did not receive enough training because of limited resources. Skills training in a virtual reality (VR) environment might be an alternative protocol to enhance the surgical proficiency of novice surgeons. 9
VR simulators have been playing an introductory role in training residents for laparoscopic, gastrointestinal, plastic, ophthalmological, dermatological, and laryngological procedures.10-14 The aim of VR training is to enhance the surgical proficiency of novice surgeons from the “pure novice” to the “pretrained novice” level. 9 More important, simulation in surgery provided opportunities for novice surgeons to learn from errors in a safe environment. 15 Until now, several commercial VR simulators have been validated for teaching surgical skills. The minimally invasive surgical trainer, VR (Mentice AB, Gothenburg, Sweden) allowed novices to undergo structured training of basic skills for laparoscopic cholecystectomy, such as picking up objects, moving objects, and rotating objects.16,17 LapSim VR laparoscopic simulator (Surgical Science, Gothenburg, Sweden) provided advanced surgical training protocols, such as cutting, knot tying, and dissection. 18 ProMIS (Haptica Ltd, Dublin, Ireland) provided an environment for surgeons to complete a laparoscopic colon procedure using actual and simulated physical tissues all through a VR interface. 19 The high cost and the console-specific characteristics of these simulators are obstacles that prevent them from becoming prevalent. In attempting to overcome these drawbacks, some studies showed that playing video games could be used an alternative strategy to train surgical proficiency. Schlickum et al 20 trained individuals with first-person shooter games and assessed their performance in 2 VR endoscopic surgical simulators (MIST-VR and GI Mentor II). This study showed that playing video games indeed enhanced surgical performance. Badurdeen et al 21 found similar results and concluded that learning effects of fundamental eye-hand coordination skills in Nintendo Wii and basic laparoscopic tasks overlapped. However, Rosenberg et al 22 indicated that playing video games might only be used to predict the level of laparoscopic skill in novice surgeons.
It is still under debate whether playing 3D video games could enhance fundamental laparoscopic skills. The objective of our study was to address the following questions: (1) Do trainees show improvement in fundamental robot-assisted surgical skills with dVSS after training in a VR environment with a portable simulator? (2) Compared with playing a 3D game, does training with a VR simulator show more benefits in enhancing fundamental robot-assisted surgical proficiency? We hypothesized that novices would experience a significant enhancement in fundamental robot-assisted surgical proficiency after training in our portable VR simulators as compared with playing a 3D game.
Materials and Methods
Participants
In all, 14 medical students from the University of Nebraska Medical Center with no previous experience operating the dVSS participated in this study. They were randomly assigned to either the experimental group training with the VR simulation or the control group playing the 3D game. This study was approved by the Institutional Review Board of University of Nebraska Medical Center.
Training Tasks
Two fundamental surgical tasks, bimanual carrying (BC) and peg transfer (PT), were developed identically in both actual and virtual environments. The PT task was more complex than the BC task because it required more coordinated hand motion with better control of spatial orientation. In the BC task, participants simultaneously picked up pieces from metal caps and placed them in 2 other metal caps. In the PT task, they randomly pulled a peg out from 1 of 6 columns with 1 hand, transferred the peg to another hand in space, and then placed the peg in another column located on the opposite side. Once they transferred all pegs from the nondominant hand to the dominant hand, they repeated the drill from the dominant hand to the nondominant hand. Both tasks have been designed to mimic training of real-life surgical skills in terms of coordination (BC task) and grasp and release skills (PT task).
Experimental Protocol
In the VR group, participants were trained to practice both tasks in the VR environment and completed 10 trials for both virtual tasks in random order after practice. In the control group, participants completed the same procedures but practiced maneuvering the pair of simulators with the 3D game for 40 minutes. The practice time in the control group was similar to the average training time in the VR group. All participants completed 5 trials for both actual tasks in the pretraining and the posttraining in the dVSS.
Apparatus (VR Training System)
The portable VR simulator consists of a pair of manipulators (SensAble Technologies, MA) and a virtual simulator training platform (WorldViz LLC, CA; Figure 1). The 3D tennis game for the control group was made by H3D, which is an open source for our manipulators. Our VR training environment was coded by Python, which is a cross-platform computer language; it is highly compatible with any personal computer systems. The total weight of our simulator is less than 10 kg, and all components can be placed in a simple backpack. The cost of our VR simulator is approximately $4000, which is affordable.

Portable virtual simulator.
Data Collection and Analysis
Kinematics of the surgical robot arms were recorded for all trials. The kinematic dependent variables were time to task completion, total distance traveled, and differences in both variables between pretraining and posttraining. The total distance traveled was the sum of Euclidean distances obtained by moving the instrument tips of the surgical robot arms between each time sample. They were acquired to use the dVSS Application Programmer’s Interface provided by Intuitive Surgical, Inc (Sunnyvale, CA). A custom program using LabView (National Instruments Corp, Austin, TX) was written to interface with the dVSS via an Ethernet connection. Kinematic data were streamed at 75 Hz. All data were postprocessed using MATLAB 2009 (MathWorks Inc, Natick, MA). The learning effect was examined by the differences between the pretraining and posttraining trials using a paired t test. An independent t test was used to analyze the learning effects in the 2 training groups.
Results
Our results demonstrated that the VR group had a significant decrement in the time to task completion both in the BC task (P < .001) and in the PT task (P = .002; Table 1) after VR training. Moreover, there was a significant decrement in the total distance traveled in the VR group both in the BC task (P = .03) and in the PT task (P = .018; Table 2). However, the control group only had a significant decrement in the time to task completion in the BC task (P = .047) but not in the PT task (P = .76; Table 1). There were no significant differences in the control group for total distance traveled, neither in the BC task (P = .79) nor in the PT task (P = .56; Table 2).
Time (s) to Task Completion in the BC and PT Tasks.
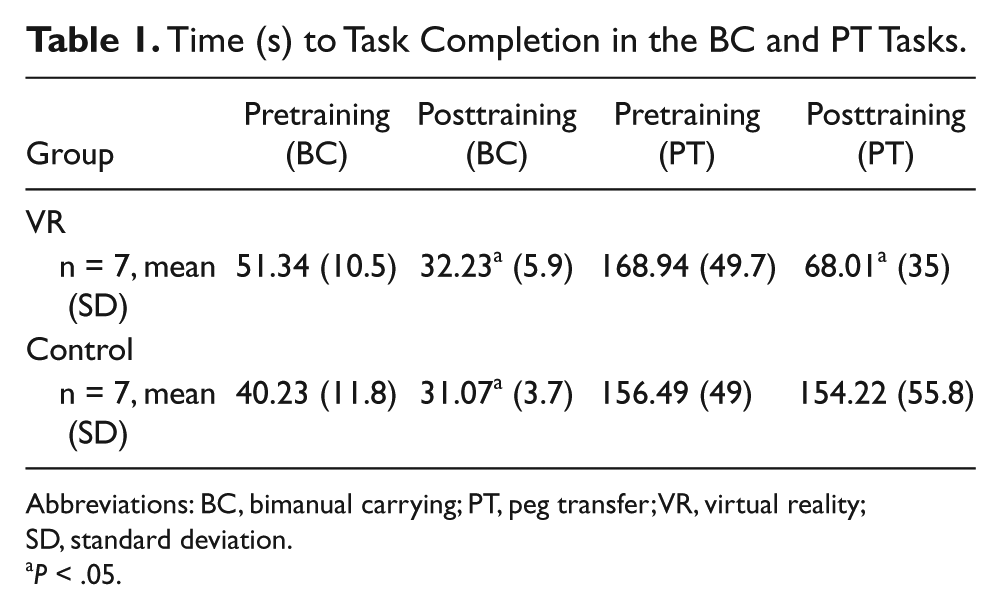
Abbreviations: BC, bimanual carrying; PT, peg transfer; VR, virtual reality; SD, standard deviation.
P < .05.
Total Distance Traveled (mm) in the BC and PT Tasks
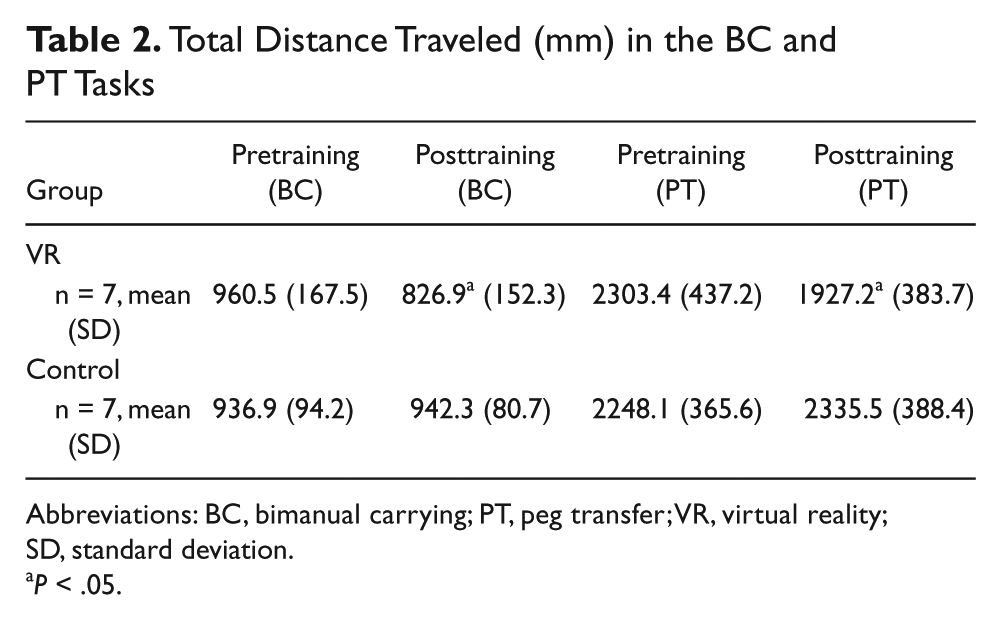
Abbreviations: BC, bimanual carrying; PT, peg transfer; VR, virtual reality; SD, standard deviation.
P < .05.
When the VR group was compared with the control group for the BC task, the VR group showed a significantly larger difference between pretraining and posttraining in the time to task completion (P = .008; Figure 2) but no significant difference between pretraining and posttraining in the total distance traveled (P = .058; Figure 3). For the PT task, the VR group showed a significant decrement in the time to task completion (P = .002; Figure 4) and in the total distance traveled (P = .027; Figure 5).
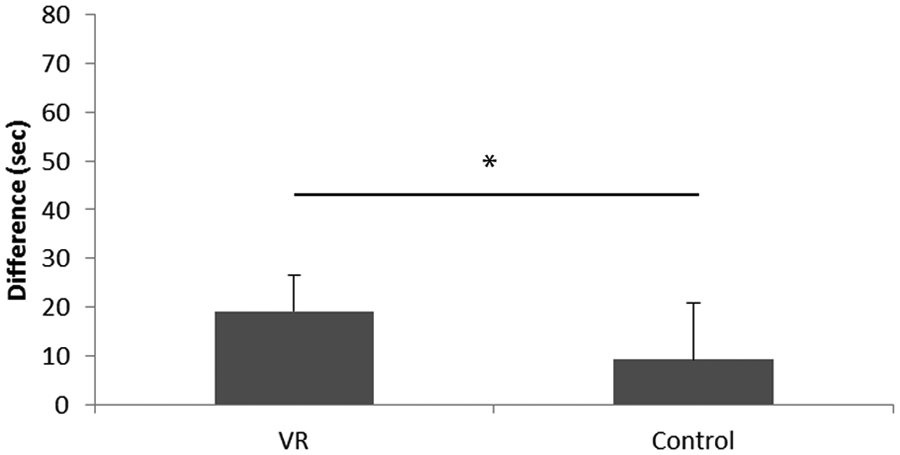
Learning effect of the time to task completion in the bimanual carrying task.
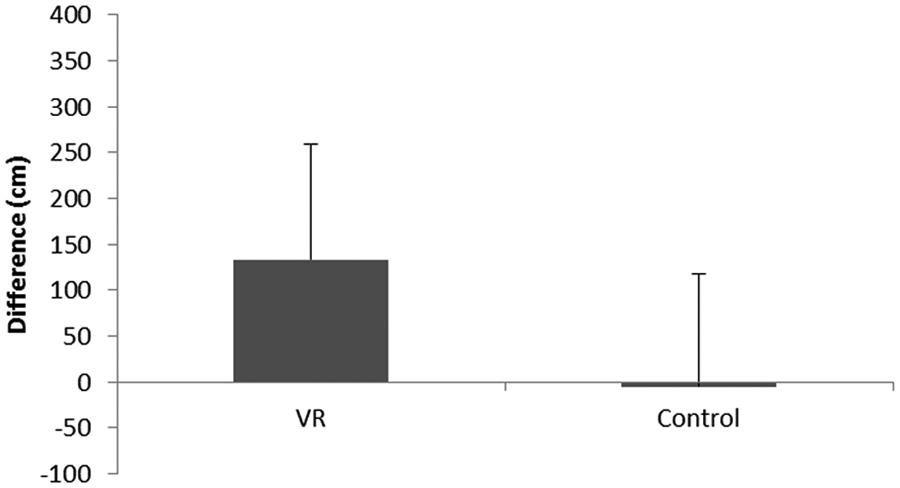
Learning effect of the total distance traveled in the bimanual carrying task.
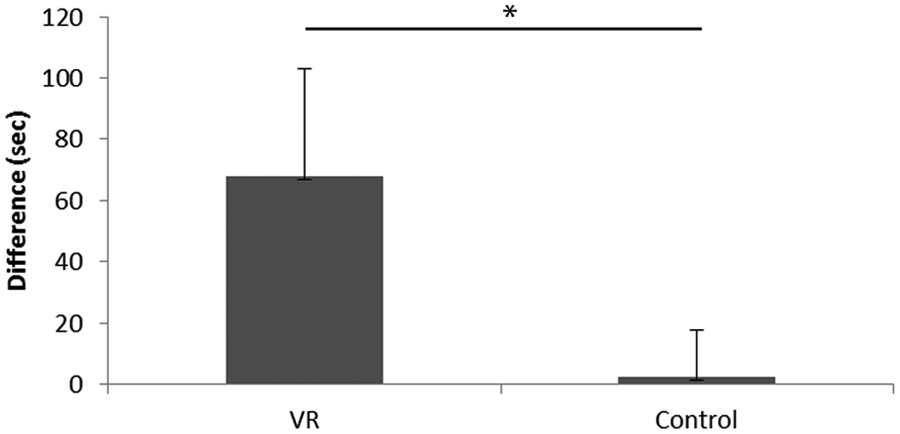
Learning effect of the time to task completion in the peg transfer task.
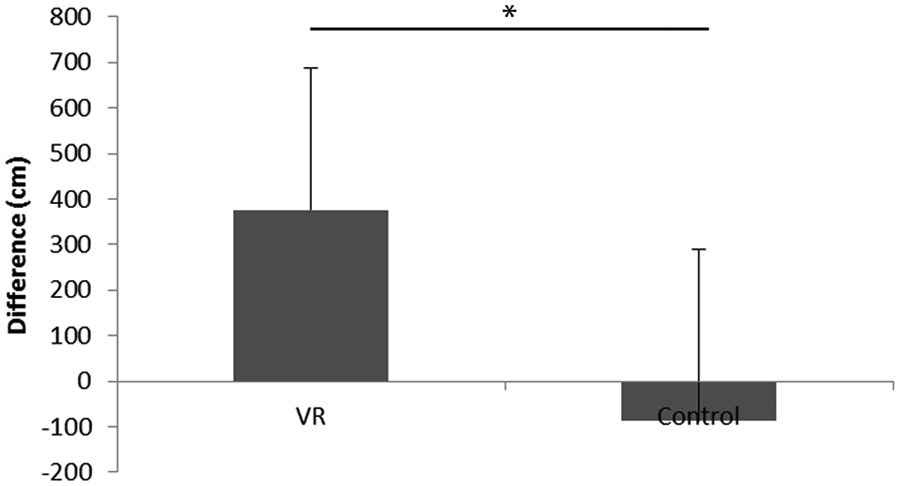
Learning effect of the total distance traveled in the peg transfer task.
For the control group, the average differences in total distance traveled between pretraining and posttraining in the PT task were negative (Figure 5); in other words, those training with the 3D game seemed to perform even worse at posttraining than at pretraining.
Discussion
The purpose of our study was to investigate the following issues: (1) Did trainees have better performance after training with the portable VR simulators? and (2) Did trainees also have a better performance after training with the portable VR simulators compared with training with a 3D game? We hypothesized that trainees would have significant improvement in fundamental robot-assisted surgical proficiency after training with the portable VR simulators as compared with playing the 3D game.
Our results support our hypothesis that the portable VR simulators indeed enhanced fundamental surgical proficiency and transferred the surgical skills from the virtual environment to the actual robot-assisted surgical environment. Especially, participants performed significantly better after VR training in the PT task compared with those who received the 3D game training. Our results were in line with previous studies that VR training provided a new opportunity for training novices at a fundamental stage.10-14 Novices are able to learn fundamental skills from “errors” using VR. There is no longer a need for surgical trainees to practice their surgical skills on animals or even on patients at the early stage of surgical learning.
Inappropriate use of simulation might have a negative impact for users. 9 Therefore, it was very crucial to select the appropriate virtual training environment for novices. We chose the BC and PT tasks for the following reasons: (1) They are fundamental and can be performed by medical students with no prior experience in robot-assisted surgery; (2) they are well-designed tasks that mimic real-life surgical skills in terms of their coordination and grasping and releasing skills; and (3) training from simple to moderate tasks can assist novice surgeons in achieving the level of a pretrained novice easily. 9 Aggarwal et al 18 indicated that training at the easy level allows the learner to better understand how to control the simulators and the nature of the tasks to be performed. Medium-level tasks might lead learners to refine their performance. In the current study, our results are in agreement with these rationales that novices perform better both in the BC task and in the PT task after receiving the VR training.
It is interesting to note that while comparing those who received VR training with those who played 3D games, we found that both groups showed significantly better performance in the BC task. The result was in line with previous studies that even playing video games might enhance fundamental surgical skills.20,21 However, only the VR group showed a better performance in the PT task. To answer the question of whether training in VR is more beneficial than playing games, we further used a second paired t test to investigate the training effect between the last trial before the game training and the first trial after the game training. We found that training by playing 3D games yielded no significant differences between the 2 trials in the BC task, either in the time to task completion or in the total distance traveled; however, the 3D game training reduced the fundamental surgical proficiency in the PT task in both time to task completion (P=.014) and total distance traveled (P = .05) when 2 trials were compared. These results suggest that playing a PC game might only enhance proficiency in a specific level of the task. For training purposes, to create as similar an environment as possible would provide the best learning effect for trainees. 23 This could be the reason why those who received VR training had a better performance than those who played the 3D game. Because of the distinctly different environments between virtual task training and playing tennis, those in the control group even showed a negative learning effect (increased total time to task completion and increased total distance traveled; Figure 5).
Potential limitations of the current study are the following: (1) the stylus type handles of the manipulator were quite different from the gripper of dVSS console. However, our lab is currently modifying the handles to be similar to the ones in the dVSS console to reduce the ergonomical discrepancy. (2) no questionnaire is provided to evaluate how well our medical students adapt in the VR training environment. This could be important information and future studies could try to determine how simulator users can adapt to a virtual training environment; (3) although the 3D game used in this study was not related to surgery, it requires bimanual coordination skills similar to the VR training tasks. Further studies using surgery-related 3D games could be beneficial to confirm our finding.
Although the effectiveness of VR training in surgery still requires more extended investigation, our study provides supportive evidence to encourage the development of virtual simulators for surgical education. Training with the portable VR simulator enhances robot-assisted surgical skill proficiency in comparison to playing 3D games. Our results suggest that development of and practice with a task-specific virtual training environment could improve actual surgical skills.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by the Nebraska Research Initiative Grant and the Center for Advanced Surgical Technology, University of Nebraska Medical Center.