
Abstract
Background. A retained surgical item in patients (gossypiboma) is a persisting problem, despite consistent improvements and existing guidelines in counting instruments and sponges. Previous experiences with radiofrequency identification technology (RFID) tracking sponges show that it could represent an innovation, in order to reduce the criticism and increase the effectiveness during surgical procedures. We present an automated system that allows reduction of errors and improves safety in the operating room. Methods. The system consists of 3 antennas, surgical sponges containing RFID tags, and dedicated software applications, with Wi-Fi real-time communication between devices. The first antenna provides the initial count of gauzes; the second a real-time counting during surgery, including the sponges thrown into the kick-bucket; and the third can be used in the event of uneven sponge count. The software allows management at all stages of the process. Results. In vitro and in vivo tests were performed: the system provided excellent results in detecting sponges in patients’ body. Hundred percent retained sponges were detected correctly, even when they were overlapped. No false positive or false negative was recorded. The counting procedure turned out to be more streamlined and efficient and it could save time in a standard procedure. Conclusions. The RFID system for sponge tracking was shown to be experimentally a reliable and feasible method to track sponges with a full detection accuracy in the operating room. The results indicate the system to be safe and effective with acceptable cost-effective parameters.
Introduction
Retained surgical items is one of the most common sentinel events reported in common surgical practice. An estimated 250 to 300 surgical tools (including needles, sponges, and instruments) are used during surgical procedures in operating rooms (ORs). 1 The number of adopted items can significantly increase up to 600 in advanced and emergency operations. Retention of surgical instrumentation inside the body, usually called “gossypiboma,” can occur during almost all the surgical procedures, although the risk seems to increase during abdominal surgery (46% to 55% of retained surgical item). 2
A retrospective study estimated the incidence of retained surgical instruments as 1 in every 10 000 surgical procedures that involve an open cavity. The incidence of retained surgical sponges, considering open surgery, is the highest, with a value of approximately 1/2000 surgical procedures. 3 A landmark study reported that the error in counting gauze and surgical instruments occurs in 12.5% of surgical procedures. 3 Moreover, it should be mentioned that this number still remains underestimated due to a large number of omitted gossypiboma, both to the patient and to the care institution.
Despite the enormous improvement in counting guidelines for OR equipment, the risk of retaining foreign objects still remains elevated, increasing during emergency operations with unplanned changes in procedure, in the case of patients with a higher body mass index (BMI), and intraoperative bleedings or other complications. The sequelae arising from retained sponges are difficult to diagnose and can cause serious damage to the patients such as acute and chronic intestinal obstruction (15%), abscess formation or sepsis (43%), and fistulization or bowel perforation (7%), even long after the surgical procedure.4-6
The morbidity rate linked to this event rises up to 40% with a 5% mortality rate. 7 A second surgical procedure is required to remove foreign bodies in 69% to 83% of cases, with cumulative risk for patients mainly represented by postoperative infections. Furthermore, readmission and prolonged hospital stay (30% to 59%) generates additional costs for the health care system and consequent litigations have significant legal and economic implications due to refunds to patients and families. As a relevant negative consequence, image and marketing damages have to be considered by the hospital management.3,6 Sponges are usually the most frequent retained object in surgical practice, with rates being 48% to 69% of reintervention for gossypiboma.
In order to track items during surgery and to prevent human errors, hospitals developed strict protocols to count sponges.
The standard procedure consists of manual count usually performed by nurses, but the procedure is extremely liable to errors.
Several studies showed a high rate of false positive during a final count, which was wrongly thought to be correct.3,8 A 2011 study identified 57 different potential reasons for the failure of manual counting, describing why it did not adequately prevent counting of the retained sponge. 9
The introduction of X-ray detectable sponges contributed to reducing incidence of gossypiboma, although not eliminating the issue. Kaiser et al 10 reported 3 cases out of 29 in which X-ray was used to screen for radiopaque sponges, resulted in a false negative.
Automation can reduce counting time and human errors as demonstrated in a wide number of industrial fields. Nowadays different system such as bar-coded sponges and radiofrequency tagged sponges have been designed and tested to reduce the incidence of sponge gossypiboma in surgical practice; however, definite data concerning routine use in surgery are not available because these system have not had large diffusion in clinical settings. Commercialized devices have showed different rates of sensibility and specificity, especially in relation to the patients’ BMI, showing a reduction of sensibility in the case of obese patients. 9
The authors designed, developed, and tested an original integrated system based on radiofrequency identification technology (RFID) that is able to localize and count in real time the tagged sponges, detectable by a remote reading. Moreover, the system includes an integrated array antenna able to scan a patient’s body and identifying retained sponge.
Methods
A dedicated RFID transponder (tag) has been designed to detect radio waves and then convert it to electrical energy, which can be detected by an antenna device, called reader. The antenna interrogates the tag by a specific signal, which every tag can read and reply to, allowing “real-time” inventory management. The adopted tags are passive RFID tags; they do not contain a battery and the power is supplied by the reader. Passive RFID tags have several advantages, such as being inexpensive and very small. 11 After thorough evaluations, high-frequency tags (13.56 MHz) were preferred, as they are characterized by technical standards applicable in health care and an optimal reading range in the biological environment.
Based on this concept, a prototype was developed and tested. The system consists of the following:
Check-in antenna for the initial count of sponges (Figure 1); this antenna is located in a small washable box.
Sponges (40 × 40 cm) integrated with passive RFID tags −15.5 ± −0.75 mm, 1.5 g, operating in high frequency at 13.56 MHz, 512 bit of memory (Figure 2). Each sponge is equipped with an RFID tag; individual tag identification is possible but not of use for our research aim. Each tag is hand-sewn within the sponges with a texture design to prevent the accidental drop of the tag from sponges. Tags are made of biocompatible material: water, chemicals, and high-temperature resistant, and approved for human use. They are qualified for sterilization process, have good mechanical strength with specific reference to impact, and have high resistance to chemical and biological fluids.
Check-out antenna (basket antenna) for the count of used sponges (Figure 3). The system is designed to contain the kick-bucket normally used in ORs and consists of an array of 6 antennas (4 on the lateral surface, 1 at the bottom, and 1 at the intermediate level). The antenna is washable and is provided with a hole at the base to allow leakage of fluids.
An integrated array antenna for scanning the patient. It includes 6 detectors with a multiplexer (Figure 4). The device can translate over the entire body, making the procedure objective and independent of OR team skills.
A management software in communication with readers identifies and counts sponges, showing real-time data then supporting OR staff in surgical sponges management (Figure 5).

Antenna for the initial count of sponges before and during surgery.
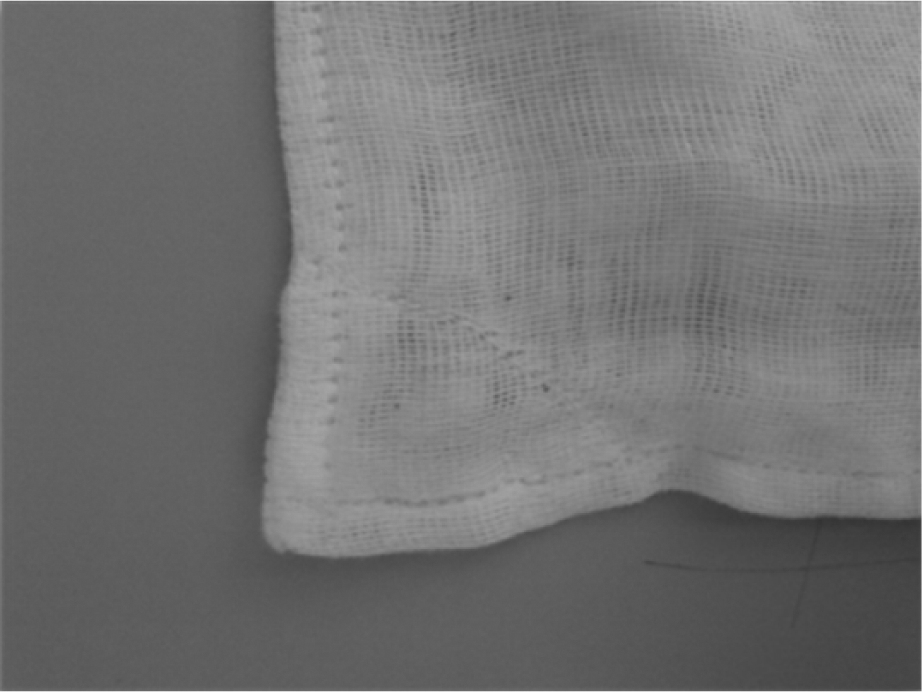
Tagged sponge; each tag is hand-sewn within the sponges.

Basket antenna for count of used sponges during and at the end of surgery.
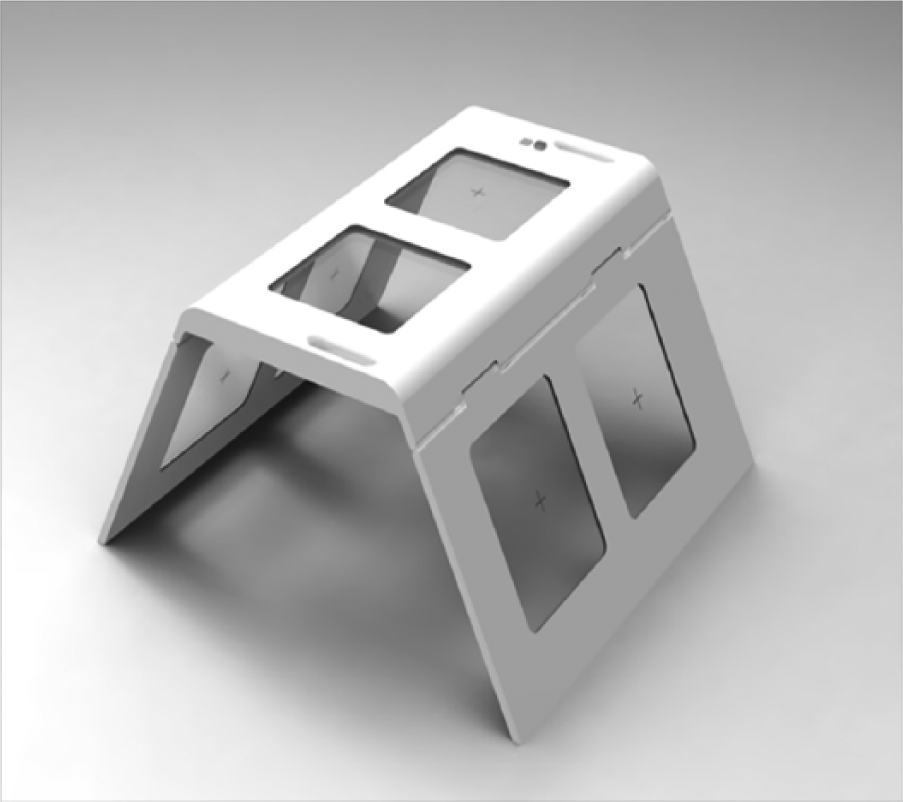
Prototype antenna for patient’s scanner to identify retained sponges.

Management software screenshot for gauze count and records compared with the traditional way of counting.
The software is designed to give information of any uneven count: it informs and alerts the operator, who can activate the check in the patient’s body through the patient scanner antenna. Before the start of the surgery, all sponges must pass through the basket antenna. A continuous counting process is performed during surgical procedure, so ongoing counts can be obtained at any moment in real time and the final one is immediate. Abdomen scanning on the OR table can be easily performed to identify the presence of retained sponges.
RFID-integrated sponges and the antennas plus software system are both new medical devices that must be compliant with the essential requirements according to European Directive 2007/47/EC of the European Parliament and of the Council of 5 September 2007 amending Council Directive 90/385/EEC on the approximation of the laws of the Member States relating to active implantable medical devices, Council Directive 93/42/EEC concerning medical devices, and Directive 98/8/EC concerning the placing of biocidal products on the market; 2007/47/EC. 12
The study was approved by the institutional review committee and conduct in accordance to the Animals (Scientific Procedures) Act 1986 (ASPA).
The initial phase of analysis was dedicated to identify the best configuration tags/antenna in terms of biocompatibility, size, reading distance, and radiated power for detection of retained sponge. The reading distance used was 15 to 30 cm, with radiated power of 2 to 4 W.
The following steps have been performed to evaluated the system by experimental in vitro and in vivo tests.
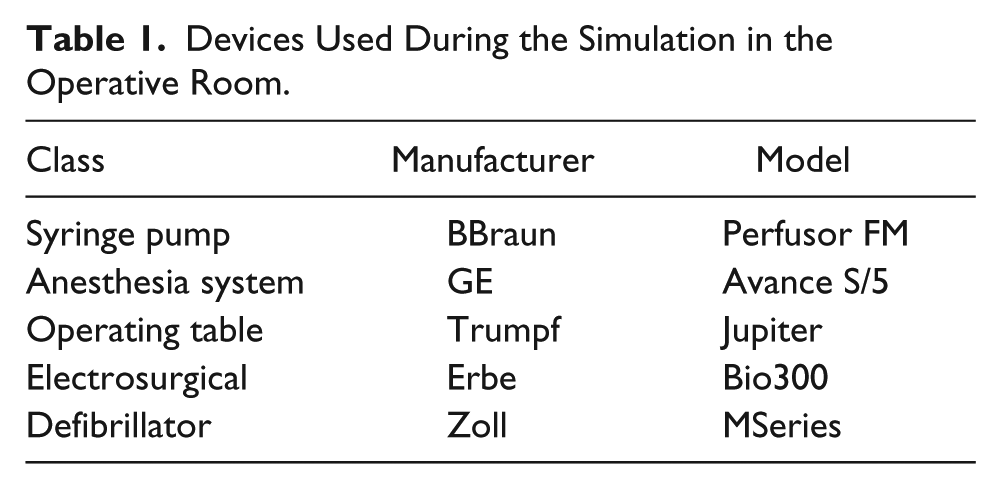
In vitro test: Preliminary in vitro tests were performed to assess the efficiency of the system, as well as to improve the ergonomics of the device. Initial tests were carried out to identify any possible electromagnetic interference (EMI), and tests were carried out according to International Electrotechnical Commission guidelines, IEC EN 60601-1-2:2007. 13 A protocol of experimental measurement to assess the presence of EMI as result of the distance between the equipment and antenna was performed by gradually moving the antenna to the OR device (electrosurgical unit, infusion, pumps, monitoring vital system, defibrillator, operating table), repeating the test at different distances (Table 1). Tests were repeated distributing the registered sponges in the OR to simulate a surgical operation and the system detection ability was investigated. Identification tests were performed positioning isolated and multiple sponges overlapped or sewn together by suture thread or agrafes. Finally, the same test was repeated with different volunteers from the team lying on the sponges or having them positioned over the abdomen and thorax to simulate retained sponges.
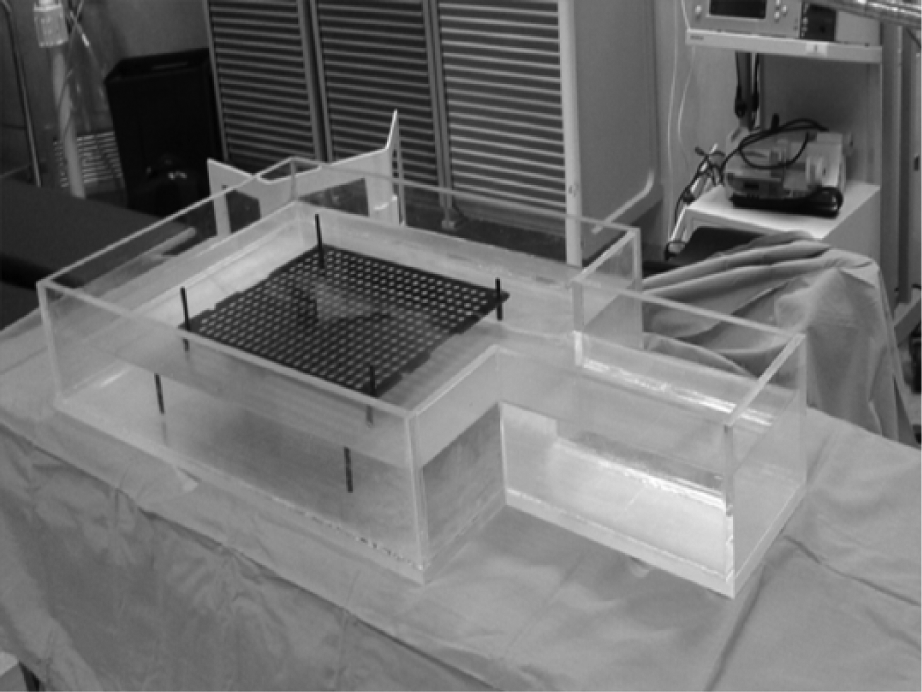
Final in vitro test: A final prototype was developed to increase the electrical and mechanical safety. We conducted in vitro tests in the operating theatre simulating a surgical procedure, in order to assess the maneuverability and the ease of use of the prototype. The test was designed and conducted to detect gauzes during a simulated abdominal surgical procedure, in a standard OR, with standard staff involved (2 surgeons, 1 scrub nurse, and 2 circulating nurses), with active devices normally used in daily surgical practice. All devices were connected to appropriate patient simulators, which are used by the Department of Medical Engineering to verify systematically their safety and functionality. In order to simulate the human body, a phantom was used to represent the human electromagnetic conductivity (Figure 6).
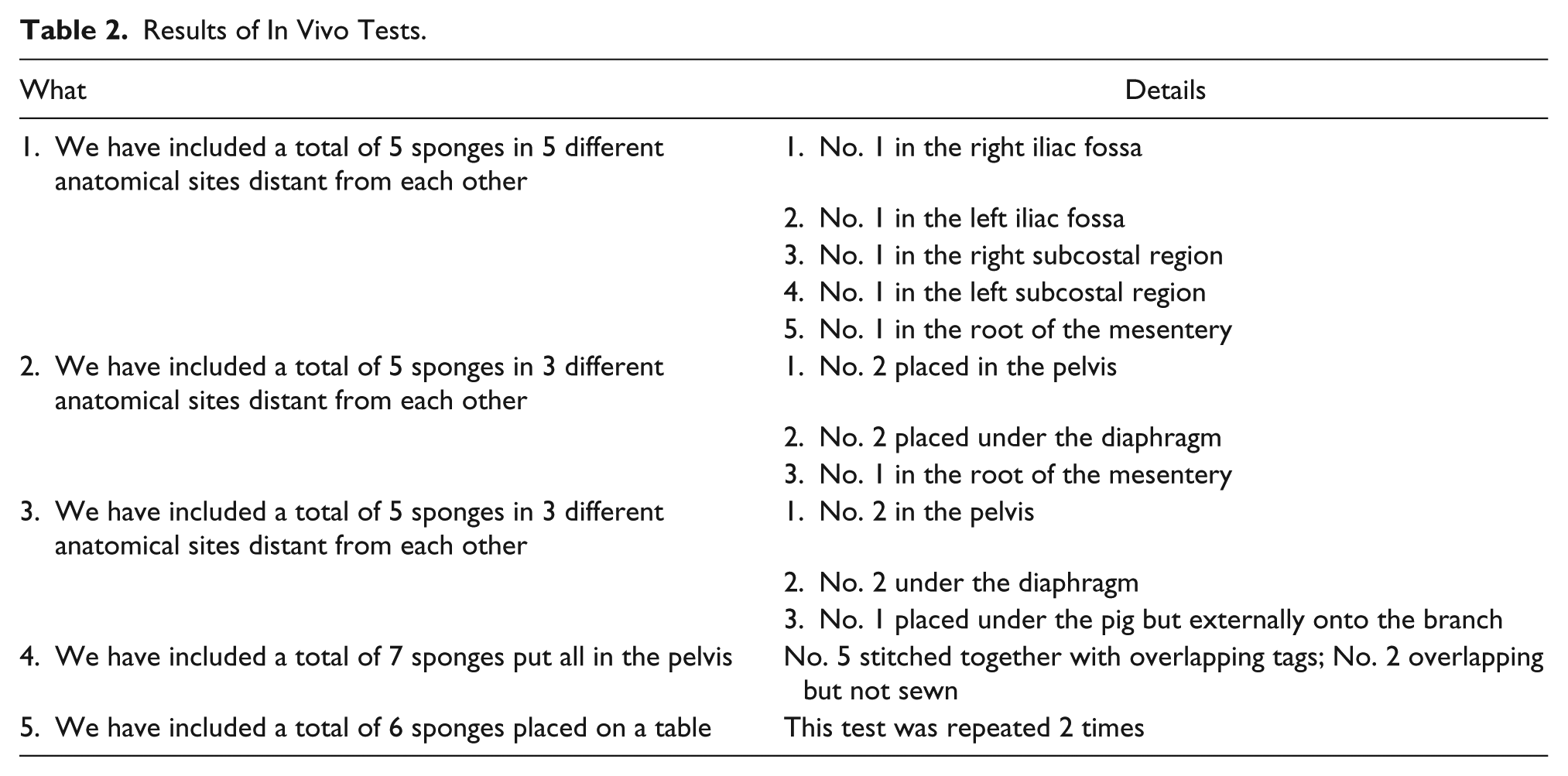
In vivo test: Further tests were conducted at the Station for Animal Technology (STA) of the University of Rome Tor Vergata. The experiments were carried out after approval of the ethics committee and according to the protocol for animal experiments. The experiment was conducted on a pig weighing 60 kg, sedated by intravenous/inhalation (propofol/isoflurane) and premedication (atropine, medetomidine, acepromazine) with ongoing cardiopulmonary monitoring. Tagged sponges were inserted, during open abdominal surgery, into different locations of the abdominal cavity through a midline incision. Others were placed outside the animal. The anti-collision protocol was tested overlapping the tagged sponges (Figure 7). Five different tests were performed and repeated 3 times each, as described in Table 2.
Devices Used During the Simulation in the Operative Room.

Phantom used during in vitro test.
In vivo test to simulate retention during surgery.
Results of In Vivo Tests.
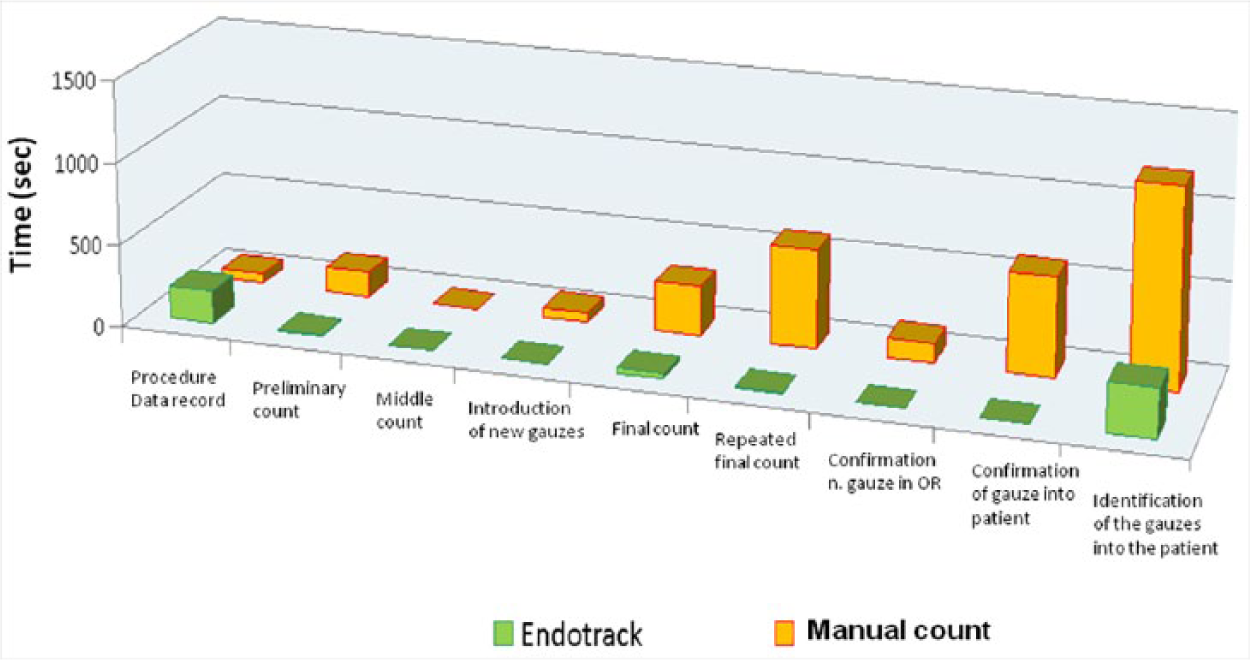
To assess advantages in terms of time saved, we measured the average time for counting during standard surgical abdominal procedures (Figure 8). We analyzed the mean time spent for sponge counting in 1 month of surgical activity and the time spent for counting with our RFID system during in vivo simulation. We considered the following: time spent for the checklist, initial count, ongoing count (time to count further sponges added), and final count. In case of mismatch we considered time to repeat count, confirmation of gauze loss, and time to identify gauze in the patient’s body.
Measuring of saved time comparing manual gauze count versus radiofrequency gauze identification.
Results
Tests performed to record any type of interference between the RFID system and the electromedical device present in the OR were negative for malfunction of all the involved devices. An antenna with emission power up to 10 W in high frequency was placed around the medical equipment, from a distance of 2 m until contact with the device, and the interposition of the operating table or any other active OR devices did not affect the performance of the reader. Thus, the system was able to give the correct count of all gauzes distributed in the OR. Both in vitro and in vivo tests were performed with single and multiple tags and the real-time detection rate was 100%. No false positive and false negative have been observed, and sensitivity and specificity were 100%. The mean BMI of 5 volunteers who participated in the ex vivo experimental phase was 28.7 kg/m2 (ranging from 22 to 31 kg/m2). Furthermore, the detection of multiple tagged sponges randomly crumpled and overlapped was tested and the sponges were correctly detected, identifying their number in all tests, including when they were positioned in the body cavity. The maximum reading distance of the body scan antenna prototype reaches a range of 50 cm from each side, for a total diameter of 1 m. Also in case of sponges presenting agrafes (previously applied with the aim to simulate a common condition following a mechanic anastomosis) no interference was demonstrated in phantom and in vivo models. The other 2 reader antennae, the check antenna for initial count and the other one placed in the basket for used gauzes, showed a maximum reading distance of 30 to 40 cm.
Results concerning time saving by the RFID Endotrack system compared to the manual standard count procedure are reported in Figure 8. A global time consuming reduction, up to 75%, has been recorded using the Endotrack system due to the real-time count operated by the software and the short time (less than 1 minute) required by the body scanner antenna to identify the retained sponges. Time saving using our automated system was about of 28 minutes for each surgical procedure. This time has been calculated comparing the average time spent on sponge counting in real surgical procedures in a month of surgical activity with simulation of the final in vitro test.
Discussion
Health care providers are paying greater attention on increasing patient safety during surgical practice, and the event of a gossypiboma is an hot topics implying medical and legal sequelae with a great impact on patients’ health and institution image.
Despite existing strict protocols, guidelines, and checklists, in an effort to promote positive patient outcomes and safety in the OR, the record of gossypiboma sentinel event is not infrequent. Gauzes have been reported to be the most frequent retained issue, especially in surgical procedure involving body cavity. Miscounting can arise from multiple factors such as incorrect gauze packaging, defective gauzes, or excess gauzes (9 or 11 sponges packed instead of 10), human errors during manual count, the shift change of the scrub nurses during the procedure, and the sending out sponges from the OR (eg, with the specimen). Used sponges, embedded with blood and biological fluids, are difficult to detect in the patient’s body and between organs during surgical procedures, especially during emergency cases and in obese patients. In case the final count is different from the initial one, usually an X-ray should detect the error. In order to reduce incidence of gossypiboma, sponges equipped with radiopaque strips have become the standard, to allow identification by X-ray. In case of sponge count mismatch, the amount of time spent searching for the missing gauze exposes the patient to prolonged anesthesia and will surely result in longer operative time and economical disadvantages for hospitals. According to the New York Cardiac Surgery Report data, for coronary heart by-pass grafting (CABG) procedures, on the basis of the national volume of CABG operations per year (347 570 in 2004), considering portable X-ray costs and additional procedure time, the estimated cost of count discrepancies for this procedure alone is $24 million. 14 The costs of reoperation for retained foreign bodies are relevant. According to a report by Blue Cross, Blue Shield on thoracic procedures, reoperating on a thoracic patient to retrieve a sponge and then treat for an infection or foreign body reaction can cost $50 000 or more than the original surgery. 15 The Agency for Healthcare Research and Quality indicates that a retained foreign body adds approximately 4 days to an average hospital stay. 16
Hospitals need to develop systems to prevent human errors; in fact, some US insurance companies stopped refunding providers for procedures involving a foreign object left behind from a surgery.
For this reason, new technologies to improve sponge count and reduce human errors are under development.
Technology oriented solutions have been proposed to track items with an RFID device support in the surgical background.
RFID technology is largely applied in industrial fields (ie, automotive, retail, public administration, and transport), and it could be the potential solution to improve patient safety. The RFID and wireless technology applications have had a slow introduction in the surgical theatre, due to the need of avoiding interferences with existing monitoring and diagnostic equipment. Three main technologies are actually available to prevent sponges gossypiboma, Bar-coded sponge system (SurgiCount Medical, Temecula, CA), RF-tagged sponge system (Blair-Port Wand model and RF Mat Assure Detection System, RF Surgical System Inc), which are already commercialized, and experimental prototype of RFID tracking system.
Bar-coded systems, based on a handheld scanner of the bar-coded sponge at the beginning of the procedure, have shown in a clinical trial including 298 surgical procedures 17 to be efficient to prevent sponges error count comparing to manual count protocol, but do not provide a body scanner system able to identified retained sponges.
The RF-tagged sponge system product by Surgical System Inc is available in 2 different formats: the wand and the mat. The system does not aim to improve the accuracy of the sponges count, but to identify retained sponges in a patient’s body by performing a body scan during or at the end of the surgical procedure. In case of retained sponges identification a sound signal is emitted by the system. The wand requires a body scan performed by an operator holding and moving the device along and around patient’s body. The mat instead is operator-independent, and a patient is placed on it and the device is activated to perform the scan. A comparative study of the 2 device have been performed simulating detection of retained surgical sponges in a sample of volunteer patients including obese patients (total 117 patients, 85 obese). 9 The mat showed a sensitivity of 98.1% and specificity of 100%, reporting 12 false negative out of RF 812 reading; but considering only the morbid obese study population the sensitivity decreased to 96.9%. The negative predictive value of the mat device was 86.7% against 100% while using the wand. The sensitivity of the wand was tested on 117 subjects already tested by the mat.
Concerning the RFID prototype, Kranzfelder et al have developed a tracking system reporting 100% success in vitro tests; however, during in vivo tests successful sponge detection decreased to 70%. 18 RFID application seems to increase detection accuracy for retained sponges, but the same authors demonstrated declining accuracy when sponges were overlapped. 18
Rivera et al 19 have developed ASSIST, an automated system to track instruments and sponges with a detection rate of 95%.
Another study showed a detection accuracy of 100%, using a high-frequency RFID handheld device, but despite the success, the possibility of human error persists, arising from incorrect scan performed. 20
Our RFID technology is based on a high-frequency device and the transponders are detected by 6 antennas. They are assembled on a device that surrounds the patient, meaning that the entire body is within the detection field making the procedure more independent from OR personnel’s skills. This should increase the accuracy of the system, especially when sponges are overlapped or blood soaked. Moreover, the body antennae allow to perform a whole body scan without changing patients’ position, and the antennae are placed in the upper and lateral sides of the device performing a contemporary scan in multiple planes and directions. This design improves the efficacy of the scan if compared to the handheld operator-dependent device or the mat system. The minor sensitivity reported by the mat in obese patients should be due to a missed reading in case of sponges sited in the later anterior part of the abdomen that should be outside of the reading field.
These theoretical concepts, inspiring our instrument design, have been experimentally confirmed. The staff evaluated the software in terms of available functions, intuitiveness of the interface, speed in recording, and saving data; the clinicians evaluated the ergonomics and maneuverability of the antennas; both the evaluations were fully positive. Experimental data have shown an excellent accuracy of the system, in detecting gauzes, outside and inside the body, more maneuverability of the 6 detector antennae, resulting in a user-friendly interface. In our series, we recorded 100% success in readings, in all conditions explained above. Apart from safety, a relevant advantage is represented by time saving. During counts, nurses are unfocused from the surgical procedure with a significant increase in the OR time, and our system allows to perform a real-time count in every moment of the surgery avoiding the manual time-consuming procedure.
Conclusion
The use of our RFID system leads to a better accuracy in sponge count with relevant time saving during surgical procedures as well as a significant decrease in X-ray usage.
Our preclinical evaluation and preliminary results are encouraging and the prototype has correctly identified the number of sponges in both in vitro and in vivo tests. Efficacy and repeatability of the prototype have also been demonstrated.
Preclinical experimentation has led to satisfactory results, respecting the efficiency and repeatability of measurements; however, further technological advances and clinical trials are needed to confirm the reliability and applicability of our system.
Footnotes
Acknowledgements
The authors thank Dr Silvia Colangelo, Eng, PhD, Medical Engineering Service, Fondazione Policlinico di Tor Vergata, Rome, Italy, and Mr Stefano Croci, Luigi Salvadori Spa, respectively, for their support of this research through provision of data and data management support.
Authors’ Note
Institutional review board approval and informed consent were obtained from all individual participants included in the study.
Author Contributions
Study concept and design: Alessandra Lazzaro, Arianna Corona, Luca Iezzi, Silvia Quaresima, Luca Armisi, Ilaria Piccolo, Carlo Maria Medaglia, Sergio Sbrenni, Pierpaolo Sileri, Nicola Rosato, Achille Lucio Gaspari, and Nicola Di Lorenzo
Acquisition of data: Alessandra Lazzaro, Arianna Corona, Luca Iezzi, Silvia Quaresima, Luca Armisi, Ilaria Piccolo, Carlo Maria Medaglia, Sergio Sbrenni, Pierpaolo Sileri, Nicola Rosato, Achille Lucio Gaspari and Nicola Di Lorenzo
Analysis and interpretation: Alessandra Lazzaro, Arianna Corona, Luca Iezzi, Silvia Quaresima, Luca Armisi, Ilaria Piccolo, Carlo Maria Medaglia, Sergio Sbrenni, Pierpaolo Sileri, Nicola Rosato, Achille Lucio Gaspari and Nicola Di Lorenzo
Study supervision: Alessandra Lazzaro, Arianna Corona, Luca Iezzi, Silvia Quaresima, Luca Armisi, Ilaria Piccolo, Carlo Maria Medaglia, Sergio Sbrenni, Pierpaolo Sileri, Nicola Rosato, Achille Lucio Gaspari and Nicola Di Lorenzo
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by FILAS (Financing, Innovation and Research) through a grant, under a call promoting the research and technological innovation (POR FESR Lazio 2007-2013 Asse I).