
Abstract
Purpose. Negative-pressure wound therapy (NPWT) is increasingly used for primary surgical incisions despite the paucity of evidence. Study objectives were to assess the use of NPWT on surgical sites to prevent infections and other wound complications after elective primary hip arthroplasty and to consider feasibility of a larger trial. Methods. A nonmasked, randomized controlled pilot trial. Patients were recruited preoperatively from the preadmission clinic of an Australian hospital during 2013-2014. Computer-generated randomization was performed with allocation concealed until completion of surgery. The intervention group received NPWT (PICO) while the control group received the standard care hydrocolloid, reinforced with 2 absorbent dressings. Patients were followed for 6 weeks for postoperative complications (infection, length of stay, readmission) and skin complications (bruising, seroma, hematoma, dehiscence). Feasibility end points included numbers recruited, randomized, and followed up; fidelity; and costs. Results. Of 77 people approached, 76 were recruited, and 70 were randomized. Of 35 in the negative-pressure group, 2 received the standard dressing. Attrition at 6 weeks exceeded 10% in both groups. Dressing costs were lower in the control group ($3.01/d vs $38.40/d); SSI incidence was 2/35 in the NPWT and 3/35 in the control group (intention to treat: risk ratio [RR] = 0.67; 95% confidence interval [CI] = 0.12-3.7; P = .65). NPWT patients experienced more postoperative wound complications (RR = 1.6; 95% CI = 1.0-2.5; P = .04). Conclusion. A reduction of 3% in SSI incidence suggests that a definitive trial requires approximately 900 patients per group. Yet there is uncertainty around the benefit of NPWT after elective hip arthroplasty.
Introduction
Total hip arthroplasty (THA) is a major orthopedic procedure where the prosthetic implants alone cost in excess of AUD $25 000. According to the Australian National Joint Replacement Registry, there were 37 466 THA procedures performed in Australian hospitals during 2012. 1 Postoperative complications such as surgical site infection (SSI) although rare (0.2%-2.3%)2,3 have an impact because they are serious and because of the sheer volume of THA procedures performed. The sequelae of SSI in this patient cohort can lead to significant human and economic impacts, such as longer hospital lengths of stays, increased resources for patient care, and reduction in the patient’s quality of life.4-6 Therefore, using scientifically robust interventions to reduce the potential for postoperative wound complications in this patient population is imperative.
An intervention that warrants further investigation is vacuum-assisted closure, also known as negative-pressure wound therapy (NPWT). The use of NPWT is increasing for surgical incisions where there is a high risk of dehiscence, seroma, and other wound healing complications.7-10 Despite the burgeoning use of NPWT in high-risk surgical wounds,7,10,11 previous work in this area was limited by small sample sizes, lack of randomization and control groups, or nonprospective data. 12 Table 1 provides an overview of the limited level 1 evidence available on the use of NPWT in patients undergoing orthopedic procedures.
RCTs Where NPWT Was Used in Orthopedic Procedures: Clinical End Points and Complications.
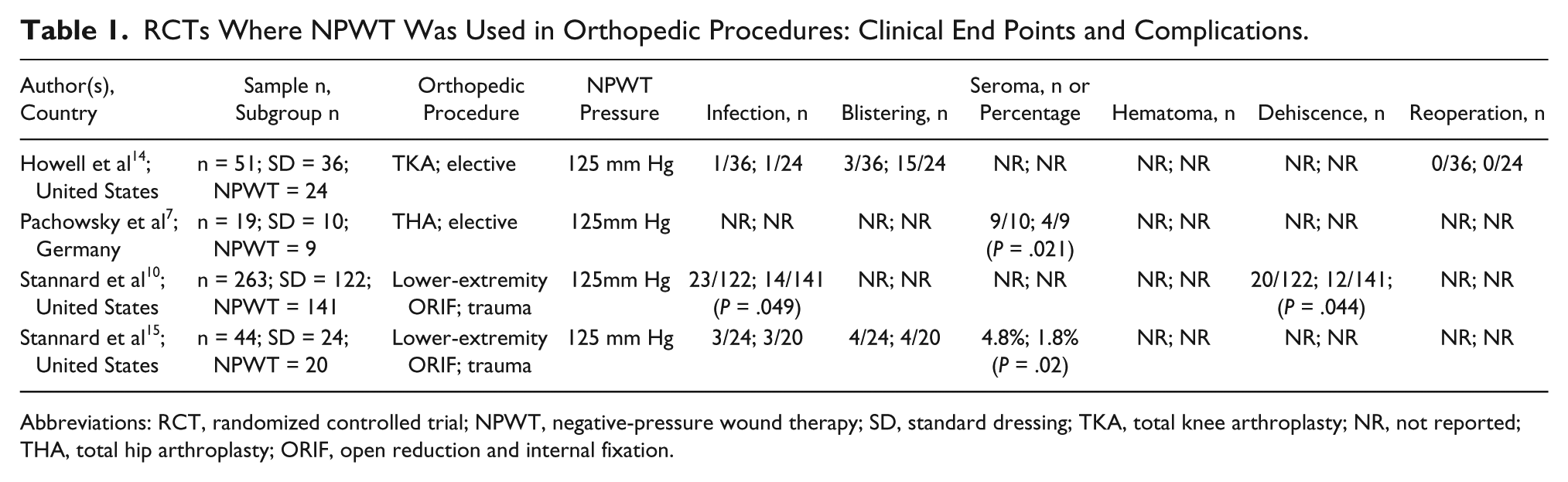
Abbreviations: RCT, randomized controlled trial; NPWT, negative-pressure wound therapy; SD, standard dressing; TKA, total knee arthroplasty; NR, not reported; THA, total hip arthroplasty; ORIF, open reduction and internal fixation.
A necessary first step prior to undertaking a definitive efficacy trial is a feasibility trial to inform the development, implementation, and evaluation of a clinical intervention. 13 The objectives of this study were 2-fold: (1) to assess feasibility outcomes for a larger study and (2) determine initial estimates of effect for NPWT compared with standard dressings on SSI and skin complications in patients undergoing primary THA.
Materials and Methods
This was a single-center, pilot randomized controlled trial (RCT) where either NPWT or standard dressings were used in adult patients undergoing primary THA. A parallel-group, nonblinded, randomized controlled design was used. Feasibility data were needed to inform decisions to proceed to a full-scale trial. Institutional ethics approval was given from the hospital and university, which included accessing patients’ electronic medical records. The trial was preregistered (Australian and New Zealand Trial Registration number ACTRN12612000550808).
At the time of this trial, more than 7000 surgical procedures were performed at the hospital annually. Of these, approximately 1800 were orthopedic surgeries, with more than 200 of these being primary hip arthroplasty. Patients eligible were those undergoing elective primary THA, aged ≥18 years, able to provide informed consent, and who attended the hospital’s preadmission clinic. Patients were excluded if they had an existing infection, had previously participated in the trial, or were unable to speak and understand English.
In 4 previous RCTs7,14-16 using NPWT in patients having elective and trauma orthopedic procedures, sample sizes ranged from 19 to 263 patients (Table 1). The estimated reduction for a definitive trial would, therefore, be based on the observed reduction in this pilot. Because this was a pilot, the target sample size was set at 60 to 100. 17 A sample of 70 reflected what was feasible given the limited budget and short time frame.
Feasibility was assessed against the following: eligibility, ≥75% of patients screened; recruitment, ≥70% of eligible patients will agree to enroll; protocol fidelity, ≥95% of patients in both groups will receive the dressing allocated; retention, follow-up data on the primary end point (SSI) will be assessed on ≥90% of patients randomized. We also calculated resource costs relative to research personnel hours and dressings.
Our primary clinical end point was SSI incidence, based on a composite measure that included superficial, deep, and organ space SSI categories. 18 Secondary end points included individual SSI indicators (erythema, swelling, leakage, purulence) and any SSI indicator, individual wound complications (dehiscence, hematoma, seroma) and any wound complication, proportion of patients who had dressings replaced before day 5 in the postoperative period, hospital length of stay (HLOS), and readmission. The endpoints, SSI indicators and wound complications were treated as binary composite measures. Clinical endpoints (except HLOS and readmission) were assessed daily while patients were in hospital and followed up for 6 weeks.
At baseline, the Research Nurse Assistant (RNA) documented demographic and clinical data, including age, gender, number of comorbidities and medications, ASA status, length of surgery (minutes), type of prosthetic implant (cemented or cementless), wound closure method (sutures, staples, and/or glue), and percutaneous drain insertion. A structured outcome assessment form was developed, and 2 independent clinicians (blinded to group allocation), performed interrater reliability checks of all patients for the primary end point, SSI. Patients were followed up at 3 time points: each postoperative day while in hospital, at 30 days, and at 6 weeks in the outpatient clinic.
Prospective patients were screened in the hospital’s preadmission clinic by the 4 treating surgeons during their final preoperative visit and assessed for the inclusion and exclusion criteria. Eligible patients were approached and given verbal and written information they gave informed consent prior to enrolment. Prior to commencing, a trial-specific education program was implemented to promote consistency and fidelity in the delivery of the intervention.
A computer-generated randomized schedule (1:1 ratio) in randomly varied blocks was prepared by the statistician on the research team (not involved in recruitment). Patients were randomly allocated to either group in the OR at near completion of the procedure. On skin closure, the RNA opened the next sealed, opaque, numbered envelope and advised the surgeon on whether to use NPWT or standard care. Masking was not possible for those administering the intervention, and nor was it possible to mask the patients receiving it because the dressing had to be applied and observed for complications by the clinical staff. The independent outcome assessors (SSI) as well as the data analyst were blinded to group allocation.
Those randomly assigned to NPWT received a PICO dressing (Smith & Nephew, Hull, UK), applied by the lead surgeon under aseptic conditions. The PICO applies a continuous pressure of 80 mm Hg. On day 5, or the day of discharge, patients in the NPWT group had their dressing changed to a hydrocolloid product (OPSITE Postop Visible, Smith & Nephew). The control group dressing was a hydrocolloid (Comfeel, Smith & Nephew) reinforced with 2 absorbent dressings (Primapore, combine pad, both Smith & Nephew) and then with a self-adhesive, nonwoven tape (Hypafix, Smith & Nephew). The standard dressing was left intact, and patients were discharged with their original dressing unless it became soiled.
For analysis, all patients randomized were analyzed using intention to treat, regardless of the treatment received. Risk ratios (RRs) with 95% confidence intervals (CIs) were calculated for clinical outcome data. A P value <.05 was considered statistically significant. Interrater reliability analysis using κ was performed for SSI to determine consistency among raters.
Results
Recruitment and follow-up of patients occurred from March 2013 to May 2014. Of the 76 patients recruited, 70 were randomized (Figure 1). These 6 recruited but not randomized patients had no further data collected. Of the remaining patients, 35/70 were randomly allocated to the NPWT group. There was a slightly higher proportion of male than female patients across the entire sample (37/70), with a mean age of 63.2 years (±13.1, range = 23-91 years). There were no significant baseline differences (Table 2) relative to gender and age, and both groups were similar in relation to most preexisting risk factors except number of medications (P < .05) and wound closure methods (wound glue, P < .001).
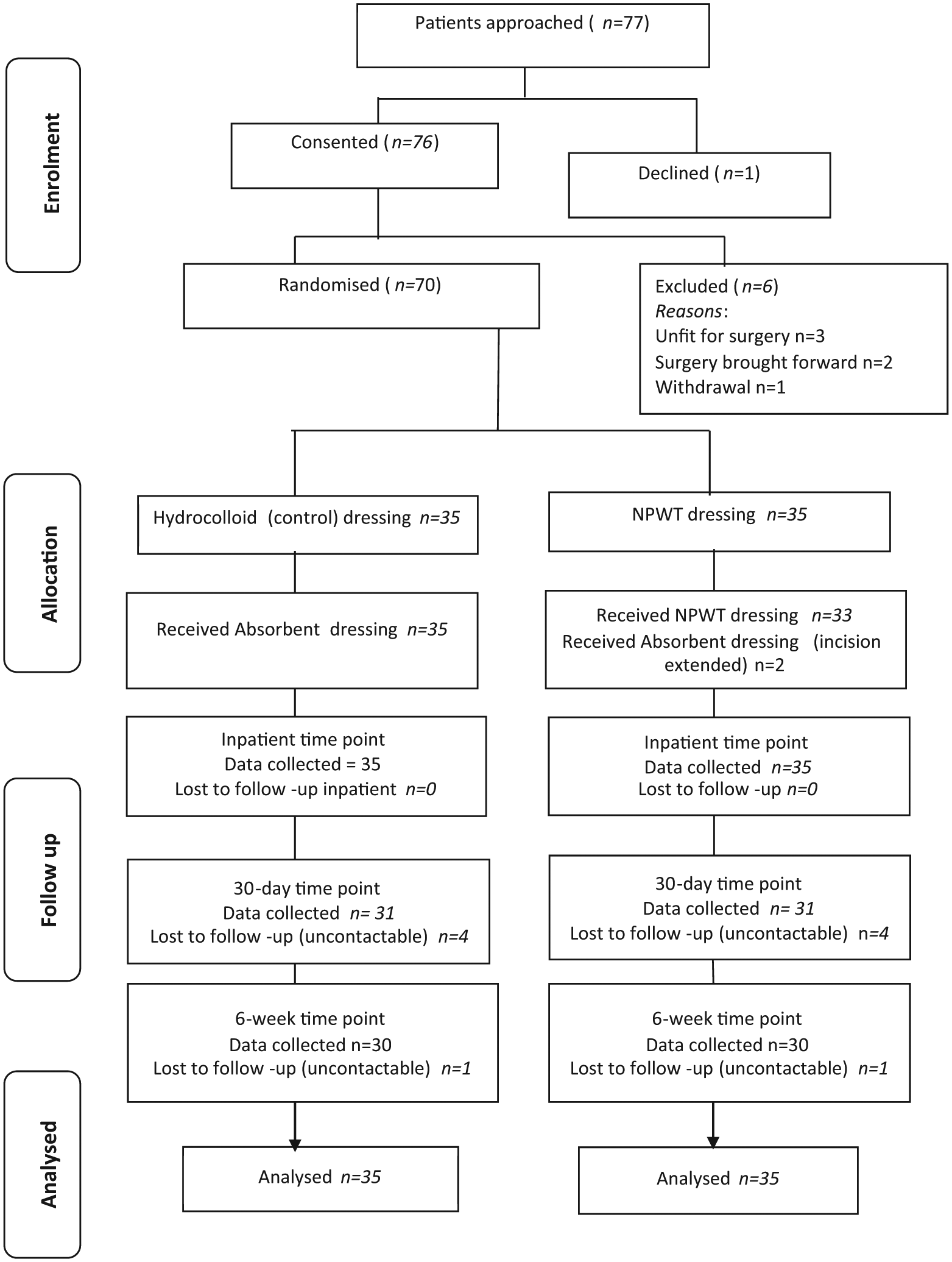
Flow diagram of patients through the trial.
Baseline Demographics and Clinical Characteristics (n = 70).
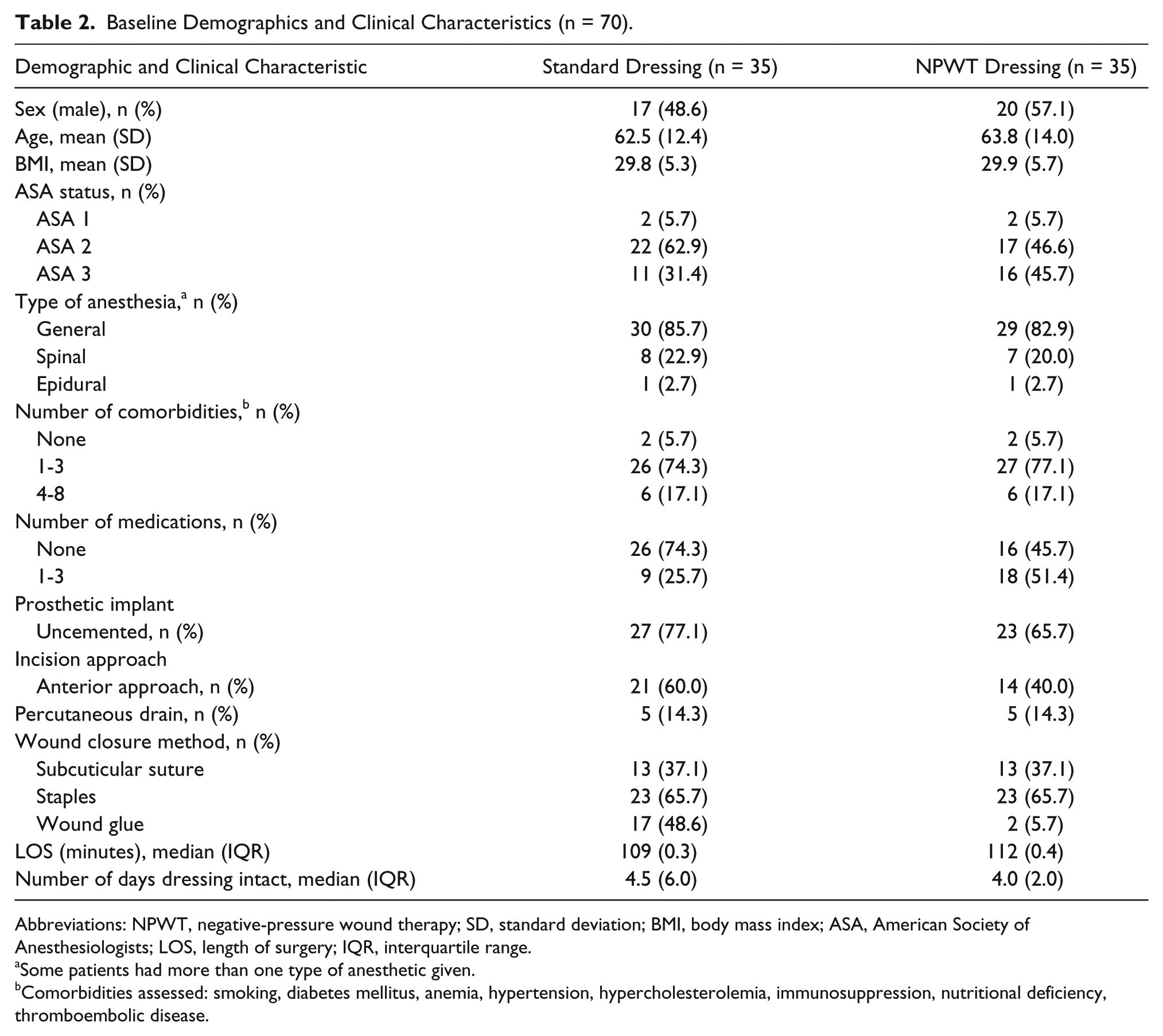
Abbreviations: NPWT, negative-pressure wound therapy; SD, standard deviation; BMI, body mass index; ASA, American Society of Anesthesiologists; LOS, length of surgery; IQR, interquartile range.
Some patients had more than one type of anesthetic given.
Comorbidities assessed: smoking, diabetes mellitus, anemia, hypertension, hypercholesterolemia, immunosuppression, nutritional deficiency, thromboembolic disease.
Feasibility End Points
Of the 77 eligible patients approached, 76 were recruited at the preadmission visit. All patients in the standard care group received the dressing to which they were randomized. However, 2/35 patients randomly allocated to the NPWT group received the absorbent dressing because their surgical incision had to be extended during surgery to enable better access. Attrition rates were lower in the standard care group (Figure 1). Resource costs* for an experienced RNA employed 30 h/wk over the trial period totaled AU$65 508 (AU$41.20/h). For each patient, daily dressing costs were calculated based on the total cost of the products divided by HLOS (Table 3). Cost differences between groups were significant (P < .0001). Patients in the NWPT group had their dressings replaced at least once during their hospitalization, whereas those in the standard care group were discharged with the original dressing intact (P < .001).
Clinical End Points for Patients (n = 70).
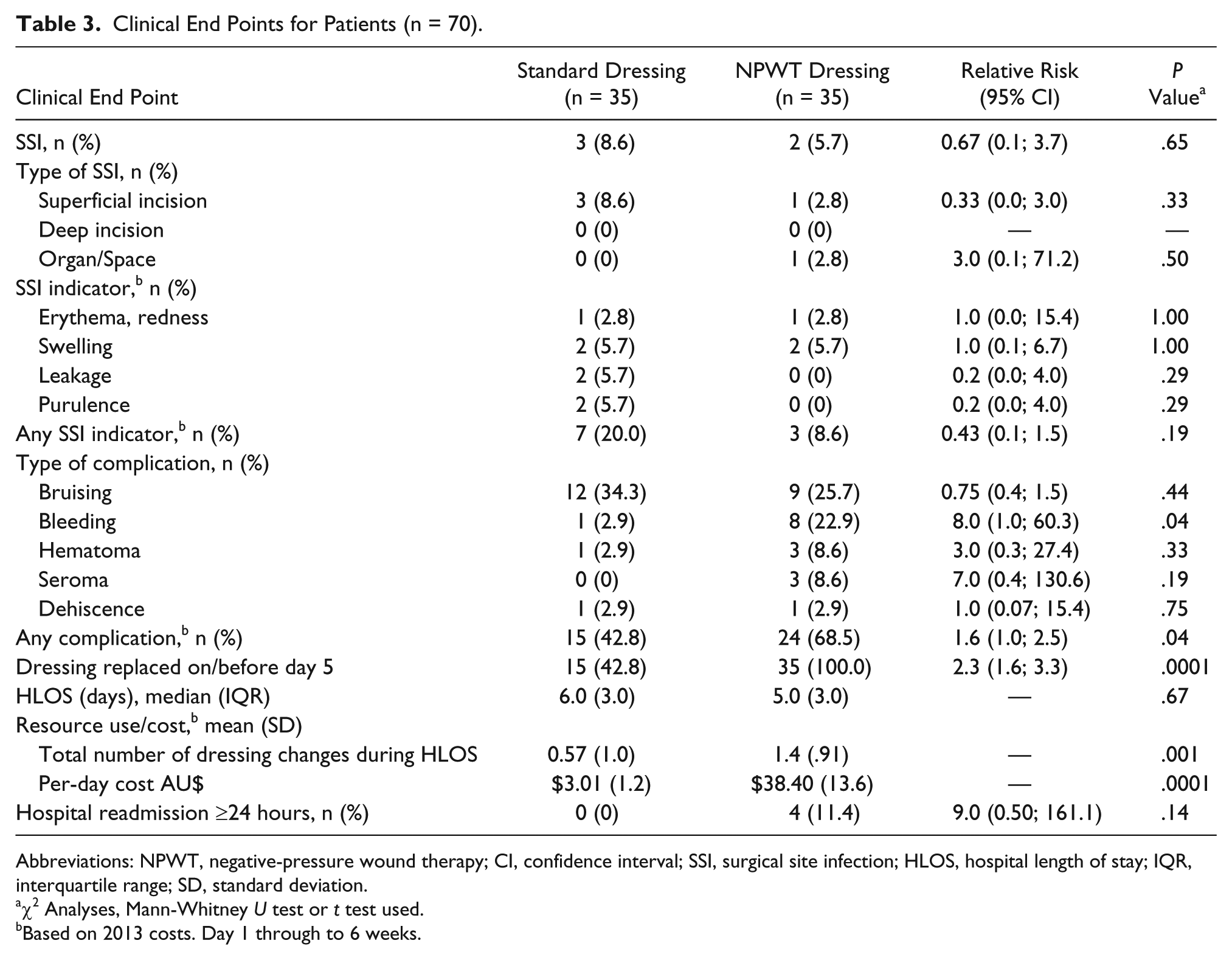
Abbreviations: NPWT, negative-pressure wound therapy; CI, confidence interval; SSI, surgical site infection; HLOS, hospital length of stay; IQR, interquartile range; SD, standard deviation.
χ2 Analyses, Mann-Whitney U test or t test used.
Based on 2013 costs. Day 1 through to 6 weeks.
Clinical End Points
Across the sample, 5/70 patients developed a SSI; group differences were not significant (3/35 controls vs 2/35 in the NPWT group, P = .65; Table 3). Of 70 patients, 10 developed at least 1 SSI indicator (swelling, erythema, purulence, leakage). Of these, 3/35 patients in the NPWT compared with 7/35 patients in the control group had at least 1 SSI indicator, but these differences were not significant (P = .19). The number of wound complications (other than SSI) was statistically different between groups, with patients having a relative 160% increase (P = .04) in the risk of any wound complication (bleeding, bruising, hematoma, seroma, dehiscence) in the NPWT group compared with the control group. Bleeding was also significantly increased in the NPWT group when viewed alone (P = .04).
One (of the 2) patients allocated to the NWPT group who instead received the hydrocolloid dressing (control) did not develop a SSI or any wound complication during the 6-week follow-up period. However, the other patient developed a superficial SSI, diagnosed at 6 weeks. There were significant group differences in the timing of dressing replacement. On the day of discharge, patients in the NPWT group routinely had mandatory dressing replacement with the standard dressing (hydrocolloid), whereas 15 patients in the control group required a replacement as a result of the condition of the dressing (P < .0001; Table 3). Reasons for additional replacements of the NPWT dressing while in hospital included pain and completion of therapy. The manufacturer recommends that the NPWT dressing be left in situ for 5 days. After that period, a standard (hydrocolloid) dressing may be applied. No control group patient was readmitted, but 4 NPWT patients were readmitted for ≥24 hours to treat either pain or infection associated with the surgery (P = .14).
A κ score of 0.48 (P < .0001) for the assessment of SSI and type was achieved, indicating moderate interrater agreement. 19
Discussion
This study is, to our knowledge, the largest RCT using NPWT conducted in patients undergoing primary THA (Table 1). Our observed rates of SSI of 6% (NPWT) and 9% (hydrocolloid) indicate that 832 patients per group would be required to detect a statistically significance difference (α P < .05, 90% power). In this cohort, the observed reduction in SSI of 3% may be clinically important (RR = 0.67; 95% CI = 0.11-3.4; absolute risk reduction = 2.9%; number needed to treat = 35). Although these CIs are wide, the clinical importance evidenced in any reduction is determined by the baseline rates of SSI. Our baseline rates exceed previously reported SSI rates2,3 and may be related to minor variations in clinical practice. For instance, the timing of prophylactic antibiotic administration, incision approach, suture materials used, wound closure methods, and timing of dressing removal may have increased patients’ risk of SSI. Chance imbalances in baseline prognostics can lead to overestimation of treatment effects, especially in trials with small samples. 20 A 3% reduction in SSI rates may be statistically significant if balance was achieved in a larger definitive trial.
Insofar as benefits derived from NPWT, evidence relative to skin complications in patients undergoing orthopedic surgery remains inconclusive (Table 1). Reductions in rates of seroma, hematoma, skin breakdown, and reoperation following orthopedic surgery have been inconsistently reported7,10,14 and any assertion of effect cannot be justified. The small trial by Pachowsky et al 7 found a significant reduction in the incidence and size of seroma, in contrast to our findings of 3 seromas in the NPWT group, yet none with the hydrocolloid dressing. We noted 69% skin complications in the NPWT group, with the most common being bruising, suggesting that the therapy must be used carefully. A major issue identified with NWPT dressings is that they can be painful.21,22 We observed anecdotally that NPWT dressings were more painful than the standard dressing; future studies should formally measure this side effect.
That 4 patients in the NPWT group had been readmitted for wound complications, including SSI and pain, is concerning. Our result suggests that 3 patients developed a SSI in the standard care group compared with 2 in the NPWT group, but the only organ space infection (which may have required additional hospital days) was in the NPWT group. Also, 4 patients in the NPWT group required readmission, compared with none in the standard care group. Given the modest sample, a null result in relation to SSI was expected. In a sufficiently powered trial, a more definitive result is possible. Stannard et al 15 investigated the use of NPWT in high-risk lower-extremity fractures and tibial plateau, pilon, and calcaneus fractures (Table 1). Although a nonblinded and industry-funded study, there were significant reductions in SSI and dehiscence with use of NPWT in comparison to standard dressings. Notably, the significant reductions evidenced in that study were likely because those particular types of trauma fractures had a greater propensity to infection than expected in other orthopedic procedures. Thus, the impact of the intervention effect on the clinical outcomes was more likely to be detected in our THA cohort.
Although our cost estimates are conservative, they suggest that product cost associated with NPWT dressings is more than 10 times greater than would be used routinely in patients undergoing THA. Our calculations were limited to resource costs based on patients’ median HLOS. Others have calculated costs associated with NPWT use to be less than US$500 for the mean 2.5 days of therapy per patient. 16 In that trial, Stannard et al 16 concluded that NPWT was cost-effective because savings from a shortened HLOS and prevention of SSI offset the initial product cost. However, those cost savings estimates of NPWT were based on theoretical economic modeling. As yet, no study has definitively compared costs between patients receiving NPWT and standard dressings. Given that ours was a pilot trial, a cost analysis was not undertaken. For a definitive trial, we recommend including an economic substudy focusing on cost-effectiveness (specialists’ time or number of visits, potential costs savings from the change in the number of bed days, and costs stemming from adverse events and complications).
Limitations
The most notable limitation of this trial is its nonblinded design. Blinding was not possible because of the obvious differences in the nature of the dressing products used. We had considered using dressings that looked identical, but patients and staff would almost certainly have been aware if suction was activated. Although our study groups were similar in respect to known prognostic variables, there were group imbalances with respect to number of baseline medications (higher in the NPWT group), anterior approach (higher in the control group), and use of cyanoacrylate glue for wound closure (higher in the control group; Table 2). Despite randomization, prognostic imbalances may still arise, 20 and these may have increased the SSI risk in one or both groups. This is not unexpected in a smaller pilot trial, and differences would likely be avoided with a larger sample. There was also a cointervention inherent in the study design, in relation to timing of dressing removal. All NPWT patients had their dressing removed and replaced with the standard product (hydrocolloid) just prior to hospital discharge, whereas control patients were discharged with their original dressing intact (unless soiled). This difference may have biased our results. Finally, the brief 6-week follow-up period was insufficient to capture wound complications or SSI occurring up to 12 months postsurgery. Surveillance for the first 12 months following hip and knee arthroplasty is recommended.1,18,23
Conclusion
Our results indicate that the benefit of NPWT in patients undergoing primary THA is currently uncertain, although there is some suggestion that the therapy may reduce SSI indicators but increase other wound complications. There is currently no justification to apply NWPT to all postoperative wounds because the cost is much higher than that for standard care. Multicenter trials are needed to determine which high-risk postoperative wounds would benefit from NPWT as prophylaxis against SSI and associated skin complications.
Footnotes
Author Contributions
BMG contributed to conception and design; acquisition of dataanalysis, and interpretation; drafted the manuscript; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
CMR contributed to conception and design; analysis, and interpretation; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
LT contributed to analysis, critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
EK contributed to acquisition of data; analysis, and interpretation; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
TF contributed to interpretation; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
AH contributed to interpretation; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
GL contributed to interpretation; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
DP contributed to acquisition of data; interpretation; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
WC contributed to conception and design; analysis, and interpretation; critically revised the manuscript; gave final approval; and agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: BG gratefully acknowledges the financial support of The Queensland Government Department of Employment, Economic Development & Innovation Smart Futures Research Fellowship and the Office for Medical & Health Research, Queensland Government; BG, CR, EK and WC also acknowledge the support of National Health & Medical Research Council Centre for Research Excellence in Nursing Interventions for Hospitalised Patients
*
Costings based on 2013 rates.