
Abstract
Objective. The objective is to determine the possible improvement in outlet obstructive constipation symptoms after vaginal stent treatment for rectocele. Methods. Female patients with rectocele (n = 156) accompanied with outlet obstructive constipation were selected in this study. Longo’s obstructed defecation syndrome (ODS) questionnaire, rectoanal pressures, and rectal balloon expulsion (BET) were evaluated at baseline, 1 month follow-up, and 6 months follow-up. Moreover, the side effects and the potential reasons for giving up treatment were also detected. Results. Vaginal stent significantly decreased the straining intensity, shortened the straining extensity time, decreased the use of laxatives, and alleviated the symptoms of incomplete evacuation (P < .05). The vaginal stent also increased the rectal pressure and shortened the balloon expulsion time (P < .05). Conclusions. As an effective, feasible, and safe procedure, the vaginal stent can be recommended as a treatment of choice for rectocele combined with outlet obstructive constipation.
Keywords
Introduction
Pelvic floor disorders (PFDs), including urinary incontinence (UI), fecal incontinence (FI), pelvic organ prolapse (POP), and sexual dysfunction, are common debilitating conditions among women across the world. 1 Rectocele is a type of POP, in which the anterior wall of the lower rectum and posterior vaginal wall are curved and protrude into the vaginal canal due to defective or weak rectovaginal septum.2,3 Rectocele combined with obstructive constipation symptoms, such as sensation of blockage of the rectum, inability to evacuate, rectal pain and/or feeling incomplete evacuation, is the common manifestation. 4 By estimation, the lifetime risk of rectocele having surgery for pelvic disorder is 11.1% by the age of 80 years, with 46% of those who undergo repairing defects in the posterior compartment. 5 The weakness of posterior pelvic floor supporting system, including uterosacral ligament, rectovaginal septum, and perineal body6,7, reportedly causes the rectocele during defecation because of a pressure gradient created by the higher intrarectal pressure and the lower vaginal pressure, which may induce the symptoms of outlet obstructive constipation.8-10 For treatment of rectocele, reinforcing and repairing the posterior pelvic supporting system might be promising and effective strategies, such as posterior colporrhaphy, transanal plication, abdominal suspension, and mesh implantation.11-13 However, the potential risk for those therapeutic strategies is the complication of surgery and the unpredictability of prognosis. In the present study, we have innovatively designed a vaginal stent, which reinforces the uterosacral ligament-rectovaginal septum-perineal body system and improves the symptoms of obstructive constipation.
Methods
Participants
This study was approved by the Ethics Committee of Shengjing Hospital of China Medical University. Written consent was obtained from all study subjects. Between April 2016 and March 2018, female patients with rectocele in Pelvic Floor Disease Diagnosis and Treatment Center of China Medical University-affiliated Shengjing Hospital were evaluated to meet the following inclusion criteria: (1) fulfilling the Rome III criteria 14 ; (2) undergoing constipation more than 6 months; and (3) history of excessive straining on defecation with normal bowel frequency. The excluded criteria included: (1) younger than 18 years old or deny sexual life history; (2) frequent or chronic bacterial vaginosis; (3) active or chronic vaginal ulcerative disease; (4) megacolon or megarectum; and (5) cognitive impairment. Female patients (n = 156) who were eligible based on the inclusion criteria were invited to take part in the study at baseline and distributed by computerized randomization into the stent or control groups (n = 78/each group). Nine women in the stent group failed in the initial fit and were allocated in the control group. Moreover, 4 patients in the stent group and 8 patients in the control group loss follow-up because they were no longer in contact. 7 patients gave up the stent treatment. At last, 58 patients in the stent group and 79 in the control group completed the study (Figure 2). This study was nonintention-to-treat analysis.
Procedure
A newly designed vaginal stent (Figure 1) was inserted into the vagina of the patient in the stent group. The stent is made up of polypropylene. The vaginal stent was an inverted trapezoidal structure, with a thickened surrounding structure. The upper edge was wider which could strengthen the uterosacral ligament, and the lower edge was narrower which could strengthen the perineal body. The main structure of the stent could strengthen the rectovaginal fascia. There were holes in the surface of the stent to facilitate the secretion of vaginal secretions. A detachable handle was designed. The patient could remove the handle in daily life and left the stent in the vagina to relieve the rectocele. The handle could be installed according to individual needs when defecation, to facilitate the patient to give a stress to the rectum direction, which could prevent the rectum hernia to the vagina, therefore relieved the symptoms of the outlet obstructive constipation. In addition, the angle of the handle could be adjusted to help the patient selecting the appropriate stress angle. A newly designed vaginal stent.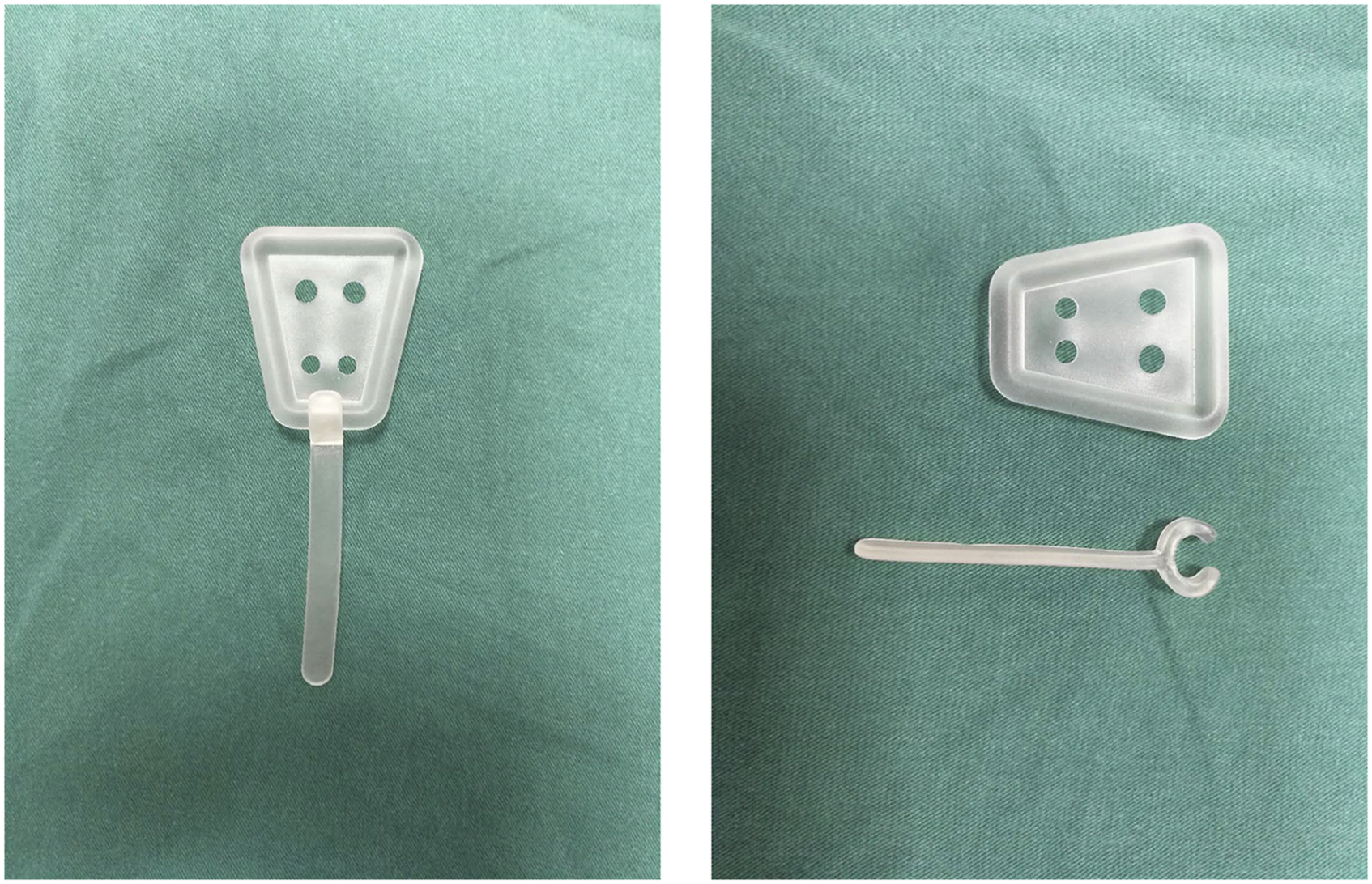
An initial fit should be made first aimed to determine the correct size. An appropriately sized intravaginal stent was placed into the vagina by the same experienced gynecologist based on the vaginal length and length of the genital hiatus. The patient tested the vaginal stent while walking around for 30 minutes and squatting 10 times. If the right size was found, the initial fit was considered successful. If the initial fit was unsuccessful, the patient would be allocated to the control group. After placement, all patients received instructions about vaginal stent treatment. The vaginal stent should be inserted in the morning and taken out before sleep at night. Estrogen ointment was allowed to use for the patients with severe vaginal atrophy. The handle of the stent was encouraged to used when defecation. Handle placement angle could be adjusted according to the individual situation of the patient. With the help of the handle, a backward stress could be given to the vaginal stent, which prevents the rectal hernia into the vagina to alleviate the outlet constipation symptoms. Most of patients placed the vaginal stent was for the whole time, but some with inflammation and/or ulceration only placed it for defecation. The control group did not add additional medical intervention. There was a suggestion for the patient to increase the fiber content in food, the daily intake of liquid, and activities appropriately. The same suggestion was also encouraged in the stent group.
Measurements
Patients in both groups were asked to complete the Longo’s obstructed defecation syndrome (ODS) questionnaire. The anorectal manometry test and the rectal BET examination were acquired immediately before the study, and 1 and 6 months after the study, respectively. To measure the qualification of obstructed defecation, the ODS questionnaire composed of 9 items, which reflected different clinical manifestations. The summed global scores of ODS range were 0-40. The total score and each question score were analyzed. The number of people with different symptoms was also compared according to ROME III criterion. 15
Rectoanal pressures were measured at rest, during squeeze, and simulated evacuation with an HRM catheter (Sierra Scientific Instruments; Los Angeles, CA).16,17 Rectal balloon expulsion test (BET) was evaluated with validated techniques. 18
During the pelvic examination, patients were in the lithotomy position. The side effects and potential reasons for giving up treatment were detected, including vaginal erosions, abnormal vaginal bleeding, vaginitis, voiding difficulty, difficulty in inserting or removing stent, stent falling out, discomfort, fear of foreign body reaction, and nonimproving symptoms.
Statistical Analysis
SPSS19.0 software was used in statistical analysis. The comparison means between the 2 groups were performed by a Mann-Whitney U test for skewed distributed variables. ANOVA was used for multiple groups of data. Chi-square and rank test were used for proportion comparison. A P value <.05 was considered statistically significant.
Results
Baseline
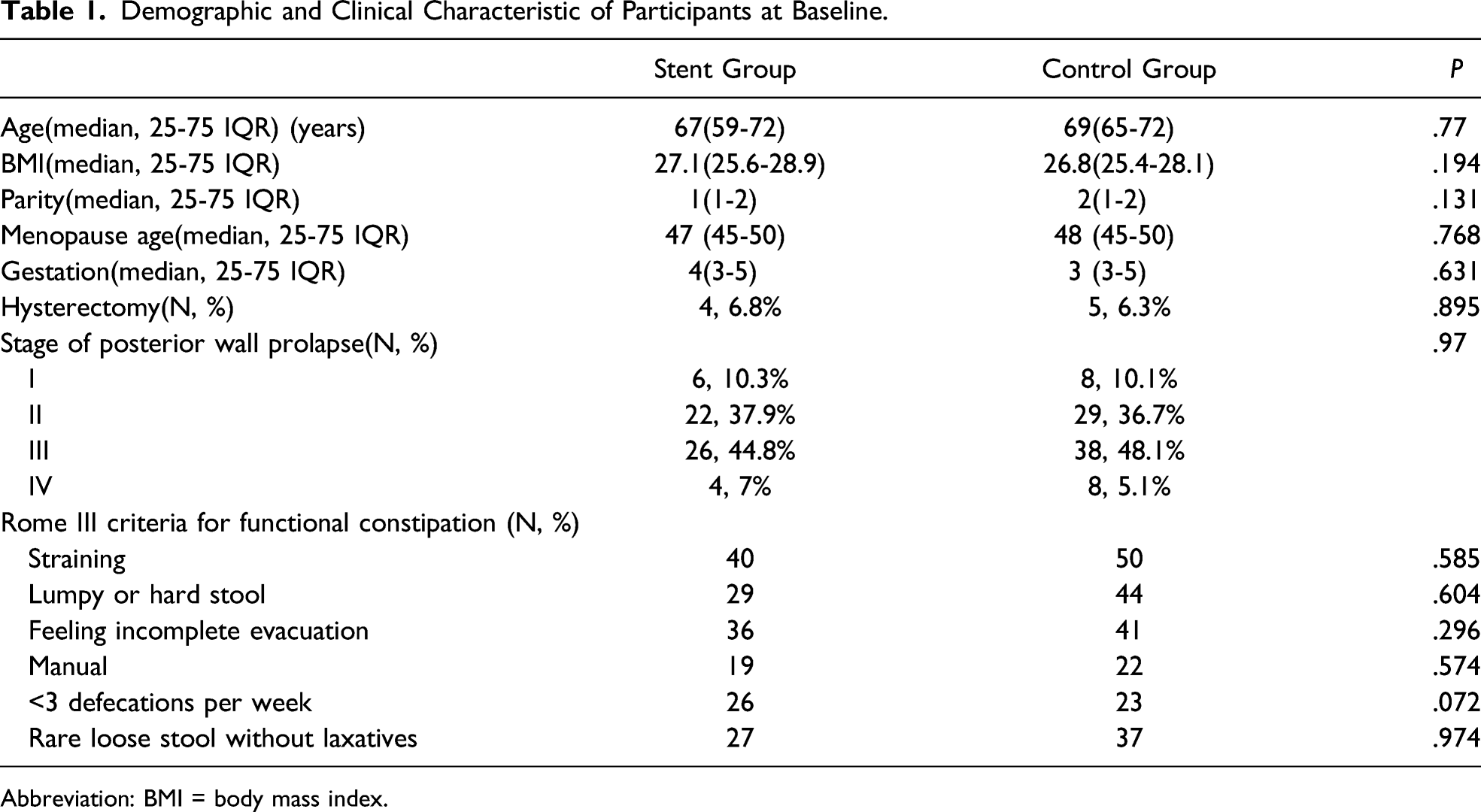
Of the 156 participants at baseline, 137 participants completed the follow-up questionnaire, with a follow-up rate of 87.8% (Figure 2). The demographic data were showed in Table 1. There were no differences between the 2 groups regarding age, body mass index (BMI), gestation, parity, and age of menopause using Mann-Whitney U test. There were also no differences between the 2 groups regarding stage of posterior wall prolapse using the Wilcoxon rank sum test. Additionally, the symptoms of rectocele and the history of hysterectomy had no differences between the 2 groups using the chi-square test. Patients and randomization. Female rectocele patients (n = 156) underwent randomization. Finally, patients in the stent group (n = 59) and in the control group (n = 79) were analyzed. Demographic and Clinical Characteristic of Participants at Baseline. Abbreviation: BMI = body mass index.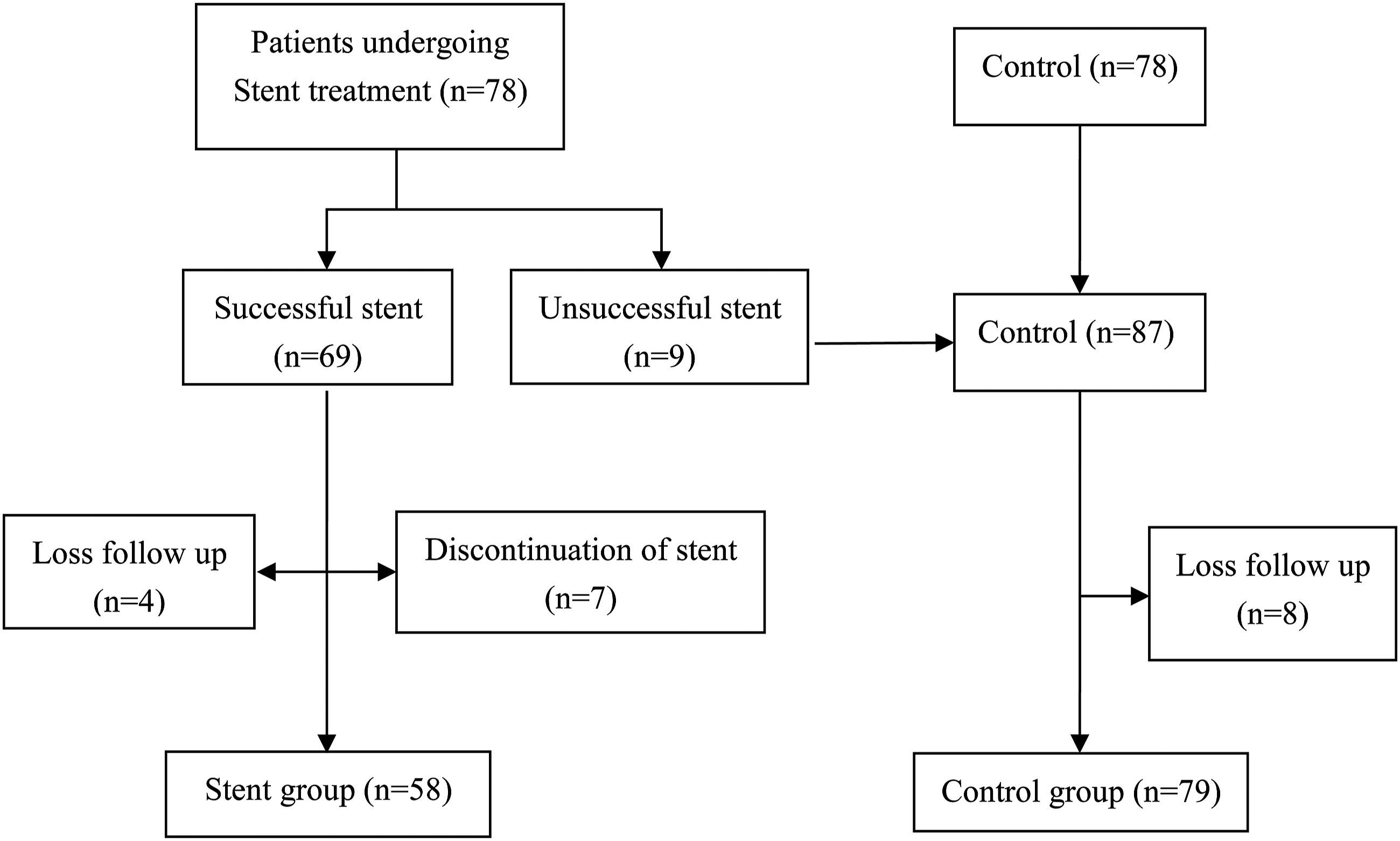
ODS Score
Changes in the Total ODS Score and Score of Each Item at Baseline, 1 Month Follow-Up, and 6 Month Follow-Up.
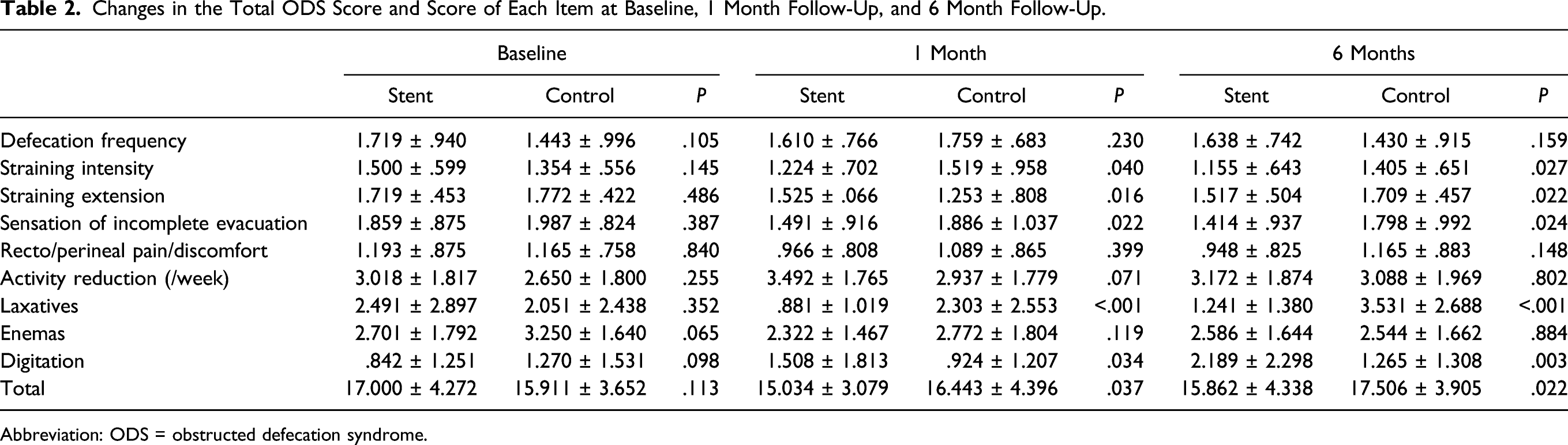
Abbreviation: ODS = obstructed defecation syndrome.
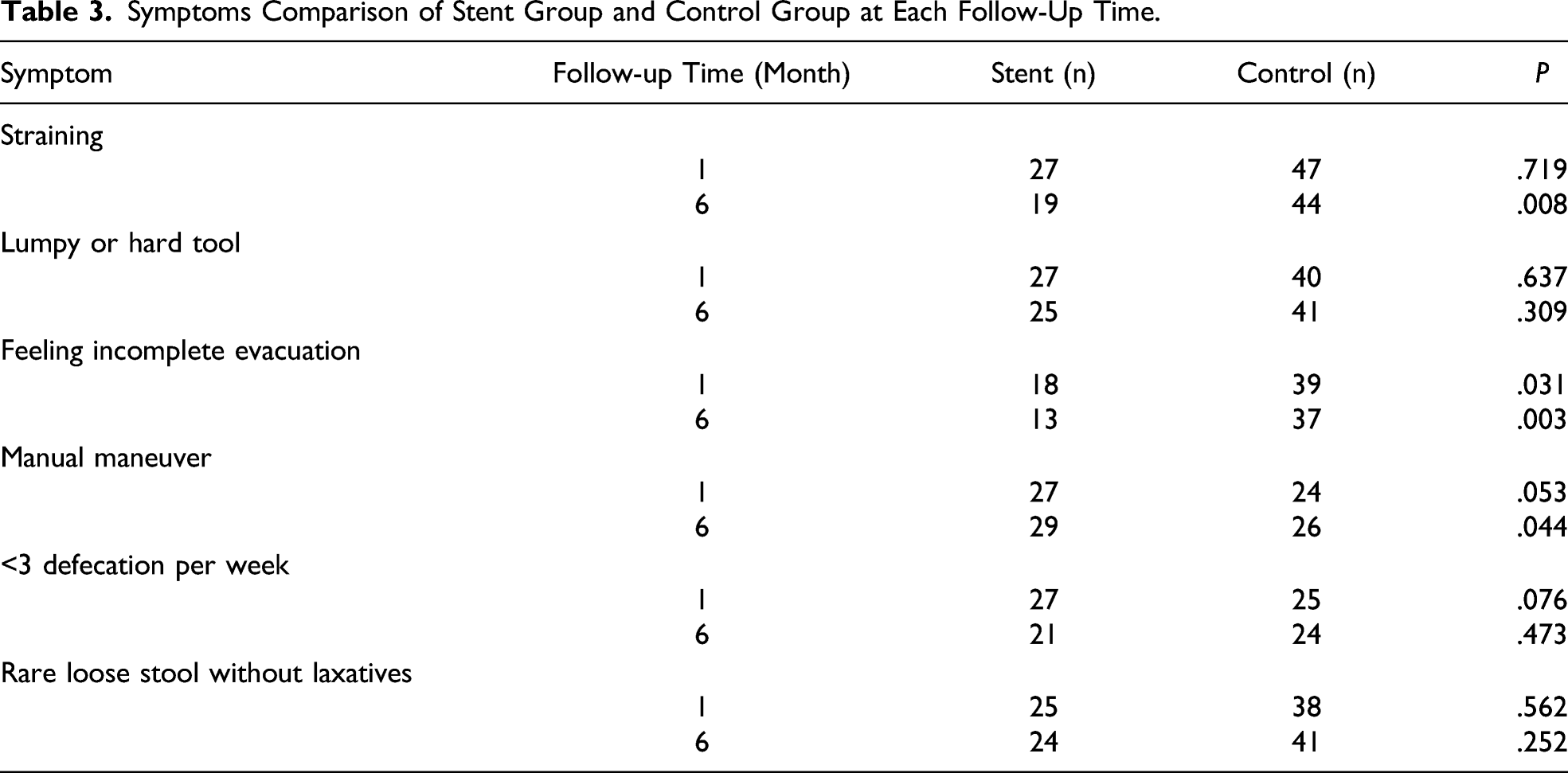
Symptoms Comparison of Stent Group and Control Group at Each Follow-Up Time
Symptoms Comparison of Stent Group and Control Group at Each Follow-Up Time.
Anorectal Pressure
Anorectal Pressure at Each Follow-Up Time.
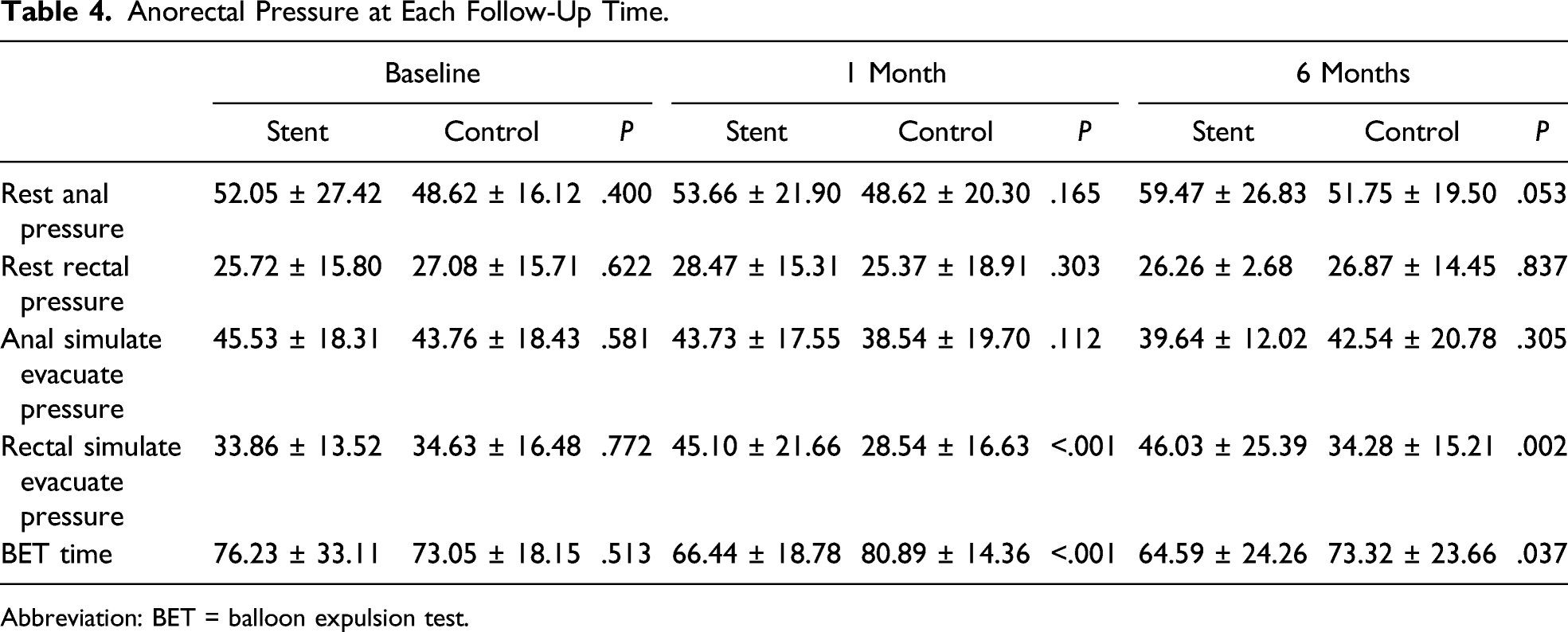
Abbreviation: BET = balloon expulsion test.
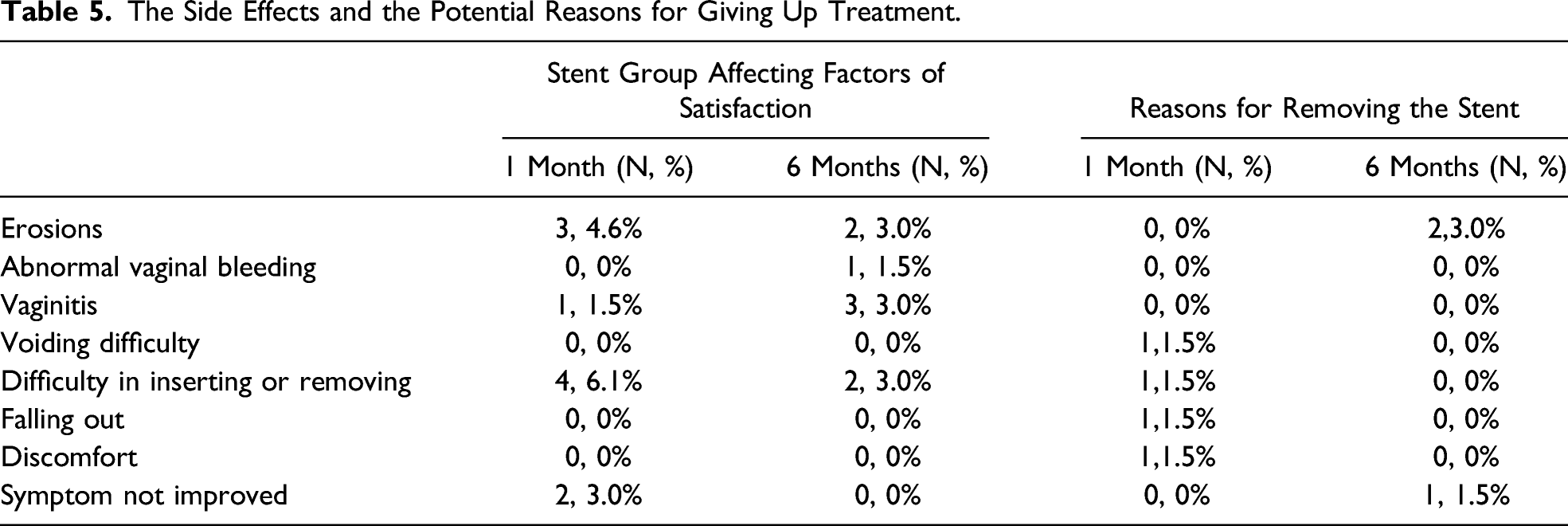
The Side Effects and Potential Reasons for Giving Up Treatment
The Side Effects and the Potential Reasons for Giving Up Treatment.
Discussion
Outlet obstructive constipation is a common manifestation of rectocele. Patients with rectocele often suffer from painful defecation, bleeding, prolonged defecation time, incomplete defecation, and other symptoms because of rectovaginal fascia injury and pelvic floor muscle dysfunction.19,20 In our study, we have found that vaginal stent shortens the straining extensity time, alleviates the symptoms of incomplete evacuation, and decreases the straining intensity and the use of laxatives. The vaginal stent increases the rectal pressure and shortens the balloon expulsion time by reinforcing the uterosacral ligament-rectovaginal fascia-perineal complex. Vaginal stent provides a promising and alternative treatment for rectocele with outlet obstructive constipation.
Many other studies have evaluated the clinical improvement of rectal outlet obstructive constipation through ODS scoring. For example, Hicks et al have found that the biofeedback reduces ODS scores and improves the symptoms of defecation difficulties in patients. 21 Ribaric et al have found that reducing ODS score improves the quality of life after stapled transanal rectal resection. 22 Similarly, in this study, the use of vaginal stent decreases ODS score and effectively improves the symptoms of outlet obstructive constipation, which provides a conservative treatment for elderly patients or patients with serious medical complications. We have also found the increase in the score of digitation and the number of manual maneuver, suggesting that more patients may use the handle function of the stent, in order to resist the force of rectum hernia to the vagina during defecation, thereby improving the symptoms of obstructive dysfunction of defecation. A surgical treatment that improves the symptoms by implanting a mesh into the vaginal rectal space was using the same principle. When compared with the surgical method, the vaginal stent method is safer and achieves the same effect. This method is used for preoperative experimental diagnosis. If the outlet defecation of the patient difficultly improves after stent inserting, the surgical method is considered to improve the satisfaction after operation.
We have compared the anorectal manometry between the stent treatment group and the control group. The results have shown that the rectal pressure in the condition of simulated evacuation is increased in the stent. In the rectal BET, the time of balloon expulsion was shortened. There is no significant difference in other indicators. These results suggest that vaginal stent placement may increase the rectal pressure and shorten the defecation time by inhibiting rectum hernia to the vagina and reducing the lateral force from the rectum to the vagina, which is in line with Luo’s view. 23 The inadequate pushing force is an important reason for obstructed defecation by the method of anorectal manometry. 24 David et al have concluded that patients with rectocele usually have more abnormal rectal BET time, lower median rectal pressure, and more negative median rectoanal gradient. 16 These all consist of the view of our study.
Since the vaginal stent is alike with the pessary, the side effect is similar to some extent. The symptoms are classified into erosion, bleeding, inflammation, voiding difficulties, difficulty in inserting or removing the stent, stent falling out, discomfort, and nonimproving symptoms, which are also found in a previous study. 25 Bai et al reported that 76(73.1%) patients have complications such as bleeding, erosion, or foul odor when using pessary. 26 Differently, in our study, we have found that only 14(21.5%) patients have complications in 1 month follow-up and 15(23.1%) in 6 months follow-up. Previous literature suggests that erosions may be the most common complication, no matter in the stent group or in the control group. 27 We have found that the erosions are not serious. There are 3 persons who have erosions in the stent group in 1 month follow-up with the continuous use of the stent. After vaginal estrogen cream treatment, the erosions have cured 1 month later. Another 2 patients encounter the erosion in the stent group in the 6 months follow-up and cure in the same method. Only 1 patient gave up the stent treatment because of worrying about the erosions. In our study, the difficulty in inserting or removing the stent has also high incidence. 6% in 1 month follow-up, 3% in 6 months follow-up, and 1.5% patients gave up treatment because of this reason. We conclude that the shape of the inverted trapezoid structure of the stent may be the main reason.
The innovative point of this study is that the vaginal stent is independently designed by the research team. The effect of the stent is similar to the pessary, which improves the symptoms of outlet obstructive constipation while relieving the rectocele. Yamada et al have conducted a study on the pessary effect on the outlet obstructive constipation. 28 They have found that the therapeutic effect is unsatisfactory because the ring pessary cannot reinforce rectovaginal fascia. In this study, the vaginal stent we designed is an inverted trapezoidal structure, and a removable handle better reinforces the uterosacral ligament-rectovaginal fascia-perineal complex and improves the symptoms of outlet obstructive constipation. The limitation of this study is that although the design of the handle can facilitate the patient to provide a backward force during defecation, it also increases the probability of manual assistant defecation, which may make some users feel less convenient. We may try to improve it in the future. In addition, the inverted trapezoidal stent structure may cause some difficulties in patients’ self-placement of stent, but this structure has important significance in reinforcing effects. Therefore, in future studies, we may explore some more flexible materials to improve the vaginal stent.
In summary, vaginal stent placement can reinforce rectovaginal fascia, increase rectal pressure during defecation, reduce defecation time, reduce ODS score, and improve quality of life, which provides an effective treatment for female patients with rectocele.
Footnotes
Author Contributions
Study concept and design: Yitong Yin, Zhijun Xia
Acquisition of data: Yitong Yin, Meng Luan
Analysis and interpretation: Meiying Qin
Study supervision: Zhijun Xia
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The National Ministry of Science and Technology of China provided financial support for this research, Project Number: 2014BAI05B02. Special project on Transformation of medical scientific and technological achievements of Liaoning Province. Project Number:1553067953705.