
Abstract
Background
Low-grade lesions may benefit from pancreatic-sparing techniques. Resection of the uncinate process is rarely performed and reported due to its complexity that requires careful patient selection and accurate knowledge of the pancreatic anatomy. This study describes relevant anatomical elements to safely perform this complex operation in the minimally invasive setting.
Methods
In this study, consecutive patients undergoing resection of the uncinate process of the pancreas were studied. Patients undergoing open approach were used for comparison. Preoperative and intraoperative variables were recorded, and the diagnosis and tumor size were determined from the pathology reports. Immediate postoperative results and hospital stay were analyzed. Follow-up was used to assess long-term complications and endocrine and exocrine functions.
Results
Twenty-nine patients underwent resection of the uncinate process. The median age was 57 years. There were 21 males and eight females. Twenty patients underwent minimally invasive resection (14 laparoscopic and six by robotic approach) and nine were operated by open approach. A clinically relevant postoperative pancreatic fistula was observed in one patient (3.4%). Biochemical leakage was present in 44.8% of our patients. Mean follow-up was 62 months (3–147). Two patients needed reoperation during follow-up. No patient presented exocrine or endocrine insufficiency during late follow-up.
Conclusion
Minimally invasive resection of the uncinate process of the pancreas is a complex but a feasible procedure that preserves the pancreatic endocrine and exocrine functions. This pancreas-sparing procedure is an interesting alternative to pancreaticoduodenectomy in selected patients.
Introduction
Pancreatoduodenectomy is the treatment of choice for tumors arising in the head of the pancreas and in the periampullary area. 1 However, some low-grade neoplasms may benefit from pancreatic-sparing techniques such as enucleation and isolated resection of the uncinate process of the pancreas.2,3 This latter technique, although described originally in 1996, is rarely performed and reported, mainly due to the complexity of this procedure, requiring careful patient selection and accurate knowledge of the pancreatic anatomy.3-11
The precise knowledge of the anatomy of the uncinate process of the pancreas is essential to understand and to perform this pancreas-sparing procedure. The limits of the uncinate process lack specific anatomical landmarks on its superior border representing the Achilles heel of this technique. Failure on the correct identification of this limit can be hazardous, leading to main pancreatic duct injury.
With the introduction of minimally invasive techniques, this procedure has been performed by laparoscopic and robotic approach.6,11 The aim of the article is to point out the relevant anatomical elements to safely perform this complex operation in the minimally invasive setting. We describe our laparoscopic and robotic technique for the uncinate process resection, highlighting the main steps and surgical results. A comparison with the open counterpart is presented.
Methods
Study Design and Setting
All patients undergoing pancreatic resection at our institution are recorded in a database prospectively maintained. In this study, consecutive patients undergoing minimally invasive and open resection of the uncinate process of the pancreas between January 2008 and December 2019 were studied. Preoperative variables analyzed were age, sex, and surgical indication; intraoperative variables collected were operative time, bleeding, and blood transfusion. Immediate postoperative results such as morbidity and hospital stay were also recorded. Pancreatic fistula was assessed and graded according to the International Study Group on Pancreatic Fistula recommendations. The diagnosis, tumor size, and margin status were determined from the final pathology reports. Pancreatic endocrine and exocrine functions in the postoperative period were assessed during late follow-up.
Preoperative Assessment and Surgical Indication
A variety of imaging modalities were used for assessing pancreatic lesions including ultrasonography (US), computed tomography (CT), magnetic resonance imaging, and endoscopic ultrasound (EUS). The use of relevant clinical information and key radiologic features were essential for adequate lesion characterization/differentiation and thus surgical planning. Preoperative workup included MR and EUS for most patients.
Isolated uncinate process resection was only performed in patients with low-grade pancreatic neoplasms. The criteria for resection of intraductal papillary mucinous neoplasms (IPMNs) were based on the current Fukuoka guidelines for management of such neoplasms 12 . Superficial neuroendocrine tumors (NETs) with a safe distance from the pancreatic duct were treated with enucleation and were not included in the present study. Deep located NET and/or those close to the uncinate process pancreatic duct (less than 2 mm) were treated with resection.2,13
Surgical Technique
Knowledge of the anatomy of the uncinate process is key to performing this complex operation. The real anatomy will eventually derive from the preoperative workup studies and some variations may be present. The most important variation is the presence of a pancreas divisum, which if present facilitates the procedure. The relationship of the pancreatic lesion to the main pancreatic duct offers important clues about the procedure. Intraoperative ultrasound was used in all cases to locate the tumor and to assess the distance from the line of parenchymal transection and the main pancreatic duct.
Anatomy of the Uncinate Process of the Pancreas
The uncinate process of the pancreas is merged to the dorsal pancreas, and its limits are difficult to identify especially its superior margin that maintains a close relationship with the main pancreatic duct that must be preserved (Figure 1(A)). The uncinate process has the superior mesenteric vein on its left border where the venous branches can be found. This leads to massive bleeding if the plane of dissection is inaccurate (Figure 2(A)). There is an arterial arcade in the lower and right limit formed by the inferior pancreatoduodenal artery and its tributaries anterior (AIPD) and posterior (PIPD) that are responsible for the perfusion of the duodenum and must be preserved (Figure 1(A)). This plane of dissection should preserve the IPA while controlling its arterial branches toward the uncinate process (Figure 2). In the case of pancreas divisum, the main pancreatic duct is far from the dissection plane and the isolate resection of the uncinate process is easier and safer. Schematic drawing showing the arterial anatomy of the uncinate process of the pancreas and the main steps to its anatomical resection. (A) Anatomy of the uncinate process of the pancreas. GDA, gastroduodenal artery; SMV, superior mesenteric vein; SMA, superior mesenteric artery; IPA, inferior pancreatoduodenal artery; AIPD, anterior inferior pancreatoduodenal artery; PIPD, posterior inferior pancreatoduodenal artery; J1, first jejunal artery; T, tumor. (B) Inferior part of the uncinate process is already dissected from the duodenum. Arterial and venous branches are ligated. Duodenum perfusion is preserved. (C) Superior part of the uncinate process is carefully transected. Main pancreatic duct is preserved, and the uncinate process duct is ligated (if identified). (D) Final aspect after isolated resection of the uncinate process of the pancreas. Secondary pancreatic duct from the uncinate process is ligated (arrow). Cadaveric specimen showing the anatomy of the uncinate process of the pancreas and the main steps to its anatomical resection. (A) The uncinate process of the pancreas (UP) before resection. SMV, superior mesenteric vein. (B) Inferior part of the uncinate process (UP) is being dissected from the duodenum. SMV, superior mesenteric vein; AIPD, anterior inferior pancreatoduodenal artery. (C) Inferior part of the uncinate process (UP) is already dissected from the duodenum and it is lifted. SMV, superior mesenteric vein; AIPD anterior inferior pancreatoduodenal artery. (D) Final aspect after isolated resection of the uncinate process of the pancreas. SMV, superior mesenteric vein; AIPD, anterior inferior pancreatoduodenal artery; PIPD, posterior inferior pancreatoduodenal artery.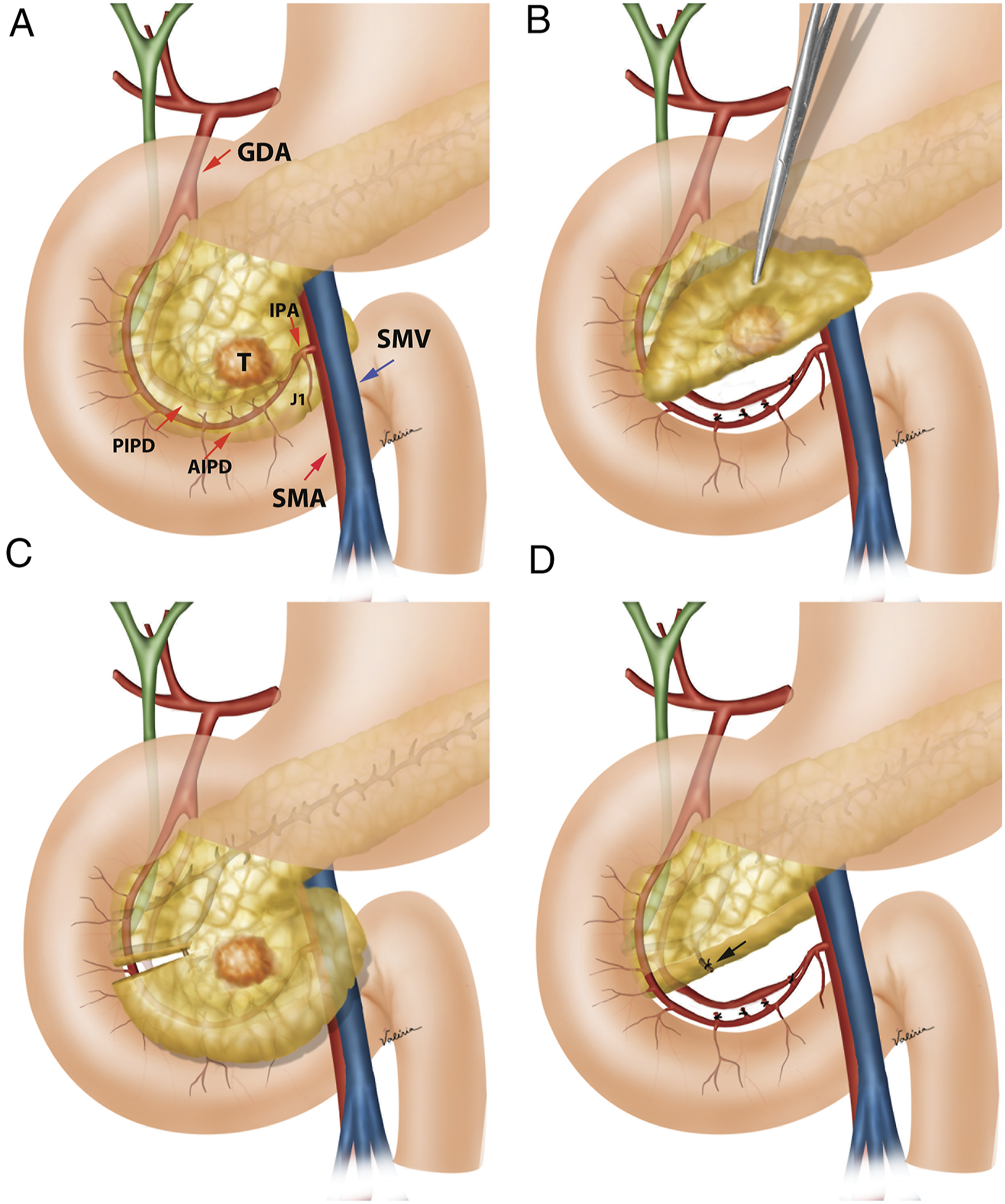

Laparoscopic Approach
The patient is placed in a supine and a reverse Trendelenburg position with the surgeon standing between patients’ legs. Four trocars—one 10 mm and three 5 mm—are used. During inspection, the inferior vena cava, transverse colon, duodenum, and pancreas are identified. A Kocher maneuver is performed with complete exposure of the pancreatic head and uncinate process. Intraoperative ultrasound is then performed to locate the tumor and to assess the main pancreatic duct. The uncinate process is dissected from the superior mesenteric vein, and the venous branches are divided between metallic clips or by use of laparoscopic coagulation shears (LCS; Ethicon Endo Surgery Industries, Cincinnati, OH, USA). Blood supply of the duodenum is preserved by ligature of small pancreatic branches from the inferior pancreatoduodenal artery (Figure 3). Transection of the pancreatic parenchyma is performed using laparoscopic coagulation shears. Hemostasis is achieved with temporary gauze compression. Surgical specimens are removed through a small extension of the infraumbilical incision inside a retrieval bag. A hemostatic absorbable tissue is placed in the raw pancreatic surface, and the abdominal cavity is drained. Isolated resection of the uncinate process of the pancreas by laparoscopic approach. (A) Intraoperative ultrasound is performed to locate the tumor and to understand the anatomy. (B) Inferior part of the uncinate process (UP) is already dissected from the duodenum and it is lifted. Duodenum perfusion is preserved. SMV, superior mesenteric vein. Superior part of the uncinate process is carefully transected. Main pancreatic duct is preserved. (C) The uncinate process is already transected. Main pancreatic duct is preserved, and the uncinate process pancreatic duct (UP branch duct) is identified and ligated. (D) Final aspect after isolated resection of the uncinate process of the pancreas. SMV, superior mesenteric vein.
Robotic Approach
The patient is placed in a supine and reverse Trendelenburg position. This robotic technique uses five ports: two 12-mm and three 8-mm trocars. After docking the robotic system, a robotic Cadiere forceps (Intuitive Surgical Inc., Sunnyvale, CA, USA) is inserted through the third robot arm with a bipolar grasper forceps on the second robot arm and a pair of ultrasonic coagulating shears inserted through the first robot arm. The plane between the right colon and the duodenum is dissected, and the right colon is removed to expose the duodenum using ultrasonic coagulating shears. The duodenum is then fully mobilized using upward traction and division of ligaments. The Kocher maneuver is carefully performed to not damage the duodenum wall. The uncinate process of the pancreas is then identified (Figure 4). Intraoperative ultrasound is then performed to locate the tumor and to assess the main pancreatic duct. The resection begins with division of small arterial branches from the inferior pancreatoduodenal artery followed by control via either bipolar forceps or ultrasonic energy of venous branches to superior mesenteric vein. Intraoperative localization of the ampulla of Vater can be performed using indocyanine green-enhanced fluorescence.
11
A combination of harmonic shears and bipolar energy is used to transect the pancreas. Pancreatic division is made under ultrasonographic guidance to avoid damage to the main pancreatic duct (Figure 4(A)). Temporary hemostasis uses gauze. Hemostatic tissue is applied to the raw pancreatic area, and the abdominal cavity is drained. Surgical specimens are retrieved through an umbilical port inside a plastic bag. Isolated resection of the uncinate process of the pancreas by robotic approach. (A) Intraoperative ultrasound is performed to locate the tumor and to understand the anatomy. (B) Inferior part of the uncinate process (UP) is partially dissected from the duodenum. Duodenum perfusion is preserved. SMV, superior mesenteric vein; AIPD, anterior inferior pancreatoduodenal artery. (C) Superior part of the uncinate process is carefully transected. Main pancreatic duct is preserved. SMV, superior mesenteric vein; AIPD, anterior inferior pancreatoduodenal artery. (D) Final aspect after isolated resection of the uncinate process of the pancreas. SMV, superior mesenteric vein; AIPD, anterior inferior pancreatoduodenal artery.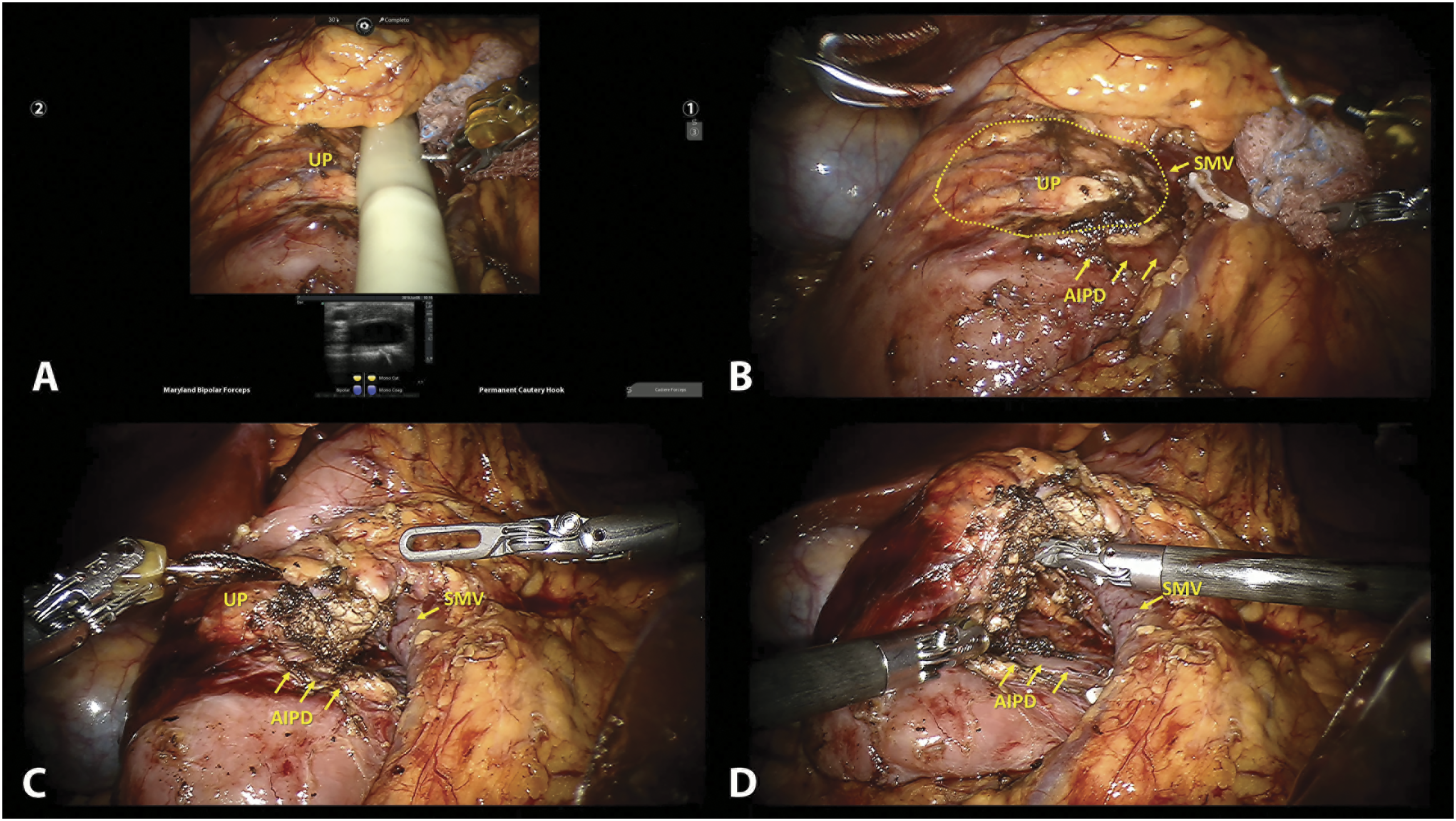
Results
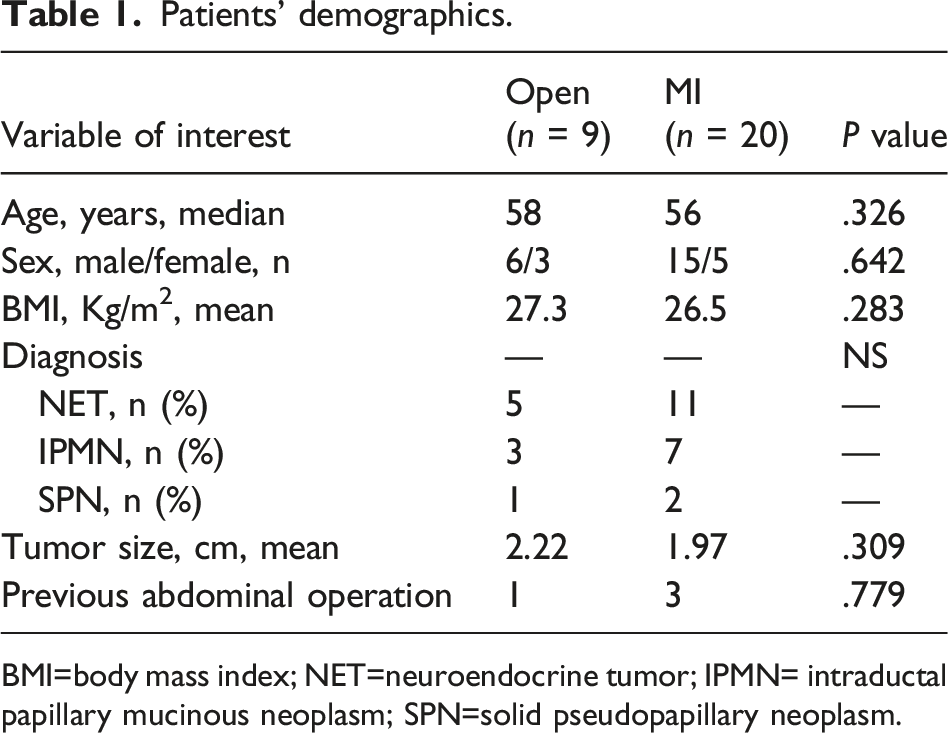
We studied 29 patients who underwent isolated resection of the uncinate process of the pancreas. The median age was 57 years old (range 26–77 years); there were 21 males and eight females. Twenty patients underwent minimally invasive (MI) resection. Fourteen patients were laparoscopic, and six patients had robotic resection of the uncinate process. Nine patients underwent open operation and were used for comparison (Figure 5). All patients were operated on for low-grade pancreatic neoplasms and distribution was not different among open or MI group (Table 1). Sixteen presented neuroendocrine tumors (NETs), ten intraductal papillary mucinous neoplasms (IPMNs), and three patients had solid pseudopapillary neoplasm (SPN). Mean tumor size was 2.1 cm and there was no significant difference between open and MI groups (p=.309). Mean body mass index (BMI) was 26.7 kg/m2 and there was no significant difference between both groups (Table 1). Four patients had previous upper abdominal operations (Table 1). Isolated resection of the uncinate process of the pancreas by open approach. (A) Inferior part of the uncinate process (UP) is already dissected from the duodenum and it is lifted. Duodenum perfusion is preserved. SMV, superior mesenteric vein; AIPD, anterior inferior pancreatoduodenal artery. (B) Superior part of the uncinate process is carefully transected. Main pancreatic duct is preserved. (C) The uncinate process is already transected. Main pancreatic duct is preserved, and the uncinate process pancreatic duct (UP branch duct) is identified and ligated. (D) Final aspect after isolated resection of the uncinate process of the pancreas. SMV, superior mesenteric vein; AIPD, anterior inferior pancreatoduodenal artery. Patients’ demographics. BMI=body mass index; NET=neuroendocrine tumor; IPMN= intraductal papillary mucinous neoplasm; SPN=solid pseudopapillary neoplasm.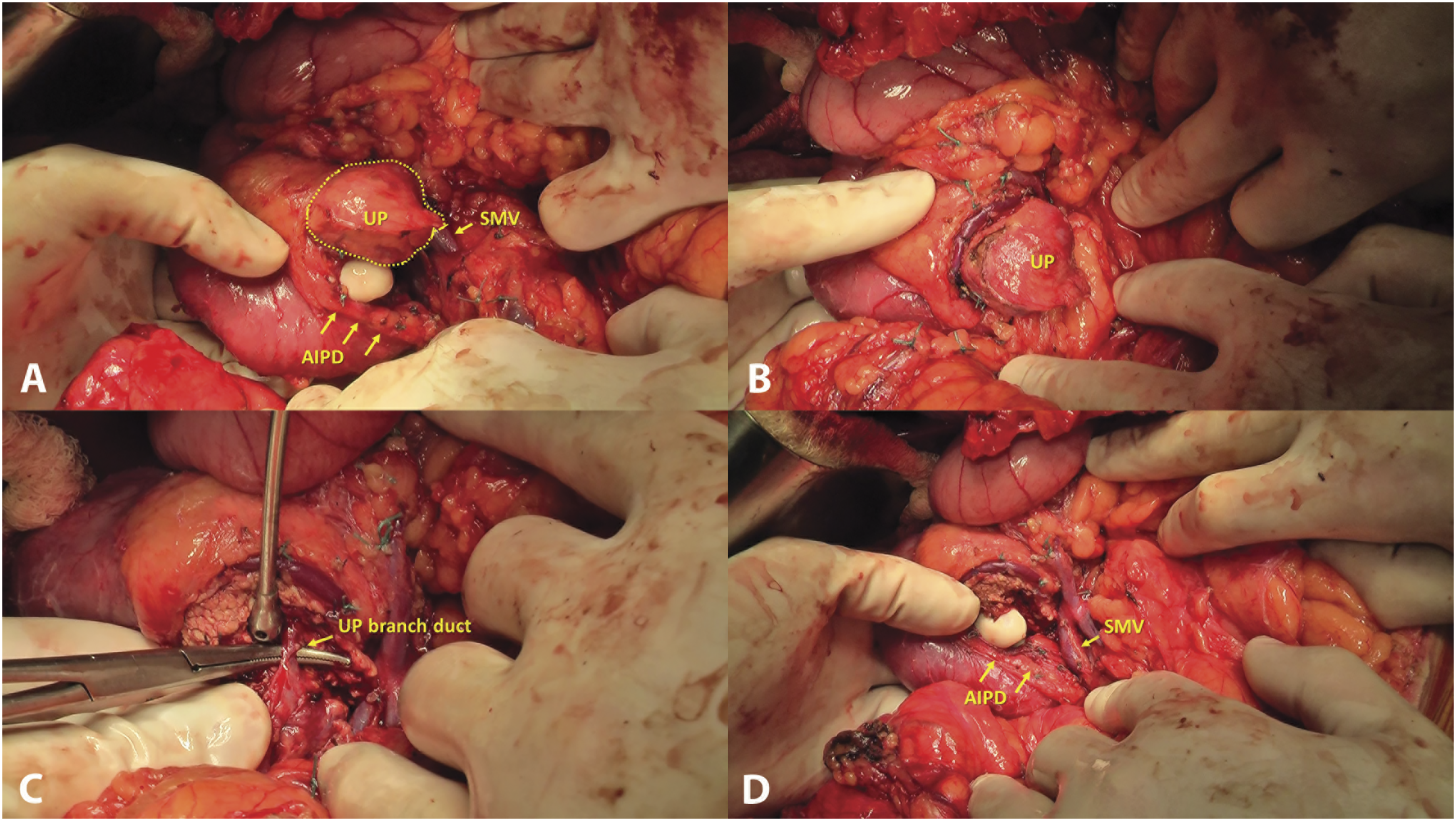
Results from uncinate process resection.
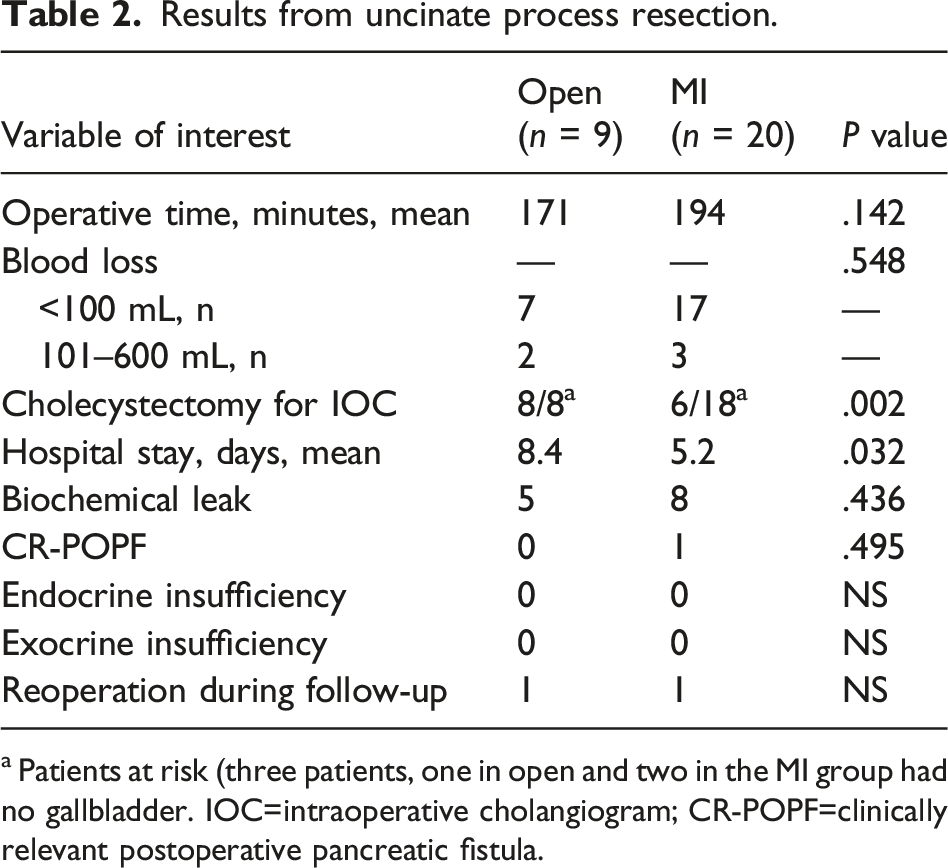
a Patients at risk (three patients, one in open and two in the MI group had no gallbladder. IOC=intraoperative cholangiogram; CR-POPF=clinically relevant postoperative pancreatic fistula.
The median hospital stay was 5 days but was significantly lower in the MI group (p = .032). Just one patient with severe coronaropathy needed the intensive care unit during recovery. Clinically relevant postoperative pancreatic fistula was observed in one patient (3.4%). Biochemical leakage was present in 44.8% of our patients. One patient with pancreas divisum presented no pancreatic fistula or biochemical leakage. No differences were found between the open and MI approach (Table 2).
Mean follow-up was 62 months (3–147). Two patients needed reoperation during follow-up. One patient operated by open approach developed incisional hernia. Another patient operated by robotic approach had persistent pancreatic pseudocyst and underwent a successful robotic Roux-en-Y cystojejunostomy with full recovery. No patient presented exocrine or endocrine insufficiency during late follow-up (Table 2).
Discussion
This study presents a large series of isolated resection of the pancreas and describes two minimally invasive approaches for the same procedure. There was an evolution toward the use of minimally invasive technique to perform uncinate process resections. Our initial cases were done open and since our first minimally invasive case, 5 all our cases were done laparoscopically. In recent years, we replace all our minimally invasive pancreatic surgeries for the robotic approach. 10 In a systematic review of the literature, only case reports were identified (8 cases).3-11
Malignant pancreatic tumors are treated with conventional procedures that always result in pancreatic anatomical and functional loss with digestive and systemic dysfunctions related to the extension of the pancreatic and surrounding resected structures. Although these procedures can be performed with low morbidity and mortality rates, 1 these procedures may also remove excessive pancreatic tissue in benign or borderline diseases. Therefore, pancreas-preserving procedures have been devised to reduce the impact of these procedure on pancreatic and surrounding structures such as enucleation 2 , spleen-preserving distal pancreatectomy, 15 central pancreatectomy, 16 dorsal pancreatectomy, 17 and pancreatic uncinatectomy.3-11 Pancreatic parenchymal-sparing surgery is indicated in selected patients with low-grade pancreatic neoplasms with a distance between tumor and main pancreatic duct of ≥3 mm (no focal stricture or dilation) according 2018 NCCN guidelines. 13
There are important clues to perform isolated resection of the uncinate process of the pancreas. After careful patient selection, the preservation of duodenal, biliary tract, and residual pancreas blood supply are critical. Preservation of the inferior posterior pancreatoduodenal artery and the duodenal arterial arcade is important in this procedure. Preoperative imaging studies are essential for surgical planning and the determination of the exact location of the benign or borderline lesions and their relationship to the main pancreatic duct are key to the success of this operation. Although preoperative endoscopic pancreatic stenting has been used for some authors to avoid pancreatic duct disruption during pancreatic enucleations, our experience with such strategy has not been as good as shown in the literature. 14 During the operation, intraoperative cholangiogram, catheterization of the main bile duct until the ampulla of Vater, and intraoperative ultrasound are necessary steps or tools to establish the superior limit of the resection and avoid main pancreatic duct injury. In the minimally invasive setting, the gallbladder could be spared (Table 2) in some patients using the findings of preoperative endoscopic ultrasound imaging, intraoperative laparoscopic ultrasound, or the use of indocyanine green fluorescence imaging during robotic approach. 10
The pancreatic fistula remains the main concern after resection of the uncinate process, but there is no study about its incidence after this complex operation due to the rarity of publications on the subject. Here, the incidence of clinically relevant postoperative pancreatic fistula was 3.4% (one patient). Biochemical leakage (previously denominated as Grade A POPF) was present in 44.8% of our patients. Adequate drainage of the raw pancreatic area and the absence of inadvertent lesions of the main pancreatic duct contribute for safe resection of the uncinate process of the pancreas. Importantly, endocrine and exocrine pancreatic functions were preserved in all patients, independently from the approach.
Minimally invasive resection of the uncinate process of the pancreas was first reported in 2008. 5 Since then, we have used this technique in selected cases. To date, twenty patients were treated with a minimally invasive approach: Six by a robotic approach and 14 via a laparoscopic approach. Recently, the robotic approach has become the standard technique for this operation. Robotic surgery has known advantages over laparoscopic approach that overcome some of the technical limitations of laparoscopy and extend the use of minimally invasive approach to more complex procedures such as uncinate process resection. It is known that the robotic procedure carries a higher cost and longer operations. However, the robot is excellent for more complex operations such as isolated resection of the uncinate process, and this procedure may be a good indication for the use of the robot.
Pancreatoduodenectomy may result in pancreatic functional loss with digestive and systemic dysfunctions related to the extension of the pancreas and resection of the surrounding structures. Although pancreas-preserving procedures have been devised to reduce the impact of extensive pancreatic resection, these procedures are rarely performed when a low-grade neoplasm is located in the head of the pancreas. Those patients have a high-risk of developing postoperative complications due to the presence of a soft pancreas and small pancreatic ducts which are common findings in those non-malignant tumors. This study compares favorably with our previous experience in both open and laparoscopic pancreatoduodenectomies.
In conclusion, minimally invasive resection of the uncinate process of the pancreas is a complex but a feasible procedure that preserves the pancreatic endocrine and exocrine functions and the upper digestive tract. This pancreas-sparing procedure is an interesting alternative to pancreaticoduodenectomy in selected patients.
Footnotes
Authors Contributions
MAM developed the laparoscopic and robotic approach for uncinate process resection. MAM: Conception and design of this study, acquisition, analysis and interpretation of all data, first drafting, and revision and final approval of the manuscript. FFM: Substantial contribution to design, statistical analysis, interpretation of all data, and revision and final approval of the manuscript. JCA: Substantial contribution to design, data acquisition, analysis and interpretation of data, and revision and final approval of manuscript. MCM: Design of the study, acquisition and analysis of data, and revision and final approval of manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.