
Abstract
Background. There is still no standardized treatment for vaginal agenesis; surgical repair using a minimally invasive technique is a good option, as it offers rapid results along with a fast postoperative recovery. Objective. To describe a new modified Vecchietti procedure by a mini-laparoscopic approach with intraoperative use of indocyanine green fluorescence technology for the creation of a neovagina in the setting of congenital vaginal agenesis. Methods. Retrospective review of all cases of congenital vaginal agenesis submitted to a mini-laparoscopic modified Vecchietti procedure with intraoperative use of indocyanine green (ICG) fluorescence (between June and September 2019). Patient relevant medical history, surgical technique, postoperative care, outcomes, and complications are described. Results. Four patients with Mayer–Rokitansky–Küster–Hauser syndrome (mean age: 19 years; mean preoperative vaginal length: 1.5 cm) were included in the study. The procedure was completed successfully and uneventfully in all patients. External traction device was removed 5–7 days after surgery and replaced by external vaginal silicone dilators. This technique was able to create 10–11 cm neovaginas in 1 week; six weeks after surgery all patients had an epithelized 10.5–12 cm length and 2.5–3 cm diameter neovagina. Complications consisted of one case of isolated fever at the ninth postoperative day, solved with empiric antibiotic treatment. Conclusion. The mini-laparoscopic modified Vecchietti approach, associated with ICG fluorescence imaging, is feasible and effective in the treatment of congenital vaginal agenesis, as it is a simple and safe procedure with promising outcomes.
Keywords
Background
Mayer–Rokitansky–Küster–Hauser syndrome (MRKHS), also referred as Müllerian agenesis, Müllerian aplasia, or vaginal agenesis, is a rare congenital syndrome, with an estimated incidence of 1 per 4.500–5.000 women, caused by the embryologic underdevelopment of the Müllerian duct system, resulting in the congenital absence of the upper part of the vagina associated with a variable degree of uterine development, in women showing a normal 46, XX karyotype.1-4
Regarding the reproductive system, it is important to emphasize that the normal pelvic anatomy may be markedly distorted with rudimentary Müllerian structures being found in approximately 90% of these patients,5,6 which may include a single midline uterine remnant or uterine horns with or without an endometrial cavity — only 7–10% of these women are reported to have functional endometrium causing cyclic or chronic pelvic pain due to possible endometriosis from retrograde menstrual flux.7-13 By opposition, the ovaries are typically normal in structure and function since they have a distinct embryologic origin, although they can be found in atypical locations.4,9,14 In up to 53% of these women, concomitant congenital malformations can be found, mostly affecting the urinary tract (such as unilateral renal agenesis, pelvic or horseshoe kidneys, or anomalies of the collecting system) and skeleton (involving the spine, ribs, and extremities).1,15-22
There is still no standardized treatment for vaginal agenesis since every different method has its benefits and disadvantages and there are no comparative studies.
Notably, the Vecchietti procedure combines a surgical procedure with a mechanical method that acts by external controlled traction, resulting in progressive elongation of the vaginal mucosa and epithelialization of the outer layer skin, with the creation of a neovagina in approximately 7–10 days. 23 The use of a minimally invasive technique with concomitant vaginal and laparoscopic approaches — the modified laparoscopic Vecchietti procedure — was an important advance in this setting, resulting in shorter operative times with minor associated complications, being presently recognized as a safe, simple, and effective procedure.24-29
Mini-laparoscopy, with 5-mm optics and 3-mm trocars, is a recent and growing surgical option in gynecology with recent studies reporting its utility and feasibility in a variety of gynecological procedures with several validated benefits.30-34
Additionally, indocyanine green (ICG) is a fluorescent dye with a well-documented safety profile that is particularly useful for fluorescence-guided surgery because its excitation peak and emission peak are in near infrared (NIR).35,36 Its applications are evolving in many fields of medicine and surgery, including lymphography and sentinel lymph node mapping in oncologic surgery, along with angiography and tissue perfusion evaluation in gynecologic, urologic, digestive, and reconstructive surgery to evaluate the viability of tissues and to assess possible anastomoses sites or anastomotic leaks.36-40 This technology has been shown to improve the identification of key anatomical landmarks and pathological structures for oncological and nononcological procedures. 41
Objective
Our aim is to present a new modified Vecchietti procedure by a mini-laparoscopic approach with intraoperative use of ICG fluorescence technology for creation of a neovagina in the setting of congenital vaginal agenesis in patients with MRKHS.
Methods
We retrospectively reviewed all cases of congenital vaginal agenesis in the context of MRKHS referred to our institution between June and September 2019, surgically repaired by a mini-laparoscopic modified Vecchietti procedure with intraoperative application of ICG fluorescence. Patient relevant medical history, surgical technique, and postoperative care are described. Outcomes and complications including intraoperative anatomical findings, total operative time, neovaginal length at the seventh postoperative day, and neovaginal size 6 weeks after surgery are presented. All the procedures were performed by the same surgical team.
Approval of the local ethics committee was obtained (176-DEFI/158-CES). Written informed consent for patient information and images was obtained before the analysis and publication of data.
Patient Description and Evaluation
All patients included in the study had primary amenorrhea, normal growth and pubertal development and normal external genitalia; all presented a markedly shortened vagina, appearing as a 1–2-cm depth vaginal pouch. The karyotype was 46, XX in all cases. The patients were evaluated for the presence of uterine remnants, either with transrectal ultrasonography, with pelvic MRI or with diagnostic laparoscopy, and for the presence of other urinary or skeletal congenital malformations. All patients were evaluated with a pelvic ultrasound to assess the dimension of the rectovesical space. The primary reason that led these patients to search for neovaginal reconstruction was the desire to start a normal sexual life, except for one case in which the goal was to restore normal vaginal anatomy due to the psychological impact of the malformation.
Case 1
An 18-year-old patient diagnosed with MRKHS in the setting of primary amenorrhea. Regarding her medical history, she also had an interauricular communication surgically repaired in childhood. No other congenital anomalies were identified. Her evaluation included a pelvic MRI in which uterus and vagina were not identified, suggesting uterine and vaginal agenesis; ovaries were present without apparent anomalies. A diagnostic laparoscopy was performed, confirming the absence of the uterus and vagina and revealing normal-appearing ovaries and the presence of the distal part of the tubes bilaterally.
Case 2
A 19-year-old patient diagnosed with MRKHS in the setting of primary amenorrhea and intense cyclic pelvic pain. Regarding her medical history, she also had Tetralogy of Fallot which was surgically corrected in childhood. No other congenital anomalies were identified. Her evaluation included a transrectal ultrasound which revealed a 59 × 32-mm anteverted uterus (fundus and body) with trilaminar endometrium, in which cervix and vagina were not identified; the left ovary had normal appearance, and the right ovary showed a 22-mm diameter tumefaction, suggestive of an endometrioma. A pelvic MRI displayed a pelvic uterus lateralized to the right with regular dimensions of the fundus and body and a small isthmus, as well as agenesis of the cervix and vagina; an endometrioma was seen in the right ovary while the left ovary had a normal appearance.
Case 3
A 19-year-old patient diagnosed with MRKHS in the setting of primary amenorrhea. No record of other congenital anomalies. Her evaluation included a pelvic MRI in which the uterus and vagina were not identified, suggesting uterine and vaginal agenesis; ovaries were asymmetric with a normal appearing left ovary and a larger right ovary with a less evident structure, being considered the hypothesis of a dysgenic gonad.
Case 4
A 19-year-old patient diagnosed with MRKHS in the setting of primary amenorrhea. Regarding her medical history, to emphasize the presence of multiple concomitant malformations including congenital heart disease (interauricular communication and interventricular communication) surgically corrected in infancy, horseshoe kidney, and epilepsy controlled with oral medication. Differently from the other cases, on physical examination, she was found to have low stature for her age, obesity, and hypotelorism with micrognathia, despite the normal feminine karyotype. Her evaluation included an abdominopelvic ultrasound and a pelvic MRI in which the kidneys were not identified in the normal topography, being found in a pelvic location at the presacral space and with apparent horseshoe morphology; uterine and vaginal agenesis were found; ovaries were present bilaterally (more lateralized than usual but with normal dimensions and morphology).
Treatment options were discussed with the patients, and decision was made to perform a minimally invasive surgical correction, using a mini-laparoscopic modified Vecchietti procedure together with ICG fluorescence.
Surgical Technique
We performed a mini-laparoscopic modified Vecchietti procedure, using 3-mm instruments (Karl Storz GmBH & Co KG, Tuttlingen, Germany) (Figure 1), under general anesthesia. Mini-laparoscopic instrument set used to perform the procedure. (KARL STORZ, GmbH and Co. KG, Tuttlingen, Germany).
Furthermore, the instrumentation set used for the procedure consisted of a traction device (26188SA, Karl Storz GmBH & Co KG, Tuttlingen, Germany) (Figure 2A), a straight thread-bearing needle (26188FT, Karl Storz GmBH & Co KG, Tuttlingen, Germany) (Figure 2B), a curved thread guide (26188FL, Karl Storz GmBH & Co KG, Tuttlingen, Germany ) (Figure 2C), and a pluggable segmented vaginal dummy (26188PP, Karl Storz GmBH & Co KG, Tuttlingen, Germany) measuring 11 × 2.4-cm and attached to two nonabsorbable threads (Ethibond Excel® 2/0 ) (Figure 2D). Instrument set used to perform the procedure. (A) Abdominal traction device. (B) Straight thread-bearing needle. (C) Curved thread guide. (D) Segmented vaginal dummy. (KARL STORZ, GmbH and Co. KG, Tuttlingen, Germany).
The procedure started by drawing of the external traction device limits on the patient’s abdomen to mark the area in which it would be placed at the end of the procedure. Mini-laparoscopy was initiated, using the 5-mm umbilical port for camera manipulation and two 3-mm lateral ports along with the 3-mm suprapubic port for instrumentation; direct visualization of the pelvic anatomy was performed in an attempt to identify the ovaries and uterine structures. The camera system used was a NIR imager device Image 1 Spies (Karl Storz GmBH & Co KG, Tuttlingen, Germany).
A 30⁰ cystoscopy was performed with bilateral visualization of both ureteral meatus. Twenty-five milligrams of ICG were dissolved in 10 mL of sterile water and injected into both ureteral orifices using 6F ureteral catheters. After a few seconds, the bladder and the ureters paths became visible due to the fluorescence offered by the camera and light source system (KS-20133701-1, Karl Storz GmBH & Co KG, Tuttlingen, Germany).
A mini-laparoscopic dissection of the rectovesical space was performed while a cystoscope light was placed against the vaginal dimple, allowing intraperitoneal identification of the vaginal pouch; then, vaginal introduction of the straight thread-bearing needle under laparoscopic visualization was performed with subsequent intraperitoneal suspension of the threads connected to the vaginal dummy. After the needle insertion, a cystoscopy was routinely performed to confirm bladder integrity and guide the introduction of a suprapubic vesical catheter (suprapubic cystostomy). Following, an abdominal lateral-umbilical incision was made at the external traction device placement site, previously marked at the beginning of the surgery, and a curved thread guide was introduced subperitoneally across the anterior abdominal wall until the rectovesical space firstly dissected. The thread was passed through the suture carrier, which was then exteriorized through the lateral-umbilical abdominal incision. This procedure was repeated contralaterally; tension of the threads on the segmented vaginal dummy was confirmed.
Parietal peritoneum was closed on the site of dissection of the rectovesical space, using monofilament absorbable suture (Monosyn® 2/0). The external traction device was placed over the abdominal wall, and the previously exteriorized threads were attached to the device producing the necessary tension on the vaginal segmented dummy.
At the end, mini-laparoscopic instruments were removed under direct visualization, and abdominal millimetric incisions were closed with Steri-strips™ (3M, St. Paul, Minnesota); the cystostomy catheter was fixed to the anterior abdominal wall by a nonabsorbable suture (silk 1/0). Key steps of this technique are illustrated in Supplementary Video 1.
Postoperative Care
After surgery, all patients remained under epidural analgesia for 3 days to control potential pelvic pain. Early mobilization after surgery was allowed, with patients starting ambulation 6 hours after the procedure.
Adjustment of the traction device was performed every day, to stretch the threads 1–1.5-cm further every day. All patients had the device removed when the vaginal length reached 10–11-cm (corresponding to the internalization of the segmented vaginal dummy), which occurred between 5–7 days after surgery, and replaced for a mechanical dilator. We used silicone dilators with a blunt end, which are softer, more comfortable to introduce and well tolerated by patients (Soul Source silicone vaginal dilators®-SOUL SOURCE THERAPEUTIC DEVICES, INC., Los Angeles, United States of America – Figure 3). The suprapubic vesical catheter was removed right after the traction device removal. Vaginal dilators used as maintenance therapy. (SOUL SOURCE THERAPEUTIC DEVICES, INC, Los Angeles, United States of America).
All patients were discharged with the indication to use the dilator during 24 hours per day in the first 2 weeks (removed only to intimal hygiene and physiologic needs); after that, the daily time of usage was progressively shortened. Every time the dilator was removed and reintroduced, it was counseled the usage of topic estriol ointment or povidone-iodine ointment. Decision to progress in dilator size was made by the clinician, with all patients starting with a 2.2-cm diameter dilator.
A close follow-up was performed with patients being evaluated twice a week during the first 2 weeks after discharge, weekly until the sixth week and then twice a month.
Results
Outcomes and Complications
Between June and September 2019, a total of 4 patients with congenital vaginal agenesis in the context of MRKHS were submitted to surgical treatment in our center, using a modified Vecchietti procedure by a mini-laparoscopic approach with intraoperative application of ICG fluorescence.
Intraoperative Anatomic Characteristics of the Pelvic Organs.
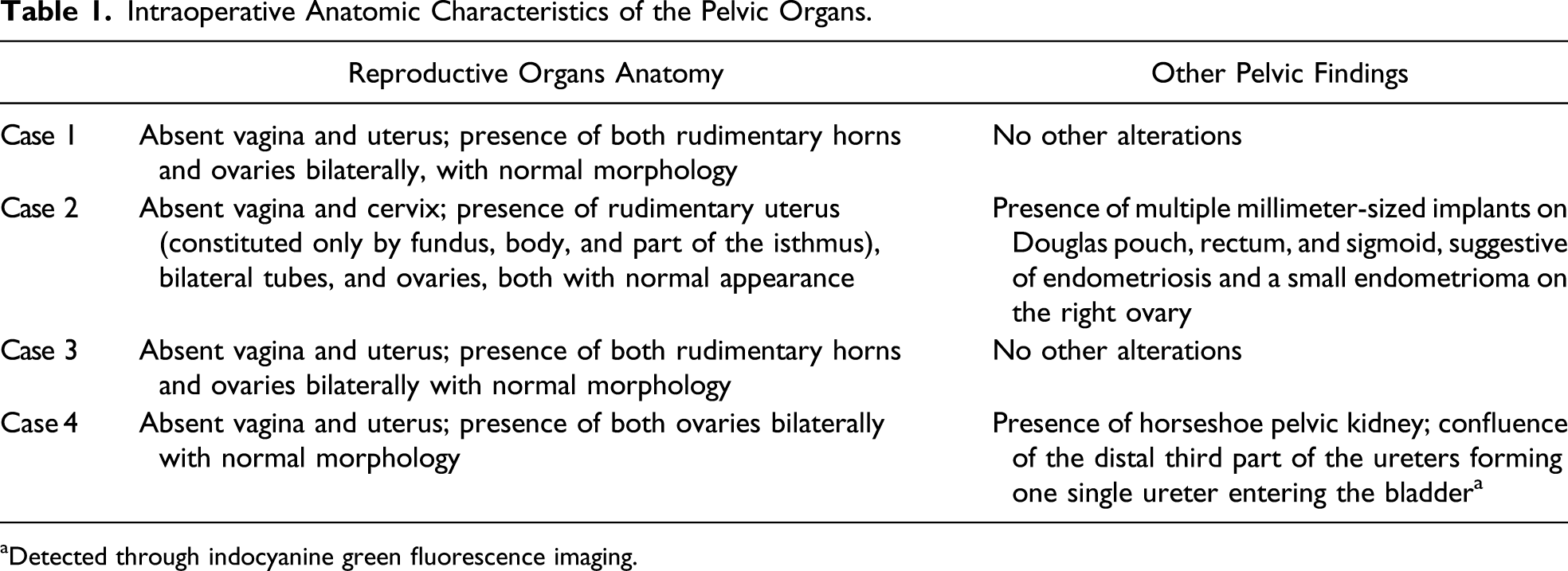
aDetected through indocyanine green fluorescence imaging.
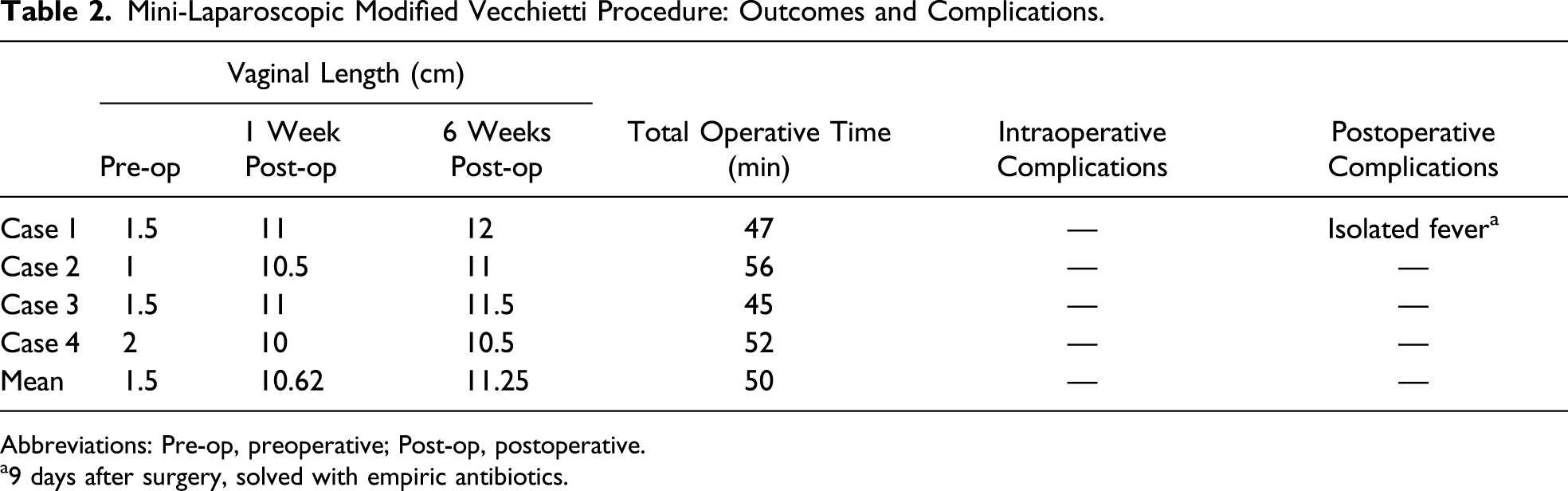
This technique was able to create 10–11-cm length neovaginas in 5–7 days. Six weeks after surgery, all patients had an epithelized 10.5–12-cm length and 2.5–3-cm diameter vagina, allowing for easy introduction of 2 fingers, were well adapted to the dilator and able to start satisfactory sexual activity. Regarding complications, 1 patient had isolated fever 9 days after surgery, which was solved with empiric antibiotic therapy. Septic workup and urine culture were negative, and CT scan of the abdomen and pelvis showed no signs of infection and an 11.8-cm length vagina (Figure 4). This complication is categorized as a type II postoperative complication in the Clavien–Dindo classification and as a type I postoperative complication in the Satava classification.
42
No other complications were found. Main outcomes and complications of this procedure are summarized in Table 2. Abdominopelvic CT scan performed 10 days after surgery showing an 11.8-cm depth vaginal canal in a sagittal plane. Mini-Laparoscopic Modified Vecchietti Procedure: Outcomes and Complications. Abbreviations: Pre-op, preoperative; Post-op, postoperative. a9 days after surgery, solved with empiric antibiotics.
Discussion
The main advantage of the Vecchietti procedure for the creation of a neovagina lays in its simplicity and rapid results. Since the early 90s that safety and success of the Vecchietti procedure, namely, the laparoscopic approach, had been successively and consistently reported. Classically, the success of this technique in the creation of a neovagina in the setting of vaginal agenesis has been defined as a resultant vaginal length of 6-cm or more, allowing for sexual intercourse. 43
Developing a neovagina from natural vaginal tissues may provide the greatest success and sexual satisfaction, as there is no tissue harvesting or grafting, which avoids accessory procedures and represents an advantage comparing with other surgical techniques.22,43-47
Comparing with the nonsurgical dilation techniques, it has the main advantage of applying continuous uninterrupted traction to the vaginal tissue, creating a functional vagina in a considerably shorter period (a few weeks vs. several months).48-51
Using the laparoscopic approach adds the advantages of a minimally invasive technique, such as early ambulation and less postoperative pain, combined with the possibility of a better visualization due to image amplification which improves surgical precision and minimizes the risk of iatrogenic lesions. These advantages are even more evident with the use of mini-laparoscopic instruments whose manipulation requires a delicate surgical technique and even more precise surgical dissection, resulting in less postoperative pain and also better aesthetic results.30,31 Benefits of mini-laparoscopy are already reported, including an enhanced cosmetic outcome and less tissue trauma, which may decrease postoperative pain without additional operative time or complications.30,31 Higher aesthetic satisfaction with scars after mini-laparoscopy has been pointed as a key benefit of this approach, since it is consistently found in a variety of surgical procedures for gynecology, general surgery, pediatrics, and urology.31-34
Therefore, the mini-laparoscopic approach shows important benefits in this specific population, since we are treating young women, whose cosmetic results often have a significant impact on patient satisfaction and self-esteem. Moreover, it is also adequate for this specific procedure, since it is a relatively simple technique with no complex dissection, perfectly adapted for 3-mm trocars, providing better aesthetic results while keeping the low morbidity associated with the classical laparoscopic approaches.
In fact, as above, several publications had already stood the benefits and safety of the laparoscopic-modified Vecchietti procedure;24-29 however, we are the first to publish the results of a mini-laparoscopic approach.
Notably, with the previously described surgical technique, which added some simple variations to the classically reported laparoscopic Vecchietti procedure, along with the use of the recently developed instruments, we were able to create 10–11-cm length neovaginas in 1 week, and this length was successfully kept at 6 weeks after surgery, with minimal complications. This minimally invasive method for neovagina creation appears to be effective. It may represent an advance in the treatment of these patients, resulting in a regular-sized functional vagina only in a few weeks after surgery, which positively influences their self-esteem, quality of life, and motivation with the use of dilators as maintenance therapy.
Indeed, there are some steps that may have contributed for the success of this technique. A key step in patient evaluation and clinical decision to perform the vaginal correction using this technique is the preoperative ultrasound assessment of the rectovesical space, particularly the distance between the bladder and rectum, to ensure that there is sufficient space to create the neovagina.
Intraoperative use of ICG fluorescence imaging for ureteric mapping is also an interesting approach in this setting to identify possible urologic malformations, as frequently seen in patients with MRKHS. Patient preoperative imaging evaluation may not accurately identify the anatomy of the urinary tract, making it vulnerable to intraoperative iatrogenic lesions. Considering that MRKHS patients have a distorted pelvic anatomy, the possibility to perform the intraureteral ICG administration with intraoperative real-time visualization of the bladder and ureteral location was helpful in many ways: first, and unlike with intravenous ICG use, only the urinary tract was highlighted by fluorescence, allowing for more accurate identification of these structures; second, since it improved the identification of critical anatomical landmarks, it helped to perform a safer and faster dissection of the rectovesical space, one of the most susceptible steps for the occurrence of iatrogenic lesions to the urinary tract, reducing surgical time. Hence, ICG technology adds great value to the surgical procedure, since it enables for proper anatomic identification in a distorted pelvis and may provide extra safety and precision to the surgical procedure, without an increase in operative time. In fact, despite the growing applications of ICG imaging in gynecology, as far as we know, we are the first to report the use of intraureteral ICG administration for bladder and ureteric mapping in the gynecological surgical approach to Müllerian anomalies: a feasible and safe way to accurately identify the ureter, which is a crucial anatomical landmark in several gynecological procedures.
Another important step is the placement of the cystoscope light against the vaginal dimple for mini-laparoscopic visualization of the vaginal pouch, ensuring an accurate placement of the thread-bearing needle and, consequently, of the vaginal dummy, which represents an advantage for proper anatomical restitution and minimizes the risk of iatrogenic pelvic organ lesions (such as accidental bladder perforation).
Of note, the surgical placement of the suprapubic bladder catheter helps to prevent the development of urinary retention caused by compression of the urethra by the mechanical dummy used to create the neovagina.
Additionally, selection of the proper dilator for each patient is crucial to ensure a good postoperative compliance, being usually preferred softer and malleable devices which should be first tried with medical assistance. Finally, ensuring a close follow-up and an easy access to medical care may contribute to the success of this procedure, as a way to stimulate patient motivation with the maintenance therapy and monitor the development of complications.
One limitation of our study is the number of cases presented, by now of four. Another limitation of our study is the short postoperative follow-up period, by now of 2–4 months. Nevertheless, these patients will continue their regular follow-up, and future studies may clarify the long-term results of this procedure.
Conclusion
The mini-laparoscopic modified Vecchietti approach, associated with ICG fluorescence imaging, is feasible and an effective approach in the setting of vaginal agenesis in MRKHS patients, as it is a simple and safe procedure with promising outcomes.
Supplemental Material
Footnotes
Acknowledgments
We would like to express our gratitude to Professor Joerg Keckstein for the collaboration in the first surgical cases and cooperation in postoperative patient orientation.
Author Contributions
Study conception and design: Andreia Fontoura Oliveira and Hélder Ferreira
Acquisition of data: Andreia Fontoura Oliveira
Analysis and interpretation of data: Andreia Fontoura Oliveira
Study supervision: Hélder Ferreira
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.