
Abstract
Background. While advanced practice providers (APPs) are increasingly integrated into care delivery models, little is known about their impact in surgical settings. Given that many patients undergo surgery in multispecialty group practice settings, we examined the impact of APP integration into such practices on outcomes after major surgery. Methods. We used a 20% sample of national Medicare claims to identify 190 101 patients who underwent 1 of 4 major surgeries (coronary artery bypass graft [CABG], colectomy, major joint replacement, and cystectomy) at multispecialty group practices from 2010 through 2016. The level of APP integration was measured as the ratio of APPs to physicians within each practice. Rates of mortality, major complications, and readmission within 30 days of discharge after the index surgery were compared between patients treated in practices with low, medium, and high levels of APP integration using multivariable regression analysis. Results. Relative to patients treated in practices with low APP integration, those treated in practices with medium or high APP integration had significantly lower rates of mortality (2.4% [low integration] vs 1.9% [medium integration] vs 2.0% [high integration]; P < .01), major complications (34.1% [low] vs 31.2% [medium] vs 30.2% [high]; P < .01), and readmission (11.7% [low] vs 10.6% [medium] vs 10.1% [high]; P < .01). This relationship was consistent for virtually all outcomes when considering each surgery type individually. Conclusions. Integration of APPs into multispecialty group practices was associated with improved postoperative outcomes after major surgery. Future research should identify the mechanisms by which APPs improve outcomes to inform optimal utilization.
Introduction
Physician assistants and nurse practitioners have become integral members of the country’s healthcare delivery system, accounting for approximately 20% of the American healthcare workforce. 1 Initially established to address the shortage of primary care physicians, the two professions, collectively known as advanced practice providers (APPs), are increasingly integrated into virtually all domains of patient care in efforts to expand delivery system capacity. In 2016, APPs were embedded into 1 in 3 primary care practices and 1 in 4 specialty practices in the United States, including surgical specialties. 2
Despite the increasing presence of APPs in surgical care, 2 relatively little is known about their impact on surgical outcomes. Most studies on the subject have focused thus far on relatively minor procedures performed within single centers.3-6 Evidence from nonsurgical settings suggests that APPs may facilitate the delivery of care through enhanced care coordination and communication and by providing coverage in light of resident duty hour restrictions. 7 Task sharing may allow physicians to focus on patients with complex needs where advanced training may have a larger marginal impact on health outcomes. 6 Moreover, multispecialty practices may be uniquely positioned to realize the potential benefits of APP integration given their access to quality improvement support, familiarity with multidisciplinary work, and payment incentives.8-10 However, with the shorter training period and core generalist education of APPs, 7 it is unclear if the generally favorable impact of APP integration in primary care settings translates into surgical settings.
Given many patients undergoing surgery do so in the context of multispecialty practices and the potentially different impact of APP integration across practice settings, we sought to evaluate the impact of APP integration on outcomes of patients undergoing major surgery in multispecialty practices. Using the staffing ratio of APP to physicians within multispecialty practices as exposure, we examined the relationship between levels of APP integration within practices and postoperative mortality, major complications, and readmissions of a national sample of Medicare beneficiaries.
Methods
Data Sources and Study Population
We used a 20% sample of national Medicare claims to perform a retrospective cohort study of fee-for-service beneficiaries who underwent 1 of 4 major surgeries (coronary artery bypass graft [CABG], colectomy, major joint [hip or knee] replacement, or cystectomy) from 2010 through 2016. These surgeries were chosen to reflect procedures that are common among older patients or are associated with high rates of mortality or major complications.
We searched for Healthcare Common Procedure Coding System codes within the Medicare Part B claims to identify patients aged 66 and older who had undergone 1 of the 4 surgeries of interest. We then linked these patients with the corresponding hospitalizations based on data from the Medicare Provider Analysis and Review file. Only patients with continuous enrollment in Medicare Parts A and B from 1 year before each procedure through 30 days after discharge, or until death, were included. Patients participating in Medicare managed care plans were excluded due to the absence of complete claims.
We limited our study population to patients who underwent surgery at multispecialty group practices using established methods. 11 Briefly, we first associated the surgeons who performed the surgery with their corresponding group practices through their tax identification number based on data from the Medicare Data on Provider Practice and Specialty (MD-PPAS) file from the Centers for Medicare & Medicaid Services. 12 We then considered practices as multispecialty if the practices included at least one primary care physician (based on specialty codes in the MD-PPAS file) and were not dominated by specialists associated with a single procedure. Multispecialty group practices were further identified as hospital-integrated or not hospital-integrated based on the frequencies of place of service codes, which reflect the entity at which services were rendered. 13
Measuring APP Integration
The involvement of APPs in patient care cannot be reliably ascertained using claims data because their services may be billed under a physician’s national provider identifier. 14 Furthermore, there is no direct way to assess the clinical specialty of APPs, and APPs may contribute to care delivery by providing non-billable services. Thus, instead of relying on incomplete claims–based characterization, we used a practice-level staffing ratio as an estimate of APP integration as the exposure variable. This approach is similar to that of Needleman et al. 15 who used the nurse to hospital bed ratio as the exposure variable in examining the association between staffing and quality of care. First, we identified the number of APPs and physicians within each multispecialty practice. Then, we divided the number of all APPs within each practice by the number of all physicians within said practice to create a staffing ratio. In theory, a higher APP to physician ratio would correlate with more contributions from APPs and more interaction between APPs, physicians, and patients.
To facilitate comparisons, practices were stratified into tertiles by levels of APP integration (Supplementary Material Table 1). First, we ranked all practices by their APP to physician ratio in ascending order. Then, we selected cutoffs for low, medium, and high levels of APP integration that most closely divide the practices into three groups of equal sizes (due to ties, there was some deviation). We developed separate cutoffs for both the overall cohort and for each individual surgery type. For instance, when analyzing all surgery types together, cutoffs for the tertiles of APP integration were practices with 0 to 1 APPs per 10 physicians (“low”), >1 to 3 APPs per 10 physicians (“medium”), and >3 APPs per 10 physicians (“high”).
Outcomes
For all outcome measures, we used the patient as the unit of analysis. We measured 3 outcomes occurring within 30 days of discharge after the index surgery: mortality, major complications, and readmissions. Major complications were identified using a composite measure based on the occurrence of at least one Agency for Healthcare Research and Quality patient safety indicator. 16
Analysis
We tested whether patient- and practice-level characteristics varied by tertile of APP integration using linear regression for continuous variables and the Mantel–Haenszel chi-square test for categorical variables. We fit multivariable logistic regression models inclusive of all surgery types to characterize relationships between postoperative outcomes and levels of APP integration while adjusting for patient age, race, comorbidity, 17 socioeconomic status at the zip code level, 18 case volume, hospital integration, and surgery type. From these models, we backed out adjusted predicted probabilities of mortality, major complications, and readmission at different levels of APP integration. Because relationships might vary by surgery type, we included an interaction term between levels of APP integration and surgery type. This interaction term was statistically significant, providing rationales for further stratified analysis by surgery type. Thus, we fit a second set of multivariable logistic regression models and derived predicted probabilities for postoperative outcomes for each surgery type. All analyses were performed using SAS 9.4 (Cary, NC), at the 5% significance level. This study used de-identified claims data and was deemed exempt from review by the institutional review board.
Results
Patient and Practice Characteristics Across Multispecialty Group Practices With Low, Medium, and High Levels of APP Integration.
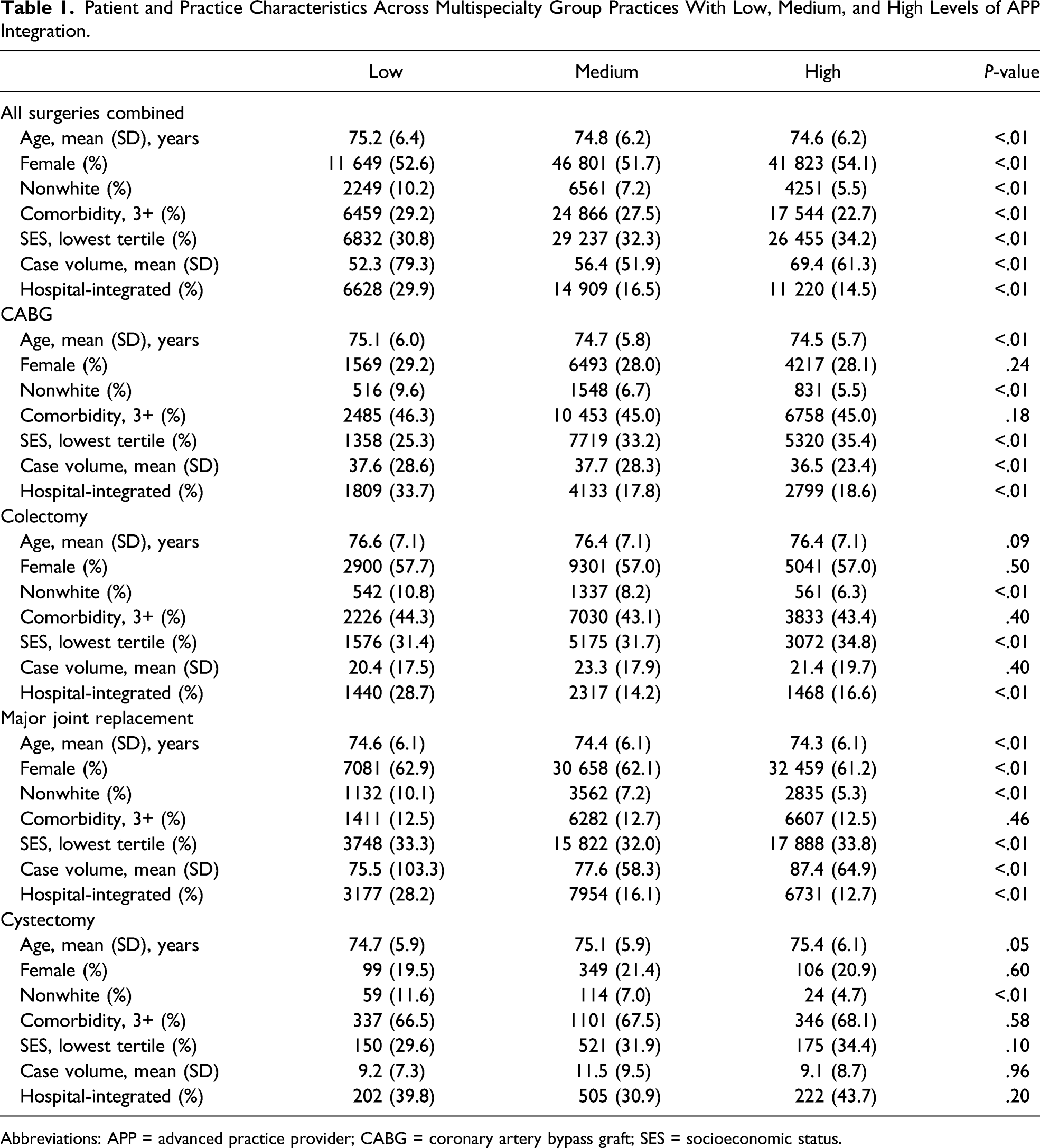
Abbreviations: APP = advanced practice provider; CABG = coronary artery bypass graft; SES = socioeconomic status.
Figure 1 illustrates the predicted postoperative outcomes of the entire cohort by the levels of APP integration of practices in which patients were treated. Patients treated in practices with low levels of APP integration had higher rates of mortality than patients treated in practices with medium or high levels of APP integration (2.4% [low] vs 1.9% [medium] and 2.0% [high]; P < .01). The same trend was found for rates of major complications (34.2% [low] vs 31.2% [medium] and 30.2% [high]; P < .01) and for rates of readmission (11.7% [low] vs 10.6% [medium] and 10.1% [high]; P < .01). Caption: Outcomes within 30 days of discharge after index surgery (CABG, colectomy, major joint replacement, and cystectomy considered together), by levels of APP integration of practices at which the surgery was performed. Description: With increasing tertiles of APP integration from low to medium to high, mortality rate ranged from 2.4% to 1.9% and 2.0% (P < .01). Major complication rate decreased from 34.1% to 31.2% and 30.2% (P < .01). Readmission rate decreased from 11.7% to 10.6% and 10.1% (P < .01). APP = advanced practice providers; CABG = coronary artery bypass graft.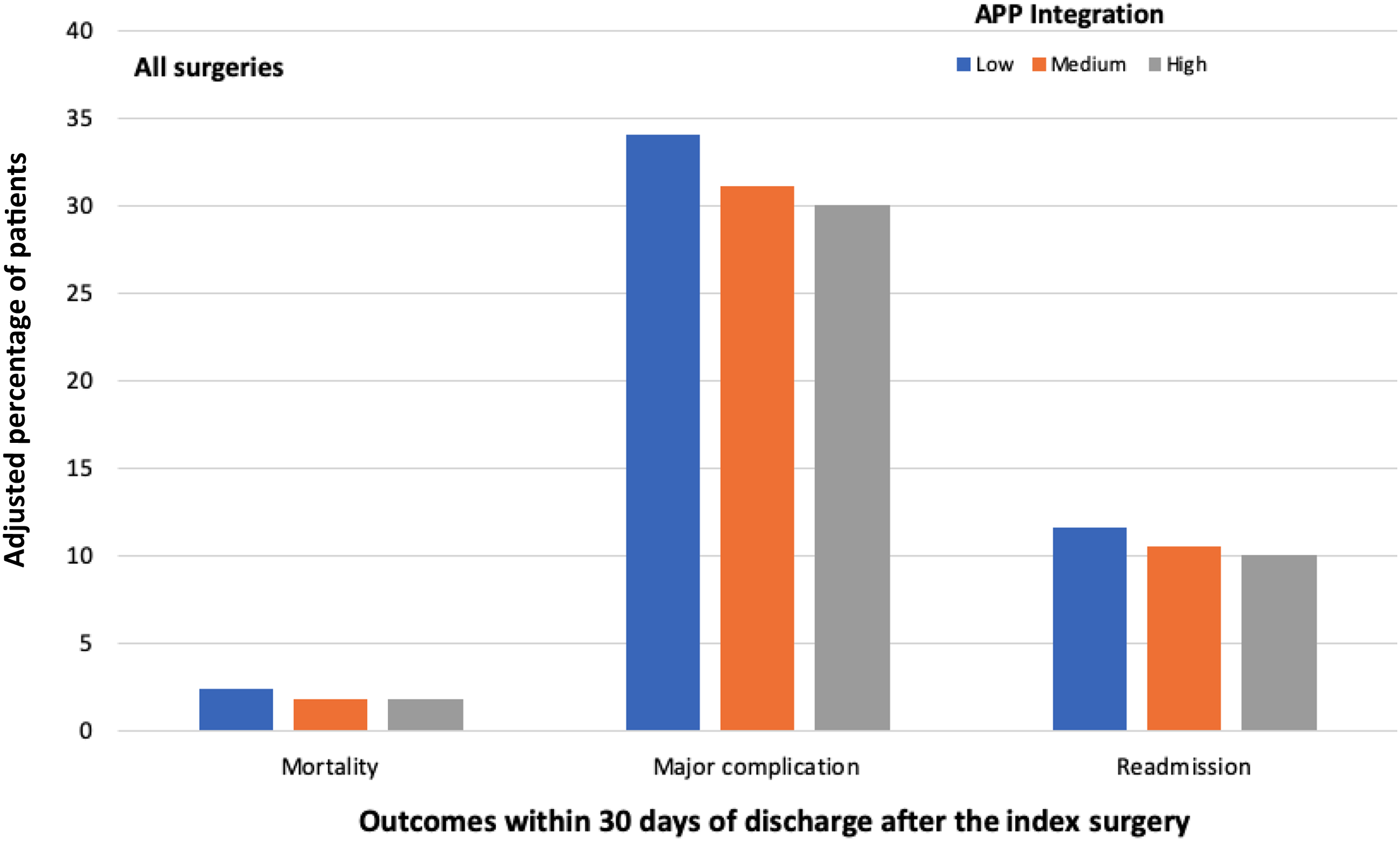
Figures 2A-D demonstrate the predicted postoperative outcomes by levels of APP integration for each surgery type. Consistent with the trend observed when considering all procedures together, patients who underwent surgery at practices with medium or high levels of APP integration virtually all had improved postoperative outcomes, compared with patients who underwent surgery at practices with low levels APP integration. For example, patients who underwent CAGB in practices with low levels of APP integration had a mortality rate of 3.9%, whereas patients who underwent CABG in practices with medium or low levels of APP integration had a mortality rate of 3.3% and 3.5%, respectively (P < .01). One notable exception to the trend was the rate of major complications for patients who underwent cystectomy, where patients treated in practices with low levels of APP integration had lower rates of major complications (38.3%) compared with those treated in practices with medium or high levels of APP integration (44.8% and 42.4%, respectively; P < .01) (Figure 2D). Caption: Outcomes within 30 days of discharge after CABG (A), colectomy (B), major joint replacement (C), and cystectomy (D), by levels of APP integration of practices at which the surgery was performed. Description: (A) With increasing tertiles of APP integration from low to medium to high, mortality rate ranged from 3.9% to 3.3% and 3.5% (P < .01). Major complication rate ranged from 41.2% to 37.9% and 39.1% (P < .01). Readmission rate ranged from 12.5% to 11.2% and 11.3% (P < .01). (B) With increasing tertiles of APP integration from low to medium to high, mortality rate ranged from 8.0% to 6.2% and 6.3%. Major complication rate ranged from 49.6% to 46.0% and 46.4% (P < .01). Readmission rate ranged from 11.5% to 11.6% and 11.4% (P < .01). (C) With increasing tertiles of APP integration from low to medium to high, mortality rate remained stable at .2% to .2% and .2% (P < .01). Major complication rate decreased from 8.5% to 7.3% and 7.1% (P < .01). Readmission rate decreased from 5.1% to 4.4% and 4.3% (P < .01). (D) With increasing tertiles of APP integration from low to medium to high, mortality rate ranged from 3.1% to 1.9% and 2.4% (P < .01). Major complication rate ranged from 38.3% to 44.8% and 42.4% (P < .01). Readmission rate decreased from 21.8% to 19.8% and 19.6% (P < .01). APP = advanced practice providers; CABG = coronary artery bypass graft.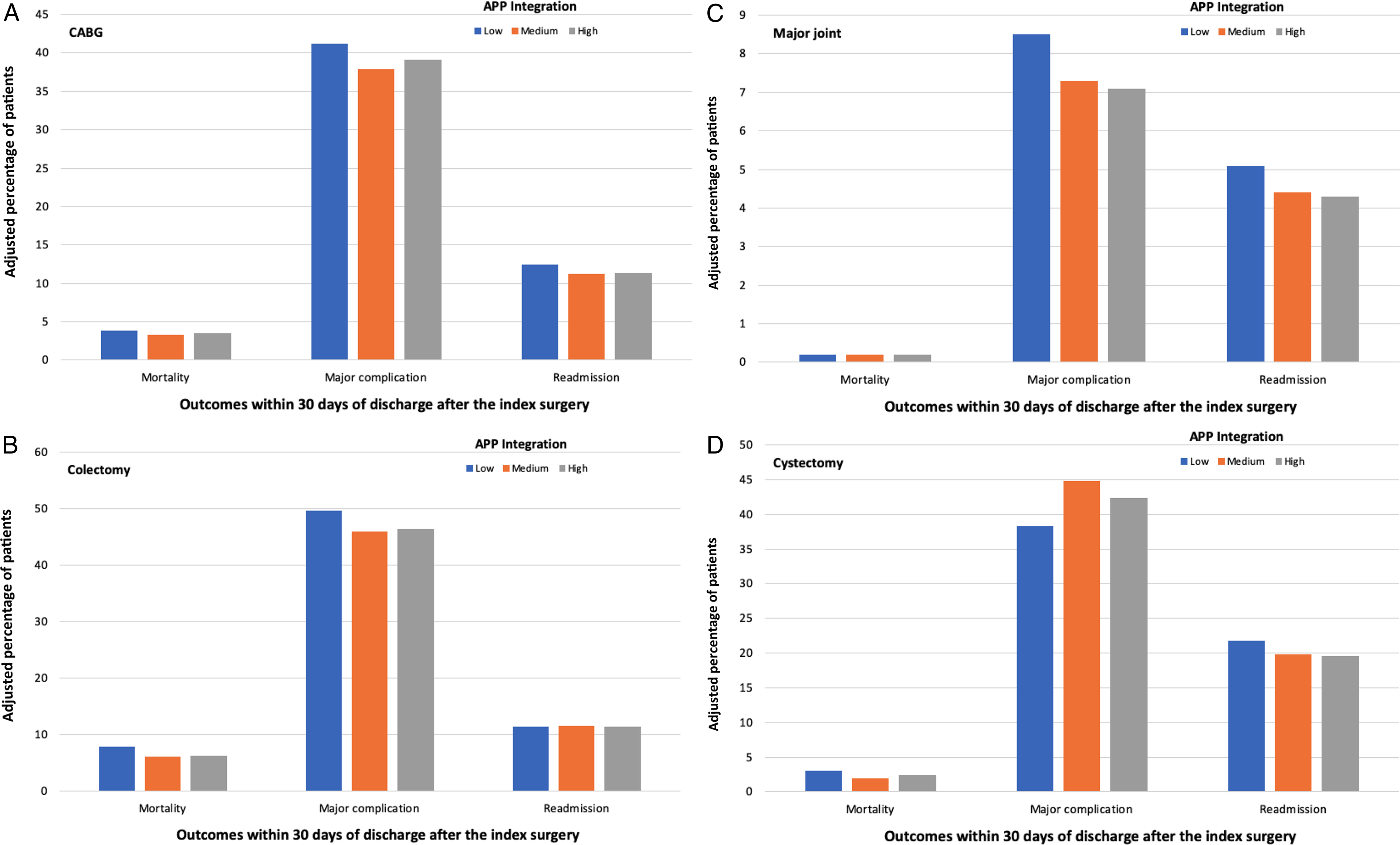
Discussion
Using the staffing ratio as a proxy for APP integration within a practice, we demonstrated that the level of APP integration was associated with postoperative outcomes among Medicare beneficiaries who underwent major surgery in multispecialty group practices. Patients who underwent surgery in practices with medium or high levels of APP integration had lower rates of mortality, major complications, and readmission than those treated in practices with low levels of APP integration. While the contribution to care by APPs cannot be fully captured by a single ratio, the findings from the current study lend support to the value of integrating APPs into multispecialty group practices for improving surgical outcomes.
Our findings add to the existing literature reporting the beneficial effect of APP involvement in surgical care. In a national survey of pediatric surgeons, nearly all respondents endorsed that integration of APPs in inpatient and outpatient settings positively impacted care, particularly with regard to continuity of care, efficiency of service, education of parents and patients, and patient satisfaction. 19 Single-center studies have shown that APPs can safely perform a range of procedures that were previously performed exclusively by physicians, such as thoracostomy insertion, 3 upper endoscopy, 4 and newborn circumcision. 5 In the immediate postoperative period, increased presence of APPs may help with early recognition of patients at risk of clinical deterioration and promote timely escalation of care.20,21 It is conceivable that streamlining the provision of care with help from APPs allows physicians to tend to more patients in a timely manner, which then translates into reduced rates of mortality, major complications, and readmission rates after major surgery.
Although increasing levels of APP integration were consistently associated with improved postoperative outcomes in the overall cohort, findings in the setting of specific surgery types were more nuanced. For example, with the exception of major joint replacement, increasing APP integration from medium to high levels was not consistently associated with further incremental improvements in outcomes. This may occur because increasing APP integration beyond a certain threshold affects the quality of care due to reduced supervision or collaboration with their physician counterparts. Moreover, some outcomes were worse among practices with higher levels of APP integration. Most notably, the rate of major complications was significantly higher among patients who underwent cystectomy at practices with medium or high levels of APP integration, compared with those treated in practices with low levels of APP integration. The clinical explanation for this finding is not obvious and perhaps reflects differences in how APPs interact or function in specific surgical contexts. However, it could also represent a chance finding, and indeed, mortality and readmission rates were lower for patients who underwent cystectomy at practices with medium or high levels of APP integration, consistent with the general trend of improved outcomes with increasing APP integration.
This study has several limitations. First, the integration of APPs into the care of surgical patients was not directly measured but rather inferred through the staffing ratio of APPs to physicians within the group practice. This approach allows for substantial heterogeneity in how APPs were utilized and the degree to which they interacted with surgical patients, across practices. However, such heterogeneity would tend to bias to the null, such that the consistent finding of benefit associated with APP integration that we observed may in fact be conservative in magnitude. 15 Nevertheless, future qualitative studies that more directly assess interactions between APPs, physicians, and patients are needed to verify the findings of the present study. Second, we grouped physician assistants and nurse practitioners together as one entity to present broad trends, possibly conflating potential differences in the impact of the two professions together. Although this might be the case, physician assistants and nurse practitioners offer many of the same services across a variety of settings. 22 Third, our results may be vulnerable to issues of patient selection. For example, there was an uneven distribution of patients with three or more comorbidities across levels of APP integration within practices. However, we adjusted for comorbidity in our regression analyses for the overall trend and within surgery-specific cohorts. Moreover, the distribution of patients with three or more comorbidities was not statistically or clinically different when stratified by surgery type.
Conclusion
In this study of Medicare beneficiaries who underwent major surgery at multispecialty group practices, patients treated in practices with medium or high levels of APP integration generally had improved postoperative outcomes compared with those treated in practices with low levels of APP integration. Our results provide evidence in support of integration of APPs in surgical settings. Additional research should identify the mechanisms by which APP involvement improve outcomes. Mixed methods studies may further clarify the opportunities and challenges that APPs encounter when caring for surgical patients and inform the optimal strategies for integrating APPs into surgical settings.
Supplemental Material
sj-pdf-1-sri-10.1177_15533506211013150 – Supplemental Material for Impact of Advanced Practice Provider Integration into Multispecialty Group Practices on Outcomes Following Major Surgery
Supplemental Material, sj-pdf-1-sri-10.1177_15533506211013150 for Impact of Advanced Practice Provider Integration into Multispecialty Group Practices on Outcomes Following Major Surgery by Lillian Y. Lai, Samuel R. Kaufman, Parth K. Modi, Chad Ellimoottil, Mary Oerline, Megan E.V. Caram, Brent K. Hollenbeck and Vahakn B. Shahinian in Surgical Innovation
Footnotes
Author Contributions
Study concept and design: Lillian Y. Lai, Brent K. Hollenbeck, and Vahakn B. Shahinian.
Acquisition of data: Samuel R. Kaufman, Brent K. Hollenbeck, and Vahakn B. Shahinian.
Analysis and interpretation: Lillian Y. Lai, Samuel R. Kaufman, Parth K. Modi, Chad Ellimoottil, Mary Oerline, Megan E.V. Caram, Brent K. Hollenbeck, and Vahakn B. Shahinian.
Study supervision: Brent K. Hollenbeck and Vahakn B. Shahinian.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by research funding from the National Institute on Aging (R01 AG-048071) to Brent K. Hollenbeck. Lillian Y Lai is supported by funding from the National Cancer Institute (T32CA180984). The views expressed in this article are those of the authors and do not necessarily reflect the position or policy of the United States government.
Ethical Approval
This study used de-identified claims data and was deemed exempt from review by the institutional review board.
Supplementray material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.