
Abstract
Background. Transoral endoscopic thyroidectomy vestibular approach (TOETVA) has evolved from a novel procedure to a cosmetically appealing alternative to the traditional open thyroidectomy. TOETVA is limited to only high-volume centers with the hope to expand and demonstrate the safety, reproducibility, and application for the correct patient with thyroid disease. We present our experience with the first 50 TOETVA procedures performed at our institution. Methods. From September 2016 to June 2018, we performed 50 transoral endoscopic thyroidectomies via the vestibular approach for a variety of thyroid pathologies. Outcomes were analyzed from a prospectively maintained database. Patients were treated for a different range of thyroid pathologies. Results. A total of 12 (24%) patients underwent total thyroidectomy, whereas 38 (76%) patients underwent a subtotal thyroidectomy or thyroid lobectomy. The mean surgical time was 149 ± 40.0 (90-256) minutes for lobectomy and 217.6 ± 33.3 (175-276) minutes for total thyroidectomy. Of our 50 patients, 16 (32%) had postoperative transient lower lip numbness with an average time to recovery of 23.8 (.43-48) weeks, with 1 (2%) patient having persistent, but improving, lower lip numbness beyond the 6-month follow-up. There were 13 (26%) patients with transient chin numbness with an average time to recovery of 15.7 (2-48) weeks. Two (4%) patients had transient recurrent laryngeal nerve (RLN) injury with hoarseness, whereas 1 (2%) patient had permanent injury. Conclusion. The TOETVA is a safe and reproducible procedure. For selected patients, this technique is a viable alternative to conventional thyroidectomy.
Keywords
Background
Transoral endoscopic thyroidectomy vestibular approach (TOETVA) has evolved from a novel procedure to a cosmetically appealing alternative to traditional thyroidectomy. Natural orifice transluminal endoscopic surgery (NOTES) was adopted for thyroid surgery as a way to avoid scarring in the neck.1,2 Scarring and potential disfigurement in this highly exposed area could be especially distressing to some patients with darker skin pigmentation or with a history of hypertrophic and/or keloid scars.3,4 Categorization as NOTES can be misleading, as TOETVA entails creating a subplatysmal dissection plane after initial incisions in the oral cavity.5,6 Therefore, TOETVA could more aptly be categorized as a remote access surgical technique with hidden scars and optimal visualization of the thyroid gland.3,4,7
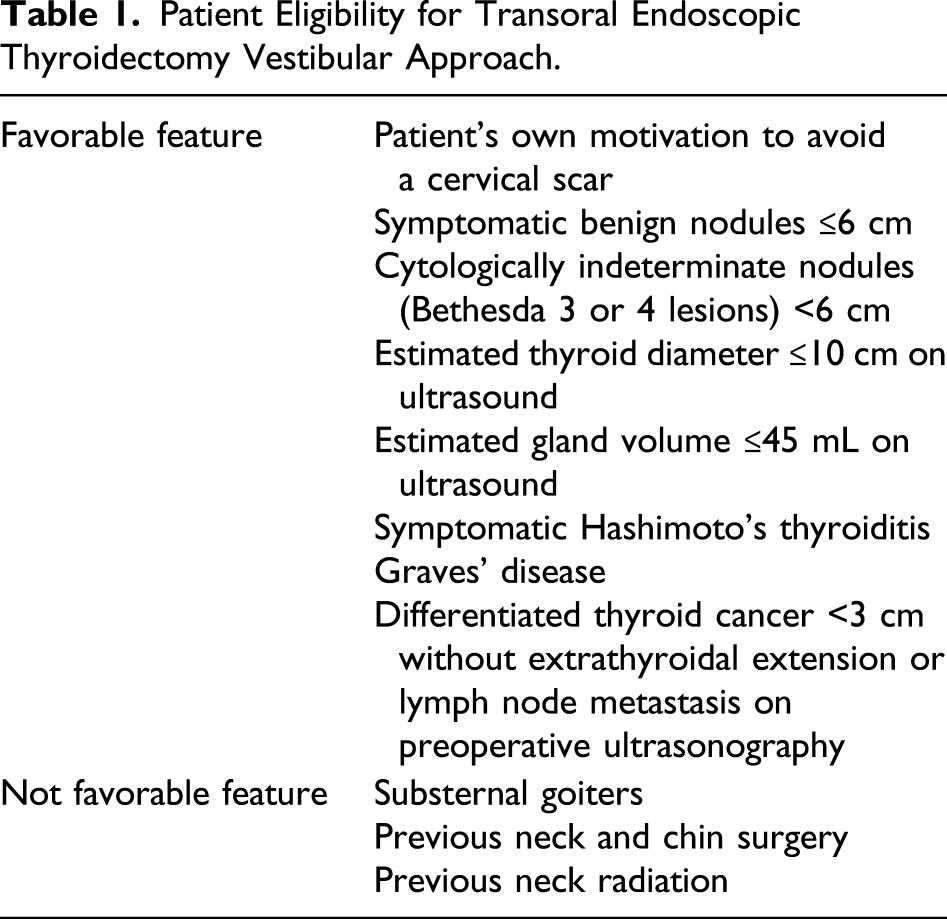
To this point, there have been over 1200 TOETVA procedures performed worldwide.8-10 Safety profile has been found to be comparable to the gold standard technique (traditional transcervical thyroidectomy). 8 This technique has been applied to various types of thyroidectomies: total thyroidectomies, lobectomies, subtotal thyroidectomies (eg Hartley-Dunhill procedure), and total thyroidectomies with central lymph node dissection.1,6,11 The variety of thyroid pathologies this approach has been used for has ranged from discreet nodules and diffusely enlarged thyroid glands due to Graves’ disease to patients with low-risk well-differentiated thyroid cancer. Despite its wide applicability, it is important to be clear that not every patient or any thyroid gland is amenable to the transoral approach. There are specific features and thyroid gland characteristics that have been deemed favorable or nonfavorable for this procedure. Therefore, while underlying thyroid disease does have a part to play in whether or not the TOETVA procedure can be used, it is the patient and thyroid characteristics that truly determine feasibility.
This procedure is currently being performed nationally and internationally, but its use, thus far, has been limited to only a limited number of centers. Another limitation to its widespread applicability has been the steep learning curve, even among surgeons having expertise in traditional thyroidectomies and endoscopic procedures. 4 This could be overcome with increased volume. 9 The purpose of this article was to present our experience with the first 50 TOETVA procedures performed at our institution.
Methods
Patient Selection
Patient Eligibility for Transoral Endoscopic Thyroidectomy Vestibular Approach.
Demographics and Patient Population
Patient Demographics.
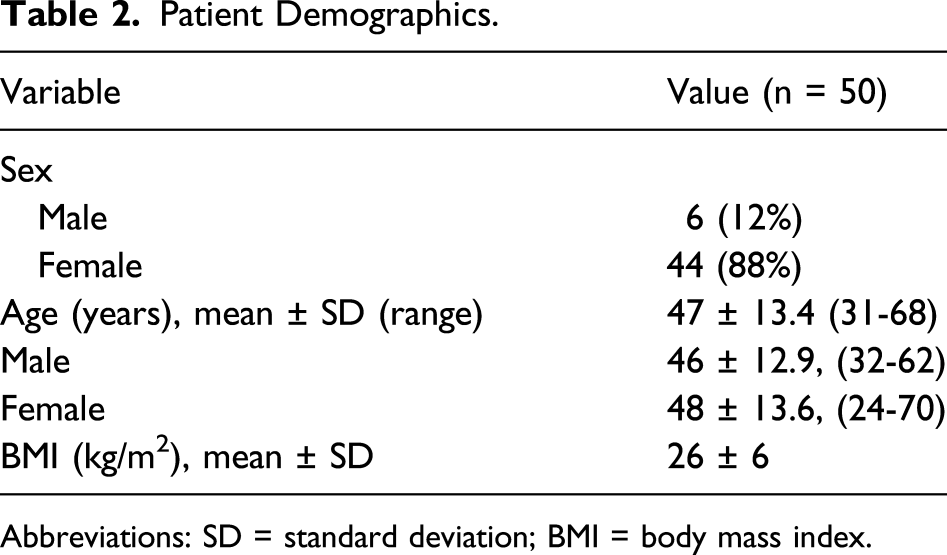
Abbreviations: SD = standard deviation; BMI = body mass index.
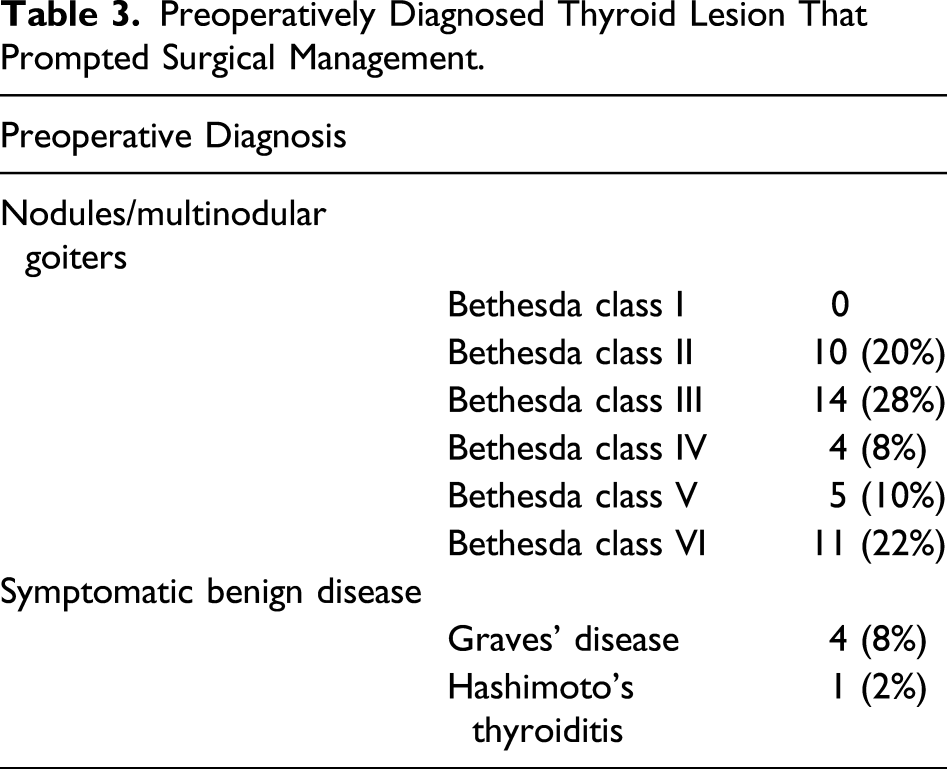
Preoperatively Diagnosed Thyroid Lesion That Prompted Surgical Management.
Surgical Technique
The originally described vestibular approach, and later modifications of this technique, has now become the established method by which the transoral technique proceeds.1,2,6,13 Our method involves placing the patient in the supine position on the operating table, with the neck mildly hyperextended. General anesthesia is administered after nasotracheal intubation is established (orotracheal is also an alternative). All patients received prophylactic antibiotics within 1 hour of incision time. For the first 10 cases, the antibiotic prophylactic coverage was extended to 5-7 days. As our protocol changed based on recommended guidelines, the following 40 cases received a prophylactic single dose of intravenous antibiotic during the induction of anesthesia. After induction, the oral cavity and upper neck are prepped and draped in sterile fashion. Three incisions are made through the alveolar mucosa of the lower lip vestibule, opposite to the incisors—a 15- to 20-mm transverse medial incision along with 2 vertical 5-mm incisions (the 2 lateral incisions are just medial to the canines and just in the inner aspect of the inferior lip to avoid injury to the mental nerve). Three ports: a central 10- to 12-mm port (a 5-mm port can at times be used in cases with small glands/nodules) and 2 lateral 5-mm ports are used. Before port placement, a working space is created by tissue dissection through the mentalis muscle with the use of electrocautery and/or blunt dissection. Subsequently, hydrodissection is performed with a Veress needle where about 60 cc of a mixture of NaCl containing epinephrine (1 mg in 500 cc NaCl) is injected to create a space beneath the platysma, which is then dilated with a blunt dissector (Anuwong dilator, Kelly-Wick tunneler, or Hegar dilators). 9 A 10- to 12-mm port is first placed through the central incision and then over the mandible advancing the port about 2 cm distally to the chin, taking care to avoid penetration of mentum skin. Next, the 2 lateral 5-mm ports are placed. The surgical space is then maintained with insufflation of CO2 at a pressure of 6 mmHg. A 30-degree 5- or 10-mm camera is then placed through the central port. A Maryland dissector and bipolar energy or ultrasonic energy device are used on either side of the camera for further development of the surgical space. 5 Dissection is carried out in the caudal direction toward the sternal notch, always staying beneath the platysma muscle and anterior to the strap muscles. Laterally, dissecting to bilateral sternocleidomastoid muscles further enhances exposure. Once the strap muscles are visualized, they are divided in the midline to expose the thyroid gland. The strap muscles are then retracted laterally by placing stay sutures preferably using monofilament sutures. The thyroid vessels are ligated and divided in sequence, starting with the middle thyroid veins to allow medial rotation of the thyroid lobe and then with the superior thyroid vessels, taking care to avoid injuring the external branch of the superior laryngeal nerve. The superior lobe is then mobilized, and the recurrent laryngeal nerve (RLN) is identified. The use of a nerve monitoring system is highly encouraged and has been used in all the cases. The inferior thyroid vessels are divided, and the rest of the lobe is then mobilized. The parathyroid glands are meticulously sought and preserved, along with their blood supply. The same approach and technique are then applied to the contralateral lobe, if a total thyroidectomy is undertaken. The gland is then placed in an endocatch bag and brought out through the central port.2,9,12,14 The strap muscles are approximated with the use of a running absorbable suture. The mentalis muscle is approximated with absorbable 3-0 sutures and the mucosa closed with 5-0 absorbable sutures. On postoperative day 0, the patients are immediately started on a liquid diet. From postoperative day 1, the patients are started on a soft diet and advanced as tolerated.
Results
Of the first 50 TOETVA procedures, 12 (24%) patients underwent a total thyroidectomy, 37 (74%) underwent a thyroid lobectomy, and 1 (2%) patient underwent a subtotal thyroidectomy.
Operative Details of the First Conducted TOETVA Procedures.
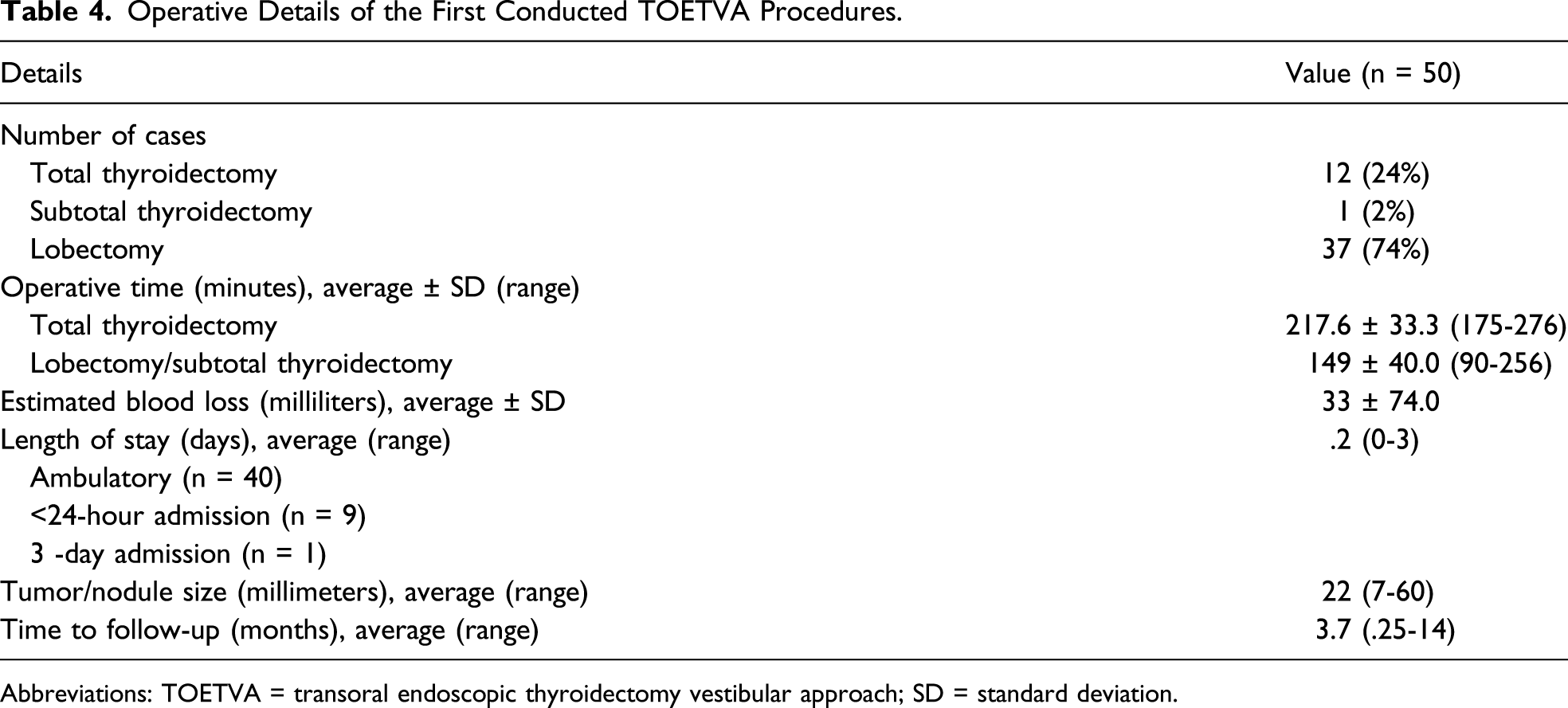
Abbreviations: TOETVA = transoral endoscopic thyroidectomy vestibular approach; SD = standard deviation.
Most patients who underwent the TOETVA procedure exhibited different degrees of postoperative ecchymosis/bruising in the overlying skin, but every case resolved within 1 to 2 weeks after the procedure. There were a total of 4 patients who suffered cutaneous lesions during the procedure: 2 (4%) patients had burns from dissection using electrocautery, and 2 (4%) had full-thickness tears of the skin that occurred during the subcutaneous dissection phase of the procedure. One (2%) patient had intraoperative blood loss that would be considered more than expected from a traditional thyroidectomy—as a result of damage to the anterior jugular vein. The bleeding was well controlled intraoperatively and did not require conversion to an open approach.
Intraoperative Events and Postoperative Complications Encountered During the First 50 TOETVA Procedures Performed.
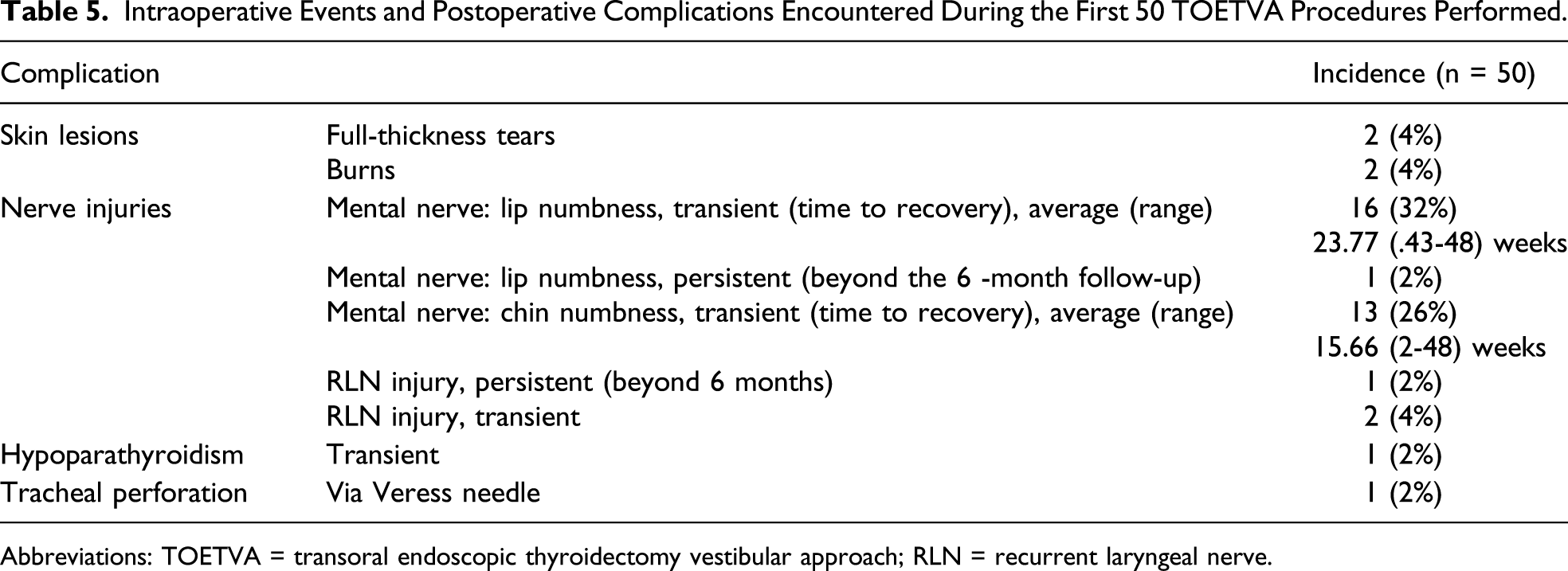
Abbreviations: TOETVA = transoral endoscopic thyroidectomy vestibular approach; RLN = recurrent laryngeal nerve.
Discussion
As was mentioned previously, in addition to being considered a NOTES procedure, this technique can be characterized as an endoscopic remote-access thyroid surgery. Sun et al 15 revealed that other remote-access procedures (eg total endoscopic thyroidectomy via areolar approach), such as TOETVA, could both achieve similar therapeutic effects of central neck dissection in the treatment of PTC when compared with open surgery. Compared with other remote-access approaches (eg transaxillary and BABA), TOETVA has the advantage of avoiding skin incisions and being truly scarless, although differences in effectiveness may be negligible.
Like any new surgical technique, there are early hurdles, never before encountered complications, and a learning curve. Given the use of laparoscopic equipment and a camera, with a cranial to caudal view, also described as a “bird’s eye view” of the thyroid gland, there is a steep learning curve. 13 The identification of anatomical landmarks from a new perspective and the need to have expertise in endoscopic surgery make this approach particularly challenging.16,17 For this reason, it is important that surgeons performing this procedure are proficient in the traditional open technique and general cervical dissection. In our experience, as many as 15 cases were needed to acquire the necessary skills to feel comfortable with this new approach.
International experience with TOETVA has unveiled complications that had never been encountered with conventional thyroid surgery. This was not unexpected, given the new route undertaken by this approach. Preceding the now standard vestibular approach, there was a sublingual approach to the transoral endoscopic technique that was abandoned because of complications, as result of violations to the floor of the mouth.18-20 The never before seen complications, reported in the literature, included mental nerve injury, nonpermanent cutaneous lesions, subcutaneous emphysema, and CO2 embolism.1,2,10,12,21-23 Another concern that has arisen with the transoral route is the uncertainty about prophylactic antibiotics. Despite the consensus, among surgeons performing traditional open thyroidectomies and/or central neck dissections, that prophylactic antibiotics are unnecessary, most surgeons regularly administer at least 1 dose of a first-generation cephalosporin within 1 hour of incision time, to cover normal skin flora.23,24 The difference with the transoral approach is that thyroidectomy is no longer a clean wound because there is violation of the oral mucosa; therefore, it should be categorized as a clean contaminated wound.13,25 The mucosa of the oral cavity is colonized with a very diverse bacterial population (eg Gram-positive aerobes/anaerobes and Gram-negative aerobes/anaerobes). In the literature, there have been no reports of surgical site infection with the oral vestibular approach.1,2,14,26 Different surgeons performing the procedure have used different antibiotics, with different spectrums of bacterial coverage, but we have made it our practice to use antibiotics that provide coverage of the polymicrobial flora found in the mouth. Amoxicillin-sulbactam, cefoxitin, or cefazolin+ an anaerobic covering antibiotic (clindamycin or metronidazole) would provide adequate coverage. 23
As was alluded to before, minor skin lesions have become a potential complication of the transoral thyroidectomy. The most frequently noticed lesion, in the immediate postoperative period, is ecchymosis/bruising of the chin and the anterior neck.19,20 This generally resolves within 1 to 2 weeks. Full-thickness injuries or piercing of the skin caused by the Veress needle during hydrodissection, electrocautery, or even with the use of clamps during dissection of the superior neck flap has been reported. Other skin injuries include skin tears at the lip commissures from traction or a burn caused by the energy devices used during the procedure.3,20
During the early phases of TOETVA, there was a high incidence of postoperative sensory deficits in the vicinity of the lower lip and chin. This problem was addressed by adjusting the placement of the lateral 5-mm ports. 26 The 2 vertical incisions for the 5-mm ports were repositioned to the vestibular mucosa medial to the level of the canines and just in the inner aspect of the inferior lip to avoid damage to the mental nerve. Even with these adjustments, the mental nerve can still be encountered during creation of the operating space, given the proximity to the port sites. 5 As a result of contact with the mental nerve, during creation of the working space, patients can present with transient lower lip and/or paresthesia. In all cases, our patients experienced complete resolution or, at the very least, significant improvement of their lower lip and/or chin numbness. To date, there has been nothing in the literature to indicate that there is a greater incidence of RLN among those undergoing TOETVA versus those undergoing open thyroidectomies. To the contrary, there have been various articles revealing TOETVA to be as safe as the open approach.27,28
With the exception of 1 patient who stayed for 3 days, most patients were managed as ambulatory surgery (n = 40) or as less than 24 h. admissions with an average LOS of .2 days. This differs from other large-volume institutions (eg in Asia), where social and cultural factors within the health care system, or protocols, perhaps dictate LOS.
TOETVA is being performed at various international institutions and multiple hospitals in the United States. There are studies proving its efficacy and safety profile, when compared with the traditional technique. 8 A common critique has been longer operative times, but as the steepness of the learning curves decreases, so will overall operative times. Mainstream applicability is only limited by a lack of understanding of the approach and lack of patient awareness that a cosmetically appealing alternative to the traditional open technique exists.
Conclusion
TOETVA has evolved from being a novel procedure to now being a legitimate alternative to the traditional transcervical technique in selected patients. For patients who are highly motivated, this technique can provide the means to manage thyroid disease in a scarless fashion. The literature and our experience have shown that it is safe and feasible with a reasonable surgical duration in the appropriate circumstances.
Footnotes
Author Contribution
Study concept and design: Gustavo Fernandez-Ranvier, William B. Inabnet
Acquisition of data: Gustavo Fernandez-Ranvier, William B. Inabnet, Aryan Meknat, Daniela Guevara
Analysis and interpretation: Gustavo Fernandez-Ranvier, Aryan Meknat, Daniela Guevara, Aida Taye, Hyunsuk Suh
Study supervision: Gustavo Fernandez-Ranvier, William B. Inabnet, Aida Taye, Hyunsuk Suh
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.