
Abstract
Purpose. Absorbable meshes used in inguinal hernia repair are believed to result in less chronic pain than permanent meshes, but concerns remain whether absorbable meshes result in an increased risk of recurrence. The aim of this study was to present an overview of the advantages and limitations of fully absorbable meshes for the repair of inguinal hernias, focusing mainly on postoperative pain and recurrence. Methods. This systematic review with meta-analyses is based on searches in PubMed, Embase, Cochrane, and Psychinfo. Included study designs were case series, cohort studies, randomized controlled trials (RCTs), and non-RCTs. Studies had to include adult patients undergoing an inguinal hernia repair with a fully absorbable mesh. Results. The meta-analyses showed no difference in recurrence rates (median 18 months follow-up) and chronic pain rates (1 year follow-up) between absorbable- and permanent meshes. Crude chronic pain rates for the RCTs were 2.1% for the absorbable meshes and 7.6% for the permanent meshes. For the absorbable meshes, medial hernias were more susceptible for recurrence compared with lateral hernias (P < .0005). None of the studies reported allergic reactions or other serious adverse events related to the absorbable mesh. Conclusions. Patients with an absorbable mesh seem to have less chronic pain following inguinal hernia surgery compared with permanent meshes, without increased risk of recurrence.
Introduction
Worldwide, more than 20 million inguinal hernia operations are performed annually 1 and surgeons have used synthetic permanent meshes to prevent recurrences for decades. 2 One of the disadvantages of inguinal hernia repair is that some patients develop postoperative chronic pain. 3 There may be numerous mechanisms behind this, of which traumatic mesh fixation, inflammatory reactions, and mesh shrinkage may be involved. The meshes induce an inflammatory response in the surrounding tissue that can persist for many years, resulting in scar tissue formation. 4 If synthetic meshes with less polypropylene are used, the inflammation of the surrounding tissue is reduced as well, 5 which in turn leads to less connective tissue formation. 4 In recent years, there has been a tendency to use meshes with less material—so-called lightweight meshes. A meta-analysis that compared lightweight with heavyweight meshes in Lichtenstein repair showed that patients with lightweight meshes had significantly less postoperative chronic pain and foreign body sensation. 6 The principle of using less foreign material in inguinal hernia surgery is further expanded with the use of meshes that are fully absorbed over time.
Surgeons have started using absorbable meshes (biological or synthetic absorbable) in the repair of inguinal hernias, and several types of meshes are currently on the market, see Table 1. Biological meshes have furthermore been used with promising results in patients where permanent meshes have been judged to be too risky in terms of complications, that is, in patients with a high risk of infection. 13 Absorbable meshes are thought to serve as a regenerative scaffold for new tissue ingrowth and collagen deposition. 7 Since the meshes are fully absorbed, they might give rise to less chronic pain. However, since the meshes completely disappear, leaving only the collagen deposition to prevent a recurrence, concerns remain whether the recurrence rate is higher for absorbable meshes compared with permanent meshes. If the recurrence rate is high, the positive effects on other postoperative complications may not justify the use of absorbable meshes.
Summary of the Absorbable Meshes Used in the Included Studies.
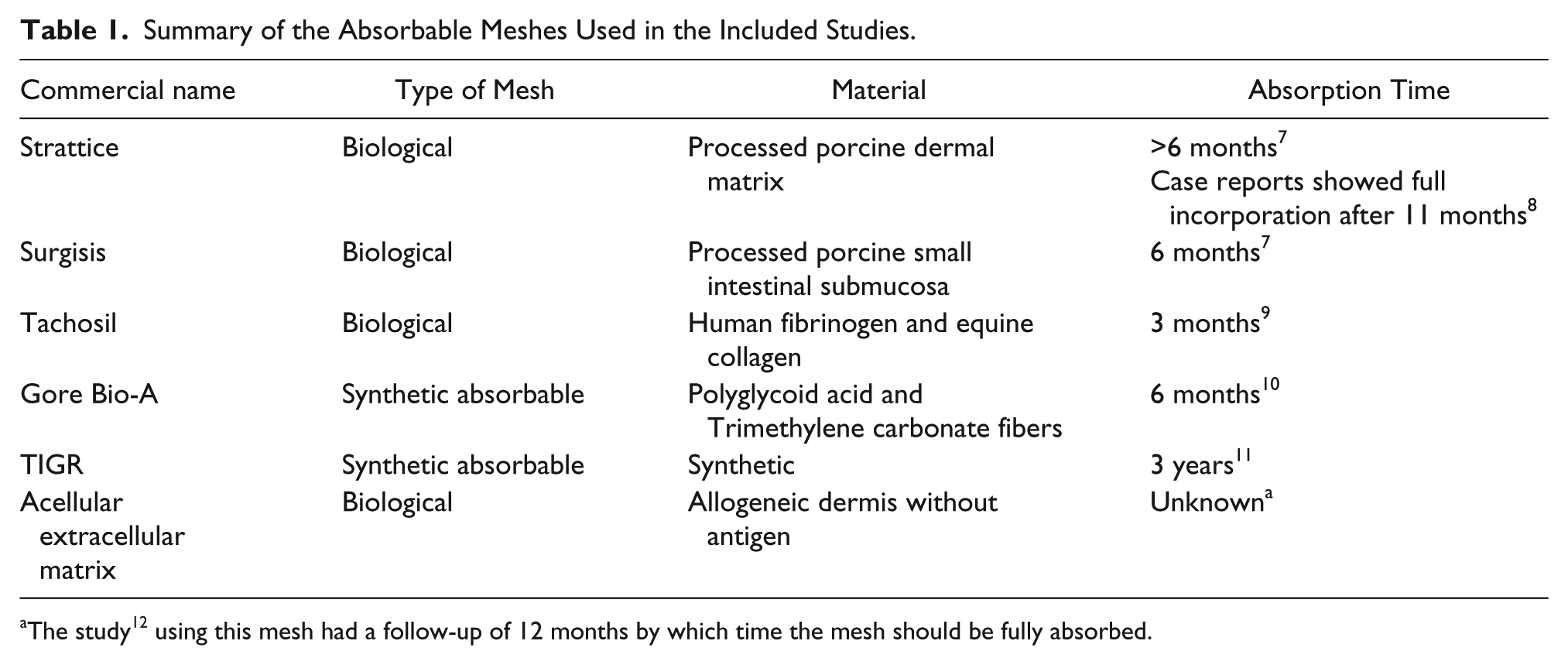
The study 12 using this mesh had a follow-up of 12 months by which time the mesh should be fully absorbed.
The aim of this study was to investigate the advantages and limitations of using fully absorbable meshes in inguinal hernia surgery, with the main focus on pain and recurrence.
Methods
This systematic review and meta-analysis was reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 14 The protocol was registered at PROSPERO (http://www.crd.york.ac.uk/PROSPERO/) with the registration number CRD42015017385. The eligibility criteria were studies that included adults with a primary inguinal hernia, or inguinal hernias for which the preoperative status (primary/recurrent) was unknown, who underwent elective inguinal hernia operations with mesh implantation. A fully absorbable mesh had to be used in at least some of the patients. Included study designs were case series, cohort studies, randomized controlled trials (RCTs), and non-RCTs. Case reports and reviews were excluded. Studies reported in either English or Scandinavian languages were included.
The main outcomes were postoperative pain and recurrence, where chronic postoperative pain was defined as persistent pain minimum 6 months postoperatively.15,16 Secondary outcomes were mobilization and activity, per-operative complications and other objective outcomes including seroma, hematoma, and wound infection. The secondary outcomes did not have to be reported in order for the study to be included.
We conducted searches in 4 databases: PubMed (last searched December 2, 2014), Embase, Cochrane, and Psychinfo (last searched December 4, 2014). In brief, the search terms included “inguinal hernia AND absorbable meshes”. The reference lists for full-text articles were screened for relevant studies. The search strategy had no limits and the search in PubMed can be seen on the following webpage: http://www.crd.york.ac.uk/PROSPEROFILES/17385_STRATEGY_20150209.pdf. The search strategy was modified for the other databases but kept as similar as possible.
All studies were screened on title and abstract according to the prespecified eligibility criteria by the first and second author independently in a standardized fashion. Disagreements about inclusion were resolved by discussion until consensus was reached. The same procedure was used for the inclusion of the full-text studies. The data extraction process was primarily conducted by the first author to a premade Excel sheet. It was tested by extracting data from 2 of the included studies, after which it was slightly modified and data were extracted in the same manner for all studies. When there were any doubts, agreement was reached between the first and second author in the same way as for the study selection process. The study characteristics are presented in Table 2.
Characteristics of the Included Studies.
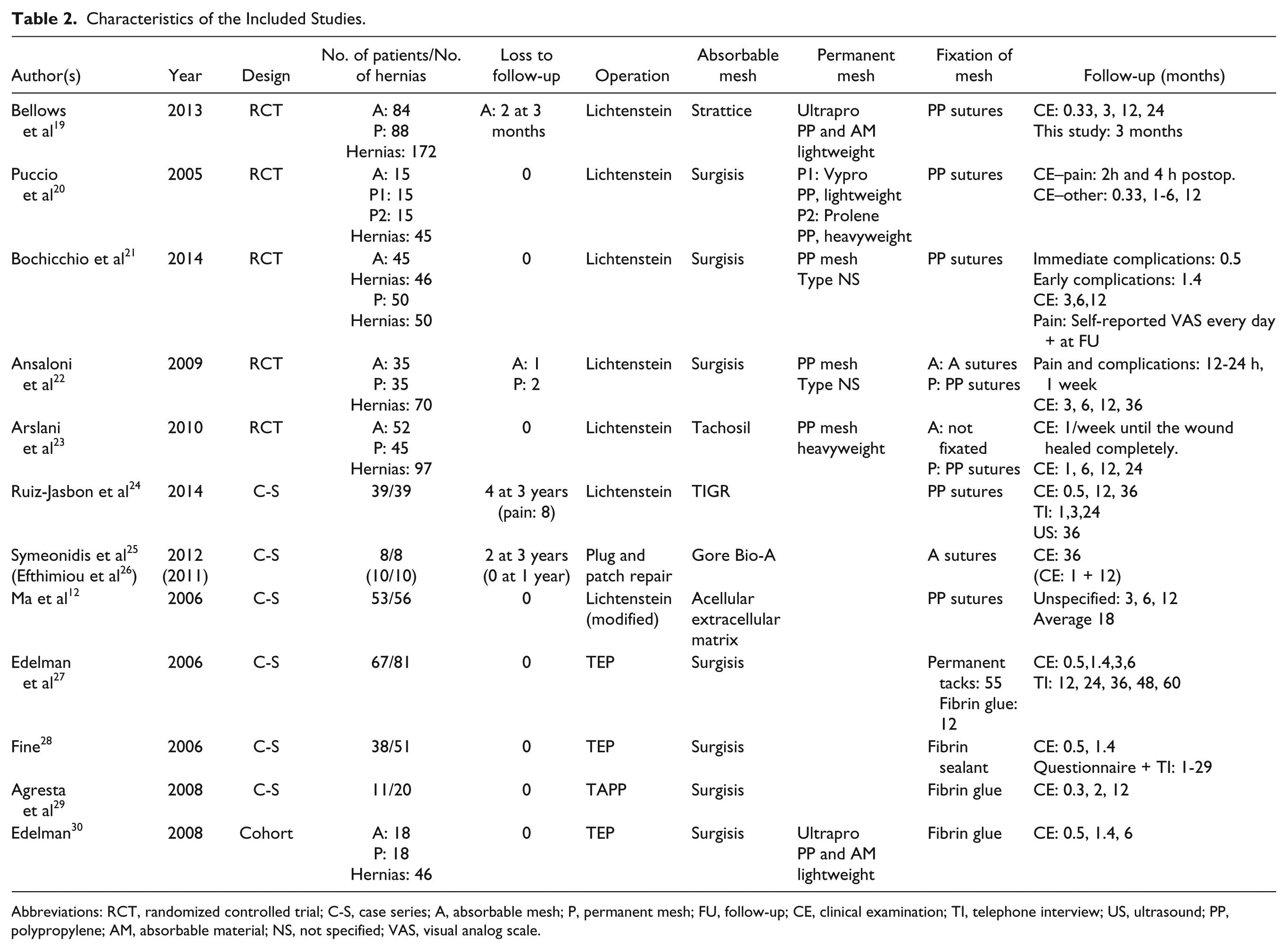
Abbreviations: RCT, randomized controlled trial; C-S, case series; A, absorbable mesh; P, permanent mesh; FU, follow-up; CE, clinical examination; TI, telephone interview; US, ultrasound; PP, polypropylene; AM, absorbable material; NS, not specified; VAS, visual analog scale.
Risk of bias was assessed for each study. The cohort study was assessed by the “Newcastle-Ottawa Quality Assessment Scale.” 17 For the case series, there is no bias assessment tool that we know of and they were assessed in the same way as the cohort studies, with the exception that comparability could not be assessed. This resulted in a modified scale, where a maximum of three stars could be given for “selection.” RCTs were assessed according to the Cochrane bias assessment tool, and for “other bias,” for example conflict of interest was assessed. The first author assessed bias and the second author reviewed the studies, agreement again being reached by discussion. To assess risk of publication bias for the RCTs, we used funnel plots for the outcomes used in the meta-analyses (not shown).
The meta-analyses were performed in Review Manager 5.3 (The Cochrane Collaboration, 2014) using risk difference or risk ratio (including confidence intervals) and presented in forest plots. Only RCTs were included in the meta-analyses, and minimum 2 clinically homogenous studies were required. Measurement of heterogeneity (I2) was calculated. I2 ranges from 0-100%, where 0% means that the studies are as homogenous as possible and 100% means that the studies are as heterogeneous as possible. Studies should be homogeneous, in other words have a low I2, to increase the possibility that the same outcome is compared. 18 The summary measures for the observational studies were crude rates, that is, number of patients with the outcome divided by number of patients (or hernias) followed. Outcomes were analyzed per protocol when possible.
Results
A total of 13 studies were included,12,19-30 3 of them comprising the same study population with different follow-up periods,25,26 leaving a total of 12 studies with unique participants. Figure 1—the PRISMA flow diagram—presents details of the studies screened and excluded. A kappa value of 0.78 was calculated for the agreement between the first and second authors in screening the title and abstracts. Study characteristics are presented in Table 2. All studies reported recurrence and pain. The study designs were 5 RCTs, 1 cohort study, and 6 case series. A total of 467 participants received an absorbable mesh out of a total of 733 participants. The biological Surgisis mesh was used in 7 studies, whereas the remaining 5 studies used different absorbable meshes, and all permanent meshes consisted at least partly of polypropylene. All RCTs performed the Lichtenstein repair, and all but one of the observational studies used either Lichtenstein or laparoscopic repairs.
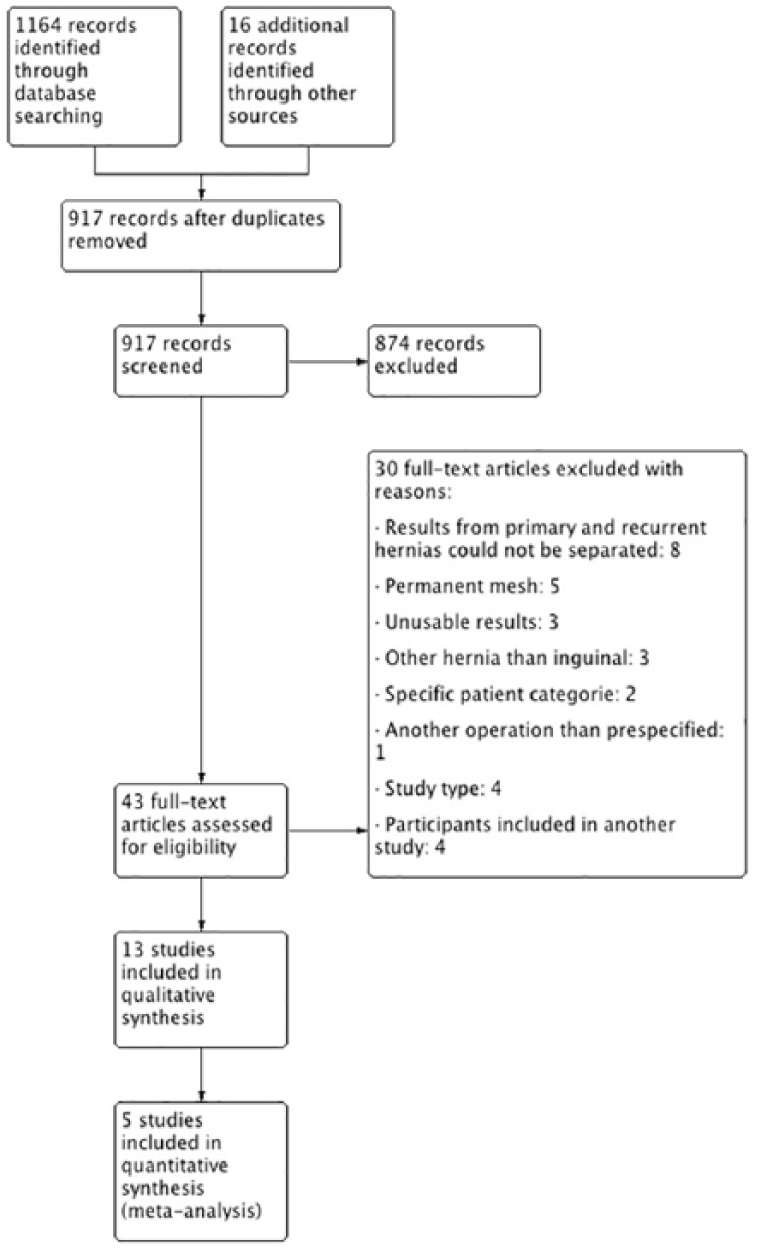
PRISMA flow diagram.
Risk of Bias
Bias assessments of the 5 RCTs19-23 are presented in Figures 2 and 3. In general, there was a low risk of bias, shown by the majority of green colors in the figures. We assessed a low risk of publication bias for the outcomes in the meta-analyses (only assessed for Figure 4a-d). For the cohort study, 30 we assessed the study to have a moderate risk of bias, since the study did not report statistics on the baseline characteristics and therefore incurred a risk of selection bias. Regarding the case series, the risk of bias was low for the selection part, and to receive all stars, the studies had to report preoperative pain (only reported for 1 study 24 ). The majority scored all stars on the outcome parameter, resulting in a low general assessed risk of bias. Reasons for lacking the 1 star were either because of a short follow-up time 28 or because of a large loss to follow-up. 25

Bias assessment for randomized controlled trials —table form.
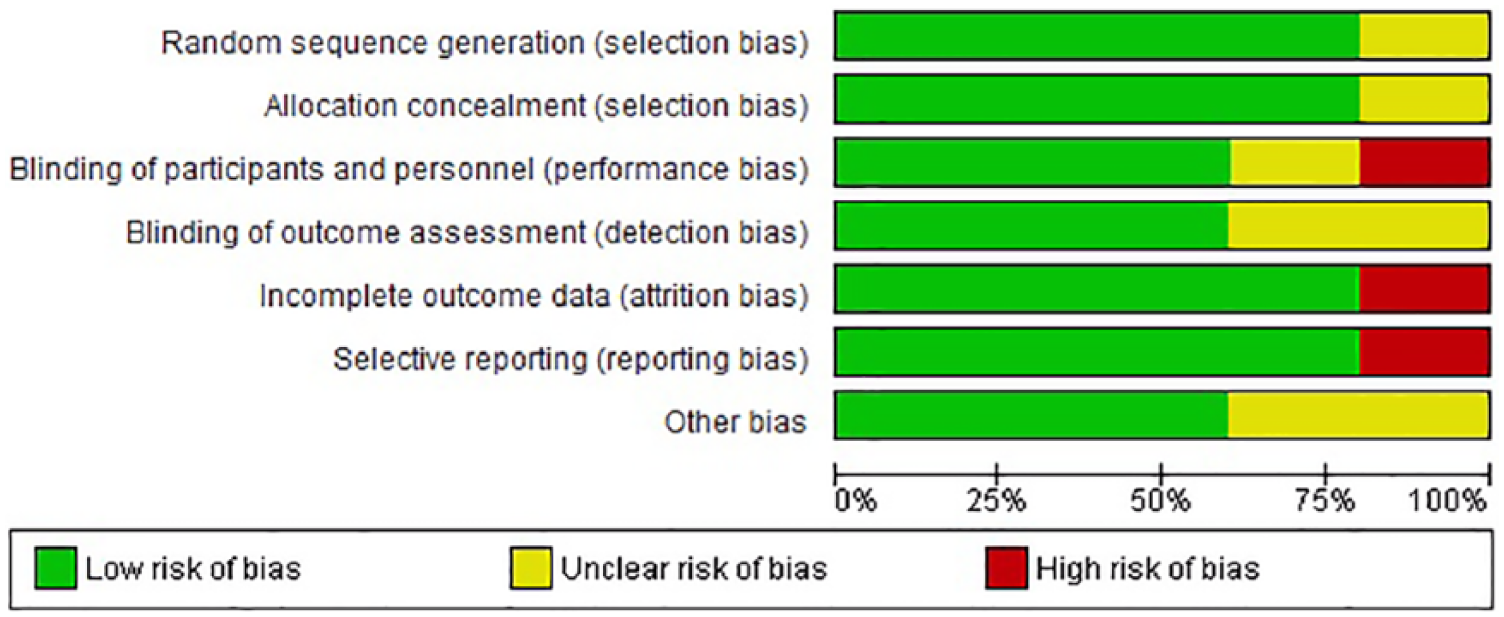
Bias assessment for randomized controlled trials—graphic form.
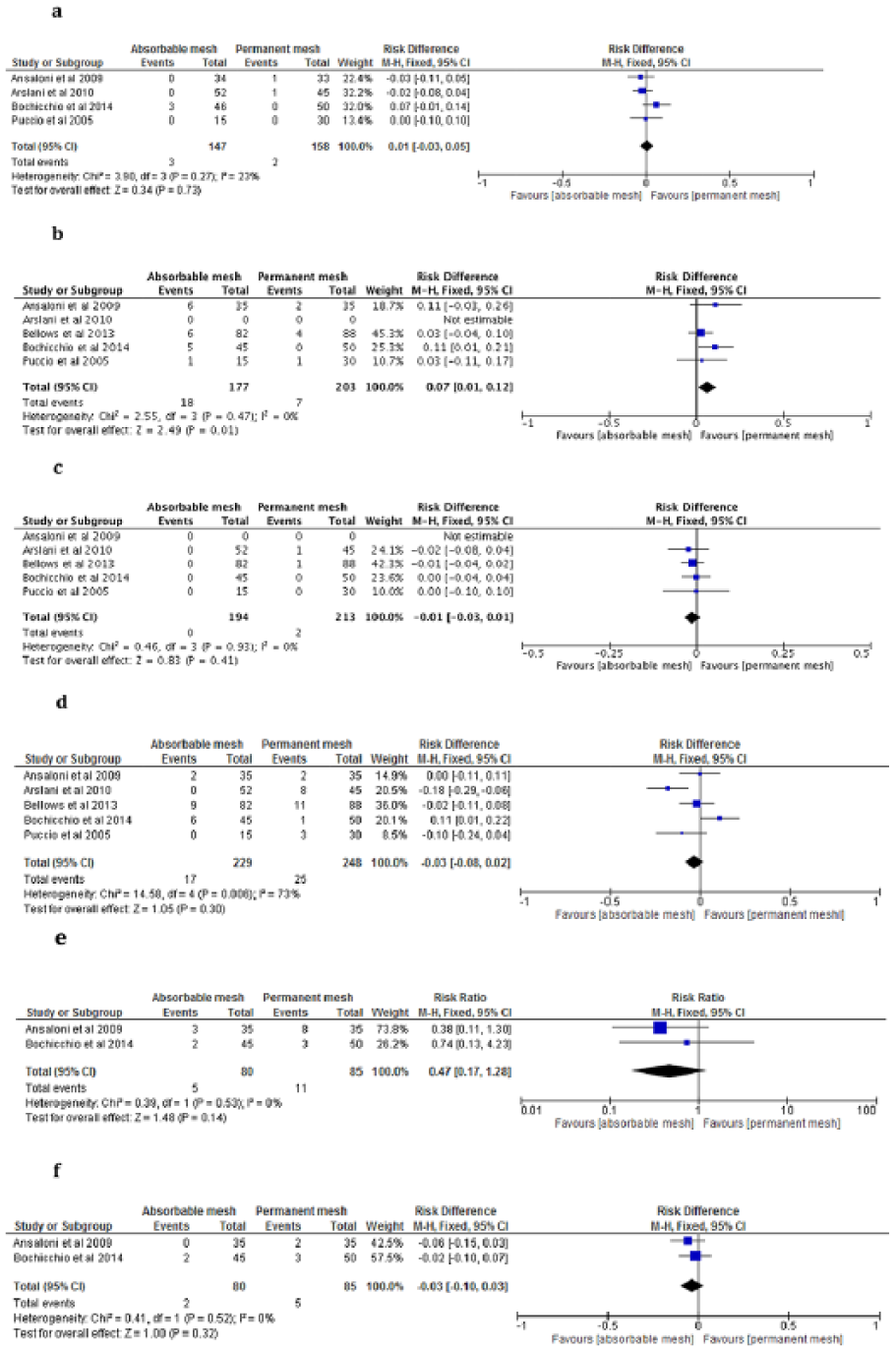
Meta-analyses: (a) recurrence, (b) seroma (earliest results chosen), (c) infection, (d) hematoma, (e) chronic pain (all pain), and (f) chronic pain (moderate/severe).
Recurrence
Recurrence rates are presented in Table 3. One study did not have sufficient follow-up to ensure full absorption of the absorbable mesh, and this study was therefore excluded when reporting recurrence rates. 19 The total recurrence rate for absorbable meshes was 5.6%.12,20-25,27-30 with a median follow-up of 13 months (range 6-60 months); 2.8 % in the first postoperative year12,20,21,26,28-30 and 8.1% 2-5 years postoperatively.22-25,27 Only considering the RCTs,20-23 absorbable meshes had a recurrence rate of 2.0% compared with 1.3% for the permanent meshes; follow-up was median 18 months (range 12-36 months). A majority of the recurrences were diagnosed by clinical examination.
Recurrence.
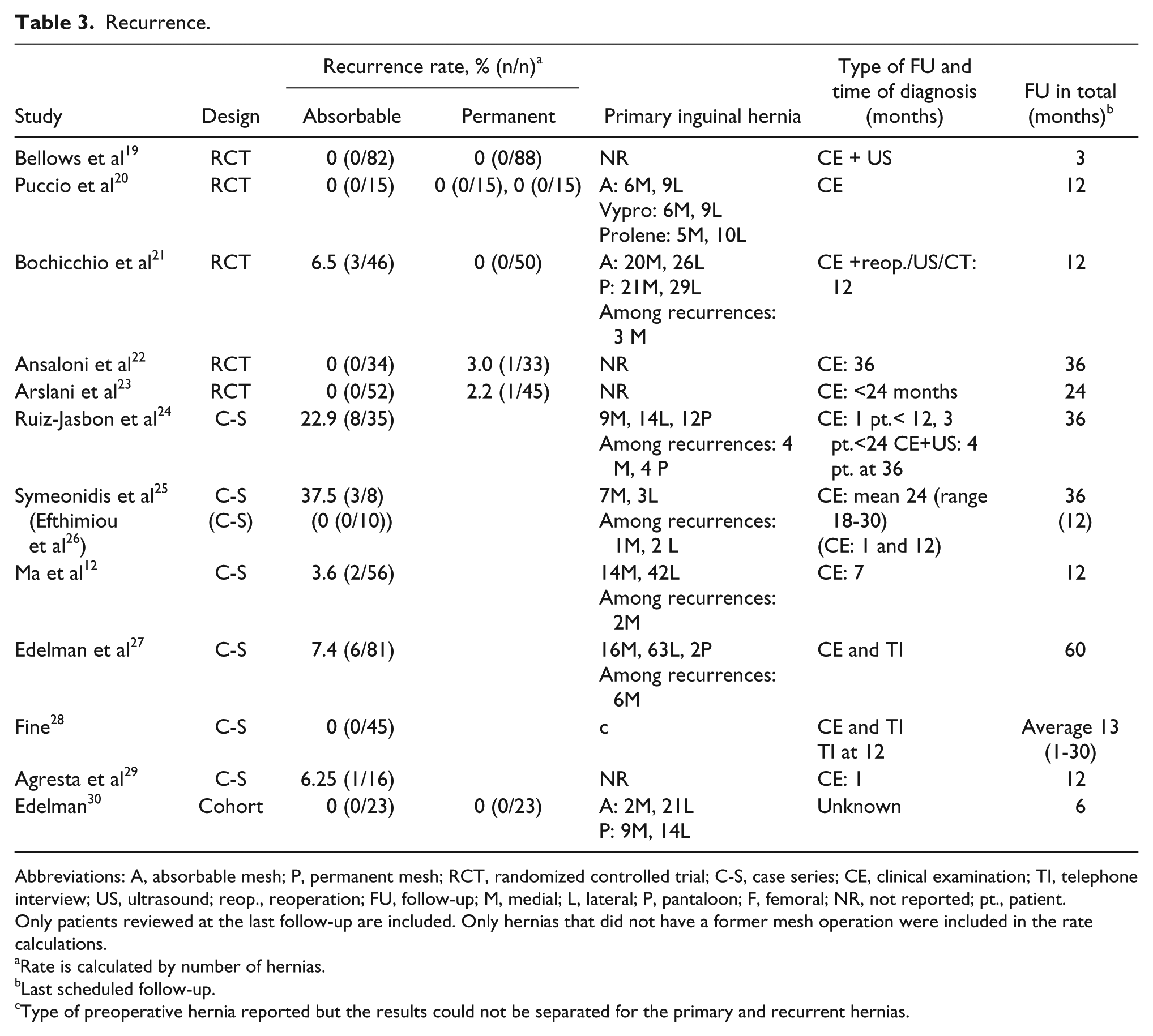
Abbreviations: A, absorbable mesh; P, permanent mesh; RCT, randomized controlled trial; C-S, case series; CE, clinical examination; TI, telephone interview; US, ultrasound; reop., reoperation; FU, follow-up; M, medial; L, lateral; P, pantaloon; F, femoral; NR, not reported; pt., patient.
Only patients reviewed at the last follow-up are included. Only hernias that did not have a former mesh operation were included in the rate calculations.
Rate is calculated by number of hernias.
Last scheduled follow-up.
Type of preoperative hernia reported but the results could not be separated for the primary and recurrent hernias.
For the permanent mesh group, the primary hernia type for recurrent hernias was not described. However, for the absorbable meshes, the type of primary hernia was described for 96% (22/23) of the hernias that recurred. Among these, 73% had a primary medial hernia, 9% a lateral, and 18% a pantaloon hernia. For the same studies, 65% of the primary hernias in total were lateral hernias and only 29% medial. Furthermore, seven studies described all primary hernias repaired in the absorbable group12,20,21,24,25,27,30. Of these, 21.6% (16/74) of the primary medial hernias and 1.1% (2/178) of the primary lateral hernias recurred (P < .0005, chi-squared test).
Pain and Discomfort
Results for pain and discomfort are presented in Supplementary Table 1.
Randomized Controlled Trials
All but one RCT 20 assessed postoperative pain with the visual analog scale (VAS) at some point during follow-up, but apart from VAS, both different measurements of pain and different follow-up times were used. Early pain: Two studies showed significantly less pain for absorbable meshes during the first postoperative days19,23 and 1 study reported significantly less pain 1 month postoperatively for the absorbable group. 22 Chronic pain: One study showed significantly less pain for absorbable meshes after 6 months, and also on movement three years postoperatively. 22 The other 3 studies that reported chronic pain showed no difference between the groups.20,21,23 Numbers with chronic pain (including mild pain) at last follow-up was 2.1% (3/146 patients) in the absorbable group and 7.6% (12/158 patients) in the permanent mesh group.20-23 When excluding mild pain, it was 1.4% (2/146) for the absorbable group and 5.7% (9/158) for the permanent group.20-23 Three of the RCTs also reported the use of analgesics during the first postoperative days.19,22,23 One study 23 showed a significant difference during the first 5 postoperative days, where a majority with absorbable meshes used no analgesic and a majority in the permanent mesh group used stronger pain medications. Another study 22 reported a significantly greater use of analgesics in the permanent mesh group after 6 months. Two20,22 of the 5 RCTs reported discomfort and 1 study found significantly less discomfort after 3 years for absorbable meshes on coughing and movement. 22
Observational Studies
Six of the studies reported chronic pain, and we report results from the last follow-up12,24,25,28-30; the type of operational approach was anterior in 3 of the studies12,24,25 and posterior in the 3 others.28-30 Four studies reported 0% chronic pain.12,25,29,30 Two studies had participants with chronic pain24,28 with a prevalence at last follow-up between 4.4% and 10.3%, depending on how pain was assessed (specified in Supplementary Table 1). Only one of the observational studies reported participants with a mesh sensation, which was present only in patients with primary medial hernias. 24
Meta-Analysis
All RCTs used the Lichtenstein repair and had an overall low assessed risk of bias. Sex and age were similar (not reported in 1 study 23 ), with 100% male patients and a mean age in both groups of 58 years (range of reported mean in the absorbable group 54-64 years; in the permanent group 54-61 years). For recurrence, 1 study was excluded due to a follow-up shorter than the absorption time of the mesh. 19 Three of the studies used the same absorbable mesh20-22 and all used a polypropylene mesh. The analysis showed no difference in recurrence rates between the absorbable and permanent meshes, and median follow-up time was 18 months (range 12-36 months) (Figure 4a). There was still no significant difference after subdividing the meta-analysis on recurrence after 1 year20,21 and recurrence after 2-3 years22,23 (these meta-analyses are not shown). Regarding other complications, permanent meshes had slightly less seroma, but no differences for hematoma or infection were found (Figure 4b-d).
Of the 4 studies reporting chronic pain,20-23 2 did not report how pain was assessed and was excluded from the meta-analyses.20,23 The remaining reported using VAS and/or SVS (simple verbal scale), and both reported pain 1 year postoperatively, and were included in the meta-analyses. Unfortunately, the studies did not report if meshes were lightweight or heavyweight. There was no difference in chronic pain 1 year postoperatively, regardless if only moderate/severe pain (when possible) or all pain was considered (Figure 4e and f).
Secondary Outcomes
Seven studies mentioned per-operative complications19-22,24,27,29: 2 studies reported patients with complications19,20 but with no significant differences between absorbable and permanent meshes. No allergic reactions in relation to the absorbable meshes were reported in any of the studies. Three RCTs reported mobilization and activity: two studies reported a significantly earlier mobilization for the absorbable group20,23 and the last study reported no difference between the groups. 19
Discussion
The meta-analyses showed no difference in recurrences between permanent and absorbable meshes. The hernias that recurred for the absorbable meshes were mostly medial, even though they constituted a small proportion of the primary hernias. Regarding pain, several studies reported results that favored the absorbable meshes and none of the RCTs favored the permanent meshes. The meta-analyses showed no difference in chronic pain. For other complications, there were no differences between the meshes apart from seroma, which was slightly higher among absorbable meshes. Finally, none of the studies reported allergic reactions related to the absorbable meshes.
The recurrence rate for all hernias with an absorbable mesh was 3% the first postoperative year and 8% after 2 to 5 years. This is slightly higher than results from a study based on the Danish Hernia Database, which reported a reoperation rate of about 4% for the Lichtenstein procedure and about 6% for laparoscopic techniques 8 years postoperatively, 31 though the true recurrence rate was probably higher. 32 For the RCTs, there was no difference in recurrence rates after median 18 months when comparing the absorbable with the permanent mesh group. The recurrent hernia type was only described for the absorbable meshes, where the majority of the recurrent hernias had a primary medial hernia, even though the overall majority of the primary hernias were lateral. Primary medial hernias have a significantly higher risk of developing a recurrence than primary lateral hernias 33 and in this study, we found that among the absorbable meshes, 22% of the primary medial hernias recurred while this was only the case for 1% of primary lateral hernias. The key factor for the absorbable meshes to prevent a recurrence is new collagen formation to replace the mesh. The etiology of inguinal hernias is not fully understood, but studies have found medial hernias to have a different connective tissue composition compared with samples from lateral hernias, and controls without an inguinal hernia.34,35 If lateral and medial hernias truly have different etiologies, 36 they may require different surgical treatments, where permanent meshes might be preferred for medial hernias.
Several of the observational studies reported no chronic pain, and since an equal number of studies had surgery by anterior and posterior approaches, and participants with chronic pain were reported for both approaches, the results do not seem to be affected by the type of surgery. Chronic pain for the absorbable group of 2% for the RCTs is furthermore low.3,37 Even though there was no difference in chronic pain rate in the meta-analyses between the absorbable and the permanent group, we were only able to include 2 clinically homogenous RCTs. There is need for RCTs describing the pain assessment methods, and with a long enough follow-up time for the mesh to be completely absorbed and to enable a recurrence to occur. Studies should also specify the primary hernia types repaired, and which types that recurred. The studies included in our meta-analyses on chronic pain did not report if the permanent meshes were lightweight or heavyweight, and since lightweight meshes have shown less long-term discomfort in open inguinal hernia repair, 38 the possible effect on our results is unknown. Mesh pore size should therefore be reported in future RCTs. Regarding discomfort, 1 observational study 24 detected a mesh sensation, which only applied to medial hernias after the meshes were fully absorbed. Since no mesh remained, the mesh sensation must arise from new collagen deposition and scar tissue that was perceptible to the patients. Regarding inguinal hernia questionnaires, it may therefore be more correct to ask whether there is a sensation of foreign material in the groin rather than to ask whether the patient has a mesh sensation. Furthermore, no complications or allergic reactions related to the absorbable meshes were registered and it seems that the meshes can be used safely.
The strengths of this study were that there was a low risk of bias for the RCTs, and a low to moderate risk of bias for the observational studies. Secondary outcomes were reported in the majority of the studies, enabling us to perform meta-analyses on “other complications.” Homogeneity in the meta-analyses was high for recurrence, chronic pain, seroma, and infection, and only hematoma had a large heterogeneity and therefore should be interpreted with caution. The absorbable meshes were expected to be fully absorbed at the time of last follow-up for all but one study, 19 which was excluded from the meta-analysis of recurrence. The type of primary hernia for recurrent hernias was well described for the absorbable meshes, which gave rise to our considerations on the etiology of inguinal hernias. Furthermore, most of the studies included clinical examinations during follow-up and median follow-up time was more than one year, allowing time for a recurrence to appear. The overall recurrence rate could furthermore be subdivided on follow-up time, which is relevant since recurrences are time dependent.
The limitations of this study were that there were only 5 RCTs and the observational studies had risk of bias due to their design. In general, we found a low risk of bias for the RCTs, but bias might be present, since there are a few items for which the assessment of risk of bias was “unknown.” If detection bias is divided into two aspects, the blinding of health care workers regarding patient-reported outcomes and objective outcomes, then the highest risk of bias overall was for detection bias from patient-reported outcomes and the lowest risk was for objective outcomes. An explanation of this is probably that an objective outcome is either present or not, whereas a patient-reported outcome, such as pain, can be modulated by how the health care worker asks the relevant questions. Therefore, the RCTs had to report how pain was assessed in order to be included in the meta-analyses about chronic pain, and we were only able to include 2 studies. For observational studies, there is always a risk of detection bias since health care workers assessing the outcome are unblinded, which in turn may result in performance bias. Specifically for the cohort study, the comparison part received no stars and an unknown risk of selection bias remains since no statistics were reported on the baseline characteristics of the groups. For the case series, there is an intrinsic risk of selection bias and nonrespondent bias. One limitation with biological meshes is the higher cost compared to commonly used permanent meshes. 39 However, one would expect the costs to decline if the meshes were more frequently used.
In conclusion, patients with an inguinal hernia repaired with an absorbable mesh do not show an increased risk of recurrence compared with permanent meshes. Regarding pain and discomfort, the results favor the use of absorbable meshes, but further RCTs assessing chronic pain are needed.
Footnotes
Author Contributions
Study concept and design: Stina Öberg, Kristoffer Andresen, Jacob Rosenberg
Acquisition of data: Stina Öberg
Analysis and interpretation: Stina Öberg, Kristoffer Andresen, Jacob Rosenberg
Study supervision: Kristoffer Andresen, Jacob Rosenberg
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: KA reports personal fees from Bard outside the submitted work. JR reports grants and personal fees from Bard, personal fees from Merck, outside the submitted work.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.