
Abstract
Objectives. To introduce a low-cost, self-made device for single-port retroperitoneal laparoscopic radical nephrectomy and to evaluate outcomes compared with conventional laparoscopy after initial experience using this device. Methods. Twenty-nine renal cancer patients underwent retroperitoneal laparoendoscopic single-site radical nephrectomy using a self-made single-port device with multiple manipulation channels for passage of routine laparoscopic instruments and specimen removal. A control group of 29 patients who were matched by age, gender, and cancer stage underwent conventional laparoscopy. Outcomes were analyzed retrospectively. Results. There were no significant differences in age, gender, body mass index, T stage, and maximum tumor diameter between groups (P > .05). The laparoendoscopic single-site surgery group had a significantly shorter duration of postoperative hospitalization than the conventional laparoscopy group (7.14 ± 1.38 days vs 8.17 ± 1.54 days, P = .009). Conclusions. Retroperitoneal laparoscopic radical nephrectomy using our self-made single-port device appears to be a feasible, safe, and low-cost surgical strategy.
Introduction
Along with continuous development of minimally invasive techniques, surgeons have worked incessantly to find new minimally invasive methods that could reduce surgical trauma and scarring as much as possible and achieve excellent outcomes and cosmetic results. Laparoscopic radical nephrectomy with intact specimen removal has been practiced for a decade and has become the standard practice for localized renal carcinoma. 1 However, although stage T1 and T2 renal cell carcinoma can be treated excellently with the conventional laparoscopic technique, at least 3 incisions are needed to perform this type of procedure. 2 Larger skin incisions for intact extraction also compromise cosmetic results, but intact extraction of nephrectomized specimens is preferred over morcellation of the specimen because it provides a specimen equal to that of open surgery with the advantages of accurate staging and margin assessment. 3 Even with the growing popularity and demonstrated effectiveness of laparoscopic techniques, surgeons still work continuously to decrease the number and size of surgical incisions. Recent reports have described performing simple nephrectomy and resection of renal cell carcinoma using single-port transumbilical incisions and single-port retroperitoneal approaches.4-9 The laparoendoscopic single-site surgery (LESS) procedure is considered safe compared with conventional laparoscopy, and differences in operative time and complications are not significant. 10 However, single-site laparoscopic nephrectomy is not without challenges.
Standard surgical treatment of renal cell carcinoma requires removing the kidney together with the perirenal fascia and the adipose capsule of the kidney, and sometimes the adrenal gland also must be removed. The large volume of the resected specimen makes it difficult to remove it through the natural channel or an umbilical incision. Under current technical and instrumental conditions, a corresponding incision is needed for taking out the intact renal carcinoma specimen. Also, the cost of current commercial single-port instruments is relatively high, their diameters are relatively small, special equipment is needed, and even with the latest equipment, the related manipulation is still difficult. During radical nephrectomy, the incision must be extended for removing the specimen, which makes early stage manipulation difficult as well as resulting in late stage waste of the incision length. Recent reports have described successful application of homemade single-port instruments with demonstrated cost-effectiveness and adequate range of motion for urological procedures.7,9,11 However, few have addressed retroperitoneal laparoscopic radical nephrectomy.
Our institution, the Chinese PLA General Hospital, is one of the largest hospitals in China, with around 140 patients under the care of the Department of Urology, and we treat approximately 1000 kidney tumors annually. Our surgeons include experienced laparoscopists, and it was natural for us to focus on improving minimally invasive laparoscopic surgery, especially attempting to reduce the number of incisions, operation time, recovery time, and number of incision scars, as well as to reduce costs. We have performed radical nephrectomies in 29 patients at our center using the single-port multichannel retroperitoneal laparoscopic technique. These surgeries were performed using a low-cost, self-made, multichannel device designed to minimize patient scarring, reduce costs, and allow for efficient performance of the laparoscopic technique by using readily available materials. Our purpose was to introduce this self-made laparoendoscopic single-site instrument and to evaluate patient outcomes for laparoscopic single-site radical nephrectomy after our initial experience using this device.
Patients and Methods
Patients
A retrospective study of patients with renal cell carcinoma who underwent radical nephrectomy at our institution was conducted between April 2011 and September 2011. We performed single-port retroperitoneal laparoscopic radical nephrectomy for 29 renal cancer patients. The indications for the radical nephrectomy were cases of T2 tumor stage or lower without evidence of lymphadenopathy or renal vein involvement. Patients included in the study were not candidates for partial nephrectomy (ie, localization in hilum, significant involvement of pelvicalyceal, tumor size), or the patient decided to undergo a radical procedure despite the selective indications for partial nephrectomy. In the latter cases, the patient decided between a laparoscopic partial or radical nephrectomy after a comprehensive discussion. If the patient decided to undergo the radical procedure, the possibility of a laparoendoscopic single-site radical nephrectomy was proposed. A control group included 29 age- and gender-matched patients with renal cell carcinoma of comparable cancer stage and tumor size who underwent conventional laparoscopy.
Outcomes of the 2 groups were compared retrospectively, including operation time, blood loss, duration of postoperative hospitalization, drainage volume, and complications.
Ethical considerations
All patients provided signed informed consent to participate in this study after the surgeons explained the procedure. The institutional review board of the Chinese PLA General Hospital reviewed the study protocol and approved the study.
Surgical Procedure Using the Self-Made Single-Port Laparoscopic Device
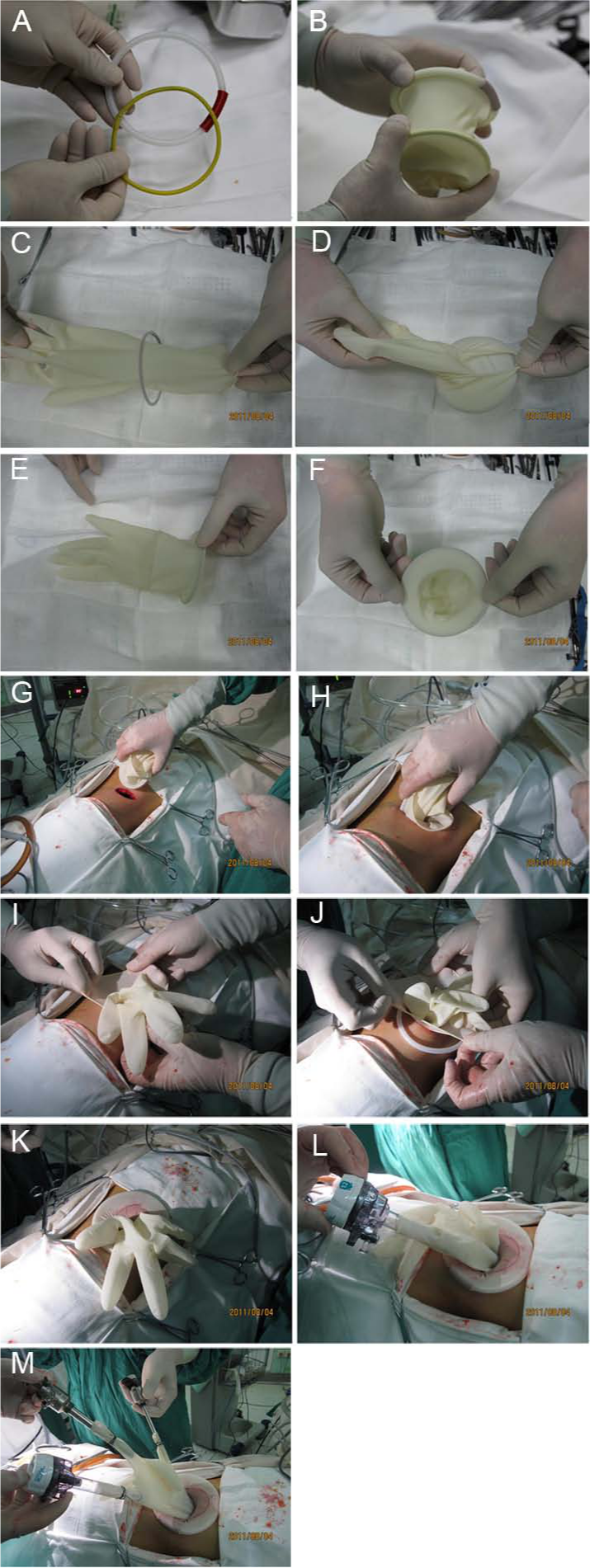
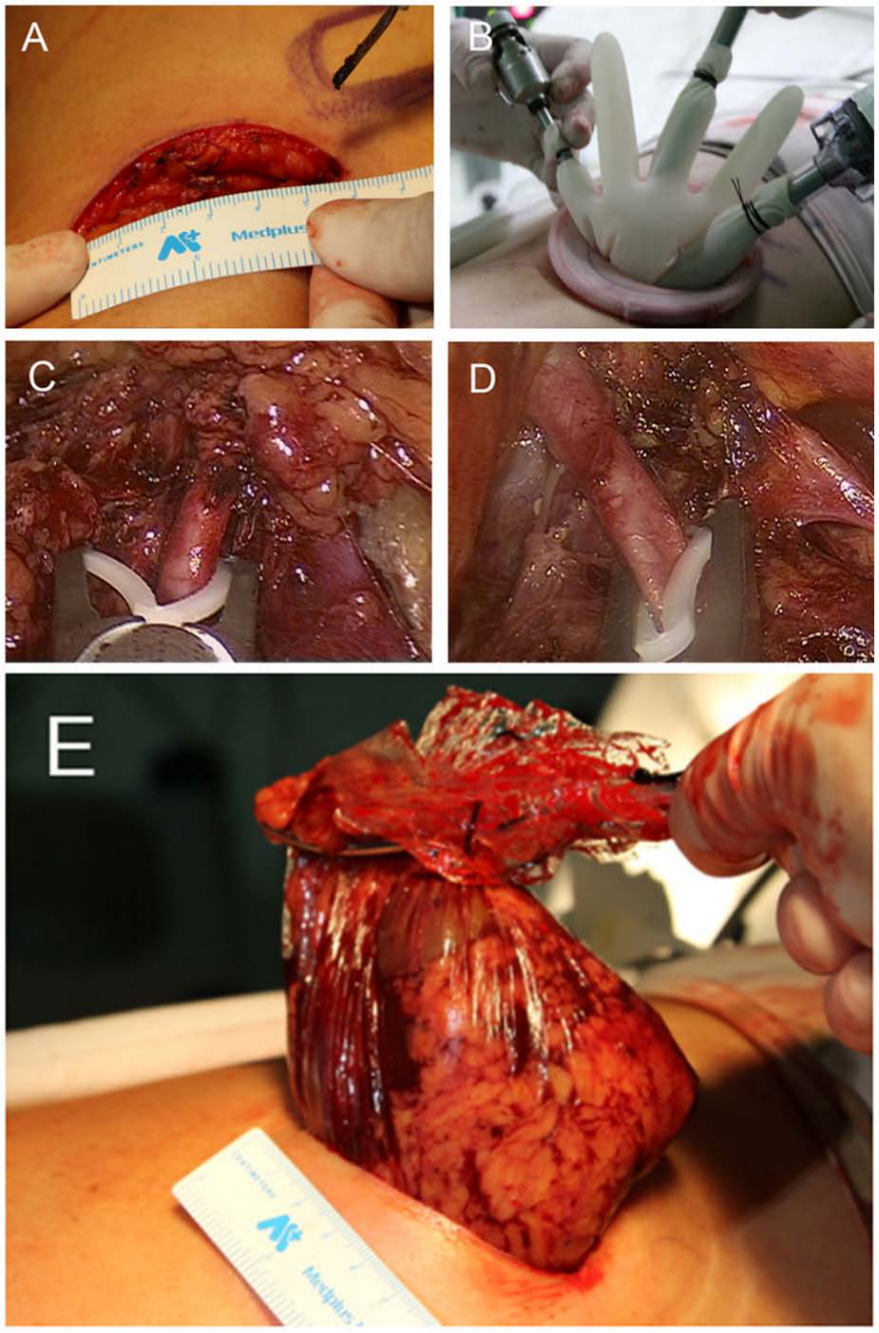
For each single-site laparoendoscopic surgery, the patient was placed in a lateral decubitus position after general anesthesia. An incision 1.5 to 2 cm in length was made anteriorly along the 12th rib, from its intersection with the posterior axillary line. The muscle layer and fascia lumbordorsalis were dissected using a large curved forceps. The incision was expanded with the index finger, pushing the peritoneum forward. Then, the finger guided a large curved forceps delivering the self-made surgical-glove dilation balloon into the retroperitoneal cavity. About 600 to 800 mL of air was used to dilate the balloon, extending the incision about 5 to 6 cm anteriorly and inferiorly, which allows intact removal of most specimens. Larger kidneys sometimes require extending the incision up to 7 cm. The incision was retracted and the extraperitoneal adipose tissue was removed as much as possible. Sharp dissection was carried out between the posterior renal fascia and the psoas muscle, and the posterior perirenal space was dissected by balloon dilation. Two self-made control rings 9 cm in diameter were placed into the operative site. The inner ring consisted of a hard guide wire and a percutaneous nephrostomy (PCNL) guide-wire sheath, and the outer ring consisted of a thick Amplatz guide-wire sheath (Cook Urological, Inc, Spencer, IN; Figure 1A-F). The 2 control rings and a size “8” powderless glove made up 1 single-port multichannel manipulation device (Figure 1G and H ). The end of the glove’s middle finger was cut off, and a trocar was placed into it and fixed (Figure 1I-M). CO2 insufflation was carried out, and the laparoscope was inserted to observe the operation space. A 12-mm trocar and a 5-mm trocar were placed in the glove’s thumb and little finger to insert conventional laparoscopic instruments and carry out retroperitoneal laparoscopic radical resection (Figure 2). Radical nephrectomy was done in the same manner as conventional laparoscopic nephrectomy. The resected kidney and adipose capsule were put into a self-made specimen bag, the instruments and glove were removed, and the specimen was taken out through the single incision serving as operation channel (Figure 2E). The incision was sutured routinely.
Instruction for self-made single-port instrument
Retroperitoneal single-port multichannel radical nephrectomy
Statistical Analysis
Comparability among the 2 groups was analyzed using independent 2-samples t test for continuous variables; Mann–Whitney U test was used for skewed distribution of data. Data are presented as a mean ± standard deviation or median (interquartile range) for continuous data. Chi-square/Fisher’s exact test was applied to determine the difference between the 2 groups for categorical variables, and data are displayed as numbers (percentages). All statistical assessments were 2-sided and evaluated at the .05 level of statistical significance. Statistical analyses were performed using SPSS 15.0 statistics software (SPSS Inc, Chicago, IL).
Results
Patients’ Demographic and Clinical Characteristics
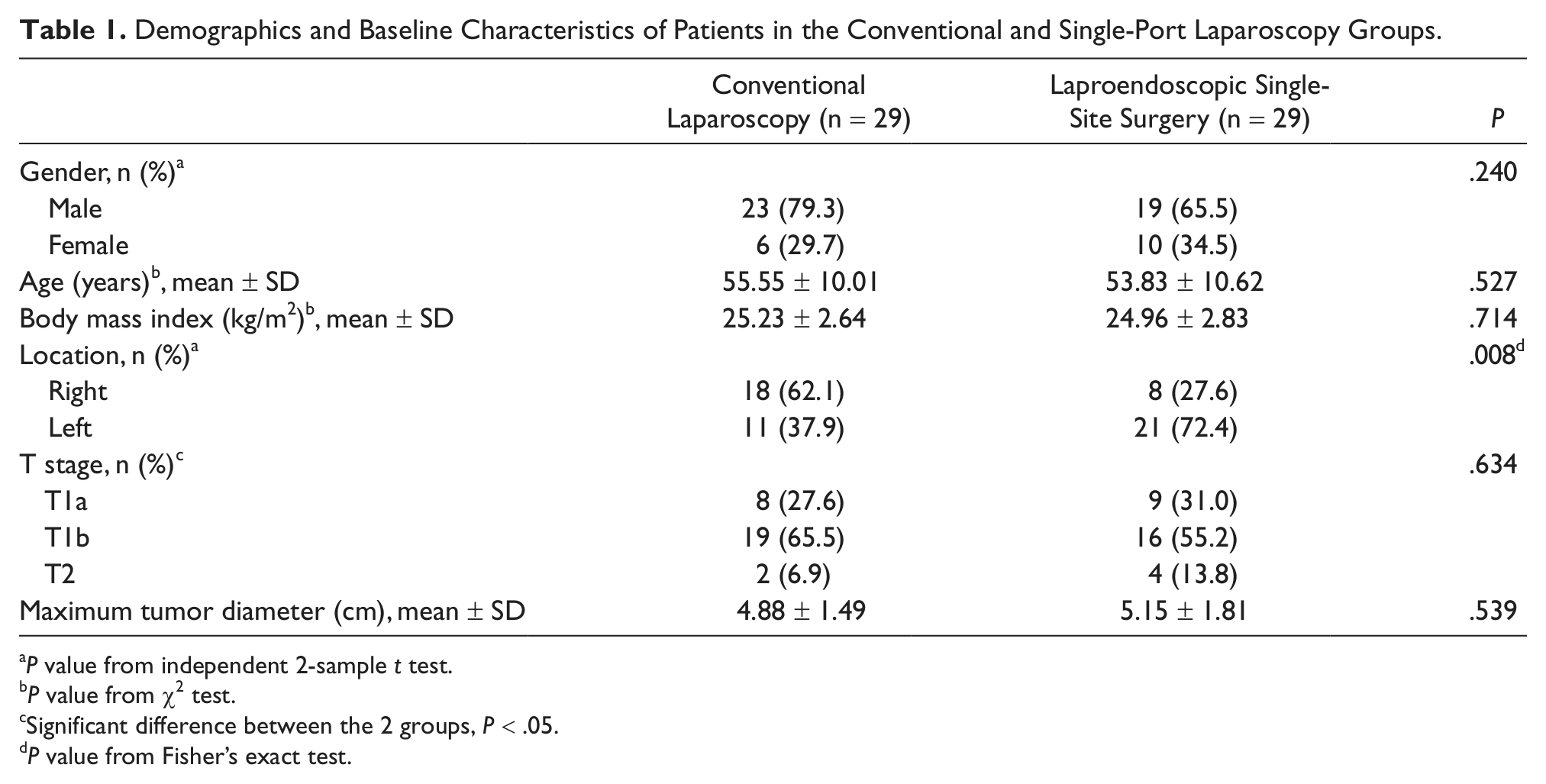
A total of 29 patients with renal cancer underwent retroperitoneal laparoendoscopic single-site radical nephrectomy using a self-made, single-port device. A control group of 29 patients with renal cancer underwent conventional laparoscopy. The laproendoscopic single-site surgery group included 19 males (65.5%) and 10 females (34.5%) with a mean age of 53.83 ± 10.62 years (ranging from 30 to 78 years). The conventional laparoscopy group included 23 males (79.3%) and 6 females (29.7%) with a mean age of 55.55 ± 10.01 years (ranging from 39 to 77 years). Basic demographic and baseline characteristics of both groups are described in Table 1. No significant differences in age, gender, body mass index (BMI), T stage, and maximum tumor diameter were found between the 2 groups (P > .05). However, there was a statistically significant difference in the location of renal cancer between the 2 groups (P = .008).
Demographics and Baseline Characteristics of Patients in the Conventional and Single-Port Laparoscopy Groups.
P value from independent 2-sample t test.
P value from χ2 test.
Significant difference between the 2 groups, P < .05.
P value from Fisher’s exact test.
Procedural Aspects: Self-Made Single-Port Laparoscopic Device
Single-port multichannel retroperitoneal laparoscopic radical nephrectomy was performed successfully for 29 cases in the present study. There was no significant air leakage from the self-made instruments, no channels were added during surgery, and there was no conversion to open surgery. Mutual interference was noted between the conventional laparoscope and the manipulation instruments located inside and outside the abdominal cavity. For intraoperative convenience, we noted that the assistant holding the mirror should stand on the same side as the surgeon. A few minutes after starting the operation, the surgeon and the assistant can adapt as needed to the procedure. Relatively large range of activity was observed in the 2 manipulation channels and 1 laparoscopy channel fixed to the 3 fingers of the glove. The observation range of the single laparoscope was larger than that of the conventional retroperitoneal laparoscope. However, the visual field of the 3-point coordinated manipulation was smaller than that of the conventional retroperitoneal laparoscope. No significant difficulty was encountered during management of the renal pedicle. Manipulation of instruments was difficult when treating the lateral side of the upper pole of the kidney. Activity of the 2 manipulation instruments and the laparoscope was better than that of the conventional laparoscope during treatment of the lower pole of the kidney and the ureter. In 4 cases with larger kidneys, the incisions were extended 1 to 2 cm for removing the specimens, making the final incisions 5 to 7 cm in length.
Intraoperative Data and Surgical Outcomes
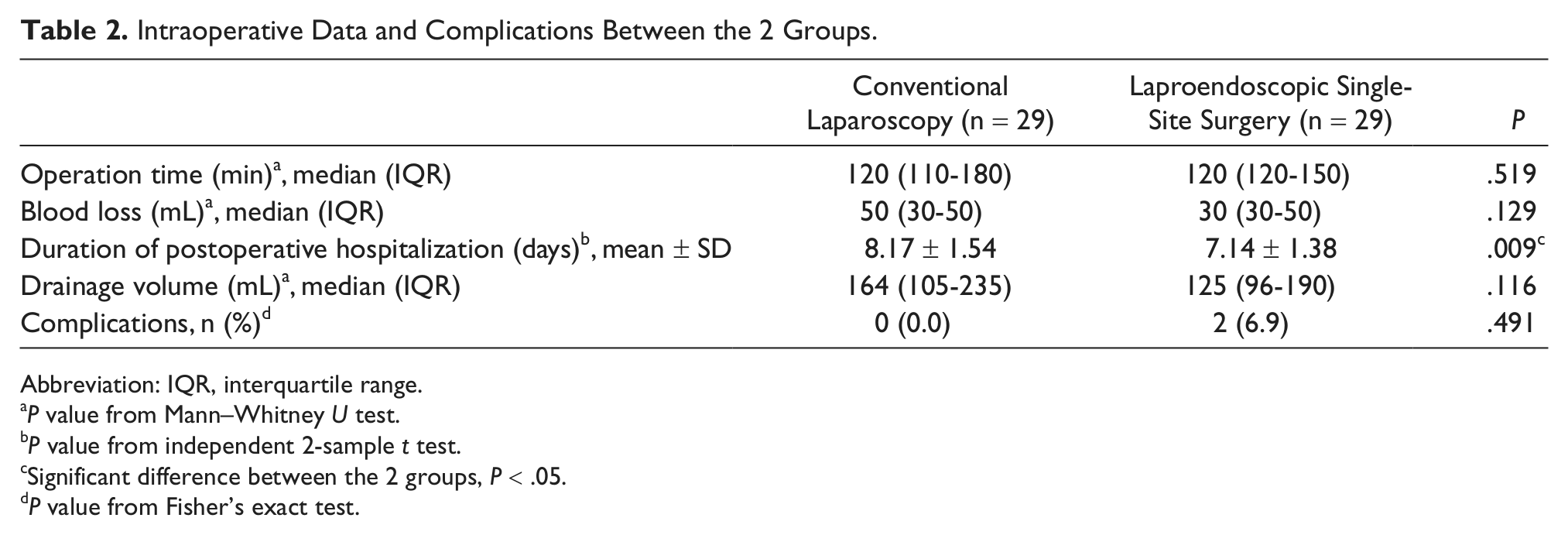
Table 2 shows the comparison of intraoperative data between the single-port and conventional laparoscopy groups. Patients receiving LESS had significantly shorter duration of postoperative hospitalization than those who received conventional laparoscopy (7.14 ± 1.38 days vs 8.17 ± 1.54 days, P = .009). No significant differences were found in blood loss, drainage volume, or complications between the 2 groups. Although there were no significant differences in complications between groups (P = .491, Table 2), 1 patient in the single-site laparoendoscopic group had atrial fibrillation and 1 patient had delayed wound healing of incision site.
Intraoperative Data and Complications Between the 2 Groups.
Abbreviation: IQR, interquartile range.
P value from Mann–Whitney U test.
P value from independent 2-sample t test.
Significant difference between the 2 groups, P < .05.
P value from Fisher’s exact test.
In the single-site laparoendoscopic group, patients started ambulation 1 to 2 days after surgery and were discharged 5 to 7 days after surgery. Intraoperative peritoneal rupture occurred in 1 case, and surgery was continued after treating it with surgical clamps. In 2 cases with stage T2 tumors, ipsilateral adrenal resection was performed simultaneously. During the operation, an accessory renal artery was found at the upper pole of the kidney in 3 cases, which was managed properly. The mean weight of the specimens was 409.09 g, ranging from 290 to 632 g. Pathological findings confirmed that all patients had renal clear-cell carcinoma.
Discussion
In the present study, single-port multichannel retroperitoneal laparoscopic radical nephrectomy was performed successfully for 29 renal carcinoma cases. Clinical data, intraoperative data, and surgical outcomes were compared with those of an equal number of age- and gender-matched renal carcinoma cases receiving conventional laparoscopic nephrectomy. Our main findings were that the LESS group had significantly shorter duration of postoperative hospitalization than the conventional laparoscopy group. Although there were no significant differences in age, gender, BMI, T stage, and maximum tumor diameter between the groups, the differences in renal cancer location between the 2 groups was statistically significant. There also were no significant differences in complications between the 2 groups, although 1 patient in the single-site laparoendoscopic group had atrial fibrillation and 1 patient had delayed wound healing of incision site. Overall, retrospective review of the single-site laparoendoscopic surgery using the easily assembled, self-made, single-site device showed it to be comparable in advantages to conventional laparoscopy but with the additional advantages of a single incision through which the resected specimen could be extracted, resulting in the excellent cosmetic result of only a single scar.
We designed a new method of performing retroperitoneal laparoscopic radical nephrectomy using the single incision for instrument manipulation and for removing the specimen. Our procedure relied on a self-made, single-port device that allowed efficient use of the conventional laparoscope and convenient manipulation of instruments through the single incision made for removing the specimen. It also eliminated the other 2 incisions used during conventional retroperitoneal laparoscopic surgery, preserved the advantages of the retroperitoneal laparoscope through easy management of the renal pedicle and reduced disturbance to the abdominal cavity while also reducing surgical trauma and the number of scars.
When applying the self-made device for radical nephrectomy, we performed balloon dilation at the space between the psoas muscle and the perirenal fascia for our initial cases. Later we discovered that performing laparoscopic dissection of the space between the psoas muscle and the perirenal fascia after the first dilation was easier and more convenient, and most cases in the present study were treated by single balloon dilation via the retroperitoneal cavity.
Characteristics of Self-Made Instruments
Surgeons, as noted above, are constantly looking for innovative ways to reduce the number and size of incisions and to improve the performance of laparoscopic procedures, which leads to development of homemade instruments. Lee and Lee 9 used a homemade single-port device for urological surgery, including 3 cases of radical nephrectomy. The device used a wound retractor and a powderless surgical glove; the wound retractor was inserted into the umbilicus incision site, and the glove covered the upper part of the retractor ring while the 3 fingers of the glove were cut off to insert 3 trocars, which were immobilized with sutures. 9 Another device was constructed in a similar manner for use in laparoendoscopic nephrectomy, although the fingers of the glove were secured to the end of 3 trocars with rubber bands and fixed to the outer ring of the wound retractor. 7 Outcomes with the use of these 2 similar instruments included minimal scarring without the need for extraumbilical incisions, reduced hospital stay, and no complications.7,9 In this study, materials used in the self-made device were inexpensive, readily available in any operating room, and construction of the device was simple. The inner and outer rings were self-made and are not commercially available. The inner control ring is made of a PCNL guide-wire sheath that has appropriate elasticity, which increases the ease and convenience of loading and unloading. The outer control ring is made using an Amplatz guide-wire sheath (Cook Urological, Inc, Spencer, IN). Diameters of the inner ring and outer ring are 9 cm, which can support the wrist area of a size “8” glove and prevent it from slippage and air leakage. No suture is needed for fixation and the tension of the inner and outer rings, and the glove allows it to be stably fixed on the manipulation channel.
Flexibility, Operative Space, and Intraoperative Instrument Manipulation
One advantage of homemade instruments using powderless 5-finger gloves is that the number and size of instruments can be varied easily for the specific operation or to satisfy the surgeon’s preference, which allows greater flexibility than most commercial laparoscopic port systems. 7 Additionally, as in earlier reports,7,9 the resected specimen can be easily extracted through one of the fingers of the device without using a separate entrapment bag. Although surgical gloves appear to be fragile, they are flexible and ductile, performing competently without breakage during the surgical procedures. In 80 urological surgeries, we had only 1 occurrence of splitting of the glove material, which required changing the self-made device. This repair took about 5 minutes to accomplish without affecting the procedure or the patient.
Intraoperative manipulation of instruments through the single incision has been mainly favorable,8-11 and it also has been reported to require the ambidexterity of the surgeon when 2 instruments must be used simultaneously. 12 In the present study, we used a range of instruments, including a 10-mm 30° rigid laparoscope, dissecting and grasping forceps, harmonic scalpel, bipolar coagulator forceps, and scissors, which were all inserted via the single port through the same skin and fascial opening and maintained in stable position for the duration of the surgery.
Manipulation space was carefully considered as we gained experience with our initial cases. Because the retroperitoneal laparoscopic operation needs sufficient manipulation space, sufficient balloon dilation is necessary. Therefore, retroperitoneal balloon dilation should be carried out using a small incision at first as in conventional laparoscopy, which will make later manipulation easier. Removal of extraperitoneal fat through the incision is also very important for successful surgery and a relatively large volume of fat tissue can be removed through the open incision. After removal of the extraperitoneal fat tissue, the initial space for the manipulation increases; the surgical field becomes clear; the peritoneum, lateral conal fascia, and psoas muscle can be identified easily; and the next steps can be carried out smoothly. Also, additional space can be produced by dissecting the interval between the posterior renal fascia and the psoas muscle through the incision, and then balloon dilation can be performed for the second time. The volume of the balloon dilation ranges from 100 to 150 mL. In the present study, the initial experience of 29 cases demonstrated that the removal of the fat tissue and the second dilation will increase the ease of later manipulation. Our initial experience with this self-made single-port multichannel instrument showed that the range of motion was relatively large in the 2 manipulation channels; and in the laparoscope channel fixed to the 3 fingers of the glove, the observation range of a single laparoscope was greater than that of the conventional retroperitoneal laparoscope. However, the observation range of 3-point coordinate manipulation was less than that of the conventional retroperitoneal laparoscope. There was no difficulty in the treatment of renal pedicle. In 3 cases, the tumor was located near the dorsal side of the renal hilum, but treatment of the renal pedicle was not significantly difficult in these cases. However, the application of this new homemade instrument was limited when managing the lateral side of the upper pole of the kidney. The treatment of the lower pole of the kidney and the ureter was easier compared with the conventional retroperitoneal laparoscope.
Patient selection may be an important consideration in laparoscopic single-site surgery. Mir et al 13 applied laparoscopic single-site surgery for 30 nephrectomies and compared outcomes and morbidity with those of 34 conventional laparoscopic nephrectomies, reporting similar complication rates and outcomes between the 2 groups. 13 Investigators suggested that patient selection was especially important and that younger patients with lower BMI and nononcologic indications were the more appropriate candidates for laparoscopic single-site nephrectomy. 13 Ramen et al 14 compared 11 laparoscopic single-site nephrectomies and 22 conventional laparoscopic nephrectomies and reported no differences in median operation time, length of hospital stay, and complications between the 2 types of surgery. 14 However, some patients had nonfunctioning kidneys and some had renal cell carcinoma, and some intact surgical specimens were removed through an extension of the single umbilical incision, which limits the results of comparison and conclusions regarding the benefits of the laparoscopic single-site nephrectomies. The current study included patients with stage T1 and stage T2 renal cell carcinoma. BMI and the weight of resected specimens were similar to those of the cases undergoing conventional retroperitoneal laparoscopy. Our initial experience suggests that the self-made single-port multichannel retroperitoneal laparoscopic radical nephrectomy is safe and feasible. There is no increased difficulty of manipulation, and the operation time, though longer than desired, will be expected to gradually decrease along with the increase of surgery cases and accumulation of experience. Because of the unique incision serving as the surgical manipulation channel and the channel for removing the specimen, the number of manipulation ports in the conventional retroperitoneal laparoscopy was reduced from 3 to 1, and the surgical trauma and scarring are also reduced. The cosmetic effect is improved, which also encourages patients to accept this kind of surgery. A skilled surgeon can substitute our single-port retroperitoneal technique for the conventional procedure.
This study has certain limitations, especially the small sample size and that it is a single-institution survey. Data on postoperative pain status were not collected with other postoperative measures. Also, because the Chinese population generally has lower BMI, further investigation of the effectiveness of the single-site, laparoendoscopic radical nephrectomy is needed for patients with higher BMI. Further investigation of other applications of our technique with single-site laparoendoscopic surgery should be explored, including partial nephrectomy and live-donor nephrectomy.
Conclusions
Retroperitoneal laparoscopic radical nephrectomy using our self-made single-port, multichannel device appears to be a feasible, safe, and low-cost surgical strategy. Recovery time is less than that of conventional laparoscopic surgery. Cosmetic results are good, with only 1 scar postoperatively. Average operation time is expected to decrease with increasing cases and experience. The noncommercial, self-made device can be easily reproduced and widely used in developing countries.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.