
Abstract
Keywords
Introduction
In recent years, the procedure known as transanal minimally invasive surgery (TAMIS) has become increasingly popular. TAMIS is defined as the use of any multichannel port combined with ordinary laparoscopic instruments, camera lens, and an insufflator for transanal surgical procedures. Reported by Atallah et al in 2010, 1 the technique stems from the use of a single port initially designed for abdominal surgery. Currently, in the United States there are 2 ports with Food and Drug Administration approval for TAMIS. They are the SILS Port (Covidien, Minneapolis, MN) and the GelPOINT Path Transanal Access Platform (Applied Medical, Rancho Santa Margarita, CA). The latter is the only multichannel port specifically designed for TAMIS procedures (Figure 1).

TAMIS port in lithotomy position.
The majority of transanal endoscopic surgical reported series were using transanal endoscopic microsurgery (TEM) or transanal endoscopic operation (TEO) rigid platforms. Due to the scarce amount of published data, it would be of interest to report and evaluate the results of more TAMIS procedures, including margin status, specimen fragmentation, and complications associated with the technique in a similar way to the TEM-TEO series. The aim of this study was to evaluate the feasibility, safety, perioperative morbidity, and short-term outcomes of the TAMIS technique in a colorectal unit with large expertise in advanced laparoscopic colorectal procedures but no previous experience in transanal endoscopic surgery.
Material and Methods
Patients
The study, approved by the institutional review board, is a descriptive review of prospectively collected data from 32 consecutive patients who underwent TAMIS procedures in our colorectal unit over a 40-month period, beginning in 2012. Preoperative workup includes physical exploration, with digital rectal examination, fecal incontinence score, tumor markers assay, endoscopy with biopsies, endoscopic rectal ultrasound (ERUS) and/or pelvic magnetic resonance imaging (MRI) and abdominal computed tomography (CT) in case of malignancies. Tumors were classified according to the American Joint Committee on Cancer and Union for International Cancer Control protocols. 2 Informed consent was obtained from all patients. Mechanical bowel preparation and antibiotic and antithrombotic prophylaxis were administered, following our standard protocol of rectal surgery.
Operative Technique
GelPOINT Path port was used in all cases. Anesthesia was usually general, but could also be spinal. The majority of procedures were performed in a lithotomy position. However, we recommend turning the patient for large anterior lesions, especially if the distance from the anal verge is in a range where there might be a risk of peritoneal entry.
The pneumorectum is maintained at a constant pressure. The rectal distension created in this way exposes the tumor and the rectal wall. A 5-mm and 30° laparoscopic camera lens was used. As previously described, 3 we recommend beginning the dissection making a dotted line with the monopolar hook about 10 mm from the tumor. We then open the mucosa along the dotted line and begin the full-thickness excision of the rectal wall, reaching the mesorectal fat using an ultrasound scalpel (Ultracision, Ethicon Endo-Surgery, Somerville, NJ). The specimen is pinned on a board and sent fresh for pathological examination. We usually wash the rectal defect with diluted povidone. We also recommend exsufflation of the rectum after complete resection, wait 3 to 5 minutes and reinsufflate in order to ensure good hemostasis. Our standard procedure includes the closure of all defects. The wound is sutured transversally to avoid stenosis of the rectal lumen and postoperative bleeding. Suturing in this area is sometimes difficult for technical reasons, as the working space is limited. If the defect cannot be completely closed, it should be reduced as much as possible, especially the upper part, due to the risk of perforation. We normally use barbed sutures in a running stitch, but interrupted knots may sometimes be preferred.
Outcomes
Demographic data, indications, tumor characteristics, morbidity, and short-term follow-up data were collected. Primary endpoints included feasibility, safety, perioperative morbidity (including peritoneal opening), and resection quality (fragmentation and microscopic incomplete resection of lateral and deep margins, R1 resection).
We consider unfavorable histological characteristics (high-risk carcinomas): tumors larger than 3 cm or affecting more than one third of the rectal lumen, rectal wall invasion more than T1sm1, positive resection margins (<1 mm), poorly differentiated adenocarcinomas, presence of lymphatic, venous, or perineural invasion, mucinous component, and tumor budding.4-6
All patients with local excision of a rectal neoplasia are followed up with a digital examination and endoscopy at 3, 6, and 12 months and when clinically indicated. Also strict controls with imaging test (ERUS, MRI, CT) in case of malignancies are recommended. Local recurrence was always confirmed by biopsy.
Statistics
Descriptive statistics were used for data analysis, with medians and means (± standard deviation) for normally distributed data, and number and percentage for continuous data.
Results
Beginning in 2012, 32 consecutive patients underwent a TAMIS procedure at our institution over a 40-month period. The mean age was 68.3 ± 12.9 year (range 42-92). Twenty-four were male (75%) and 8 were female (25%). Fifteen adenomas, 12 carcinomas, 1 gastrointestinal stromal tumor, and 1 neuroendocrine tumor were locally excised. Additionally, 3 pelvic abscesses were drained transanally using the TAMIS port. Rectal bleeding was the most frequent clinical presentation in case of rectal neoplasms. Mean distance from the anal verge was 5.6 ± 1.5 cm (range 4-10). Patients and tumor characteristics are detailed in Table 1.
Patients and Tumor Characteristics.
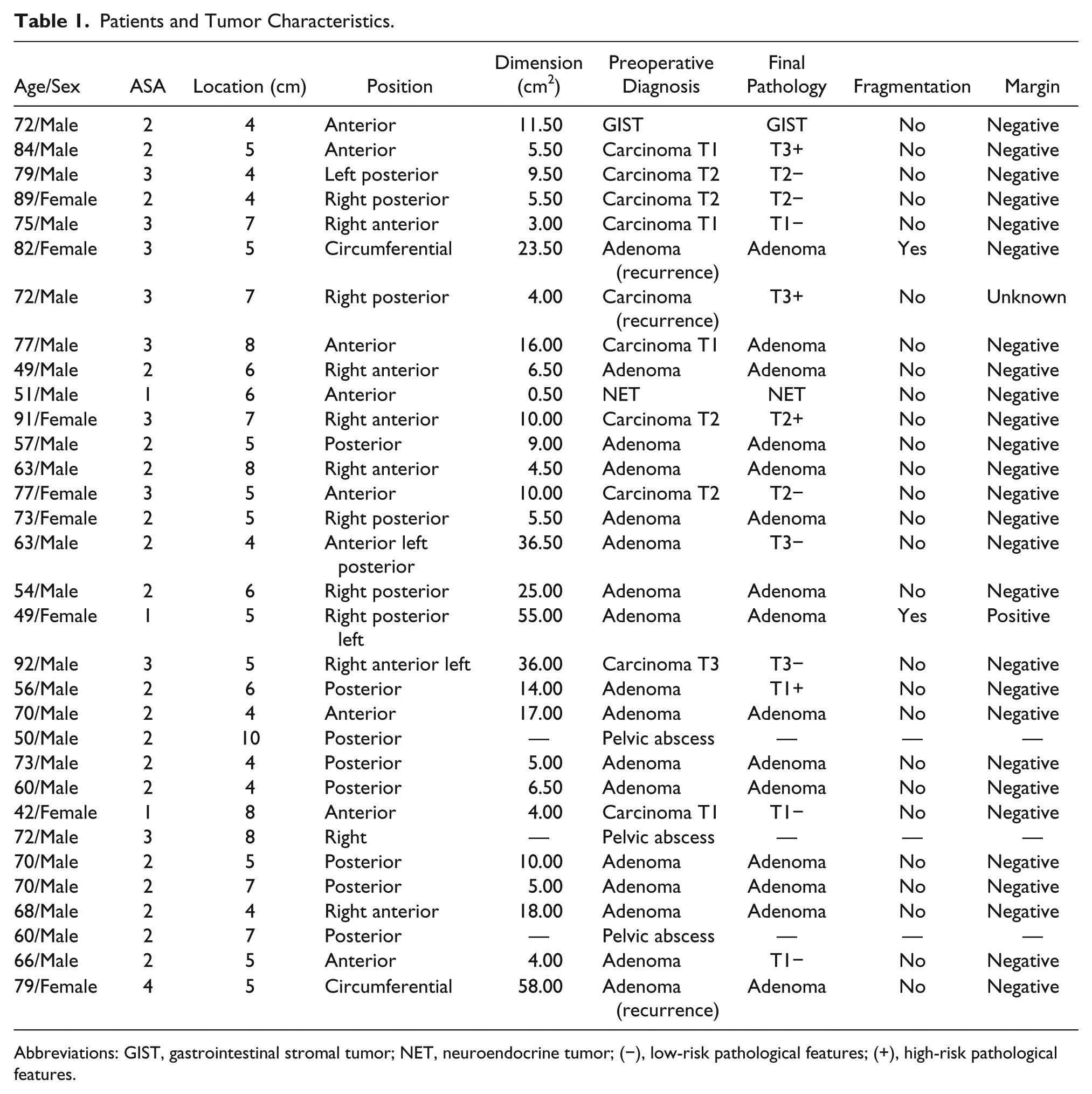
Abbreviations: GIST, gastrointestinal stromal tumor; NET, neuroendocrine tumor; (−), low-risk pathological features; (+), high-risk pathological features.
Morbidity
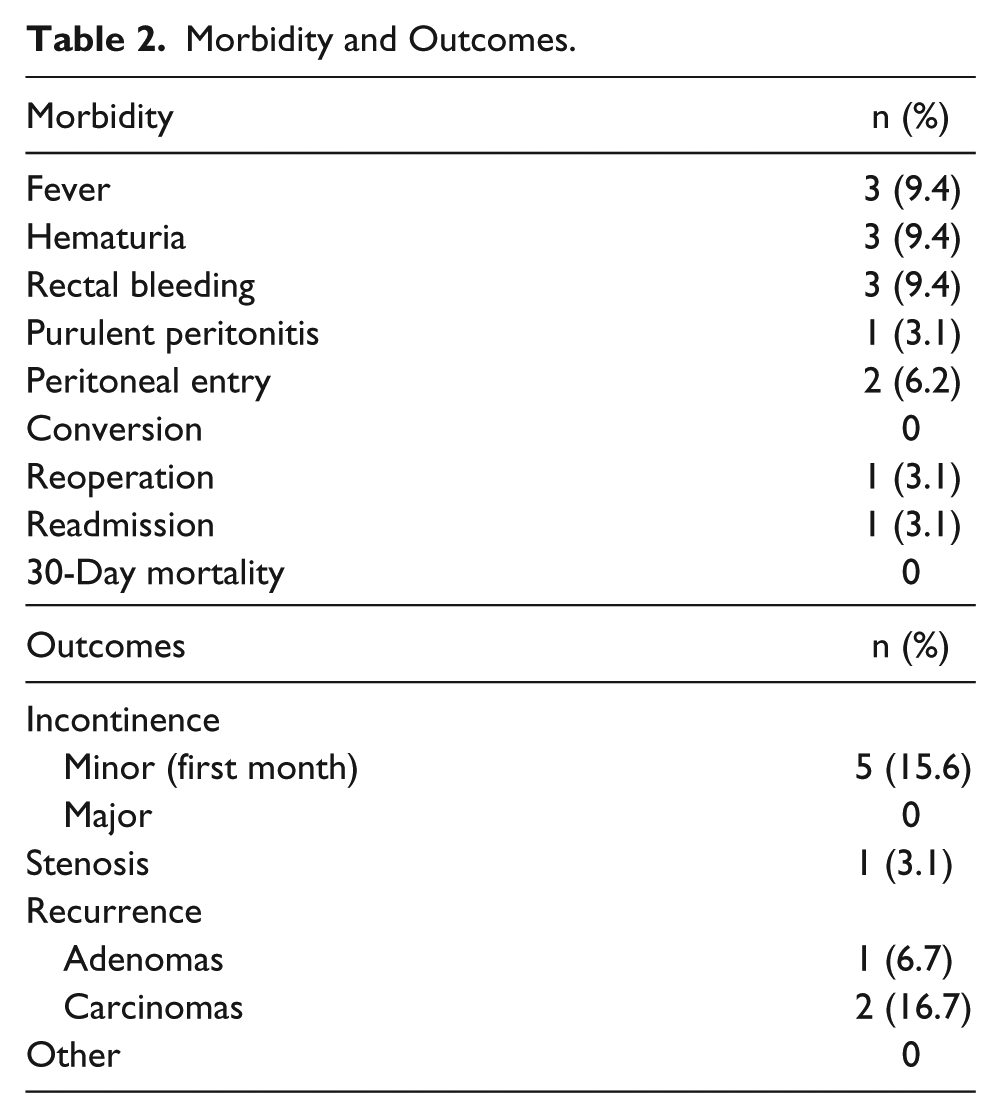
Mean operating time was 69 minutes (range 35-210). There were no major complications during the procedure and no conversions to open surgery. Two peritoneal entries were solved without need of laparotomy.
Early postoperative complications occurred in 22% of the cases, most of which were minor and managed with conservative measures. There was only one case of major complication (3.1%) requiring reoperation, and no postoperative mortality (Table 2). Mean postoperative hospital stay was 3.9 days (range 2-26).
Morbidity and Outcomes.
Pathological Examination
Four carcinomas were understaged (33.3%) and 1 adenoma overstaged (6.7%) preoperatively. Three carcinomas (2 T1 and 1 T3) were not suspected preoperatively (25%); the other case seemed to be a T1 initially and finally turned out to be a T3 cancer. Mean average tumor size was 14.5 ± 14.4 cm2 (range 0.5-58); 17.6 ± 4.4 cm2 in case of adenomas, and 11.8 ± 3.4 cm2 in case or carcinomas. All the surgical specimens were full-thickness resections with grossly negative margins. A microscopic positive lateral margin was found in one patient, and no deep affected margin was found. The fragmentation rate was 6.9%, 2 cases, both lesions over 20 cm2.
Outcomes
All patients were continent before surgery. Four weeks after surgery, 5 patients (15.6%) complained of minor episodes of fecal incontinence (for flatus or liquid stools), but after 8 weeks, these cases of incontinence were solved with no need of additional therapy. Neither urinary nor sexual functions were affected at any time. One patient, with a circumferential resection of a recurrent extensive flat adenoma (with several previous endoscopic resections), developed a rectal stenosis that required endoscopic dilatation. When pathological evaluation of the specimen revealed a tumor invasion beyond pT1sm1 or high-risk features, immediate radical surgery was always recommended, except for patients unfit for radical resection. Two patients underwent immediate salvage surgery and another 2 patients refused and were treated with adjuvant radiotherapy.
With a median follow-up of 26 months, the overall recurrence rate was 10.3%, 1 adenoma and 2 carcinomas. One recurrence was an 85-year-old man with a pT3 cancer who initially refused immediate salvage surgery and received adjuvant radiotherapy. The recurrence occurred 1 year later and he underwent radical surgery then. The other case was a pT2 cancer in a 75-year-old woman who received local excision due to her severe neurological disorder. The recurrence occurred 8 months later and she also underwent radical salvage surgery.
Discussion
Most experience with transanal endoscopic surgery derives from TEM and TEO platforms. A prospective randomized clinical trial showed no technical or clinical differences between the results obtained with the 2 systems except lower cost with TEO. 7 Moreover, there has been a steady increase in use of TAMIS over recent years. A variety of multichannel ports can be applied transanally for TAMIS procedures. 3 For some authors, the introduction of the TAMIS port into the anal canal is more complex than in TEM or TEO, 8 but we did not experience that drawback in our series. Since the inception of TAMIS, at least 390 procedures were reported worldwide from 2010 to 2013. 9 These pooled results further support the benefits of TAMIS for benign and malignant disease and may be used more widely in future. Success with robotic-TAMIS has also been demonstrated. 10 Regardless of the platform used, the basic principles of the procedure remain the same.
Appropriate patient and tumor selection is the main challenge, and preoperative staging is of paramount importance for decision making. Digital examination plays a key role. Tumor biopsy offers a low accuracy, with a histological discrepancy of up to 20% or even higher. 11 We must consider imaging studies as complementary staging modalities, and despite improvement in imaging techniques, there are patients who are not accurately staged. 12 As we have seen in our series, both adenomas and carcinomas can be under- or overstaged preoperatively. Even though ERUS appears to be the most accurate preoperative diagnostic tool for investigating tumor invasion, the rate of incidental carcinoma in lesions with benign appearance is significant. Serra-Aracil et al 13 found 52 out of 277 lesions (18.8%) with preoperative diagnosis of adenoma to be invasive carcinomas, a similar percentage to ours. Dash et al found that 13% of 167 benign lesions (with non–full-thickness excision) were unexpected cancers. This is not related to the type of lesion, although exophytic lesions may be harder to assess and classify by ERUS. 14 Some recent studies have investigated the role of ERUS, compared with MRI, for the staging of large rectal adenomas, reporting similar rates of overstaging; however, MRI might be more appropriate in case of proximal tumors that cannot be reached by the ERUS probe. 12 Due to the lack of accuracy in the preoperative staging, full-thickness resection with a macroscopic margin of 10 mm is recommended.
Whichever technique is used, morbidity and mortality are lower than for radical surgery. Operative mortality is less than 0.5%, and morbidity ranges from 4% to 30% in large series, depending on the inclusion of minor complications.15-20 Our data are in line with these percentages. The most frequent complications include acute urinary retention (0% to 11%), bleeding requiring reoperation (0.7% to 9%), peritoneal entry (6% to 20%), and recto-vaginal fistula (0.3% to 1.4%). 21 Regarding peritoneal perforation, although it was once thought to represent a complication requiring conversion to laparotomy or even a stoma, in experienced hands this can usually be avoided. 22 We have had 2 peritoneal entries with no need for conversion. A multicenter study performed from a database of 888 TEM procedures found 22 perforations into the peritoneal cavity, not resulting in any major short-term complications or adverse long-term oncological outcomes. 23
Transanal endoscopic surgery allows local excision to be performed with a higher rate of negative microscopic margins, reduced rate of specimen fragmentation, and reduced lesion recurrence compared to conventional transanal excision. 24 The reported rate of margin affectation in the surgical specimen using TAMIS procedures is 4.4%. 9 These figures are similar to ours and those obtained with TEM. Numerous studies have shown that the postoperative local recurrence rate following local excision for pT1 rectal cancer is in the range of 4% to 24%, whereas the local recurrence following radical surgery is in the range of 0% to 7%.25,26 These wide differences can be explained by the heterogeneity of cases, different selection criteria, risk characteristics, and surgical techniques. 11 The level of submucosal invasion (sm level) has shown to be a strong predictor of recurrence, with sm1 lesions having the lowest levels of local recurrence, and sm2-3 lesions with recurrence rates similar to T2 tumors. Five-year survival is consistently high in pT1, ranging between 80% and 100%, depending on the number of patients with high-risk tumours.5,11,25,27
When pathological evaluation of the specimen reveals tumor invasion beyond pT1 sm1 or high-risk features, immediate radical surgery is recommended. 28 The decision of local versus radical resection for T1 rectal cancer ultimately depends on the patient’s priorities. If the patient places a higher value on longer survival at any cost, available data suggest that they should opt for radical resection, whereas if the patient places a higher value on reducing complications, death following surgery or avoiding a stoma, they should opt for local resection. 29 We consider that local excision alone is not a suitable treatment for fit patients with pT2 or worse tumors, considering that the risk of local recurrence varies between 9.5% and 47%, but even in these cases there are considerable differences between low- and high-risk cancers. 3 Local excision might be offered to patients with high-risk T1 or T2-3 tumors with poor life expectancy and multiple comorbidities, unfit for major surgery, offering a reasonable chance of success, or simply as palliative treatment in case of disseminated disease. In this group, adjuvant radiotherapy could be an option for selected patients who decline completion surgery or are too frail for radical surgery. But even though radiotherapy appears to have some benefits added to local excision, it is still not as effective as radical surgery. 29
There are several studies that have shown similar oncological outcomes for T2 rectal cancers comparing neoadjuvant therapy and local excision versus radical resection, with good results in patients who had a significant response to chemoradiation.30,31 Currently, although neoadjuvant therapy may benefit some patients with early stage rectal cancer, indiscriminate use is not recommended in this population owing to the overtreatment of the majority. 32 The best candidates for transanal surgery following chemoradiation may be those with complete pathological response. Postoperative complications may be greater after neoadjuvant chemoradiation and may include pain, wound dehiscence, or even severe symptoms of local sepsis. 33
In case of recurrence after local excision, salvage resection offers disappointing oncological results, as this stage is usually more advanced than in primary tumors and may require multivisceral resection, an ostomy in many cases, and survival is seriously compromised. 34
Anorectal function after TEM has been addressed in several studies.35,36 The evidence available suggests that the TEM procedure seems to have no permanent deleterious effect on fecal continence. As shown in our series, short-term functional results of TAMIS are also excellent and comparable to functional results using the TEM equipment. 37 In many patients with preexistent impairment of anorectal function, their functional outcome after transanal endoscopic surgery is significantly improved, probably secondary to excision of a mucous producing lesion. Some patients may develop anorectal dysfunction, but this is usually associated with the excision of large lesions with changes in rectal capacity and compliance. Sexual or urinary disorders are very rare. When circumferential lesions are resected, particularly carpet adenomas, there can be a higher rate of rectal stenosis. We have had one of those cases. Stenosis will normally respond to surgical or endoscopic balloon dilatations, as in our patient.
As mentioned above, patients are followed-up with digital examination and endoscopy at 3, 6, and 12 months and when clinically indicated. Strict controls with imaging test (EUS, MRI, CT) in case of malignancies are also generally recommended. Maslekar et al reported that early endoscopic follow-up showed small areas of exuberant tissue in some patients, which proved to be granulation tissue following histological examination. 38 These same findings have been revealed in at least 3 of our patients with an excised adenoma. These findings have been recorded by other authors even a year after surgery, 39 and must not be interpreted as a local recurrence. Another interesting finding (in 6 patients) was the presence of a rectal pseudodiverticulum along the suture line; the tumor was located posteriorly (in 3 patients), and laterally (in the other 3 patients).
With an increase of the application of TAMIS and the experience of surgeons, the field for other possible uses has widened. There are many applications beyond local excision, the most important in recent years is the development of transanal total mesorectal excision. 40 We are beginning a surgical program at our institution for the clinical application of this technique.
Conclusions
Despite the limitations of the study, mainly the number of patients and short follow-up, TAMIS seems to be a safe and reproducible procedure for local excision of well-selected rectal lesions, with low morbidity and good functional outcomes. Quite a short learning curve is required for colorectal surgeons who have previous experience in laparoscopic and proctologic procedures. TAMIS provides a high-quality specimen with low fragmentation and a high rate of negative margins. It is also a valid platform for approaching rectal or perirectal diseases in a new way. Larger studies are needed to evaluate long-term functional and oncologic outcomes.
Footnotes
Acknowledgements
We thank Professor Mark D. J. Chappell for the general review of grammar and style.
Author Contributions
Study concept and design: Luis J. García-Flórez, Jorge L. Otero-Díez
Acquisition of data: Luis J. García-Flórez, Jorge L. Otero-Díez, Ana I. Encinas-Muñiz, Luis Sánchez-Domínguez
Analysis and interpretation: Luis J. García-Flórez, Jorge L. Otero-Díez, Ana I. Encinas-Muñiz, Luis Sánchez-Domínguez
Study supervision: Luis J. García-Flórez, Jorge L. Otero-Díez, Ana I. Encinas-Muñiz, Luis Sánchez-Domínguez
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.