
Abstract
Introduction: Postoperative shoulder pain is a condition associated with laparoscopic surgery and presumably attributed to residual carbon dioxide (CO2) in the abdomen. The intent of the current prospective, observational study was to assess the efficacy of abdominal compression in mitigating this painful complication. Methods: We recruited 30 patients who were treated with laparoscopic surgery for the management of gynecologic disease. All study participants underwent abdominal compression to evacuate the CO2 associated with their pneumoperitoneum. Postoperatively, the subjects’ pain intensity was measured via the visual analogue scale at 12, 24, and 48 hours. Results: The patients’ mean postoperative visual analogue scale pain scores were the highest during the initial 12 hours (1.93), and thereafter, steadily declined at 24 hours (0.73) and 48 hours (0.70) (P = .045). Furthermore, toxicity was reasonable, with only 20% of subjects who reported grade ≤2 nausea and vomiting. Conclusion: Abdominal compression is a relatively safe procedure that appears to sufficently evacuate residual CO2, thereby reducing the severity of laparoscopic surgery induced shoulder pain.
Introduction
Minimally invasive surgery is frequently preferred to an open surgical approach for many indications, particularly when endeavoring to reduce intraoperative morbidity, attenuate postoperative pain levels, and hasten the resumption of a patient’s daily living activities.1,2 Despite the benefits conferred by endoscopic surgery, approximately 35% to 80% of patients are afflicted with postoperative shoulder pain.3,4 When a patient develops this condition, the soreness is theoretically quite profound, transcending the discomfort traditionally attributed to the incisional sites. 5
Shoulder pain is typically ephemeral and the malady potentially develops within 72 hours postoperatively, for which a hospital readmission is an anticipated outcome.6-8 The provenance of shoulder pain is ostensibly idiopathic. However, one theory speculates that the complication originates from residual carbon dioxide (CO2) that is confined between the liver and diaphragm in association with creating the pneumoperitoneum. 2 Thereafter, phrenic nerve irritation presumably eventuates referred pain to the C4 region5-9; local acidosis and diaphragmatic nerve injury have also been implicated in postoperative shoulder pain.5,10
Several operative techniques (eg, drainage via saline or Ringer’s lactate) addressing the evacuation of residual CO2 have been considered when striving to either avert or reduce postoperative shoulder pain. Nevertheless, many of the procedures have been unreliable and select maneuvers are associated with increased side effects (eg, nausea) or prolonged operative time.5,11,12 Hence, we elected to prospectively assess the effectiveness of abdominal compression, a traditional CO2 evacuation approach, to attenuate the severity of postoperative shoulder pain.
Methods
Eligibility Criteria
All gynecologic cancer subjects were >18 years of age and scheduled for a laparoscopic surgery to address their specific disease. Patients whose endoscopic procedure was converted to laparotomy were precluded from the study analysis. Study participants had to obtain an American Society of Anesthesiologists physical status classification I-II and be available for 48 hours of postoperative surveillance, especially patients for whom a same-day discharge was indicated.
Subjects who required intravenous narcotics for control of abdominal pain or were referred for an immediate postoperative hospital admission, were summarily excluded from the investigation. This evaluation received institutional review board approval and all participants signed a consent form prior to clinical trial enrollment.
Study Intervention
Preoperatively, the gas pressure was established at 15 mm Hg and the flow of gas did not exceed 2 L/min when creating the pneumoperitoneum.13,14 The intra-abdominal gas pressure and total volume of gas administered during the procedure were routinely monitored. The laparoscopic procedure was conducted using three 5-mm ports, 1 (camera) in the left, upper quadrant, and 2 (trocars) in the right abdomen. When the surgery was concluded, all blood and irrigant were maximally evacuated.
The surgical ports were, thereafter, opened via the valve or trocar cap and the operator performed abdominal compression, characterized by gentle pressure to the abdominal wall until the CO2 was satisfactorily evacuated through the ports. If an adverse event (eg, nausea or emesis) was identified, the condition was graded and documented in accordance with the Common Toxicity Criteria for Adverse Events, Version 4.03. 15
Study Variables
The patients’ charts were systematically evaluated to ascertain baseline characteristics, including age, body mass index (BMI), surgical indication, operative time, and hospital duration. The primary efficacy endpoint, manifestation of postoperative shoulder pain, was assessed at 3 distinct time periods (12 hours, 24 hours, and 48 hours), via the visual analogue scale (VAS); 16 upon completion, the VAS forms were ultimately submitted to the research coordinators for review.
Statistical Analyses
All statistical analyses were conducted using MedCalc statistical software for biomedical research (version 9.5.1 for Windows). The initial data analysis was conducted via descriptive statistics; additional evaluation incorporated analysis of variance and multiple regression. In determining significance, 2-tailed hypotheses with a P value <.05 were utilized to assess any identified relationships amongst the relevant clinic-pathologic parameters.
Results
From March 2015 until August 2015, we consecutively identified 32 gynecologic patients who underwent endoscopic surgery and abdominal compression to evacuate the CO2 in the prevention of postoperative shoulder pain. There were 2 subjects who were ultimately precluded from study participation because of either a surgery cancellation or pronounced, chest intraoperative compression that was performed by the treating physician.
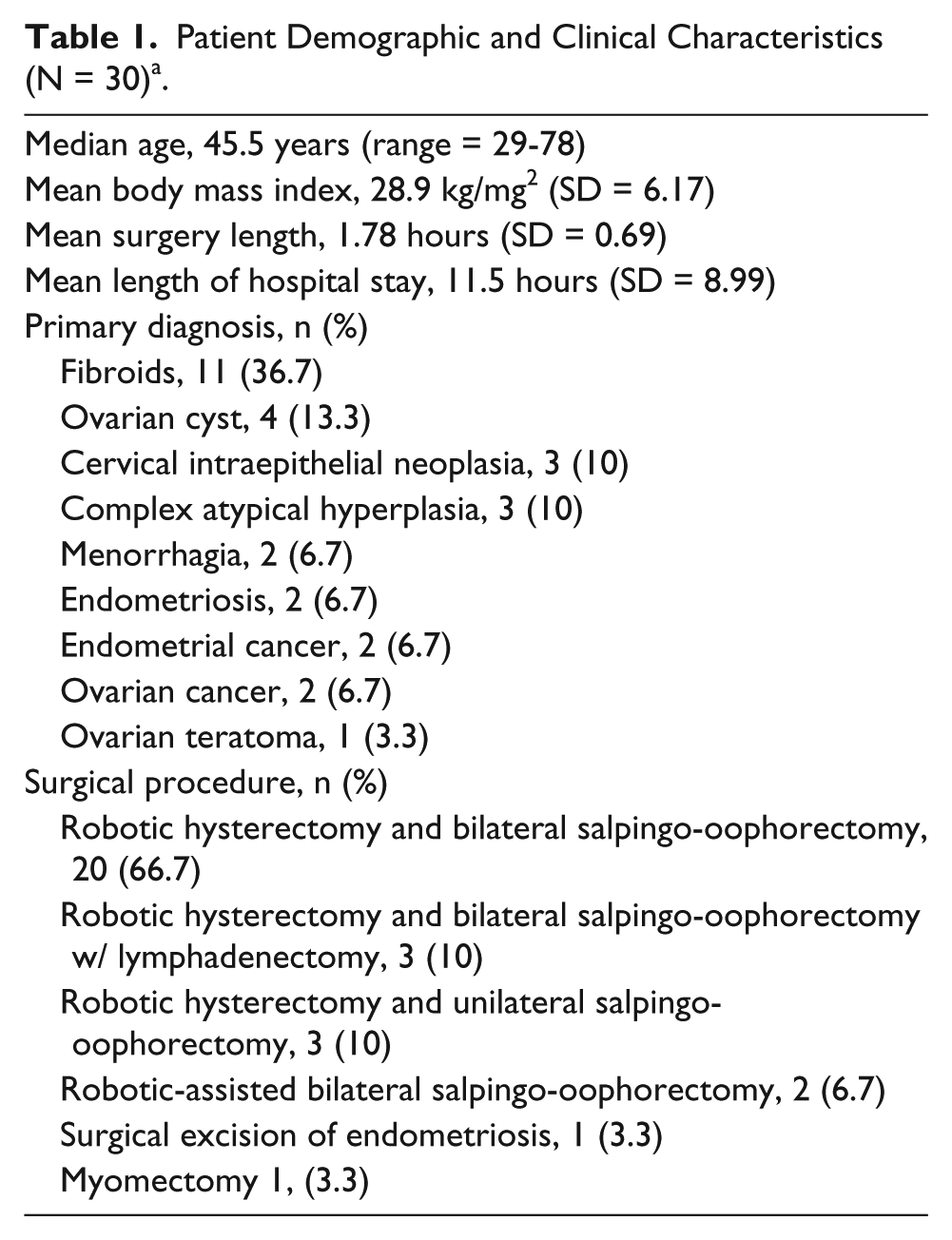
The mean age of the 30 study participants was 48.5 years (standard deviation [SD] = 11.49) and BMI was 28.9 kg/mg2 (SD = 6.17). The patients were treated with minimally invasive surgery for a variety of conditions, including uterine fibroids (36.7%), ovarian cyst (13.3%), and cervical intraepithelial neoplasia (10%). The subjects’ mean surgery time was 1.78 hours (SD = 0.69, 95% confidence interval = 1.51-2.05) and hospital duration was 11.5 hours (SD = 8.99; 95% confidence interval = 8.02-14.9); see Table 1 for the trial participants’ demographic and clinical characteristics.
Patient Demographic and Clinical Characteristics (N = 30)a.
The patients’ mean VAS score was 1.93 (SD = 2.98) at 12 hours; in contrast, the mean VAS score at 24 hours and 48 hours was 0.73 (SD = 1.26) and 0.70 (SD = 1.82), respectively (see Figure 1). There were significant differences between the VAS scores at 12 hours and 24 hours and at 12 hours and 48 hours (P = .045); the patients reported a significantly higher pain score within the first 12 hours (ie, the pain levels culminated) relative to the 24- and 48-hour intervals; however, there were no pain score differences between the 24- and 48-hour time periods (P > .05). Correspondingly, at 12 hours, 36.7% of the subjects reported postoperative shoulder pain; after 24 hours and 48 hours, only 33.3% and 16.7% of patients, respectively, indicated that they suffered from postoperative shoulder pain.
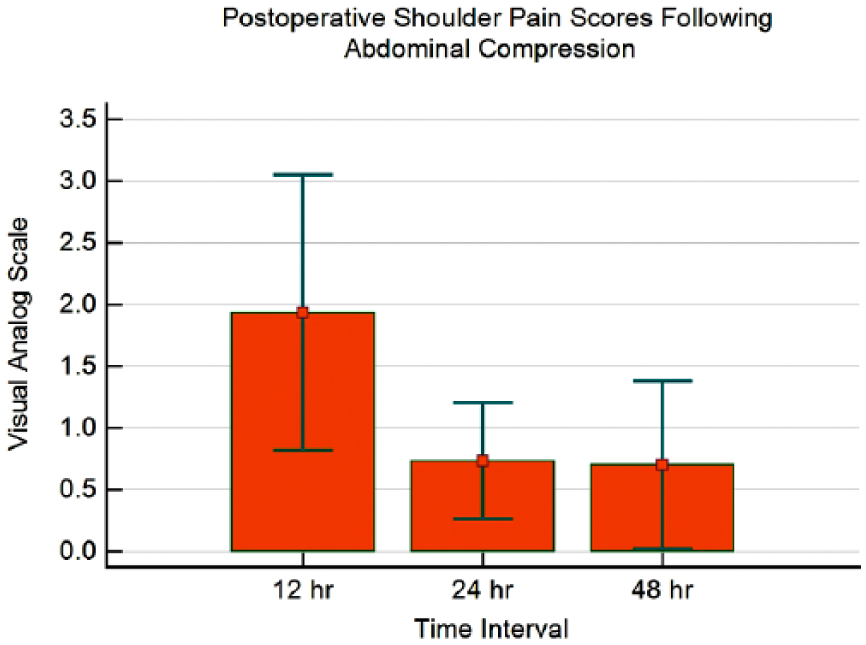
The patients’ mean visual analogue scale pain scores at 12 hours, 24 hours, and 48 hours.
In regard to toxicity, 6 patients (20%) developed postoperative grade ≤2 nausea and vomiting. There were also 21 study participants who experienced abdominal pain that were treated with either ibuprofen (n = 10) or acetaminophen (n = 11). We attempted to discern if the use of pain medication affected the subjects’ pain scores during the prescribed intervals but medicinal intervention was not a significant correlate (P = .625).
A subsequent regression analysis that incorporated age, BMI, pain scores at the identified time intervals, use of pain medication, and operative time on hospital duration revealed that only operative time was a surrogate marker (R2 = 0.2914) for increased length of hospital stay (Beta = 2.262; P = .03); the patients who had a prolonged surgery endured a lengthier hospital stay.
Discussion
Minimally invasive surgery is extensively used to manage a variety of indications and the prevailing trend continues to supersede the open surgical approach.1,2 Nevertheless, endoscopic surgery is associated with some complications, namely, the development of postoperative shoulder pain.3,4 The condition, albeit transient, can be associated with severe pain that necessitates analgesics and prolonged repose.
When attempting to avert or mitigate the risk for postoperative shoulder pain, facilitating the evacuation of CO2 from the abdominal cavity is indispensable. 2 Select investigations have reported that forced evacuation of CO2 via aspiration cannula alone or suction with manual compression dramatically attenuates shoulder pain intensity.17,18 Alternatively, in the pulmonary recruitment maneuver, the residual CO2 is mechanically removed via positive-pressure ventilation. 2 The infusion of intraperitoneal normal saline, which presumably diminishes the CO2 through the manifestation of a physiologic buffer, and bupivacaine with saline infusion, have also been utilized in an attempt to stave off postoperative shoulder pain.5,11 While many of these techniques have accorded a clinical benefit, they potentially require additional operative time, elevate the risk for side effects, and necessitate increased postoperative surveillance.5,19,20
We employed abdominal compression, a traditional method for the evacuation of CO2, essentially because the procedure neither incorporates additional resources nor prolongs operative time. In the study population, we observed that the patients’ mean VAS scores pinnacled throughout the initial postoperative 12 hours, whereupon they declined significantly during the 24- and 48-hour time intervals. We identified one subject who reported a VAS score of 10 during the initial 12 hours because she was unwilling to recline during the day (which may have contributed to the elevated shoulder pain score) although her pain dramatically subsided (to a VAS score of 3) within 24 hours. Moreover, we recognize that while pain medication was not a surrogate factor for the development of shoulder pain, the medication type and frequency of administration among the study population were not uniform, which potentially confounded the results. Conversely, instead of assessing the potential impact of pain medication, we may have considered if this variable was simply a reflection of postoperative pain, irrespective of the patients’ VAS score.
In the Phelps et al study for the prevention of laparoscopic induced shoulder pain, they similarly indicated a decrease in shoulder pain following the initial 12 hours with their gynecologic patients who underwent either passive exsufflation or the pulmonary recruitment maneuver. 5 Also, Suginami et al 12 documented their experience with gynecologic patients who were managed with either abdominal compression or saline interspersed throughout the abdomen to mitigate the development of postoperative shoulder pain; likewise, they recounted that the subjects’ pain levels culminated at 12 hours and then declined, thereafter.
In the current study, we did not encounter any pulmonary complications and the patients’ incidence (20%) of nausea and vomiting was reasonably low. Conversely, in the Phelps et al study, 57% of their study participants who underwent passive exsufflation endured nausea and vomiting. 5 We also recognize that the postoperative nausea is theoretically unrelated to passive exsufflation and, instead, may be attributed to differences in anesthesia or postoperative pain medication. However, since our follow-up duration was only 48 hours, the subjects’ overall nausea and vomiting may have further deteriorated.6,8
Conclusion
We describe our favorable experience with abdominal compression, a reasonably uncomplicated maneuver to attenuate the severity of laparoscopic surgery induced shoulder pain. Our results suggest that abdominal compression does not appear to prolong operative time, increase length of hospital stay, or adversely impact the risk for side effects. Contrariwise, we discerned that only increased operative time was a surrogate marker for protracted hospital stay. Ultimately, however, this may be considered subjective because our study did not compare patients with and without abdominal decompression.
The present study is not without limitations; in the absence of a control group or randomization, one cannot draw conclusions as to whether or not diligent CO2 evacuation actually benefited these patients; therefore, one could assert that our pain scores reflect the surgery and elapsed time, and not the specific intervention. Response bias associated with self-report measures and limited surveillance should also be considered within the context of our findings, most notably because more than a third of subjects persistently complained of shoulder pain.
We also excluded participants who required hospital admission or narcotics for pain control, which ostensibly limited the subject population to patients who experienced minimal pain. Patients with shoulder pain or other symptoms of pneumoperitoneum often require narcotics although one may conjecture that these subjects may not have accurately depicted their pain levels during the completion of the VAS. Additionally, while there was presumably limited intragroup pain variation because the number and size of the ports were standard among the patients, 21 the authors acknowledge any discrepancy could affect the scoring evaluation. In particular, the study results would have been strengthened had we accounted for incision number, port size and location.
Since we initially explained to the study participants that manifestation of shoulder pain was our primary concern, we also appreciate that incisional pain may have been de-emphasized, even if both factors were incorporated in the VAS reporting. Unfortunately, shoulder pain may be nonspecific 12 and beyond the patients’ self-reporting data, we cannot conclusively determine if the shoulder pain resolved itself during the scheduled postoperative intervals. Hence, the findings would have presumably benefited from specifically distinguishing between localized shoulder pain and abdominal or overall pain, thereby implicating the referred diaphragmatic pain component.
One may further speculate that the technique wherein we measured the effectiveness of abdominal compression in eliminating CO2 (eg, intensity and time of compression) was subjective. In particular, the manner in which we determined if CO2 was satisfactorily evacuated was imprecise. We, nevertheless, contend that due to the facility of abdominal compression, the procedure can be safely and conveniently incorporated into routine clinical management. A larger, randomized, controlled, prospective study comparing the impact of abdominal compression and a control group (eg, physician discretion) in the prevention of postoperative shoulder pain is warranted.
Footnotes
Author Contributions
Study concept and design: Bram H. Goldstein, Mark A. Rettenmaier, John P. Micha
Acquisition of data: Amber M. Wilcox, Katrina L. Lopez
Analysis and interpretation: Bram H. Goldstein, Mark A. Rettenmaier, Katrina L. Lopez, Amber M. Wilcox
Study supervision: John P. Micha, Mark A. Rettenmaier
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Women’s Cancer Research Foundation.