
Abstract
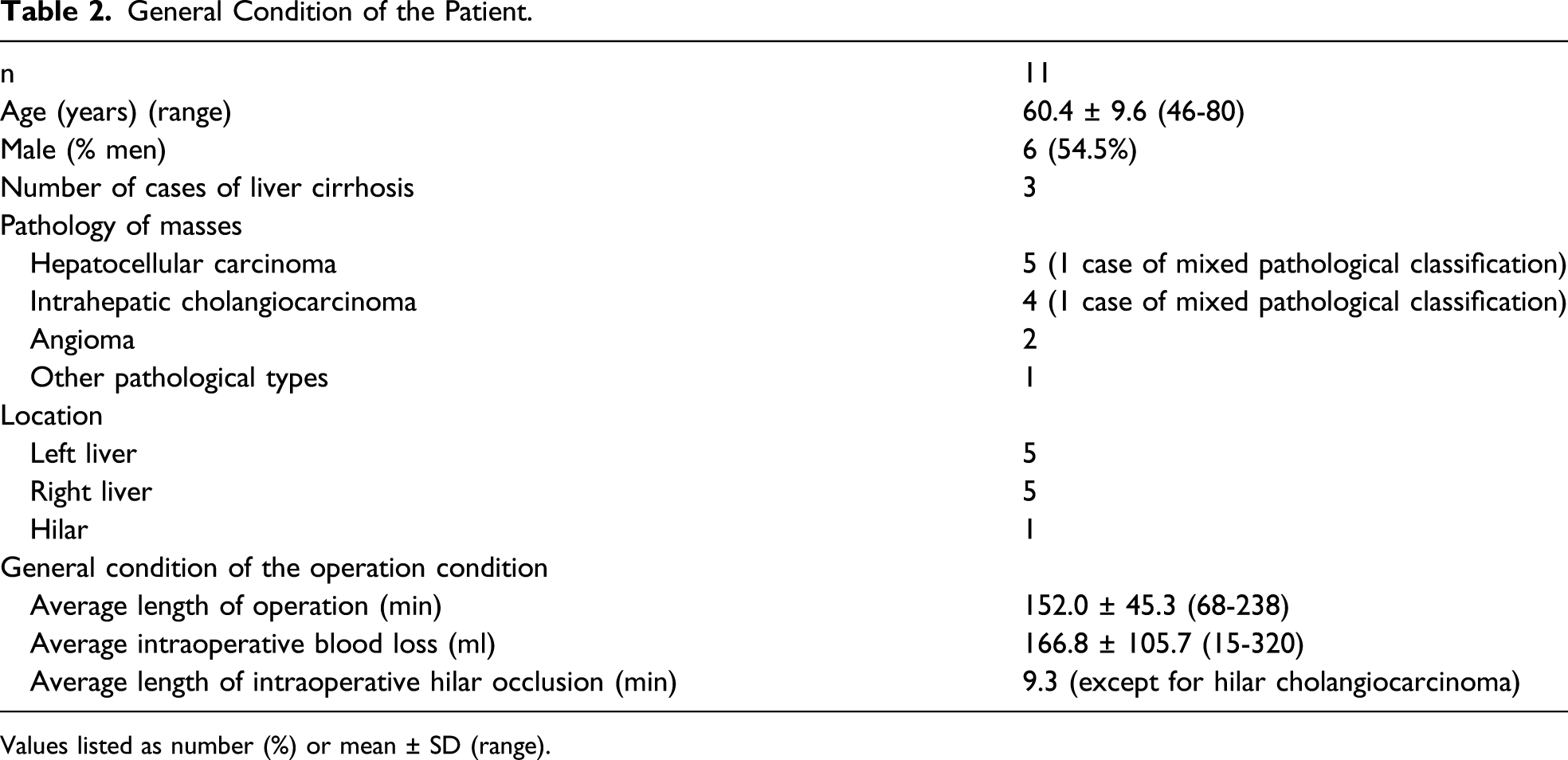
Liver surgery has entered the era of precision surgery. Therefore, how to optimize the resection of lesions and reduce the unnecessary time of liver ischemia and hypoxia have become the focus. A total of 11 patients who underwent fluorescence laparoscopic liver mass resection and preoperative three-dimensional (3D) reconstruction between August 2018 and July 2020 were evaluated. Liver cirrhosis occurred in 3 patients. The mean intraoperative blood loss was 166.8 ± 105.7 mL. The average length of the operation time was 152.0 ± 45.3 minutes. The average intraoperative hilar occlusion time was 9.3 minutes (except for hilar cholangiocarcinoma). The liver function of all patients, except patients with hilar bile duct carcinoma, returned to the preoperative level at 72 hours, and no serious complications occurred. 3D reconstruction combined with fluorescence laparoscopic imaging is safe and effective for precision liver resection.
Background
Precision liver resection is the gold standard of liver surgery. Its goals are to minimize intraoperative invasion, achieve the most reasonable level of liver protection, and maximize postoperative rehabilitation efficacy. Therefore, precise preoperative planning and rational intraoperative assessment are essential. The issue of how to reduce the time of liver ischemia without increasing the risk of hepatic hemorrhage has become a key point in precision liver resection. One of the difficulties involved is the complex anatomy of the liver, including the presence of several tubular structures, such as the hepatic artery, hepatic veins, portal vein, and bile ducts. These structures often have variations, and many of them are positioned close to major blood vessels and bile ducts, increasing the difficulty and risk of liver mass resection. 1 Medical three-dimensional (3D) reconstruction and visualization technology is a novel method of preoperative assessment that enables the rational 3D reconstruction of individualized livers and implementation of virtual surgery, thereby providing crucial assistance to preoperative assessment and surgical planning of precision liver resection. 2 Intraoperative indocyanine green (ICG) accumulates in liver tissues, causing the mass to fluoresce with sharply defined borders that present strong contrast with surrounding normal tissues. This effect allows surgeons to identify liver masses more accurately during precision laparoscopic liver resection. 3 The combination of the 2 techniques facilitates more accurate dissection and reduces the risk of bleeding and ischemia-induced liver injury during resection.
Methods
Patients
This retrospective study included a total of 11 patients who were admitted to our hospital between August 2018 and July 2020 and underwent preoperative 3D reconstruction and fluorescence-guided laparoscopic liver mass resection (the observation group). We randomly selected 10 patients who did not undergo 3D reconstruction of liver tumors before the operation and fluorescence laparoscopic imaging (the control group). All patients were operated on by the same main surgeon. And there were no subjective deviation and technical difference between the 2 groups. All patients were evaluated and underwent computed tomography (CT) before the operation. And patients in the control group underwent laparoscopic exploration or surgery. All study participants provided informed consent, and the study design was approved by the appropriate ethics review board.
The inclusion criteria were as follows 1 : confirmation of the lesion as a single mass based on preoperative evaluation combined with imaging examination, 2 preoperative Child–Pugh score of class A, 3 no history of liver surgery or abdominal trauma, 4 surgical indications for mass resection and successful performance of liver resection, and 5 no history of interventional embolization, neoadjuvant radiotherapy, chemotherapy, and other treatments prior to surgery. The exclusion criteria were as follows 1 : abnormal biliary excretion, 2 allergy to ICG or iodine, 3 major diseases of the heart, brain, lungs, and kidneys, 4 multiple liver lesions or extrahepatic metastasis that would contraindicate surgical treatment, and 5 pregnancy or lactation.
Procedures
All patients underwent preoperative abdominal contrast-enhanced CT and contrast-enhanced magnetic resonance imaging (MRI) of the liver. The PINPOINT Laparoscopic Fluorescence Imaging System (NOVADAQ, Canada) was used, which displays light-emitting diode visible light and near-infrared excitation light dual-source endoscopic images. The acquisition of intraoperative fluorescence images occurred as follows. NOVADAQ is equipped with 4 imaging modes: high-definition white light, SPY fluorescence, PINPOINT fusion fluorescence, and color-segmented fluorescence, with a control that allows for easy switching among the various modes. We used a Generator G11 ultrasonic scalpel (Ethicon Endo-Surgery, LLC Guaynabo, Puerto Rico, USA) and PSE45A Articulating Endoscopic Linear Cutter (Ethicon Endo-Surgery, LLC Guaynabo). All the patients were diagnosed using CT (Philips Brilliance ICT, Koninklijke Philips Electronics N.V., The Netherlands) and MR cholangiopancreatography (Philips Intera 1.5 T NMR spectrometer, Koninklijke Philips Electronics N.V., The Netherlands; GE Discovery MR 750 3.0T NMR spectrometer, General Electric Company, Connecticut, USA) before surgery.
Technique
All patients in this retrospective study underwent CT scanning that included upper abdominal routine scan, arterial phase, portal venous phase, and delayed phase scans. The slice thickness was 1 mm. The contrast agent was iohexol solution injection (35 g: 100 mL) at 350 mg I/mL. The contrast agent was administered through intravenous infusion via the upper limb using a high-pressure syringe in a volume of 90 mL and injection rate of 3 mL/s. 3D reconstruction was performed on the whole liver, space-occupying lesion, surrounding vasculature, and surrounding vital organs. We precisely localized the lesion site and its relationship with the surrounding vasculatures.
Intravenous infusion of ICG was routinely administered within 42-72 hours before the surgery. Patients with cirrhosis were administered ICG intravenously 72 hours before operation, and the remaining patients were administered ICG intravenously 48 hours before operation at .15 mg/kg. Full exploration of the abdominal cavity was performed once the laparoscope was inserted into the abdomen to re-evaluate the presence of abdominal cavity metastases. Real-time intraoperative guidance was provided by fluorescence imaging of the liver tumor under the 4 operational modes. Precise hilar anatomy was determined based on the imaging results of preoperative 3D visualization. The main surgeon and the assistant jointly assessed whether the duration of hepatic hilar occlusion could be reduced. The time of hilar occlusion was not subjectively reduced in all patients after intraoperative evaluation, and this aspect did not affect the decision of hilar occlusion. The surgeon and assistant made objective assessments of the section of the liver for resection and the need for hilar occlusion. During the operation, an ultrasonic scalpel was used to perform liver resection and hepatic portal anatomy, and the main trunk vein in the liver was disconnected using an articulating endoscopic linear cutter. All patients were evaluated for liver function 24 hours after operation, and patients with abnormal liver function were reevaluated for 72 hours.
Statistical Methods
The operation time, intraoperative blood loss, and intraoperative hilar occlusion time in the observation and control groups were analyzed and compared using the t test. A P value of <.05 was considered significant.
Results
A total of 11 patients were included in the observation group (6 men and 5 women; mean age: 60.4 ± 9.6 years). The pathology was hepatocellular carcinoma in 4 cases, choledochocystic carcinoma in 2 cases, hepatocellular carcinoma complicated with bile duct carcinoma in 1 case, hemangioma in 2 cases, intrahepatic cholelithiasis with bile duct cell hyperplasia in 1 case, and hilar bile duct carcinoma in 1 case. The mass of 5 and 5 patients was located in the right and left halves of the liver, respectively. Three patients had accompanying liver cirrhosis, but none of them reached the decompensation stage.
The average intraoperative hilar occlusion time was 9.3 minutes (except for hilar cholangiocarcinoma), and the longest intraoperative hilar occlusion time was 21 minutes. The observation group had a significantly lower blocking time than the control group (P < .05). The mean intraoperative blood loss was 166.8 ± 105.7 mL, and the liver function of 6 patients was normal or slightly damaged 24 hours after operation. There was no significant difference in intraoperative bleeding between the observation and control groups (P > .05). Even the average blood loss in the observation group was less than that in the control group. The liver function of all patients, except patients with hilar bile duct cancer, returned to the preoperative level at 72 hours. Only 1 patient in the control group had normal or mild liver function 24 hours after operation. Incision infection occurred in 1 case after operation, and no complications occurred in the remaining patients. The reason for incision infection occurrence was diabetes. The new technology does not increase the risk of intraoperative massive bleeding and postoperative dangerous complications. There was no significant difference in the average length and cost of hospitalization between the groups. The new technology did not increase the financial burden of the patients.
Discussion
Detailed Information of the Observation Group.
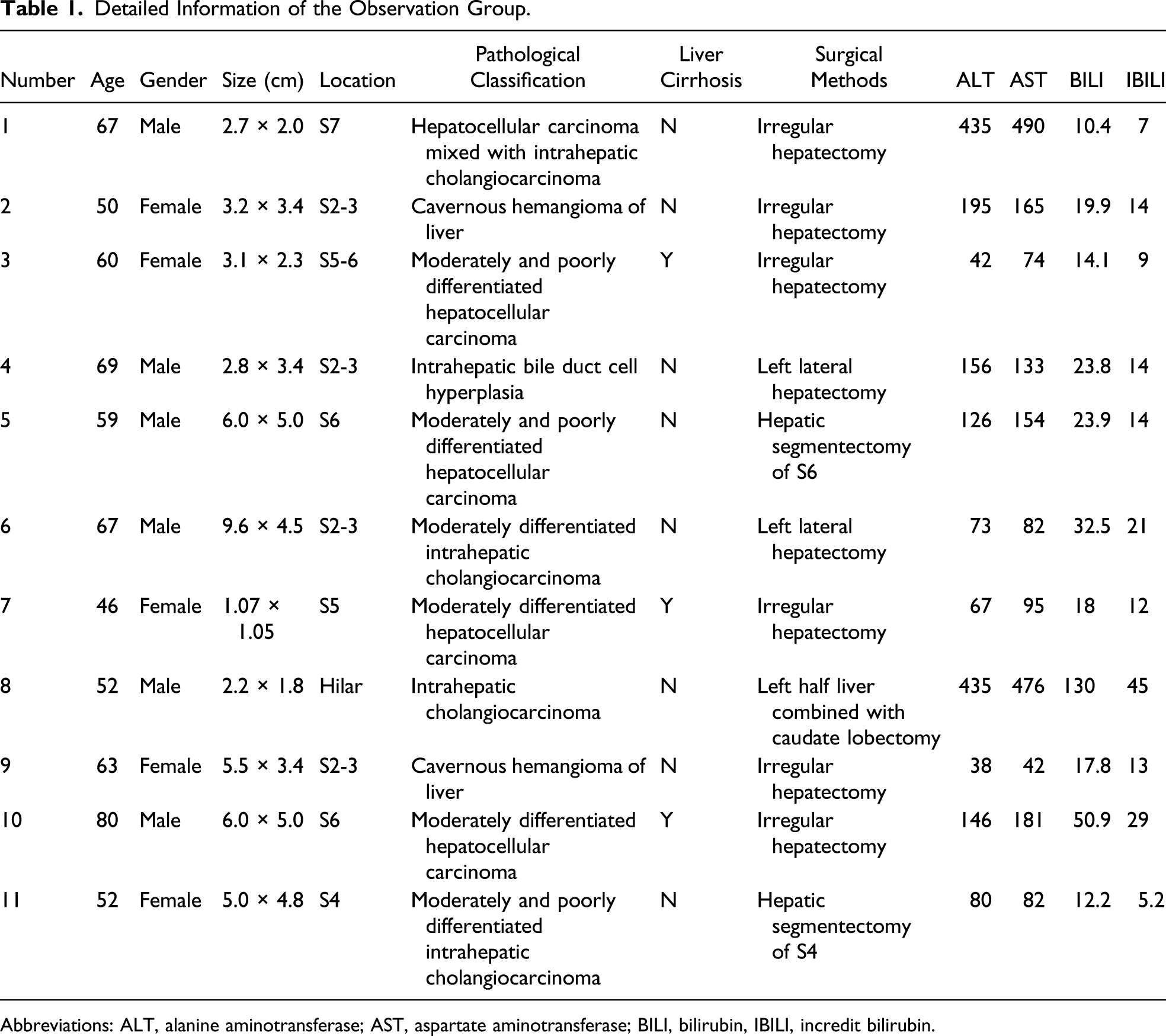
Abbreviations: ALT, alanine aminotransferase; AST, aspartate aminotransferase; BILI, bilirubin, IBILI, incredit bilirubin.
The preoperative imaging assessment is a crucial step in liver surgery. However, traditional imaging examinations lack a sense of cohesion and three-dimensionality, requiring the surgeon to perform “mental construction,” and the differences in the experiences of different surgeons lead to varying degrees of predictive deviations.
4
The 3D reconstruction technique used in this study accurately represents the direction of the hepatic veins, hepatic artery, and portal vein in the liver, as well as their relationships with the mass. It restores the actual sense of space in the liver tissues and blood vessels and enables full localization of the relationship between the mass and intrahepatic vasculature by means of rotation, magnification, splitting, and other techniques. Furthermore, it helps confirm the location of the lesion before the surgery and facilitates the localization of specific areas (areas with difficulties in anatomical localization)
5
(Figures 1A-1D). A rational approach and surgical plan should be designed to ensure that ligation and hemostasis are performed on important blood vessels adjacent to the mass. This helps to reduce the duration of anesthesia and hepatic hilar occlusion, decreasing intraoperative blood loss and enhancing surgical safety, thereby improving prognosis. In the observation group, there was a case of right hepatic tumor, adjacent to the middle hepatic vein, which was blocked by the right branch of the portal vein during the routine anatomic approach; therefore, we adjusted the conventional anatomical approach according to the visual image of 3D reconstruction to avoid the large amount of bleeding caused by the right branch injury of the portal vein and reduce the risk of increased time of hepatic portal ischemia for blind hemostasis (Table 2). (A) Three-dimensional reconstruction of the liver before operation, (B) relationship between the liver tumors and intrahepatic artery system, (C) relationship between the liver tumors and portal vein system, and (D) relationship between the liver tumors and hepatic vein system. General Condition of the Patient. Values listed as number (%) or mean ± SD (range).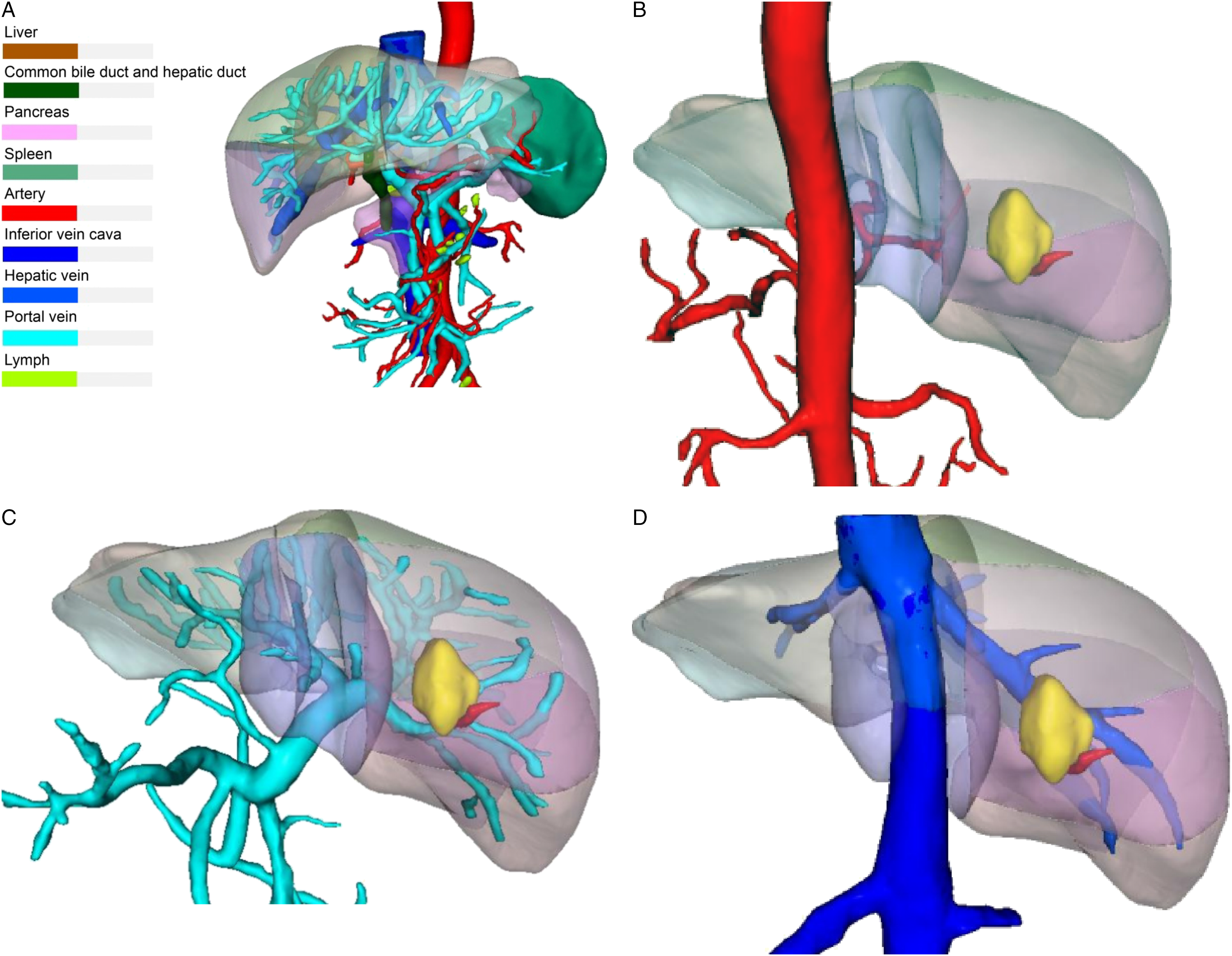
Because of the special anatomical location of the hepatic hilum, as well as the anatomical variations in hilar blood vessels and bile ducts, laparoscopic determination of hepatic hilar anatomy is key to the success of the surgery. 6 Surgeons no longer perform separation based on experience; rather, they conduct rapid identification and localization of key anatomical sites by synchronously adjusting the anatomical position of the patient’s hepatic hilum in the 3D reconstruction model. 3D reconstruction technology makes the planning of hepatic hilum pretreatment relatively easy. One patient in our cohort had hilar cholangiocarcinoma. Because tumors are characterized by their invasive growth, they often invade important blood vessels surrounding the hepatic hilum. 3D reconstruction allowed the surgeon to better clear the hepatic hilum and perform en bloc resection of all tissues within the hepatoduodenal ligament, except for the hepatic artery and portal vein. 7
Five cases in our patient group had hepatocellular carcinoma. 3D reconstruction technology provided real-time guidance for the separation of important vessels around the tumor, while completing the radical resection of the tumor, thereby optimizing the efficacy of radical treatment. It was also possible to accurately evaluate the precise location of the tumor, whether the tumor had invaded the blood vessels, and the degree of invasion preoperatively, thereby providing the best plan for intraoperative vascular dissection and ligation, 8 rather than blindly increasing the liver ischemia time to reduce intraoperative blood loss. The bleeding in the observation group was less than that in the control group, without a longer hilar blocking time. By determining the safety range and resectability in precision liver resection and ultimately deciding the most reasonable liver resection plane, this technique not only improves the precision of surgery but also prevents inoperable patients from undergoing “switch” surgery. 9
Because surgeons are unable to palpate the liver during laparoscopic surgery to locate solid space-occupying lesions, even with preoperative 3D localization prediction, the ability to trace the “precise anatomical path” in real-time in order to avoid important vasculature, thereby achieving “bloodless resection” without aggravating liver ischemia, represents a major breakthrough. Intraoperative 3D simulated surgery can synchronize the surgical field of vision in real time, and if there is a precise location of a solid tumor, it can combine 3D reconstructed image with the solid field of vision perfectly. Intraoperative ultrasound has long been used to compensate for this defect. Nevertheless, there remain significant limitations in ultrasound technology: First, it is prone to missing the diagnosis of microlesions with a diameter of <1 cm. 10 Second, the localization of superficial lesions of the liver is relatively difficult. Finally, and most importantly, it does not provide the surgeon with real-time localization and navigation during liver resection. Therefore, increasing emphasis and attention have been placed on visualization technologies for solid space-occupying lesions in precision surgery of the liver.
ICG fluorescence fusion imaging guidance technology has been used to guide laparoscopic partial liver resection. Its main advantage is that it determines the hepatic plane more accurately, while also having significant implications for guaranteeing the negative surgical margin. 11 The uptake of ICG by hepatocytes is achieved through the OATP1B3 and NTCP transporters, whereas excretion is carried out by the multidrug resistance–associated protein 2 (MRP2) transporter system on the hepatocyte membrane of the bile canaliculi. When tumors, heteroplasia, and cirrhotic nodules develop in the liver, its mechanism for ICG uptake remains normal; however, its mechanism for ICG excretion is impaired, thereby enabling ICG to remain in solid hepatic space-occupying lesions during surgery. 12 ICG is excited by external light wavelengths of 750-810 nm and emits near-infrared light at 850 nm. Finally, fluorescence imaging is performed during image visualization.
Differences exist in the imaging of particular masses. To accurately achieve bloodless resection, it is first necessary to be familiar with the fluorescence characteristics presented by space-occupying lesions (Figures 2A-2B). Moderately and well-differentiated hepatocellular carcinoma involves differentiated and mature cells that have equivalent ICG uptake to normal hepatocytes; however, tumor cells and tissues also lack an ICG excretion system; therefore, they mostly manifest as bright fluorescent nodules. The tumor cells of poorly differentiated hepatocellular carcinoma remain in an immature state,
13
while intrahepatic cholangiocarcinoma does not have hepatocyte components and, therefore, does not take up ICG. Nevertheless, the tumor compresses the surrounding tissues, which delays the metabolism of ICG by the surrounding tissues to a certain extent, thereby forming a ring of fluorescence around the tumor.
14
Studies have found that hepatic metastases also form rings of fluorescence when approaching or protruding from the hepatic envelope.
15
Van der Vorst and Miyata showed that the proliferation of immature hepatocytes and impaired expression of MRP2 led to the deposition of ICG in liver tissue surrounding the tumor.
16
Because of the spongy internal structure of liver hemangiomas that are themselves a mixture of tumor and liver tissues, they often exhibit uneven fluorescence imaging. Therefore, by using these characteristics, it is possible to judge the degree of tumor malignancy intraoperatively. Occlusion biliary drainage can also lead to liver staining, whereas localized intrahepatic bile duct stones can obstruct biliary drainage in the given liver segment, leading to the delayed disappearance of ICG fluorescence in the region. This is a new attempt to locate the fluorescence in nontumor hepatectomy. One patient in our cohort presented with left intrahepatic bile duct stones and hyperplasia that could be used to guide the identification and resection of diseased bile ducts. Regarding space-occupying lesions in the right liver, intraoperative real-time guidance of the section not only maximized the preservation of normal hepatic lobe tissue
17
but the irregular resection along the most accurate fluorescent border also avoided unnecessary intrahepatic vascular injury.
18
Preoperative 3D imaging allows the reconstructed image to be adjusted freely at 360° in real time during the operation and can be divided into liver segment imaging. According to the liver and tumor model of 3D imaging, the surgical image of real-time coincidence fluorescence imaging can even achieve the naked separation of secondary and even tertiary blood vessels in the fine anatomy of the ultrasonic scalpel. The mean duration of hepatic hilar occlusion in our cohort was 6.5 minutes, and 5 patients underwent right precision liver resection. The duration of hepatic hilar occlusion was controlled within 15 minutes, and occlusion was not implemented in 1 case. Thus, this greatly reduces the risk of injury to important vessels, thereby greatly reducing the degree of liver ischemic injury.
19
The observation group did not have a higher operation time and blood loss than the control group (Table 1). (A, B) Fluorescence laparoscopic imaging of the liver masses.
Despite the fact that studies have found the incidence of adverse reactions to ICG to be <.01%, attention should be paid to adverse drug reactions caused by individual differences. 20 In human blood vessels, ICG rapidly binds serum proteins throughout the body, taken up with high efficiency and specificity by hepatocytes and finally excreted in bile, without being involved in biotransformationand metabolism. 21
Our study has some limitations. Because of the sensitivity of ICG imaging, it has a high rate of false positives for intrahepatic nodules, especially in patients with relatively severe cirrhosis. Second, ICG imaging is significantly limited for deep exploration within liver tissues, which would naturally place higher demands on preoperative 3D imaging. Finally, ICG metabolism is affected by individual differences in liver metabolism; therefore, drug dosages and times required to achieve the optimal fluorescence imaging effect should be determined in the future. The new study is not limited to hepatectomy. We have recently tried this new technique in a patient with severe cirrhosis and portal hypertension because the tumor was close to the top of the diaphragm. Therefore, we have performed laparoscopic radiofrequency ablation of liver cancer and achieved good results.
In summary, preoperative 3D reconstruction and visualization technology combined with intraoperative fluorescence laparoscopic real-time navigation significantly reduces liver ischemia time, while also enabling the safe and minimally invasive completion of precision liver resection. It has provided a new direction for the implementation of liver resection without ischemia.
Footnotes
Author Contributions
Zhong-Kai Ni is in charge of conceiving and designing the study and writing the manuscript. Da Lin is in charge of providing critical revisions that are important for the intellectual content. Zi-Qiang Wang, Hai-Min Jin, Xiao-Wen Li, and Ye Li are in charge of collecting the data and analyzing and interpreting the data. Professor Hai Huang is in charge of approving the final version of the manuscript.
Study conception and design: Zhong-Kai Ni and Hai Huang
Acquisition of data: Zi-Qiang Wang and Xiao-Wen Li
Analysis and interpretation of data: Da Lin
Study supervision: Hai-Min Jin and Li Ye
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (grant no. 81202821), the Medical Science and Technology Planning Project of Health Planning of Zhejiang, China (grant no. 2013KYA169), and the Science and Technology Development Project of Hangzhou, Zhejiang, China (grant no. 20130633B19).