
Abstract
Introduction. Component separation (CS) has become a viable alternative to repair large ventral defects when the fascia cannot be reapproximated. However, the impact of transecting the external oblique to facilitate closure of the abdomen on quality of life (QOL) has yet to be investigated. The study goal was to investigate QOL and outcomes after standard open ventral hernia repair (OVHR) versus CS for large ventral hernias. Study design. Prospective data for all CSs were reviewed and compared with matched OVHR controls. All defects were 100 to 1000 cm2 in size and repaired with mesh. Comorbidities, complications, outcomes, and Carolinas Comfort Scale (CCS) scores, were reviewed. Results. Seventy-four CS patients were compared with 154 patients undergoing standard OVHR with similar defect sizes. Age (56.7±13.0 vs 54.7 ± 12.3 years, P = .26), defect sizes (299 ± 160 vs 304 ± 210cm2, P = .87), and BMI (32.7 ± 6.9 vs 34.2 ± 9.0 kg/m2, P = .26) were similar in both groups, respectively. There were no differences in major postoperative complications (P = .22), mesh infections (P = 1.00), wound infections (P = .07), or hernia recurrence (P = .09), but wound breakdown increased after CS (10% vs 1%, P < .001) as did seroma interventions (15% vs 4%, P = .005). Postoperative CCS scores were similar at 1 month (P = .82) and 1 year (P = .14). Conclusions. In the first comparative study of its kind, it is found that patient undergoing CS with mesh reinforcement had equal short- and long-term QOL outcomes compared with similar patients who underwent standard OVHR. Whereas wound breakdown and seroma formation are higher, the overall complication, mesh infection, and recurrence rates are similar.
Keywords
Introduction
Every year, 4 million laparotomies are performed in the United States. 1 Fascial breakdown with hernia formation is a common complication, which leads to approximately 105 000 ventral hernia repairs (VHRs) annually. 2 The 2 major predisposing factors for hernia occurrence after laparotomy are wound infection and obesity, which can increase hernia rates up to 40%.3,4
Hernia repair has evolved dramatically over the past 40 years. Previously, recurrence after primary repair was an accepted and common complication until the advent of meshes, which drastically reduced recurrences from more than 50% down to as low as 2%.1,5-8 Obesity, abdominal soft-tissue infection, staged management of the prolonged open abdomen, and suboptimal mesh selection 9 has led to larger and more complex abdominal defects, where fascial closure becomes difficult or impossible. As a result, patients with large defects or a loss of abdominal domain often receive a prosthetic bridge repair, which eliminates the gap in the abdominal wall but may result in a less functional or physiological abdominal wall. Lack of native, innervated tissue may lead to diminished mobility and can result in increased mesh sensation and impaired dynamics of the trunk while sitting, standing, bending, or performing normal activities of daily living. Biological grafts have also been utilized, but they have a high rate of recurrence resulting from mesh eventration.10-14
The value of primary fascial closure in large ventral defects and loss of abdominal domain has been extensively documented in the surgical literature.15,16 Closure of the muscular abdominal wall helps improve overall patient function and quality of life (QOL) and reduce mesh-related complications and recurrence rates. 17 With large ventral hernias, reapproximation of the fascia is not feasible, and when performed, closure under great tension can lead to a prohibitively high intra-abdominal pressure. Intra-abdominal hypertension may manifest immediately as the inability to wean from mechanical ventilation after anesthesia, urinary and gastrointestinal dysfunction, and even abdominal compartment syndrome with decreased organ perfusion and impaired venous return. In the long-term, excessive fascial tension carries a high risk of hernia recurrence as a result of facial separation. Distant tissue graft transfer is time-consuming, and outcomes are often poor. Myofascial advancement flaps or component separation (CS) was first described in 1977 by Mathes and Bostwick 18 but was not popularized until 1990 by Ramirez et al. 19 They demonstrated that the external oblique muscle can be separated from the internal oblique in a relatively avascular plane, and the rectus muscle with its overlying rectus fascia could be elevated from the posterior rectus sheath. This led to the notion that large abdominal wall defects can be reconstructed with functional advancement of abdominal wall components without the need for free-tissue transfer flaps. Since then, multiple studies have demonstrated that CS is a safe and effective option for the repair of large ventral hernias.20-24
Initially, CS became popular in patients with large ventral hernias and contaminated wounds. Surgeons believed that they could eliminate the need for a prosthetic mesh by achieving primary fascial closure using CS. Subsequently, CS alone was found to lead to very high recurrence rates, with studies demonstrating rates reaching 53%.9,25,26 Since then, reinforcement of the midline repair with mesh, either synthetic or biological, has gained popularity. In a clean, large VHR, rather than using the mesh as a “bridge,” CS with midline fascial closure over synthetic mesh reinforcement became fairly standard in the 18 000 CSs performed annually in the United States from 2006 to 2008.27 -29 This approach not only affords improved mechanical function of the abdominal wall but importantly also provides an excellent infection barrier between the mesh and the subcutaneous tissues. Although cellulitis and superficial wound complications are common, they are often easily treated as long as the overlying fascia remains intact and the mesh remains sterile. There is no evidence to suggest that CS has a negative impact on the fascial barrier function.
With improvements in the understanding of the operative techniques for hernia repair and the use of mesh reinforcement of the abdominal wall, an overall reduction in hernia recurrence has been documented. With this, a strong recommendation has been made to eliminate recurrence as the sole marker of a successful hernia repair and to include QOL as a major outcomes measure.30-33 Despite the major physical changes required in performing a CS, including transecting muscle and the strongest fascial layer (external oblique) of the abdomen, 34 important QOL issues in CS patients have not been addressed, including pain, movement, and activity limitations. Whereas studies suggest that CS patients may have persistent pain and decreased functionality postoperatively, 35 no QOL studies have addressed this topic specifically or in a comparative manner. Indeed, the importance of performing a formal comparison to standard open ventral hernia repair (OVHR) to evaluate these issues, especially given the rising popularity of CS, cannot be understated. Such analysis would provide surgeons and patients with a better understanding of the appropriate use of CS, especially when weighing the risks and benefits during the decision-making and consent process.
We undertook this study to evaluate the outcomes and QOL in patients with large defects undergoing non–perforator-sparing CS versus standard OVHR.
Methods
After obtaining institutional review board approval, prospectively collected data from September 2005 to July 2010 were reviewed. All patients who underwent OVHR via non–perforator-sparing CS or the standard approach, with defects ranging from 100 to 1000 cm2, were examined. Patients undergoing unilateral CS, endoscopic CS, and laparoscopic VHR were excluded as were patients younger than 18 years and those with concurrent soft-tissue or mesh infections or enteric fistulas. Defect size was determined intraoperatively after previous mesh excision or fascial debridement to give the most accurate determination of distance to reapproximation. All patients to be included in the study consented preoperatively in the office visit prior to surgery. All data were entered via blinded data collectors who had no knowledge of the study components. Demographics of the patient population as well as defect size, previous hernia repairs, comorbidities, postoperative complications, and QOL using the Carolinas Comfort Scale (CCS) scoring system were assessed.
The CCS is a well documented and proven hernia specific questionnaire for patients undergoing hernia repair with mesh. It measures pain, movement limitations, and the sensation of mesh for 8 different daily activities.31,36,37 These activities include lying down, bending over, sitting up, performing activities of daily living, coughing/breathing, walking, walking upstairs, and exercising. Each question is answered on a scale of 0 to 5, with 0 = no symptoms and 5 = disabling symptoms. These answers are totaled and can range from 0 to 115 or can be averaged for each individual activity or symptom (range 0-5). It has been demonstrated to be a more effective determinant of QOL and a more patient-friendly survey than the well-established SF-36. 37
All patients were placed in a supine position on the operating table. After induction of anesthesia, the abdomen was prepped and draped widely. A Foley bladder catheter was placed. Previous scar excision was performed, and the subcutaneous tissues were dissected with cautery to the hernia defect. After identification of the hernia, the sac was entered, and hernia contents were reduced back into the abdomen. Adhesiolysis was performed at the hernia site as well as to the abdominal wall circumferentially. A preperitoneal approach for mesh placement was performed as previously described. 38 The peritoneum was dissected from the anterior abdominal wall to the bilateral paracolic gutters, to the pubis, and beyond the xiphoid. The peritoneum was then closed with a running absorbable suture to provide a barrier between the mesh and the intra-abdominal contents. A determination was made at this point concerning abdominal wall closure. If the fascia could be approximated primarily without increasing peak airway pressures to >30 mm pressure or without creating undue tension on the closure, a polypropylene mesh with at least a 7-cm defect overlap, if available, was placed in the preperitoneal space and secured using interrupted permanent transfascial sutures.
For patients in whom the fascia could not be primarily reapproximated over the mesh, a CS was performed as described previously by Ramirez et al. 19 After dissection of the preperitoneal space, cautery was utilized to dissect out the subcutaneous space to the midaxillary line. Cautery was also then utilized to cut the external oblique aponeurosis (Figure 1) lateral to the rectus sheath. This incision was extended as needed from the fascia just overlying the ribs, down to the level of the anterior superior iliac spine. Release of the external oblique fascia was then repeated on the opposite side. Posterior rectus sheath release was performed by incising the sheath 2.5 cm lateral to the linea alba. The posterior rectus sheath was incised from the xiphoid to the arcuate line and repeated on the opposite side. The mesh was inserted as previously described, with the intent to place it lateral to the cut edge of the external oblique. The mesh was secured using transfascial monofilament nonabsorbable sutures. All patients received a lightweight polypropylene mesh, with or without antiadhesive coating: UltraPro or Proceed (Ethicon Inc) and Bard Soft or Ventralight ST (C. R. Bard, Cranston, RI).
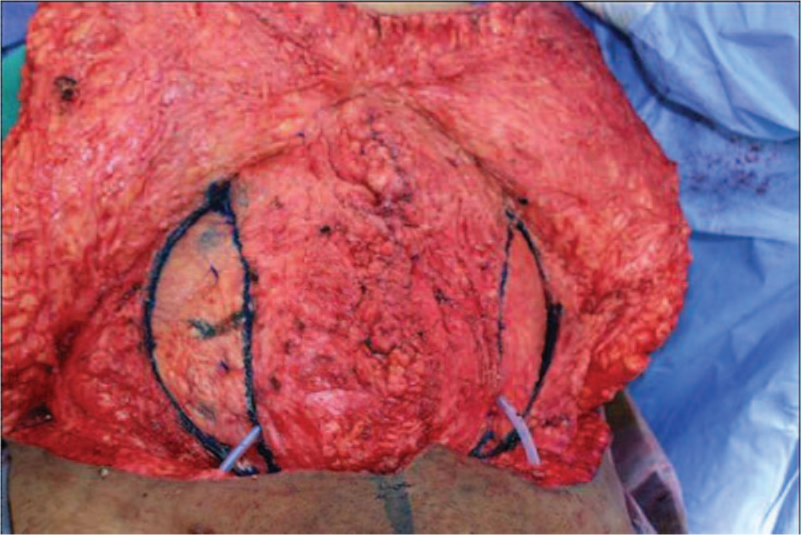
Intraoperative photographs of component separation.
Drains were then placed over the mesh while the anterior fascia was closed with a running, long-acting absorbable suture over the prosthetic with a long stitch technique. This, in effect, isolated the mesh from the subcutaneous space. The subcutaneous tissues were thoroughly irrigated. In most cases, 1 or 2 subcutaneous drains were placed over the fascia depending on the extent of subcutaneous dissection. The subcutaneous tissues were then closed with an interrupted dissolvable suture and the skin was closed using an absorbable subcuticular stitch or staples (Figure 2).

Preoperative and postoperative photographs of a patient undergoing component separation: before (left) and after (right).
Patients who underwent CS were matched to 154 patients with standard OVHR who had defect sizes from 100 to 1000 cm2. Standard statistical procedures were carried out for defect size, age, and BMI, and a 2-tailed t test was performed and confirmed similarity between groups. All subsequent data underwent standard statistical analysis. For data measured on the interval scale, the Student’s t test was used. If the data were ordinal or not normally distributed, the Wilcoxon rank sum test was used. For nominal data, the χ2 or Fisher’s exact test was used. A 2-tailed P value of less than .05 was considered statistically significant.
Results
Demographics
A total of 74 patients undergoing CS met inclusion criteria for analysis and were matched to 154 patients undergoing standard OVHR. Demographics are listed in Table 1. Our patients were more commonly female in each group (54.1% vs 61.7%, P = .31) with similar age (56.5 ± 13.0 vs 54.8 ± 12.3 years, P = .35) and BMI (32.8 ± 7.0 vs 34.2 ± 9.0 kg/m2) in the CS and OVHR groups, respectively. Hernia defects were of similar size (299 ± 161 vs 301 ± 206 cm2, P = .95). Approximately 60% of procedures were performed on recurrent hernias (59.5% vs 66.2%, P = .38), with the average patient having 2.36 ± 1.93 versus 2.09 ± 1.70 (P = .40) previous repairs, respectively, and a majority of these still had the mesh in place (54.1% vs 53.9%, P = 1.00). American Society of Anesthesiology (ASA) class was similar as well (2.5 ± 0.6 vs 2.5 ± 0.6, P = .52).
Demographics.
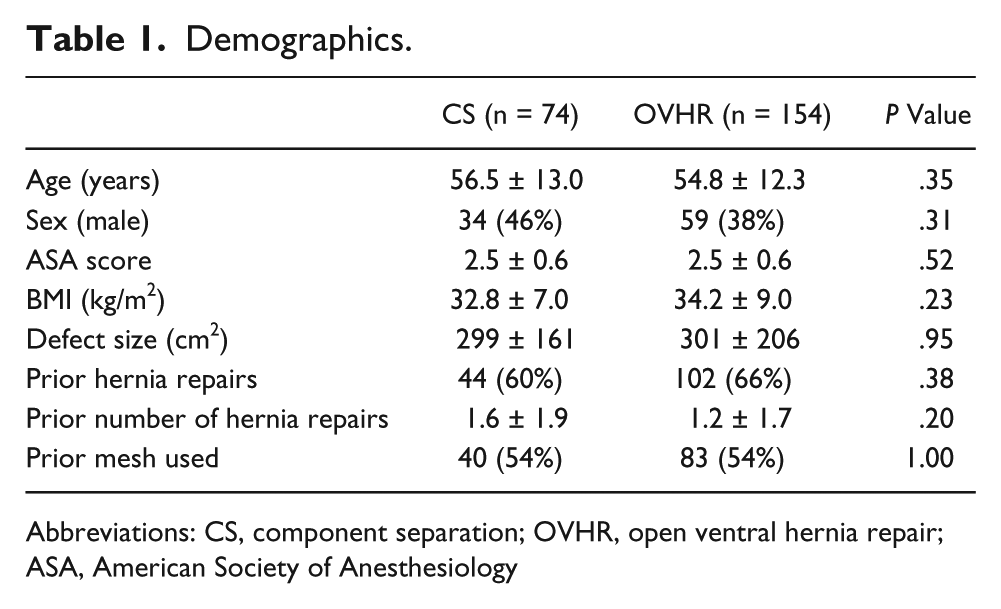
Abbreviations: CS, component separation; OVHR, open ventral hernia repair; ASA, American Society of Anesthesiology
Complications
Mean hospital length of stay was 8.2 ± 7.1 and 8.8 ± 11.8 days (Table 2) in the CS group and OVHR groups, respectively (P = .69). Wound complications were the most common complications and were seen more frequently in the CS group. Interventions for seroma formation were the most common wound complication, with 14.9% in the CS group versus only 3.9% in the OVHR group (P = .005). Also, 8 CS patients (10.8%) developed some wound breakdown (defined as simple skin dehiscence) versus only 1 patient with standard repair (0.7%). Wound infections and hernia recurrences were similar between groups. We found that 12 major complications were seen in 7 patients (9.5%) with CS versus 25 major complications in 22 patients (14.3%) with OVHR (P = .22). The most common major complication in the OVHR group was acute renal dysfunction (n = 9, 5.8%) and respiratory failure (n = 8, 5.2%), all of which resolved, whereas patients with CS most commonly experienced a pulmonary embolism (n = 3, 4.1%). One patient in the CS group developed a mesh infection versus 2 in the OVHR group (P = 1.0), and there were no statistical differences between groups for any major complication.
Complications Comparing CS Versus OVHR.
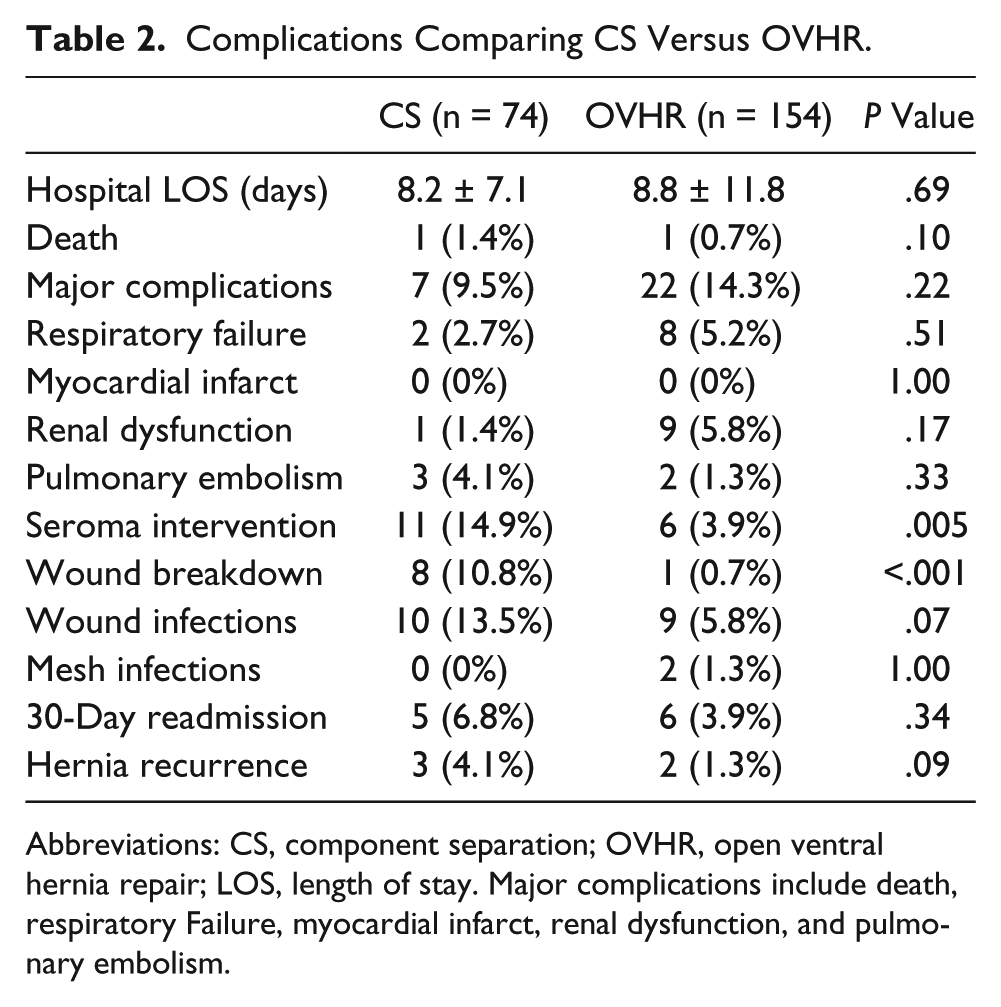
Abbreviations: CS, component separation; OVHR, open ventral hernia repair; LOS, length of stay. Major complications include death, respiratory Failure, myocardial infarct, renal dysfunction, and pulmonary embolism.
CS Pain and QOL Statistics
Immediate postoperative analgesia requirements (Table 3) were 172 ± 123 versus 179 ± 167 morphine equivalents, respectively (P = .78), with similar modes of narcotic administration. CCS symptom scores were compared for pain, movement limitation, and overall QOL (Table 4). At short-term follow-up (3-4 weeks), all 3 scores were statistically similar to preoperative scores, with overall QOL scores of 2.62 ± 1.25 preoperatively versus 2.62 ± 0.88 by 1 month (P = 1.00). At long-term follow-up (average of 10.5 months; range = 7 months to 1 year), pain (preoperative, 2.59 ± 1.25 vs postoperative, 1.59 ± 0.78; P = .003), movement limitations (preoperative, 2.71 ± 1.27 vs postoperative, 1.82 ± 1.10; P = .02), and overall QOL scores (preoperative, 2.62 ± 1.25 vs postoperative, 1.71 ± 0.68; P = .002) had significantly improved.
In-Hospital Pain Management.
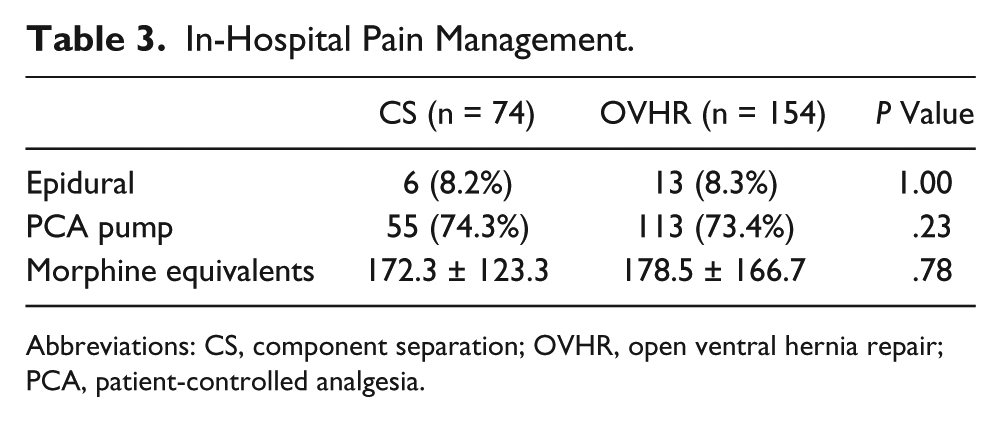
Abbreviations: CS, component separation; OVHR, open ventral hernia repair; PCA, patient-controlled analgesia.
Component Separation QOL Preoperatively Versus at Follow-up at Short Term and Long Term.
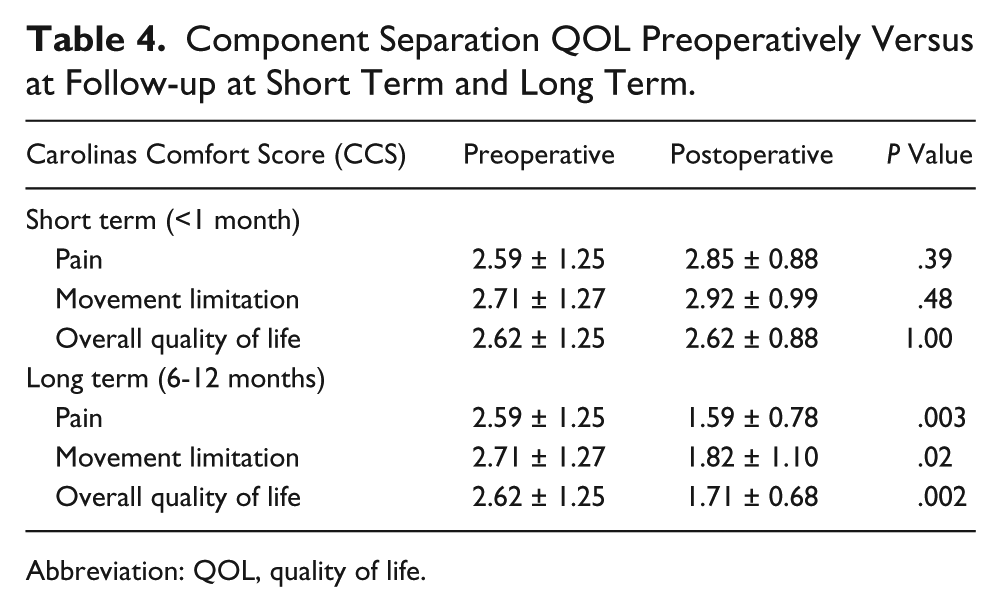
Abbreviation: QOL, quality of life.
CS Comparisons With Standard Hernia Repair
Paired analyses of postoperative CCS symptom scores were similar between the 2 groups (Table 5). Mesh sensation, pain, and movement limitations were all statistically similar between groups at both short-term and long-term follow-up. Overall QOL scores at short-term follow-up were 2.72 ± 0.86 versus 2.70 ± 1.01 (P = .82). These numbers similarly improved by long-term follow-up to 1.70 ± 0.60 versus 2.18 ± 1.28, respectively (P = .14).
QOL Comparison Between CS and OVHR at Short-term and Long-term Follow-up.
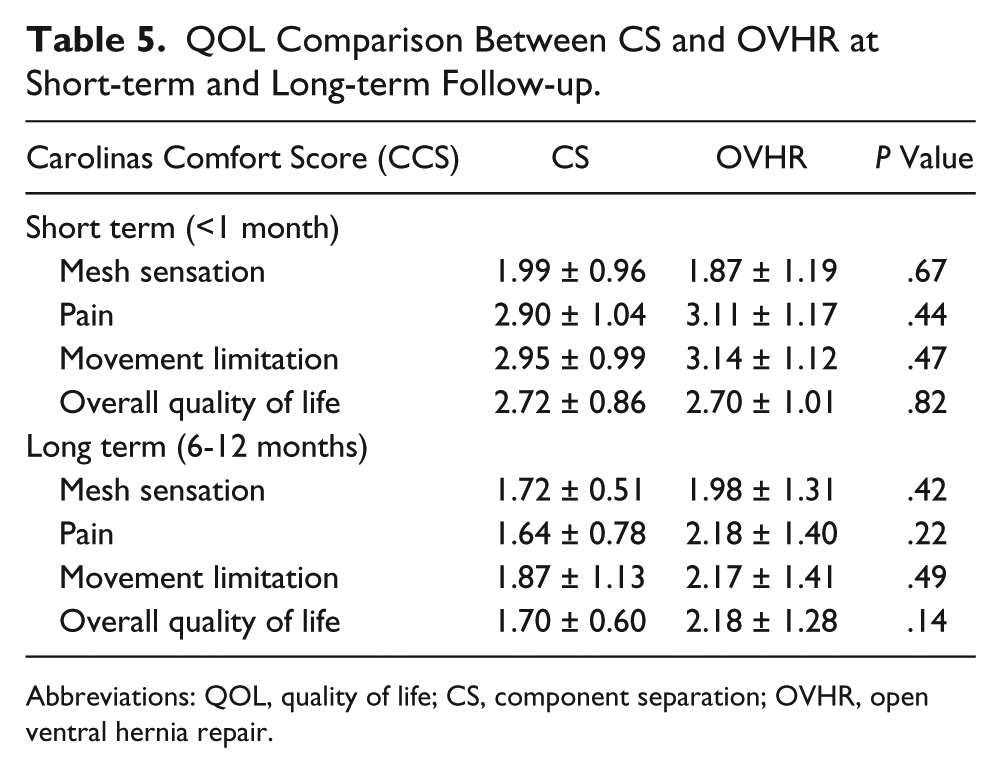
Abbreviations: QOL, quality of life; CS, component separation; OVHR, open ventral hernia repair.
Discussion
CS has become an increasingly more common procedure since it was popularized by Ramirez et al 19 in 1990. More than 18 000 CSs are performed annually in the United States, and up until this point, gathering recurrence data has been the main focus of clinical research. Reinforcement with mesh has been established as a superior operation, significantly reducing recurrence rates as it does for standard OVHR.9,39 Previously, patients with a large defect or tension on closure were relegated to a bridging mesh, which has been demonstrated to have higher recurrence and mesh infection rates. 40 Reapproximation of the rectus muscles to the midline reduces both problems by allowing closure of the fascia over the mesh, protecting the mesh from superficial wound infections and restoring abdominal wall integrity. 40 Although the consideration that abdominal muscle function is significantly improved by these techniques is worthwhile, objective evidence is lacking.
Although recurrence is an obviously important outcome, it is not the only goal of a successful hernia repair. Restoring function and integrity, preserving the vasculature and innervation, providing stable skin and soft tissue coverage, and improving overall QOL are just as important.33,41,42 CS should not be undertaken unless absolutely required, given that the subcutaneous dissection required in a majority of cases carries an increased risk of wound complications. This likely results in increased discomfort and obviously affects abdominal wall function, but to what extent is not known. Indeed, despite the enthusiasm for CS, the actual influence of this technique on patient QOL has not been studied objectively and reported in the literature. Concerns about movement limitations and postoperative pain and their effect on QOL are valid for any surgical procedure but especially pertinent in the case of CS where normal musculature is compromised to achieve the goal of rectus reapproximation. Subjective questionnaires have been used to gauge a patient’s relative happiness with a surgery; though helpful, they do not give surgeons quantitative data about functional and QOL impact using a validated metric that can be applied to subsequent surgical decision making.
The CCS is a hernia-specific QOL scoring system that has quickly become a widely accepted alternative to the generalized subjective questionnaires.31,37,43 It was developed to allow comparison of preoperative and postoperative outcomes and to compare the outcomes of different hernia repair procedures. CCS has been shown to demonstrate reproducibility, is preferred by patients, and has shown improved hernia QOL specificity when compared with the well-established SF-36. 37 It appears to have gained worldwide acceptance as the predominant QOL survey for hernia repair. Currently, it has been translated into 32 languages and is being used in 42 countries. The CCS provides the surgeon with a more objective assessment of subjective complaints such as pain, movement limitations, and mesh sensation.
In this study, the demographics and hernia-related factors of two patient populations were matched to reduce the possible impact on study outcomes by these factors. Important demographics, 25 such as BMI, gender, age, and number of repairs were similar among groups. Given the focus of this study, defect size was a major consideration in the group comparison. To qualify, hernias needed to measure at least 100 cm2. If the abdominal wall could be closed without significant tension, a primary closure over a preperitoneal mesh was performed. In those in whom the abdominal wall could not be closed without marked tension, a standard components separation was performed over a mesh placed in a preperitoneal location.
Overall, in-hospital major complication rates were similar between the two groups. Considering the effects of increased intra-abdominal pressure and its real possibility when repairing large hernias, pulmonary consequences and renal function were of particular interest in this study. The data demonstrated that there was no difference in abdominal pressure–related complications. The incidence of renal and pulmonary failure and pulmonary embolism were the same in both the CS and OVHR groups.
As expected, the extensive subcutaneous dissection required when performing a CS led to a significantly higher incidence of wound breakdown and seroma formation as compared with a standard OVHR. In the past, these complications and their unknown consequences on patient QOL have been the major arguments to avoid performing a CS during a VHR. Wound and mesh infection rates were not significantly different, but wound infections trended toward a higher incidence in the CS patients. The need for seroma intervention, aspiration, or drain placement was significantly increased following CS. The need for seroma intervention was 14% in these patients, which is similar to other reports of 14% to 21%.44,45 But whereas these other reports included only the operative or radiological interventions for seromas, the data in this study included bedside aspirations as well. The reduction in seroma-related problems is attributed to our use of talc applied to the subcutaneous tissues of CS patients just prior to closing, which began in January of 2009. In a previously reported study, we demonstrated significantly earlier removal of drains, fewer seromas, an 8-fold decrease in seroma interventions, and significantly fewer wound infections following the use of aerosolized talc in the subcutaneous space. 45 Indeed, institution of this protocol improved the outcomes of the CS group that we are now reporting. An additional option to reduce CS wound-related complications may include endoscopic CS, which has been shown to decrease these complications while still facilitating significant advancement of the rectus muscles.24,35,46,47
QOL in CS has not previously been specifically studied, although a few studies have looked at these results in a subjective format. Shestak et al 20 performed 22 CSs and suggested that “all patients reported a subjective increase in abdominal wall strength and significant improvement in the ease of performing activities of daily living.” Two patients in this group underwent quantitative assessment of truncal flexion strength, with a 40% increase in force generated. Mazzocchi et al 44 had similar, but nonspecific results, with all 22 patients being “satisfied” with their abdominal wall reconstruction, but there were no specific comments about QOL or improved function.
This study demonstrates that CS, when required to repair a large hernia, improves QOL. Although, as expected, pain and movement limitations were similar to preoperative levels at 1 month, at longer follow-up, significant improvement in all categories was observed. Furthermore, this study illustrates that the patients receiving a more complex CS operation had similar improvements in QOL outcomes when compared with those patients who underwent standard OVHR. In regard to the possible impact of CS on patient QOL, including pain and movement limitations, this study documents that these concerns were unfounded. Indeed, even when we compared the acute, in-hospital narcotic requirements, CS appeared to cause no greater discomfort than standard OVHR (Table 3).
This large, prospective study had some limitations; mesh properties have previously been demonstrated to have an effect on QOL as well as hernia recurrence.24,37,39 Comparison of individual mesh types was not performed; however, each operation utilized a lightweight polypropylene mesh (less than 50 g/m2). Although the follow-up at 1 year should be adequate to evaluate QOL, the data are somewhat limited in their ability to fully evaluate hernia recurrences. Whereas some previous studies have shown that a large majority of hernias in CS recur within the first 12 months, 26 others have demonstrated that longer follow-up reveals that a number of recurrences can be missed. 25
Conclusion
In this first study comparing CS and standard OVHR, the analysis demonstrates that CS with mesh reinforcement in patients in whom the muscular fascia cannot be closed has equal in-hospital, short-term, and long-term QOL outcomes, including pain and movement limitations, when compared with similar patients who have undergone a standard OVHR. Although wound breakdown and seroma formation are higher, the overall complication, mesh infection, and recurrence rates are similar. Other than superficial wound-related complications, surgeons can advise their patients that performing a CS with mesh reinforcement has few drawbacks when compared with a standard open hernia repair.
Footnotes
Authors’ Note
This work was orally presented at the American Hernia Society annual meeting, 2011.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.