
Abstract
Minimally invasive surgery (MIS) poses visual challenges to the surgeons. In MIS, binocular disparity is not freely available for surgeons, who are required to mentally rebuild the 3-dimensional (3D) patient anatomy from a limited number of monoscopic visual cues. The insufficient depth cues from the MIS environment could cause surgeons to misjudge spatial depth, which could lead to performance errors thus jeopardizing patient safety. In this article, we will first discuss the natural human depth perception by exploring the main depth cues available for surgeons in open procedures. Subsequently, we will reveal what depth cues are lost in MIS and how surgeons compensate for the incomplete depth presentation. Next, we will further expand our knowledge by exploring some of the available solutions for improving depth presentation to surgeons. Here we will review the innovative approaches (multiple 2D camera assembly, shadow introduction) and devices (3D monitors, head-mounted devices, and auto-stereoscopic monitors) for 3D image presentation from the past few years.
Introduction
Approximately 3 million patients undergo laparoscopic procedures in hospitals in North America every year. 1 This number is expected to rise in the future as image-guided surgery will replace the standard open surgery. Advantages offered by laparoscopic surgery over conventional surgery include less damage to healthy tissue, reduced pain and risk of infections, as well as shorter recovery time and hospital stay.2,3 Despite the benefits for patients, laparoscopic surgery is more difficult to perform and poses a number of visual, haptic, and movement challenges for surgeons. 4
One visual problem that may cause harm to the patients going through a laparoscopic procedure is the reduction of depth perception, when surgeons view the surgical site via a 2-dimensional (2D) laparoscope. 5 It is often seen that surgeons experience difficulties in coordinating their eyes and hands under 2D visual guidance. This could lead to overshooting the targets when misjudging the depth in the surgical site. 5 In the natural environment, depth perception allows us to judge objects and their positions relative to our own bodies and from each other. In laparoscopic surgery (LS), the surgeon lacks binocular disparity when seeing through a single-lens laparoscope and only has limited monoscopic visual cues, such as overlapping, texture gradient, and size familiarity. 6 This poses major mental rotation and transformation challenges to the surgeon and can contribute to response delay, misjudgment, increased cognitive workload, and fatigue.5-7 Due to the greater cognitive processing demands, these consequences could lead to intraoperative complications and unintentionally jeopardize patient safety.8,9 The need for better visualization was stressed further after the evaluation of 252 cases of laparoscopic cholecystectomy, where it was reported that 97% of surgical accidents during this procedure occurred as a result of visual misperceptions. 10
To understand depth of view in LS, we need to understand how humans perceive depth in the natural environment. In this review article, we will begin with a review of how humans perceive depth of view under an open/natural environment. Then, we will examine what visual cues are lost during image-guided surgery and how surgeons compensate for the incomplete depth perception. Subsequently, some of the available solutions for improving depth perception on surgical site are discussed.
Human Depth Perception in Natural Environment
In the natural environment, human operators perceive depth by interpreting a variety of cues collected by the visual system.
Binocular and Oculomotor Depth Cues
Stereopsis, one of the most important mechanisms of spatial vision, is the process by which the angular disparity between the images on the left and right retinas is used to compute the depth points within an image. As first explained by Charles Wheatstone in 1838, stereopsis refers to the following: “the mind perceives an object of three dimensions by means of the two dissimilar pictures projected by it on the two retinas.” 11 The 2 separate images created on both retinas are sent on to the brain for processing. When the 2 images arrive simultaneously in the visual cortex, they are united into one picture. The brain combines the 2 images by matching up the similarities and registering the small differences. The small differences between the 2 images accumulate to a large difference in the final picture, which is the 3-dimensional (3D) stereo presentation of the world.
Another group of cues that are dependent on binocular depth cues and can contribute to some extent in perceiving the world 3-dimensionally, are the oculomotor depth cues, convergence and accommodation. When we fixate on an object, we typically accommodate to the object, that is, change the power of the lens in our eyes to bring that object into focus. Once we have accommodated to the object’s distance, other objects that are much closer or farther awayfall out of focus on our retina. Convergence is the rotation of the eyes toward a single location in space. For example, when looking at a close object, the observer’s eyes angle inwards toward each other. The effort required for accommodation and convergence provides the brain with information about distance/depth.
Monocular (Pictorial) Depth Cues
Monocular or pictorial depth cues are set of 2D information pieces from which we are able to partially reconstruct 3-dimensionality. The main monocular depth cues the human eye uses to perceive depth when looking at 2D images and pictures are as follows: occlusion, familiar and relative size, shadows, dynamic shadows (shadow motion), aerial perspective, texture perspective, linear perspective, and so on (Figure 1).
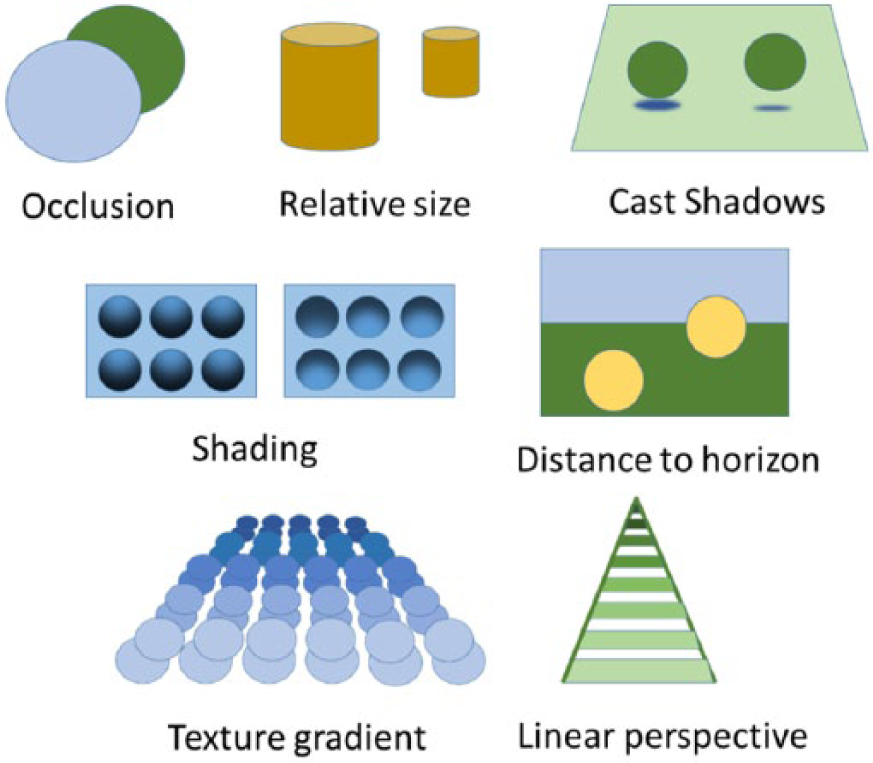
Illustration of the basic monocular depth cues.
Interestingly, most of these cues were originally discovered and used by renaissance artists to a great extent and only later studied by psychologists. Linear perspective was well known to artists (Brunelleschi, Dürer, and Alberti) by the time of the Renaissance and is a powerful indicator of depth (Figure 2).
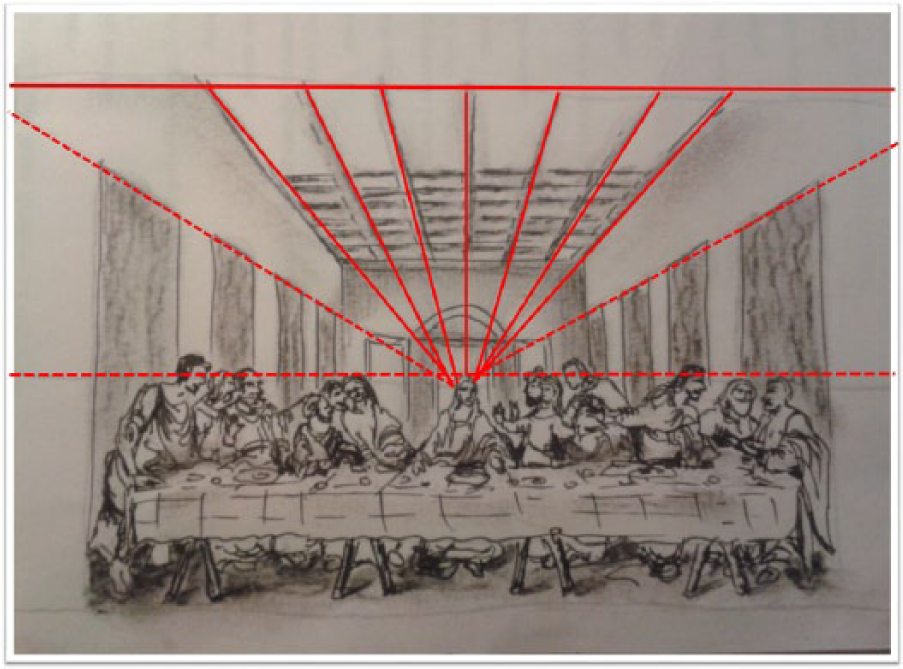
Linear perspective presentation in a reproduction of a Renaissance painting.
In the example in Figure 2, the converging lines or gradients of texture are automatically interpreted by the visual system as indicating increasing distance from the observer.12,13
Motion-Based Depth Cues
One strong depth cue that provides additional information about relative depth is the image motion resulting from observer’s movement and is also known as motion parallax (Figure 3).
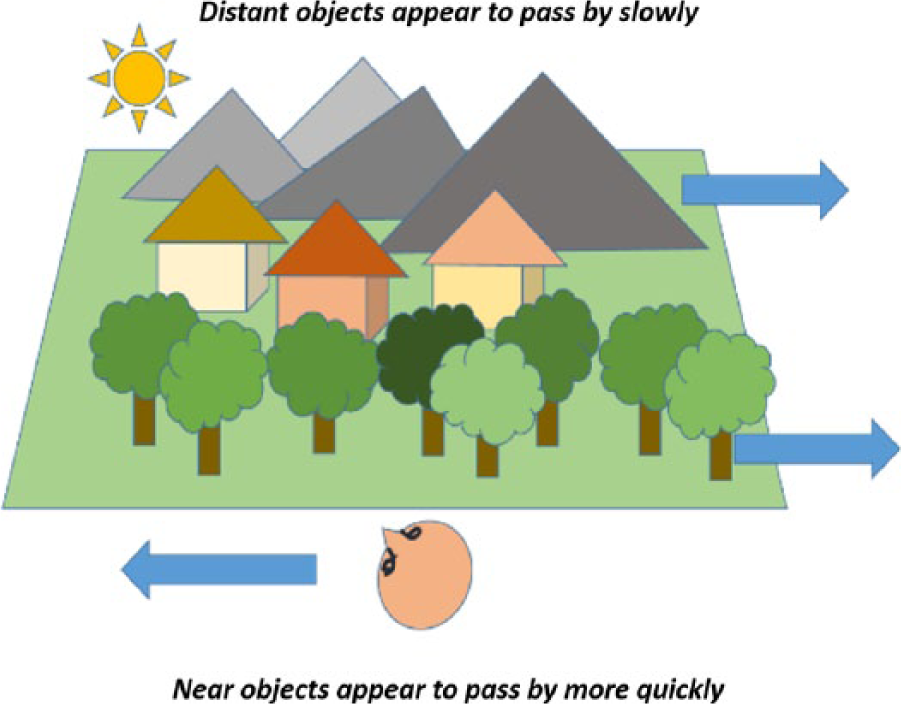
Motion parallax. When an observer passes through a scene (when driving a car), it moves through the observer’s field of vision at different speeds.
The idea of an underlying similarity between stereoscopic and motion parallax processes is not new and was studied by Helmholtz over a hundred years ago, when he argued that the impression of depth obtained from motion parallax was “just as if he were looking at a good stereoscopic view of it.” 14 Furthermore, similar and very powerful aftereffects of depth can be produced from both motion parallax and stereoscopic information.15-18
In this section, we reviewed the basic visual depth cues available for the eye under a natural environment. The following section will reveal what depth cues are lost or not fully presented in the current minimally invasive surgery (MIS) and the surgeon’s compensatory response.
Depth Perception in MIS
In open surgery, surgeons can apply all of the aforementioned cues to perceive depth of the surgical site, as well as viewing from different vantage points. However, in MIS, these strategies cannot be applied due to limitations of the imaging technology. Let us examine all of these limitations one by one.
Lack of Binocular Disparity
The images captured by single-lens laparoscopes are 2-dimensional. They do not present the binocular disparity as a main visual cue necessary for rebuilding the 3D structure. Additionally, the 2D surgical monitor in LS acts as a filter and removes stereoscopic, 3D depth cues from the operative field while retaining some of the monocular cues. Without binocular disparity as a main visual cue necessary for perceiving the 3D structure, surgeons have to rely only on 2D cues (interposition, shadows, and relative size) for estimating depth in the operative field. 6 It is observed that in this environment, poor in visual cues, surgeons try to rebuild the 3D shape by explicitly searching for shadows and other monocular cues. However, these monoscopic cues are further degraded by the imaging technology and are not freely available for surgeons. This leads to perception of depth, which is highly degraded under the MIS condition.
Small Field of View
Generally, the field of view offered by conventional laparoscopes is significantly smaller than what is available to surgeons in open surgery and thus decreasing the surgeons’ ability to see the whole operative site and perceive the target’s spatial interaction. 2 For instance, the objects perceived through the reduced field of view may appear closer than they really are, which hampers surgeons’ depth perception. 19 The small field of view is due to the optical design of the laparoscopes. There are 2 types of laparoscopes, with direct and oblique vision depending on the angle between the longitudinal axis of the laparoscope and the axis of the lenses. Direct (0°) optics provide a broader view of the surgical site and are critically important when the surgeons are not familiar with the laparoscopic methodology. In contrast, oblique (angled) optics provide the observer with a narrow field of view but allows the operator to rotate the camera and see the target plane from a wider range of directions. 20 To expand the field of view, surgeons often try to move the laparoscope in/out in relation to the operating site. However, this maneuver is restricted, first, by the fixated point of the laparoscope on the surgical site and, second, by the vestibular side effects on the surgeons when frequent changes in the field of view is generated. All these restrictions, together with the “keyhole” appearance of the surgical workspace, are reported to be reasons for additional spatial integration complexity and obscurity. This degradation in spatial orientation interferes with the operator’s ability of developing an accurate cognitive model of the manipulated environment. “Getting lost” as a result of the spatial orientation degradation is a common experience when navigating under laparoscopic condition. 21
Limited Range of Laparoscope Motion
The laparoscope is usually inserted at a single predetermined port (trocar), which restricts the view perspectives in LS. The stationary image presentation in MIS eliminates the motion cues to depth, which are freely available in open surgery. For instance, in open procedures, surgeons can extract depth information from the surgical site by moving their eyes and head to inspect the targets from numerous vantage points. The dynamic exploration of the scene from various vantage points provides important depth information such as motion parallax and optical expansion, which are highly decreased under laparoscopic conditions. 22 As the response of surgeons to movement parallax is not easily assessable in the LS context, Voorhorst and colleagues studied the effect of motion cues on operators’ performance under experimental conditions. Two groups of participants took part in the study: the first group was assisted by movement parallax, and the second group viewed a static image. Both groups were tested by performing an exploration and manipulation task. Results indicated the advantage of movement parallax for the exploration task but not for the manipulation task. They concluded that movement parallax could be applicable to laparoscopy. 23
Restricted Location of Port Insertion
In certain LS procedures, the location of the insertion points of the laparoscope on the abdominal wall is highly restricted by the topography of the diseased organ and other anatomical constrictions. The top portion of patient’s abdominal area is reserved for placing instrument trocars. The laparoscope is often placed at a very narrow angle to the plane of the operating site, which could further lead to misinterpretation of the major monocular depth cues (Figure 4).

(a) Laparoscopic and (b) open surgery condition pictures taken at 20° and 70° angles, respectively, toward the operation site.
It can be seen that along with shadowing, occlusion, and size familiarity cues, the optical angle of the camera could also change the presentation of depth cues. The narrow angle of the laparoscope (20°) toward the plane of the surgical field in the first picture (Figure 4a) degrades the information about depth because of foreshortening or compression of depth. In contrast, in open surgery, with the raising of the angle of the viewing perspective to 70° (Figure 4b), this misperception dissolves and the line-of-sight of the presented image aligns with the natural line-of-sight of the observer. When line-of-sight ambiguity occurs, surgeons have difficulties in judging the spatial relationship of the objects in a scene. The resulting perceptual difficulty leads to performance degradation when precise judgment of depth is required.
Shadowless Operative Field
An additional restriction in video imaging that contributes to the degradation of visual intake and task performance compared with direct vision is the lack of shadows in the operating field. The shadowless operating field is created by the positioning relationship of the lens and the optical systems in the laparoscope. The rod lens systems invented by Hopkins and the fiber-optic light transmitting system permit the illumination of the internal organs by an external light source through internal reflection within the glass fiber bundles. Basically, when using both components in conventional laparoscopes, light surrounds the lens, which creates a coaxial alignment relationship between the lens systems and the optical light fibers. This assembly produces good illumination of the surgical site but at the same time results in a shadowless operative field and thus eliminating shadows as one of the most powerful cues for depth.24,25
Image Resolution
Depth perception of surgeons could also be affected by image qualities such as image resolution and bit depth, which are intimately tied together in a monitor’s display. Still, the data that describe their effects on users’ depth perception have been studied mainly by computer scientists. For instance, psychophysical and physiological examination on the relationship between stimulus resolution and depth perception was studied by Tsushima and colleagues who found that a higher resolution stimulus facilitates depth perception even when the stimulus resolution difference is undetectable. 26 Similarly, a study conducted by Bando and Sasaki also demonstrated that using super-high-resolution 3D display with about 6 times higher density compared to usual 3D television could give us better depth information to perceive natural surface texture. 27 In MIS, the performance of the first prototypes of stereoscopes has been limited in resolution and contrast, both in the scope itself and in the display technology. With technology advances in the past years more powerful scopes have been developed. However, examining the effect of image resolution in surgery is still not sufficient and more thorough studies, particularly targeting the surgeons’ depth perception under the different image qualities, are needed.
Possible Solutions for Improving Depth Perception in MIS
There are 2 possible innovative points for improving depth perception. The first is about capturing or creating images with binocular disparity, and the second is about presenting images with binocular disparity to the surgeons.
Capturing Images With Binocular Disparity in MIS
An approach to improve depth perception in MIS is to provide the observer with binocular disparity of the surgical site. Technically, this can be achieved with either 1- or 2-lens systems. The mechanism of image creation in the 2-lens system imitates the human eyes, only on a smaller scale. The 1-lens system uses a standard scope and is furnished with an additional device for left and right image separation. It is claimed that the 2-lens stereoscope provides surgeons with better image quality compared to the 1-lens system.
Images of surgical site can also be captured using a system composed of thousands of microscopic lenses positioned in front of a single video chip, resembling an insect’s eye. The resulting numerous and slightly shifted images are further analyzed with a special computer algorithm for separating the images into left and right ones. 28 Binocular disparity is thus generated and perceived by the human operator as stereoscopic video images.
Besides the technology used for creating 3D images of the operating site, it is of importance to create advanced technology to present images to surgeons in a 3D fashion.
Presenting Images With Binocular Disparity to Surgeons in MIS
Available technologies for presenting binocular disparity of MIS images include the 3D video monitor, the head-mounted display, and the auto-stereoscopic display.
3D Video Monitors
One way for displaying disparity in images on a 3D TV monitor is with the use of a shutter of liquid crystal technology (active systems). The images captured by the 2 cameras in these systems can be displayed alternately with a frequency of 120 Hz. Another way of displaying stereo images (passive system) is based on filters that polarize 2 source-video images at 90° angles. To perceive the stereo images, the observer has to wear special glasses to watch active and passive signals presented to the different eyes.
Since the report of Becker et al that announced the possible application of the stereo display technology in laparoscopy, several researchers sought to find the effects of the 3D monitors on laparoscopic performance.29-34 A good number of studies found increased accuracy of performance and participants’ preference in the use of 3D visualization over the conventional 2D system.35-38 In the 1998 study, van Bergen and colleagues concluded that operators with normal spatial capability can work faster and more accurately under 3D vision. 32 Similar findings came from Kong et al, using the Wasol 3D imaging system. The results indicated that the use of this visualization system increased the accuracy of performance, with reported enhanced depth perception. 39 Pietrzak et al concluded in their research that the superiority of 3D systems over 2D systems is documented but still needs to be proven. 40
Despite the reports on the advantages of 3D imaging in terms of better depth presentation, the 3D scope has not been extensively used in the operating room (OR) since its introduction in 1990s. Surgeons continue to complain about the poor quality of the 3D image and discomfort of wearing 3D glasses. Moreover, surgeons often experienced side effects, such as visual strain, headache, nausea, and tiredness, after completing 3D laparoscopic tasks.41-43 Other researchers have found that 3D systems are not superior over 2D systems.30,44-47 A series of studies conducted by Hanna et al concluded that there is no difference between 2D and 3D display groups in execution time during laparoscopic cholecystectomy. It was again confirmed that surgeons experience visual strain, facial discomfort, and headaches immediately after operation.32,33 Later, Hanna and Cuschieri reported indistinguishable difference between 2D and 3D visualization modes, especially when many of the monocular depth cues are available in the surgical environment. 48
Head Mounted Displays
Instead of displaying images on TV screens, stereo images can also be displayed on special head-mounted displays (HMD). Geis is the pioneer in using HMD to display stereo images taken from an endoscope on 2 small screens in front of the subjects’ eyes. This technology provides the operator with more natural line-of-sight as it enables the surgeon to look down on the operative field and to see both the camera image and his/her hands simultaneously. 49 The interest in HMD was further developed by Bajura et al, who constructed an advanced see-through HMD system where it was possible to project an ultrasound scan on the patient’s abdomen, giving the observer the effect of looking through the patient. The virtual image within the patient’s body provides accurate occlusion cues for the registered ultrasound data. Moreover, the ultrasound images appeared stationary in 3D space as the observer walked around the subject. 50 An optical see-through augmentation for LS was also presented by Fuchs et al. The augmented images in their study were shown to a moving HMD user for perceiving the 3D structure. An overlaid view of the laparoscopes inserted through small incisions was successfully simulated. 51 Another see-trough system was developed by Vogt et al. Their video see-through HMD overlaid magnetic resonance imaging scans and provided views of tool manipulation hidden beneath tissue and surfaces. 52 It can be seen that there is strong evidence in support of the HMD as a trustful technology for improving surgeons’ depth perception in MIS.
Even though the stereoscopic displays used in these systems are proven to help in experiencing depth, there are still some constraints that need to be overcome before this technology is fully introduced into the OR. For instance, accommodation-convergence conflicts or low resolution and dim displays cause objects to appear farther away than they actually are. 53 It is also observed that patient information, such as vital signs and intraabdominal pressure, can be overlaid and disturb the video images produced from these technologies. 54 When wearing see-through goggles, users also need to adapt to the vertically displaced viewpoints in order to execute tasks. In an experiment by Biocca and Rolland, subjects exhibited high incidents of overshooting in a depth-pointing task after removing the HMD. 55 The HMD technology was reported to cause somatic symptoms for the users such as headache, nausea, and dizziness. 56 As a result, there is still controversy in using these HMD technologies. Additionally, it should be considered that these systems are costly and thus not easily accessible for operators.57-59
Multiple-User Auto-Stereoscopic Displays
Recently, a multiuser 3D video system was developed. 60 The use of auto stereoscopic display (AD) enables 3D perception by the whole surgical team without needing to wear special glasses. 61 This promising new AD technology still has some limitations that need to be overcome, such as the restriction of the participant’s movement in order to keep the image steady and stable. 62 The proposed next-generation multiple-view AD technology allows the whole surgical team to look at the same 3D image from different viewpoints and perceive stable (clear) 3D images not affected by viewer movement. 61 Another advantage of this technology is the lower ocular fatigue and shorter training time, enabled by the reduced pseudo-stereoscopic zone with the use of a higher number of views. Although this 3D display technology shows great promise, it is still not highly applicable in surgical scenarios due to the encumbrance of the acquisition system. At least 5 cameras need to be embedded into the device and passed through the incision site. To address this limitation, Silvestri et al tested a new prototype of this technology where they presented a device able to hold up to 7 camera modules interfaced with multiview ADs and thus supporting the use of this promising technology in advanced, multi-operator surgery. 63
To sum up, at present, there are various high-tech visual devices available for surgeons to operate under a reconstructed 3D visual guidance. Yet the possible advantages of 3D imaging, with regard to surgical performance, may be outweighed by the negative visual effects on surgeons with this mode of visualization. The introduction of new visualization technology in the OR is further affected by the adaptation mechanisms that have been built over years of practice under conventional 2D technology. Often, experienced surgeons report that they have learned to interpret the limited monocular depth cues and have developed strategies for executing procedures with satisfactory outcomes. Additionally, the increased cost associated with 3D systems is an important consideration as comparable performance is claimed with the less expensive 2D systems. All of these factors will continue to constrain the free introduction of 3D devices in the OR until more reliable and safe devices are developed for the surgeon and the patient.
While 3D technology is making step-by-step progress toward the goal of achieving stereo presentation of the surgical site, some experts promote different solutions based on expanding and enhancing the depth cues in the current 2D technology.
Other Innovations for Improving Stereoperception
Articulating Laparoscopes and Laparoscopes With Rotating Lens for Enlarging Field of View
To compensate for the narrow visual field obtained with the rigid laparoscopes used in current practice, articulating scopes and laparoscopes with rotating lens were introduced. These types of laparoscopes allow the operator to change the viewing angle and thus provide a broader picture of the operating field from a single entrance port. However, the 2 types of articulating laparoscopes commonly used do not confirm their superiority over the classic rigid endoscopes. 64 Furthermore, comparisons based on the optical performance between articulating laparoscopes and ones that use rotating lens was conducted in 2012. Results showed that the rotating lens system demonstrated the highest image resolution but also the highest distortion among the tested laparoscopes. It was defined that further assessment is necessary to determine if these findings translate into improved surgeon performance. 65
An innovative approach for expanding users’ peripheral field of view is by using fisheye lenses in see-through displays. 66 This fisheye vision is a method for expanding a user’s effective field of view by up to 180° and thus allowing users a wider field of view without sacrificing binocular vision. In general, it has been shown that this technology can expand the user’s virtual field of view but its application in image-guided surgery still needs to be determined.
With these efforts, we understand that the small field of view in MIS is difficult to be overcome with the current design of the scopes due to the limited space available for visualization and manipulation inside the abdominal cavity.
Multiple 2D Visual Perspectives
The use of multiple cameras as a tool for restoring the 3-dimensionality is optimistic and can easily resemble the different vantage points accessible during open surgery. 67 The idea of displaying several 2D images taken from different viewpoints of a 3D structure was examined in the work by Tory et al. They found that when presented with more viewing perspective of a 3D object, participants were faster and were able to more accurately judge the spatial relationship of the object in relation to its surroundings. 68 Reconstruction of 3D surgical environments by adding multiple views was also reported by DeLucia et al in 2011. It has been proven that the various perspective information improves anatomical interpretation and laparoscopic performance. However, displaying the combination of multiple views imposed more attention demands compared with a single-laparoscope view. 69 Future research should explore this limitation and determine whether this result applies to a variety of surgical tasks and whether operators can be trained to use depth information provided by the multiple laparoscopes.
Introduction of Shadows (Into the Shadowless Operating Field)
As we know, the shadow of objects is a powerful 2D cue for stereo perception. Therefore, several studies try to optimize shadow production in terms of the degree of shadow contrast, color, and the location of shadow-casting illumination. Shadows are generated by the separation of the imaging system of the camera from the illumination source. 70 It was proven that the use of various illumination sources produces different degrees of shadow that provide an environment rich with shadow depth cues. Research has shown that endoscopic task performance significantly improves when such shadow-producing systems are used. In a study conducted by Nicolaou et al, 3 visualization techniques were tested simultaneously. The aim of their study was to assess the usability of conventional 2D, 2D with enhanced depth cue based on shadows, and active 3D display in enriching visual perception input. 71 Other authors confirmed the findings of earlier research on the problem that shadow depth cues enhance minimally invasive task performance69,72,73 It was also found that shadow-luminance contrasts between 22% and 42% is optimal and is associated with prime performance, whereas more intense shadow contrasts were associated with degraded performance. 72 As the shadow perception is described by 2 parameters, shadow contrast and shadow color, the effect of the later was further explored. In the study by Shimotsu et al along with the effect of dark shadows and no shadows in the operating field, the effect of the colored shadow was similarly tested. The performance accuracy was improved with the presence of colored (cyan) and black shadows compared to the no shadow condition. Interestingly, cyan shadows lacked a significant advantage over the black ones. 74
Some scientists believe that the directional source of shadows produced by illumination systems play a significant role in visual perception of shape and position in space. For instance, the shadow that the current endoscopic systems generate in the operative field is not optimal, as the shadow illumination comes from the side and from below the light source. Research on visual psychology has found that the human visual system prefers overhead illumination. 75 This is known to be adapted from the overhead lighting by the sun and other sources of artificial light. Another technology for improving depth perception through enhancing shadow cues is a method that uses photometric stereo, which is a 3D reconstruction technique based on photometric constraints using 3 or more light sources for creating a distinct shadow cue. In the study by Collins and Bartoli, a standard monocular laparoscope, modified only with 3 color filters (red, green, and blue) placed at its tip, was used. The potential of this approach was demonstrated for successful application in close-range imaging conditions such in MIS. 76
All of these studies suggest that generating additional shadows improves depth perception and allows accurate maneuvering of the instruments, thus preventing tissue trauma.
Conclusion
Degraded depth perception remains one of the visual perception problems in MIS and continues to hamper surgeons’ performance and, subsequently, patient outcomes to a great extent. The technology used for improving video images in image-guided surgery proposes to enhance the depth perception of surgeons. However, it still lacks the finishes that allow the surgeon to operate in an environment with minimum side effects and maximum patient outcome. Furthermore, surgeons’ experience with the use of the different visualization devices is often not taken into account during technology design. There is still not sufficient objective data to support surgeons’ visual comfort and preference in the use of the proposed technology, which could negatively reflect on procedural and patient outcomes. Further studies on surgeons’ behaviors and on imaging technology are needed to develop supreme designs that align optimally with surgeons’ comfort.
One way to improve the design of MIS visual technology is to understand surgeons’ behavioral responses to different visualization technologies. Knowledge on surgeon’s depth perception will help improve the design of visual technology for MIS, assuring superior surgical performance with a final goal toward improving patient safety and health.
Footnotes
Author Contributions
Study concept and design: Rositsa Bogdanova, Bin Zheng, Pierre Boulanger
Acquisition of data: Rositsa Bogdanova, Bin Zheng
Analysis and interpretation: Rositsa Bogdanova, Bin Zheng
Study supervision: Bin Zheng
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.