
Abstract
As per-oral endoscopic myotomy (POEM) is not followed by any anti-reflux procedure, a common concern is the risk of postoperative gastro-esophageal reflux disease (GERD). Electrical stimulation of the lower esophageal sphincter (LES-EST) could be an option for post-POEM GERD. A 68-year old male obese patient underwent successful POEM but developed GERD not responsive to proton pump inhibitors. Consecutively, the patient had implanted an electrical LES stimulation device, consisting of bipolar LES-electrodes connected to a subcutaneous pulse generator. POEM reduced the Eckardt score (9 vs. 0), the LES resting pressure (52.0 vs. 16.4 mmHg), and the Integrated Relaxation Pressure (62.0 vs. 10.0 mmHg). LES-EST substantially reduced post-POEM GERD symptoms. GERD-HRQL scores indicated the elimination of heartburn (26 vs. 7) and regurgitation (24 vs. 3) at three months. A reduced total number refluxes (82 vs. 14) was observed. The %-time of pH below 4 was only slightly reduced (8.6% to 6.2%).LES-EST appears to be a feasible option to symptomatically treat post-POEM GERD for patients not ideal for conventional anti-reflux surgery.
Introduction
Per oral endoscopic myotomy (POEM) has become a globally utilized appealing option to treat achalasia.1,2 Since POEM is not followed by an antireflux procedure, a common concern is postoperative gastroesophageal reflux disease (GERD).3,4
Lower esophageal sphincter electrical stimulation (LES-EST), using leads implanted at the lower esophageal sphincter (LES), has been described to improve GERD symptoms and reducing esophageal acid exposure, while enhancing the LES tone without impairing relaxation. 5
As it is known that conventional fundoplication is less effective in obese patients, 6 we hypothesized that LES-EST would be an option for a patient requiring treatment for GERD after POEM. Additionally, LES-EST would potentially not interfere with later fundoplication if needed. To the authors’ best knowledge this is the first clinical report on LES-EST for post-POEM GERD.
Case Report
A 68-year-old male patient, body mass index of 35.3 kg/m2, had been diagnosed with Chicago Classification type II achalasia by high-resolution manometry (HRM), which revealed a lower esophageal sphincter pressure (LESP) of 52 mm Hg and an integrated relaxation pressure (IRP) of 64 mm Hg. Initial endoscopy diagnosed a hiatal hernia (HH) and signs of GERD. Barrett’s esophagus (BE) together with epithelial changes indefinite for dysplasia (IFD) was found. After an 8-week course of double-dose proton pump inhibitors (PPIs), re-biopsies still revealed IFD and led to another period on double-dose PPI. Two consecutive re-biopsies diagnosed GERD-associated epithelial changes but no BE.
The patient underwent POEM in May 2015 according to a standardized protocol. Briefly, POEM was performed under general anesthesia. After entry into the submucosa and distal tunneling, a 10-cm myotomy, extending 3 cm into the cardia, was performed. Mucosotomy was closed with 6 endoscopic clips. He was discharged on the second postoperative day and again put on double-dose PPI for 8 weeks. POEM was evaluated during follow-up visits after 1, 6, and 12 months, including timed-barium swallow (TBS), upper gastrointestinal endoscopy, manometry, and pH-impedance monitoring, as well as an achalasia symptom score (Eckardt score).
Due to GERD not responsive to PPI the patient had an electrical LES stimulation device implanted in December 2016 under general anesthesia. The LES-EST system (EndoStim Inc, St. Louis, MO) consists of bipolar electrodes, which are laparoscopically implanted about 1 cm apart from each other at the gastroesophageal junction (Figure 1), connected to an implantable, typical titanium case construction, pulse generator. The generator is implanted into a subcutaneous pocket in the left upper quadrant of the abdominal wall. An external programmer is used for interrogation and programming of the implanted generator. Electrical stimulation was executed with a regimen of 215 µs (5 mA amplitude), at 20 Hz in 30-minutes sessions (12 per day) with alternative polarity.
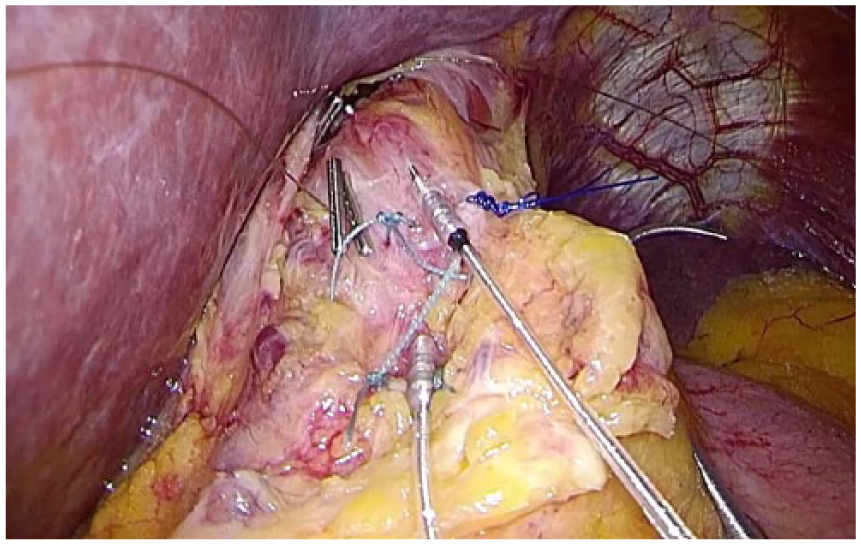
Electrodes implanted at the lower esophageal sphincter.
Three months postoperatively, the effect of LES-EST was measured by the validated GERD–health-related quality of life questionnaire (GERD-HRQL), providing a composite score based on severity and frequency of symptoms, and was compared with the baseline results obtained prior to the implantation. HRM and pH-impedance monitoring was used to evaluate LESP, IRP, and the % of time the pH at the distal esophagus was under 4.0 together with the number of refluxes per 24 hours.
During the overall 24-week course of PPI treatment for IFD changes, the patient finally presented with a preoperative Eckardt score of 9, with daily dysphagia, daily regurgitation, and weight loss of 12 kg but no retrosternal pain. Preoperative TBS (150 mL barium) demonstrated a column height of 27, 25, and 16 cm at 1, 2, and 5 minutes, respectively. Esophageal width was 4 cm.
POEM was performed without adverse events and took 125 minutes. One month postoperatively, the patient was without achalasia related symptoms (Eckardt score 0). TBS found contrast agent to be cleared at 1 minute, indicating a sufficient myotomy. After 6 months manometry revealed an LESP of 16.4 mm Hg and an IRP of 10.0 mm Hg. However, pH-impedance monitoring observed a total pH < 4 of 8.6% (recumbent 15.8%, upright 1.2%), 82 refluxes, and a positive DeMeester score (62.5). The patient was put on standard-dose PPI.
Endoscopy at the 12-month follow-up again diagnosed short-segment BE (Prague classification: C1M2). Within the next 6 months reflux symptoms became non-PPI responsive, and the patient required additional therapy for his post-POEM GERD.
The implantation of the LES-EST device took 65 minutes. Despite a subcutaneous hematoma, the postoperative course was uneventful. At the first postoperative day the patient subjectively reported less GERD symptoms. He was discharged on the fourth postoperative day.
At the 3-month follow-up, 2 weeks off PPI, the GERD-HRQL questionnaire revealed a total subjective score of 10 compared with 50 (greatest possible score 75) prior to initial LES-EST.
Postoperative heartburn score was 7 (preoperative score 26, greatest possible score 30), indicating heartburn elimination. Postoperative regurgitation score was 3 (preoperative score 24), also indicating regurgitation elimination (score ≤12 with each individual question not exceeding 2). The patient was “satisfied” with his present condition compared with a “dissatisfied” condition prior to LES-EST.
The patient had less refluxes (total 14, upright 9, and recumbent 5) and percentage of pH < 4 was 6.2% (recumbent 14.5%, upright 1.8%). DeMeester score was reduced to 29.1. LESP and IRP again were 16.4 mm Hg and 10 mm Hg. Results are summarized in Table 1.
Comparison of HRM Data, TBS, Eckardt Scores as Well as GERD-HRQL Score and pH-Impedance Monitoring Before POEM and Before as Well as After LES-EST.
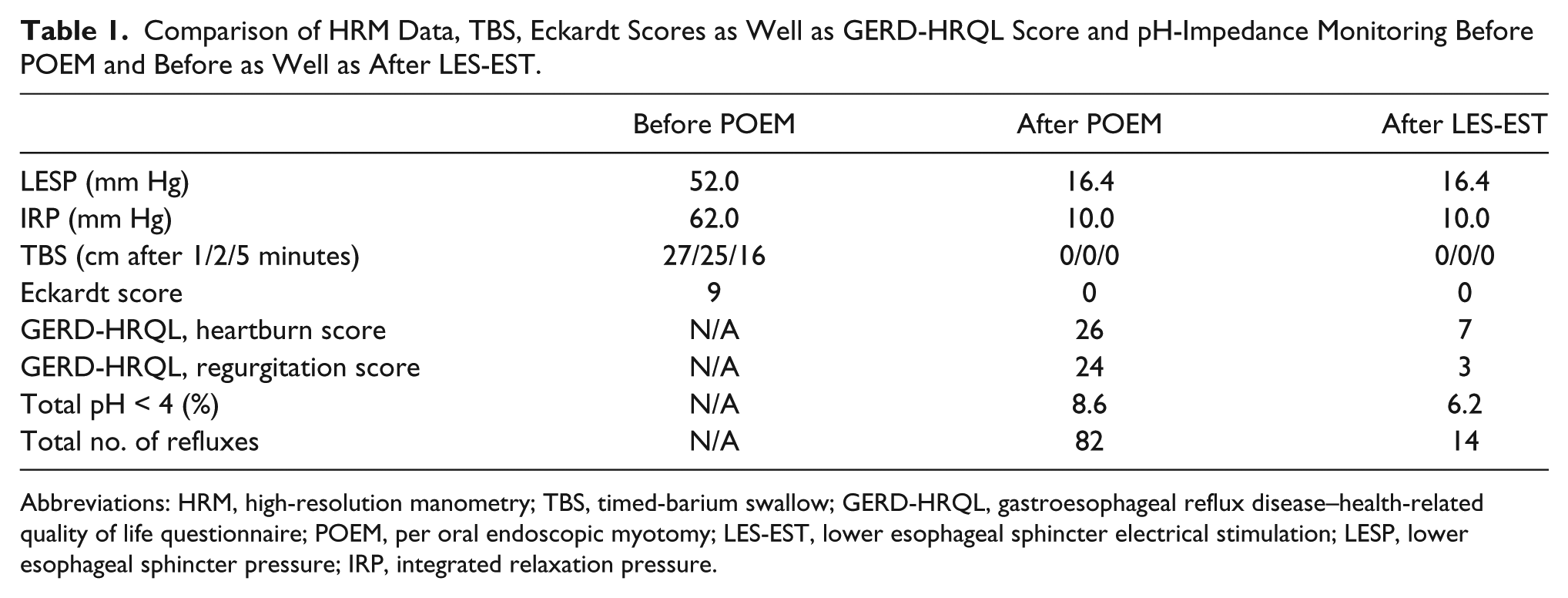
Abbreviations: HRM, high-resolution manometry; TBS, timed-barium swallow; GERD-HRQL, gastroesophageal reflux disease–health-related quality of life questionnaire; POEM, per oral endoscopic myotomy; LES-EST, lower esophageal sphincter electrical stimulation; LESP, lower esophageal sphincter pressure; IRP, integrated relaxation pressure.
Discussion
We report the first clinical use of electrical LES stimulation to treat post-POEM GERD not responsive to PPI. Three months after initial electrical stimulation the elimination of heartburn and regurgitation as well as a reduced number of refluxes was observed.
LES-EST has been recently proposed as alternative treatment for GERD, with controlled releases of electrical stimuli supposed to improve sphincter function. 5 However, data on LES-EST mainly refer to a very restricted cohort of GERD patients, excluding patients with BE or significant HH together with body mass index restrictions. Interestingly, although our patient was obese with a HH, the observed improvements of post-POEM GERD symptoms are in line with the almost universal success in the symptom elimination in highly selected LES-EST cohorts. Also, the reduced number of refluxes as well as initially only small improvement in pH exposure was found to be similar to GERD patients treated by LES-EST. 7
The appealing use of electrical stimulation after POEM has been recently described in an animal model. 8 A significantly re-increased LESP with LES-EST after POEM was observed. However, it was unclear how electrical stimulation would affect impaired muscle tissue such as in achalasia. Additionally, healthy animal data are not easily transferable to the clinical situation. Interestingly, we did not find any increase in LESP after 3 months of clinical LES-EST.
It had been hypothesized that GERD would not become an issue after POEM, as it was supposed to leave the physiological antireflux mechanisms untouched. However, a recently published study reported altered esophageal acid exposure in over 50% of patients, but less than half of it being symptomatic.3,4 However, dividing the circular fibers near the lesser curvature should not simultaneously destroy the whole antireflux mechanism. One could easily hypothesize that the oblique sling fibers, eventually emerging from a loop of circular clasp fibers, would provide some antireflux mechanism. 9 A mechanism that could be affected and trained by the generated electrical field of LES-EST.
Until today, reports of antireflux procedures for post-POEM GERD are very rare, but more patients might need a post-POEM antireflux intervention in the near future. Recently the use of transoral incisionless endoscopic fundoplication for severe post-POEM GERD has been reported. An improved total GERD-HRQL score (43 to 25) while being on PPI 10 was observed. Interestingly, in our patient LES-EST led to a lower score while being off PPI. For the rare morbidly obese achalasia patient, Roux-en-Y gastric bypass in conjunction with POEM could also be an effective, but rather invasive, antireflux treatment option.11,12
In retrospect, with obvious reflux disease and BE, laparoscopic myotomy together with an antireflux procedure would eventually have been the better choice for this achalasia patient and further studies investigating this question appear mandatory. Nevertheless, if needed, LES-EST could also be an option to treat GERD symptoms after POEM.
Footnotes
Author Contributions
Study concept and design: Erwin Rieder, Matthias Paireder, Ivan Kristo, Sebastian F. Schoppmann
Acquisition of data: Erwin Rieder, Matthias Paireder, Ivan Kristo, Katrin Schwameis, Sebastian F. Schoppmann
Analysis and interpretation: Erwin Rieder, Matthias Paireder, Ivan Kristo, Katrin Schwameis, Sebastian F. Schoppmann
Study supervision: Erwin Rieder, Sebastian F. Schoppmann
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.