
Abstract
Introduction
Peripheral nerves are frequently affected by traumatic lesions, as total or partial section, stretch, compression, avulsion, and crush cause the reduction or interruption of the nerve transmission, causing a reduction in the innerved area or loss of sensitivity and motility. 1 If not adequately treated, those lesions will result in significant deficits, disturbing patients’ quality of life or even limiting functional capacity to work and an increase of loss of working days.1,2
The gold standard treatment for peripheral nerve injuries is the neurorrhaphy.1-3 However, the lack of trained professionals and the high cost of the microscope limits the population to have this sort of assistance. 3 This deficiency is caused by the high cost of equipment necessary for microsurgical practices.3-5 Several alternatives are currently under development to avoid this situation and are showing promising results, such as endoscopes6,7 and laparoscopes.8,9 These devices have started a new era of video microsurgery; however, despite the high quality of their images, these devices have major limitations related to their short focal distance and high cost.
The quality of digital imaging in video cameras has significantly improved over the past decade, inspiring some researchers to try to use video systems as magnification.10-12 These systems have advantages such as low cost, elimination of the need to look into the microscope’s ocular lenses to see the operating field,10,11 and a more ergonomic design. 12 Conversely, the microscope adds to the stereoscopic effect through using binocular lenses.6-12
A literature review of the use of video systems for magnification has suggested that, so far, this novel magnification system has only been used to perform arterial anastomoses. One of the most important applications of microsurgery is the neurorrhaphy of peripheral nerves. The aim of this study, therefore, was to evaluate the use of a novel low-cost method of video-assisted magnification in the peripheral neurorrhaphy in rats.
Methods
Prior to its commencement, this study was approved by the Ethics Committee for the Use of Animals of the State University of Pará (UEPA). Twenty female Wistar rats (Rattus norvegicus) obtained from the Animal Colony of the Experimental Surgery Laboratory of UEPA were used. They weighed 200 to 250 g and were kept in a controlled environment with food and water ad libitum.
They were randomly assigned into 2 groups of 10 animals each: microscope group (MG), for which microsurgical procedures were performed under a DFVasconcelos microscope with 40× magnification; and video system group (VG), for which microsurgical procedures were performed under video system composed by a high-definition Sony camcorder DCR-SR42 set to 52× magnification, macro lenses, a LED high-definition 42-inch television, and a digital HDMI cable. Two low-intensity halogen light sources were used near the camera to provide adequate illumination of the operative field (Figure 1).

Video system composed of camcorder (1), HDMI cable (2), and full HD TV set (3).
The surgical procedures were performed by the same surgeon (RSMB) with over 20 years of experience in microsurgery, but without any experience in neurorrhaphy by video system magnification. All animals underwent the same surgical procedure, with the 2 groups differing only in the magnification technique used. The rats were anesthetized with ketamine (70 mg/kg) and xylazine (10 mg/kg) intraperitoneally and then shaved and placed in a horizontal supine position. Antisepsis was performed for all right hind legs. Under direct visualization, longitudinal incision took place in the anterolateral place of the right member, from the major trochanter toward the lateral condyle of the femur. There was the blunt dissection between the subcutaneous tissue to expose the femoral nerve in its full length and its branches.
A blue rubber shield was used for better visualization of the nerve. The femoral nerve was carefully dissected, and 7 mm distally to its emergence a double clamp was positioned and a neurotomy was performed at the midpoint of the double clamp. Then, clamps were approached and then sutured with interrupted sutures through the end-to-end technique using 10-0 nylon. Following the suture, the clamp was removed. The 2 groups differed only in the magnification technique used.
The procedure ended with the suture of muscles with 4-0 nylon and skin using 6-0 nylon. Saline solution (5 mL/kg intraperitoneally) was administered to balance eventual losses. The time spent on surgery was registered for both groups.
Four weeks after surgery, intraperitoneal injection of xylazine was used for euthanasia followed by dissection and harvesting the site of suture in the right femoral nerve for histologic examination. Nerve samples were fixed in 10% formaldehyde and buffered during 24 hours for subsequent dehydration in 70% alcohol until absolute alcohol, and then immersed in xilol. After that, it was held with 4-µm cuts on the microtome and stained with hematoxylin and eosin. There was computation of the number of axons in proximal and distal ends of suture site in the histologic study. Other relevant parameters were animals weight, femoral nerve diameter, surgery duration, and number of stitches.
BioEstat 5.4 software was used for analyses. Student’s i test was used to compare the weight, femoral nerve diameter, total surgery time, number of stitches, and number of axons between the groups. The number of axons of each stump on each group were compared using Mann-Whitney test. Pearson’s correlation test was used to evaluate the correlation between the time required for each neurorrhaphy and the order performed. We adopted a significance level of 5%.
Results
During the study there were no deaths or replacement of animals. There were no significant differences between the groups in the mean animals weight (MG: 202 ± 8 g vs VG: 204 ± 10 g; P = .40) or femoral nerve caliber (MG: 2.70 ± 0.48 mm vs VG: 2.50 ± 0.43 mm; P = .44). The correlation analysis between the animals’ weight and femoral nerve caliber showed no correlation (P = .67).
There were also no significant differences between the numbers of stitches (MG: 2.30 ± 0.48 vs VG: 2.20 ± 0.42; P = .71). The time required to complete each surgery was 24.70 ± 2.63 minutes in MG and 26.30 ± 2.70 minutes in VG. The difference between the groups was not statistically significant (P = .41). However, the time required to perform the neurorrhaphy was 3.20 ± 2.48 minutes in MG and 5.60 ± 2.81 minutes in VG, which was statistically significant (P < .01).
The number of axons are displayed in Table 1. There was no statistical difference between the groups; however, in both groups we found significant difference in the amount of axons comparing the proximal and distal ends of suture (P < .05).
Number of Axons Proximal and Distal of Suture According Each Group.
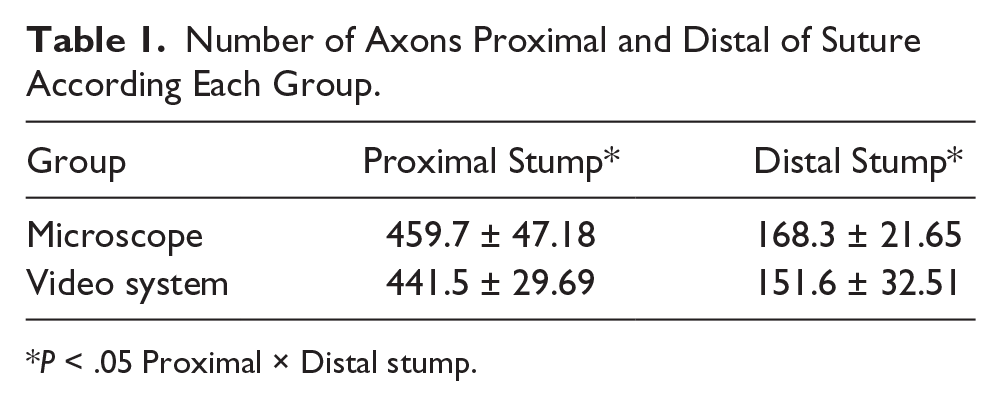
P < .05 Proximal × Distal stump.
For analyzing the learning curve acquired over the procedures in this research, we correlated the surgery duration and the animals order according to the procedures. We found reduction on time in the VG (Pearson’s ρ: −0.86; 95% confidence interval: −0.51 to −0.97. P < .01), but not in the MG (P > .05).
Discussion
Since Nylen first used an operating microscope in 1921, its basic design has remained fundamentally unchanged, 13 while the imaging and magnification of the video system has progressively been improving alongside diminishing cost and the rise of new technologies. In addition, the surgical video system provided enhanced body comfort (better ergonomy 14 ) and better deployment of the operating room personnel.6-12 And the autofocus function in the camcorder easily surpassed the microfocus in a surgical microscope.10-12
The main limitation of the video-assisted system is the lack of a stereoscopic view, although, as with laparoscopic surgery,6-8 the information on spatial depth can be derived from secondary spatial depth cues and from experience. 15 New technologies such as 3D cameras and 3D curve televisions will certainly remove this limitation.
There were no significant differences between the groups in the mean weight, caliber of nerves, or quantities of stitches when analyzed to confirm the pairing of the groups. Previous studies have used animals with similar characteristics as ours.10-12 No correlation with size and nerve caliber was found, indicating the femoral nerve as a good microsurgical training model.
The time required for the neurorrhaphy when using the video system was 1.75 times longer than that of the MG. Similar findings have been found with endoscopic and video systems when performing arterial anastomosis. We believe that the longer time may have been the result of the lack of stereoscopic view and the incipient learning curve.10-12
The negative correlation between the time taken for the surgical procedure and the order of the neurorrhaphy performed shows that there was a reduction in the time required and that there no difference in total surgical time, demonstrating at least the potential to be useful in initial microsurgery training or to practices at laboratories.
Adding to that, neurorrhaphy quality remained the same between groups since there was no difference between numbers of axons, which supports that the learning curve is not a big issue for video microsurgery. With better image quality, ergonomic design, and better teaching method, the video microsurgery learning curve is going to be less demanding and surgical excellence might be reached even faster.
Both groups show a reduction in number of axons comparing the proximal and distal stumps, although there was no significant difference between the groups, regardless of the time to perform the neurorrhaphy, showing a low effect of the video system magnification on neurorrhaphy wound healing.
The short follow-up was the major limiting factor for a better assessment of nerve function (motor and sensitive evaluation), as studies show that only from 8 weeks 16 there was a significant nerve recovery; thus, we decided for a shorter period (4 weeks) to determine accurately a possible influence on the axonal recovery. However, it is necessary for further studies to analyze more parameters to confirm this finding, such as electromyography and nerve functional index, which, in this initial study, were not carried out.
The cost of our proposed magnification system is likely to be less than US$2300. Nevertheless, our innovative setup showed similar results, for a peripheral neurorrhaphy, compared with microsurgeries under US$25 000 with a laboratory microscope. Thus, the video microsurgery is a feasible alternative for practicing complex and costly procedures at low cost, allowing it potentially to be included in trauma hospitals or in training/residency programs. 5
Of note, the video microsurgery is not completely ready for clinical application. The incipient learning curve seems to be the major limiting for now; however, it can be easily surpassed by training in experimental models. Yet our experience supports that video microsurgery is ideal for training of young microsurgeons. Images can be shared in real time for assessment with an experienced surgeon, allowing for correction of technical mistakes and suggested weaknesses, allowing an accurate individual evaluation. In addition, people are able to start training everywhere in the laboratory or even at home. Only equipment required are a monitor, ordinary camcorder, and HDMI cable.
Despite these encouraging results, we believe there will always be room for improvement in our model according to advances in imaging technologies before it is clinically applied.6,11 Refinements can be made in 2 ways: improving the surgeon’s skill with experimental video system magnification training and searching for an image system with higher resolution, including among 3-dimensional televisions and video cameras.10,11 While new technologies come out, the older ones become cheaper and video microsurgery becomes more reliable.
Conclusion
It is possible to perform a femoral neurorrhaphy in rats using a video system to provide magnification, with similar success rates compared to the traditional surgical microscope approach. However, this technique takes longer both in terms of the time taken to perform the neurorrhaphy.
Footnotes
Authors’ Note
The study described in this article followed the Brazilian law of use and care of animals (Law No. 11.794).
Author Contributions
Study concept and design: Rui Sergio Monteiro de Barros, Renan Kleber Costa Teixeira
Acquisition of data: Vitor Nagai Yamaki, Marcelo Ferreia Sabbá, Marcos Vinicius Vieira Lemos, Felipe Lobato da Silva Costa, Daniel Haber Feijó
Analysis and interpretation: Renan Kleber Costa Teixeira, Vitor Nagai Yamaki, Igor Costa Parente, Daniel Haber Feijó
Study supervision: Rui Sergio Monteiro de Barros, Marcus Vinicius Henriques Brito
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.