
Abstract
Background
This study was designed to compare the postoperative complications after Robotic total gastrectomy (RTG) and robotic distal gastrectomy (RDG) and to systematically evaluate the safety and feasibility of RTG for the treatment of gastric cancer (GC).
Methods
Patients with GC who underwent RTG or RDG for curative intent between March 2010 and August 2019 were analyzed. We used propensity score matching (PSM) to reduce selection bias. The morbidity and mortality within 30 days after surgery between the RTG and the RDG groups were compared.
Results
According to Clavien–Dindo (C–D) classification, the morbidity and mortality of the RTG group were comparable to those of the RDG group. Subgroup analyses showed no significant difference between the RTG and RDG groups in all stratified parameters (all P > .05). Multivariate analysis revealed that age ≥70 years (P = .002) and surgeons’ experience ≤25 cases (P = .013) were independent risk factors for overall complication. Surgeons’ experience ≤25 cases (P = .010) was identified as an independent risk factor for severe complication.
Conclusion
RTG is a safe and feasible surgical procedure for the treatment of GC with acceptable morbidity and mortality. More complications were observed for RTG, indicating that RTG is more invasive than RDG.
Laparoscopic gastrectomy (LG) has gradually become a globally accepted surgical procedure for patients with gastric cancer (GC).1-3 The da Vinci surgical system has several technical advantages over laparoscopic instruments, including 3D vision, greater freedom of movement, tremor filtration, and improved ergonomics for the surgeon. Since the robotic gastrectomy (RG) was first reported by Hashizume et al 4 in 2003, increasing studies have demonstrated that RG is a safe and feasible procedure for the treatment of GC in terms of short- and long-term outcomes.5-9 However, robotic total gastrectomy (RTG) has not been as popular as RDG because of its technical difficulties, undetermined safety, and postoperative complications. Compared with RDG, RTG requires dissection of lymph nodes at the splenic hilum or along distal splenic vessels, as well as anastomosis of the esophagus to the jejunum. To date, there are a few large-scale studies regarding postoperative complications of RTG.
Thus, we designed this study to compare the complications after RTG and RDG according the Clavien–Dindo (C–D) classification and to systematically evaluate the safety and feasibility of RTG for the treatment of GC.
Materials and Methods
From March 2010 to August 2019, more than 800 cases of patients with GC underwent RG using the da Vinci® Surgical System (Intuitive Surgical, Sunnyvale, CA, USA) at a high-volume center in China. Inclusion criteria of patients were
1
age older than 18 and younger than 80 years
2
; primary gastric adenocarcinoma confirmed pathologically by endoscopic biopsy
3
; underwent RTG or RDG for curative intent
4
; pT1 to pT4a, N0 to N+, M0. Patients with the following characteristics were excluded
1
: remnant GC
2
; palliative surgery
3
; emergency surgery due to a complication (bleeding, obstruction, or perforation) caused by GC
4
; previous neoadjuvant chemotherapy or radiotherapy
5
; missing data. Pathologic evaluations and staging were updated according to the 8th Union for International Cancer Control (UICC)/American Joint Committee on Cancer (AJCC) staging system of GC.
10
The study was approved by the Ethics Committee of our center. One-to-one propensity score matching (PSM) with .02 caliper width was performed using a logistic regression model with the following variables: age, sex, body mass index (BMI), comorbidities, ASA score, histological type, and pathologic TNM stage. Flow diagram of the patient selection process is shown in Figure 1. Flow diagram of the patient selection process.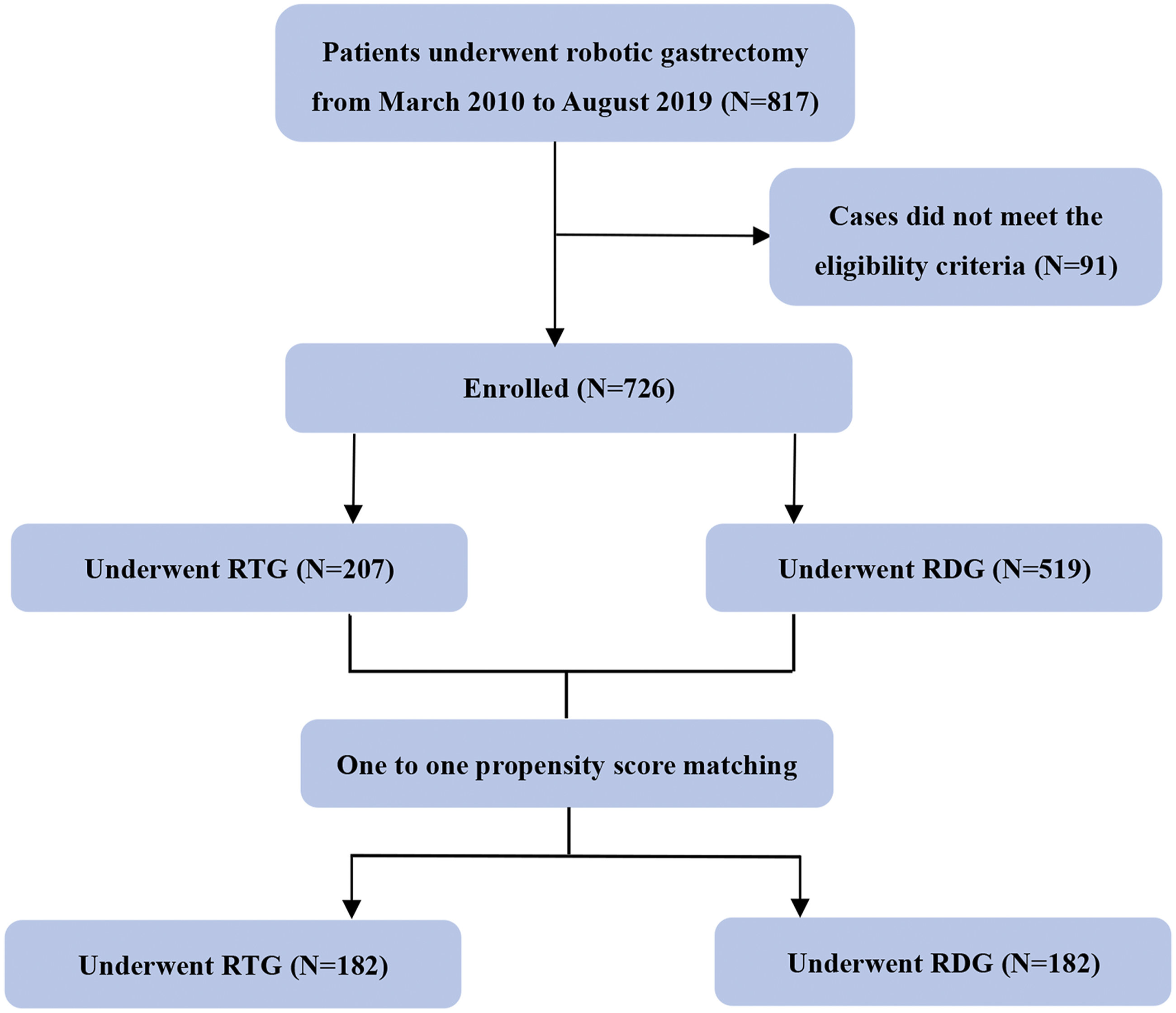
Definition of Postoperative Complication
Postoperative complications were recorded using the C–D classification and divided into local and systemic.11,12 When complication is associated with surgical technique near the operation field, such as wound or anastomosis, it was considered as local complication. The complication was classified as systemic when it was not associated with the operation field, such as pulmonary or hepatic. We reviewed morbidity and mortality occurred during hospitalization after the surgery. We also reviewed medical records of all patients until postoperative 3 months. Due to operations in general carry an overall risk and some self-limiting complications, here, we considered complications in C–D grade II or over to reflect actual technical maturity and focused our analysis on complications in C–D grade II or over. Grade II complications were considered as minor, and grade IIIa or greater, which required additional interventional or surgical treatment, were considered as severe complications.
Statistical Analysis
All statistical analyses were performed using SPSS, ver.24.0 (SPSS Inc, Chicago IL, USA). The Chi-square test, Fisher’s exact test, and independent sample t test were used for comparisons between the two groups. Categorical variables are presented as counts and percentages. Continuous variables normally distributed are expressed as the mean ± standard deviation (SD). Variables with P values <.10 in univariate analysis were included in the multivariate analysis. Multivariate analysis was conducted with the binary logistic regression model to identify independent risk factors for postoperative complications. P values <.05 were considered significant.
Results
Characteristics of Patients
Patient Background in Entire and Propensity Score-Matched Cohorts.
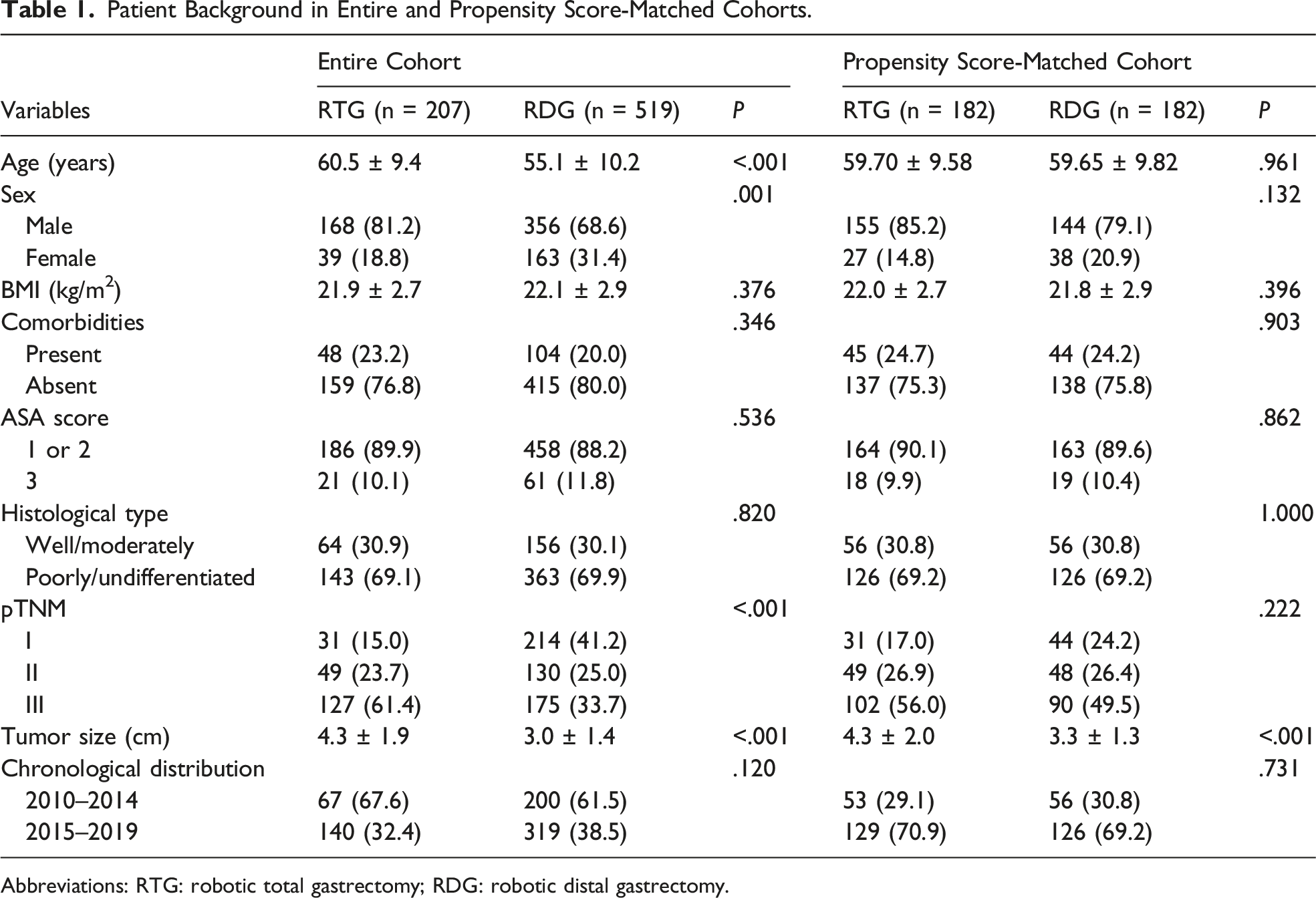
Abbreviations: RTG: robotic total gastrectomy; RDG: robotic distal gastrectomy.
Postoperative Morbidity and Mortality Following Robotic Gastrectomy in PSM Cohort
Morbidity and Mortality in the RTG and RDG Groups.
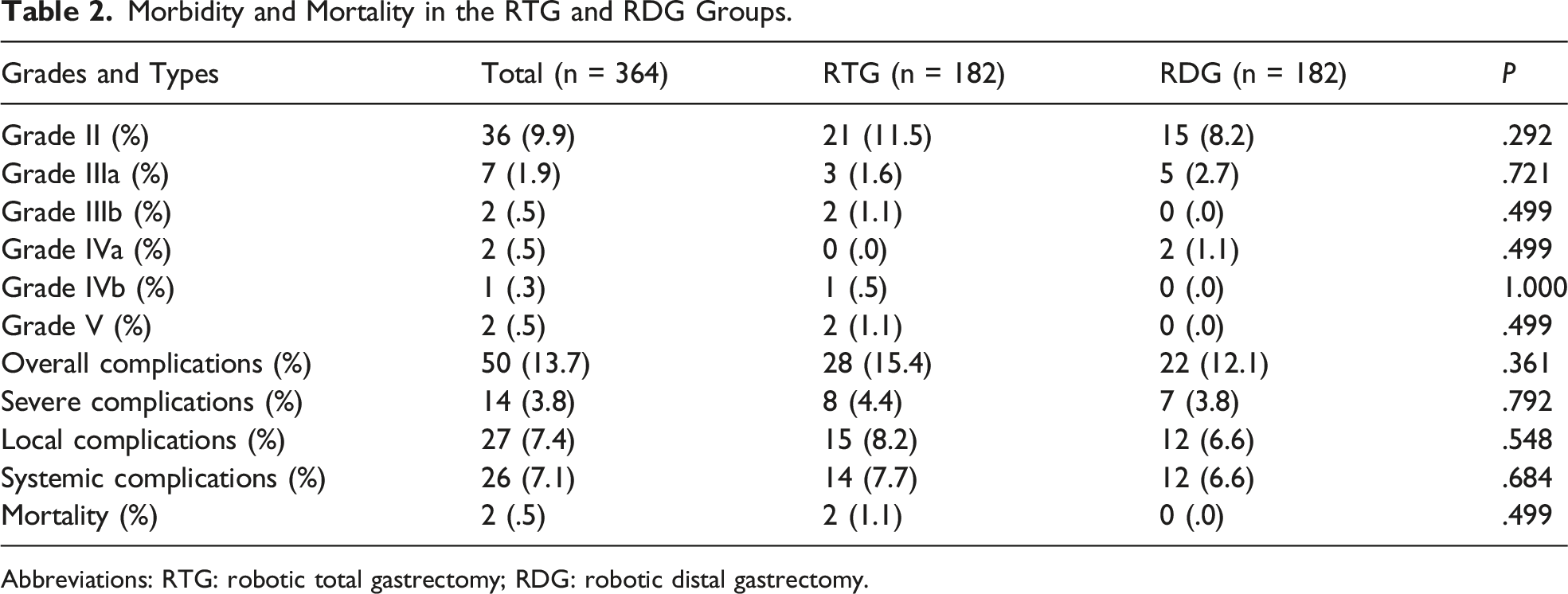
Abbreviations: RTG: robotic total gastrectomy; RDG: robotic distal gastrectomy.
Local Complications in the RTG and RDG Groups.
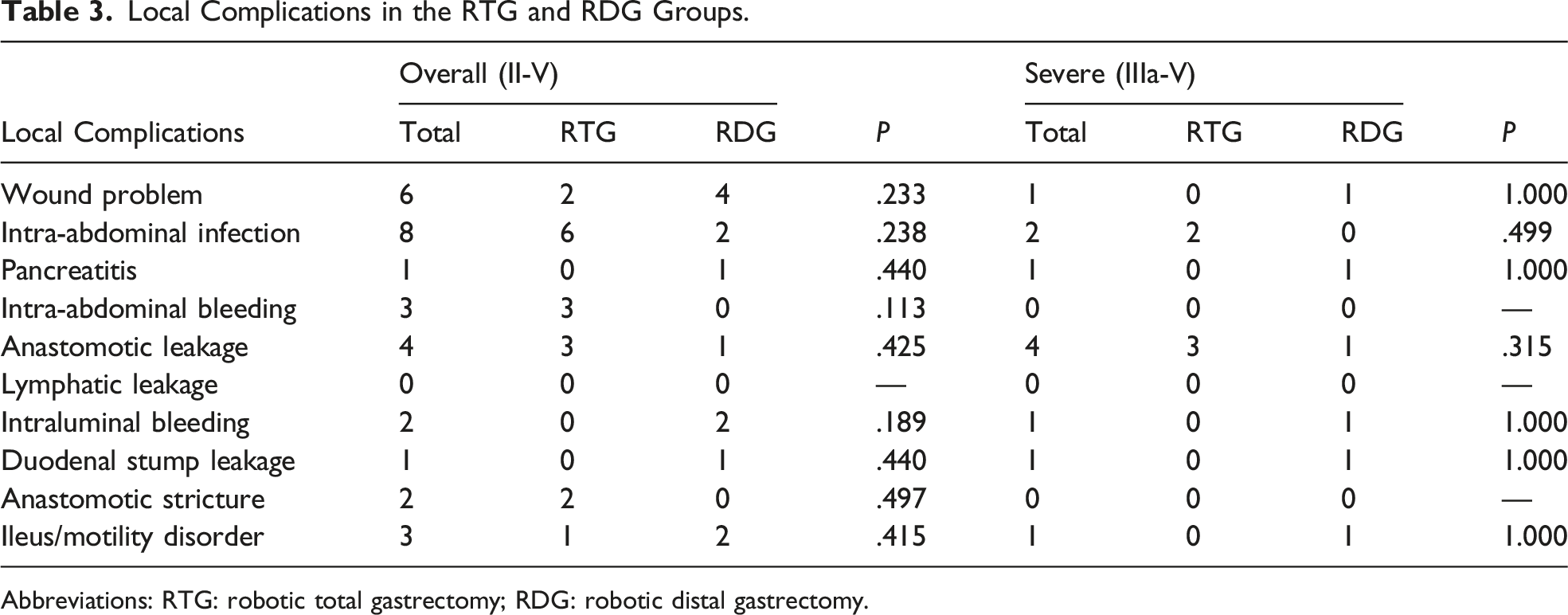
Abbreviations: RTG: robotic total gastrectomy; RDG: robotic distal gastrectomy.
Systemic Complications in the RTG and RDG Groups.
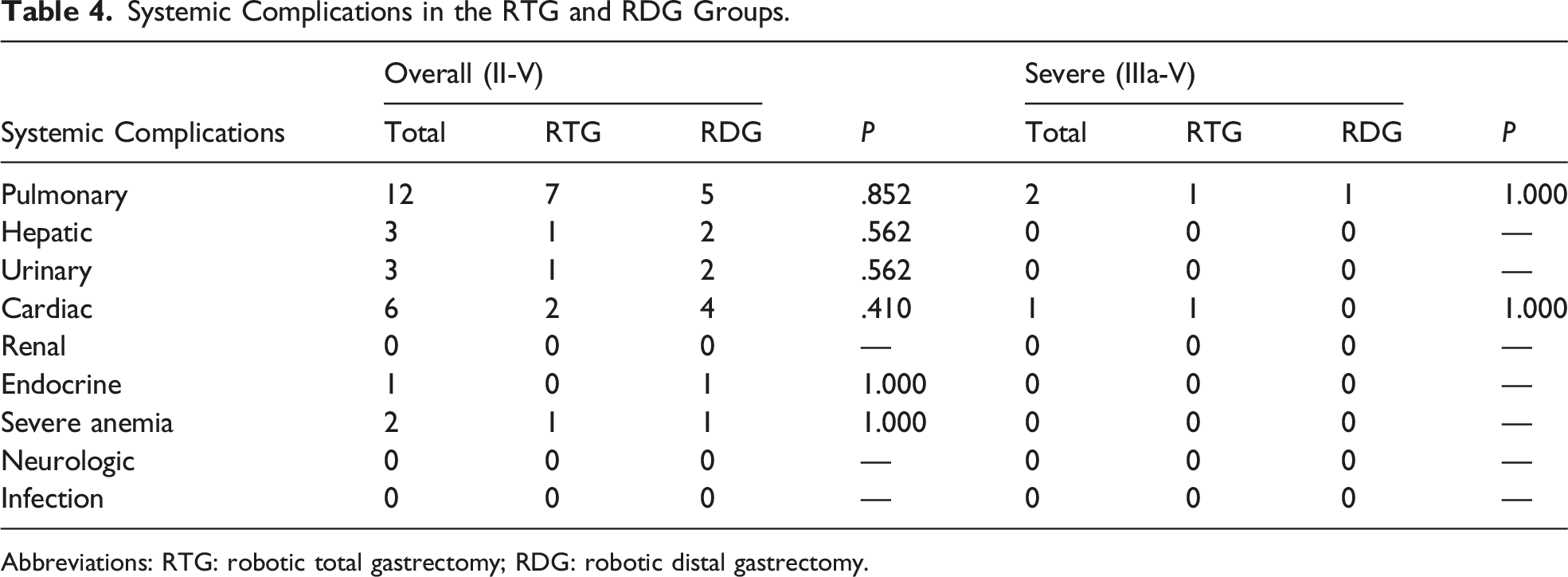
Abbreviations: RTG: robotic total gastrectomy; RDG: robotic distal gastrectomy.
In the RTG group, the most common local complication was intra-abdominal infection, followed by intra-abdominal bleeding and anastomotic leakage. In the RDG group, the most common local complication was wound problem. Most patients of intra-abdominal infection and wound problem could be cured by antibiotics or parenteral nutrition. Regarding systemic complications, pulmonary was the most common, and the majority of them were cured by antibiotics.
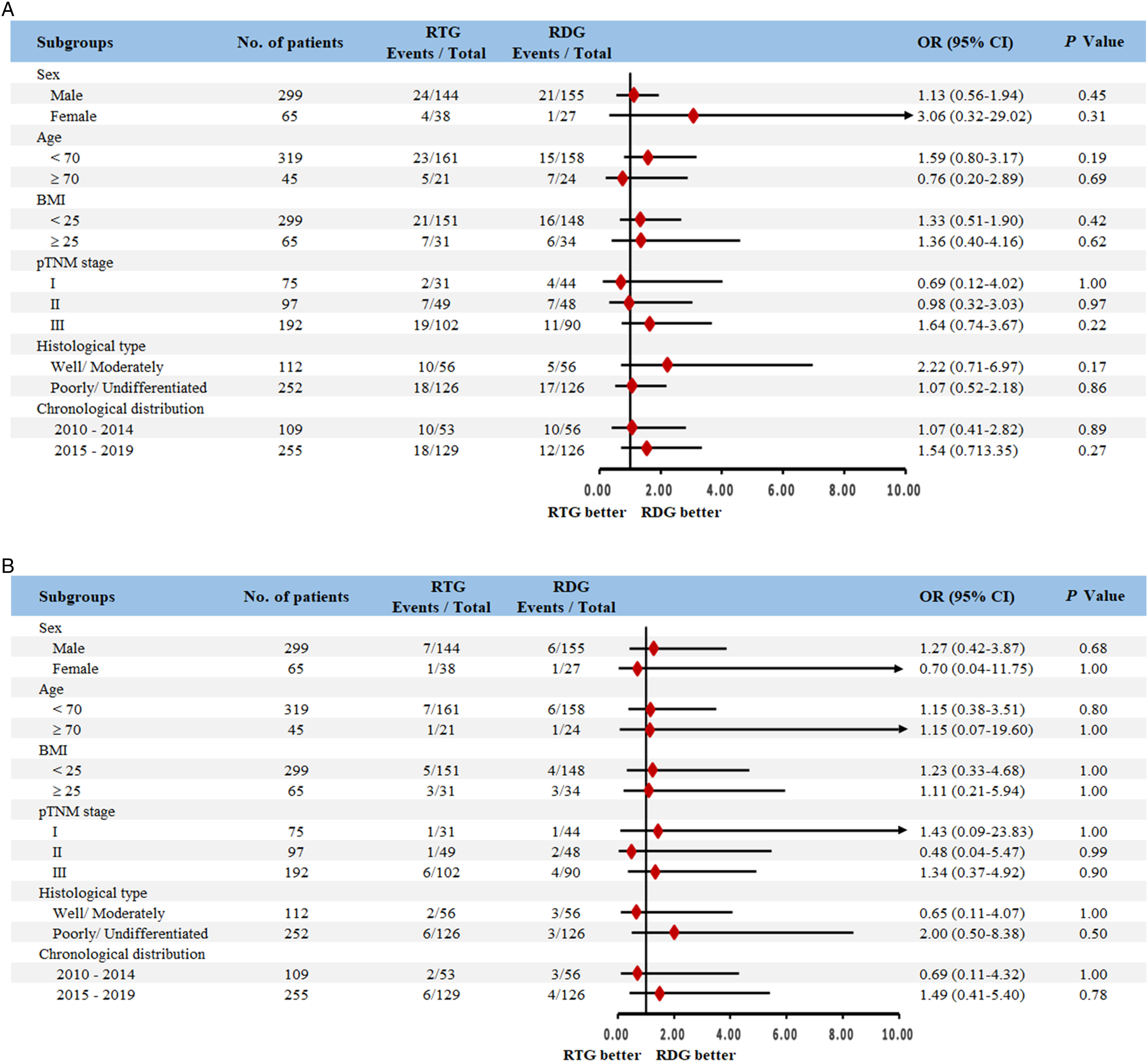
Figure 2 shows the complication rates in different age groups. The overall and systemic complication rates presented a general increased trend along with age, regardless of RTG or RDG groups. Subgroup analyses of postoperative complications showed no significant difference between the RTG and RDG groups in all stratified parameters in the comparison of overall (Figure 3A) and severe complications (Figure 3B). Postoperative complication rates in different age groups. (A) Overall complication; (B) severe complication; (C) local complication; (D) systemic complication. Subgroup analyses of postoperative complications. (A) Overall complications; (B) severe complications.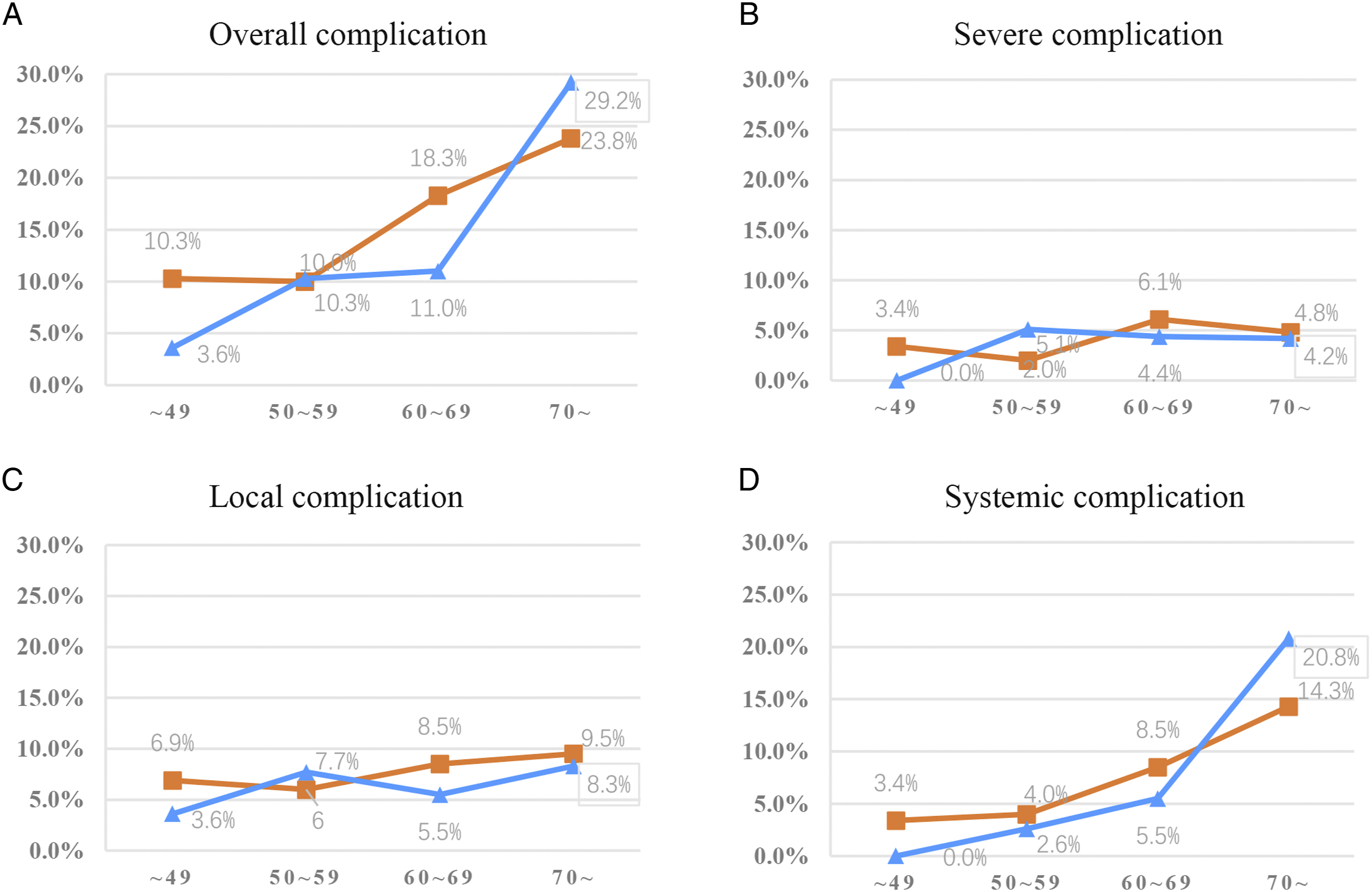
Risk Factors for Complications
Multivariate analysis revealed that age ≥70 years (P = .002) and surgeons’ experience ≤25 cases (P = .013) were independent risk factors for overall complication (Supplementary Table 1). As for severe complications, age, BMI, and surgeons’ experience were significantly correlated with severe complication in univariable analysis. Surgeons’ experience ≤25 cases (P = .010) was identified as an independent risk factor for severe complication (Supplementary Table 1).
With respect to local complication, surgeons’ experience ≤25 cases (P = .033) was identified as independent risk factor in multivariate analysis (Supplementary Table 2). In terms of systemic complication, age ≥70 years (P < .001), BMI ≥25 (P = .006), and presence of comorbidity (P = .018) were independent risk factors in multivariate analysis (Supplementary Table 2).
Discussion
In this study, patients underwent RTG showed higher complication rate when compared with those underwent RDG although the difference did not reach statistically significant.
Previous studies reported that the overall complication rate of RG varied from 5.2% to 24.1%.13-16 In the report of multicenter study evaluating safety and feasibility of RG for stage I/II GC, the severe complication rate was 2.5%. 17 Another multicenter study reported that the overall and major complication rates were 13.5% and 1.3%, respectively. 18 However, patients who underwent RDG account a large part in these studies and they did not perform specific analysis for RTG. Ye et al 14 reported a 7.5% overall complication rate in the RTG group. Wang et al 15 reported that the major complication rate after RTG was 14.3%. In the present study, the overall complication rate in the RTG group was 15.4%, which was slightly higher than that in the RDG group, but without statistically significant difference. The severe complication rate in the RTG group was 3.8%, which was comparable with those in the RDG group.
The major concern following RTG is esophagojejunostomy (EJ)-related complications. As reported by Wang et al, 15 the dominant major complication after RTG was anastomotic leakage. The anastomotic leakage rates following RTG were reported from 1.4% to 5.3%.14,15 In the current study, we observed three cases of EJ leakage and two cases of anastomotic stricture in the RTG group.
A recent multicenter study reported that 25 cases were needed to overcome complications learning curve of RG. 19 Based on this, we divided the surgeons’ experience into early (first 25 cases) and late phases, aiming at evaluating the relationship between surgeon’s experience and risk of morbidity after RG. In the present study, surgeons’ experience ≤25 cases was found to be an independent risk factor for overall, severe, and local complications. This indicated that even the surgeons proficient at LG should also be alert to the occurrence of postoperative complications during the learning period of RG. In order to minimize the incidence of postoperative complications due to the lack of experiences, we suggest that surgeons should choose patients in good conditions in the learning stage of RG. In clinical practice, surgeons tend to perform more RDG in the learning phase before they transferred toward RTG. To reduce the bias due to effect of learning curve, the patients were divided into two phases. The results of subgroup analyses for patients in different phases were consistent with that for all cases in PSM cohort.
Adequate number of retrieved lymph nodes not only improves the accuracy of staging and prognostic assessment but may also result in improved oncologic outcomes.20-22 According to the literature, the impact of number of harvested lymph nodes on morbidity following gastrectomy is controversial. Our previous study found that harvested lymph nodes of more than 30 were an independent risk factor for complication after total gastrectomy. 23 We attribute this to adequate lymphadenectomy during operation, which sometimes injures vessels and increases the risk of postoperative intra-abdominal bleeding. However, most patients in our previous study underwent open or laparoscopic surgery rather than RG. In the current study, the number of retrieved lymph nodes was not associated with postoperative complications, indicating that adequate number of retrieved lymph nodes is safe and feasible without increasing the risk of morbidity. Ye et al 14 reported that RTG could retrieve more lymph nodes as compared with laparoscopic total gastrectomy (LTG). This may attribute to the robotic surgical system allow the surgeons to reach deep-seated vessels and some delicate areas more easily. Meanwhile, the stable working platform and 3D views could facilitate lymph node dissection in tough areas. The superiority of RG during the procedure of lymph node dissection was also observed in the study conducted by Kim et al. 24 They found that RDG could provide an advantage over LDG in the dissection of technically demanding suprapancreatic area and the splenic vessels. A recent meta-analysis showed that more lymph nodes were harvested during RG than during LG. 25 Given these results, we recommend that adequate lymphadenectomy should be performed by surgeons experienced in RG.
According to the current evidence, the impact of age on morbidity following RG has seldom been reported. Okumura et al 26 demonstrated that the morbidity after RG in elderly patients with GC was similar with those underwent LG, indicating that RG could be a safe and feasible procedure. In the current study, elderly patients (age ≥70 years) were associated with increased morbidity. Furthermore, the specific analysis for morbidity in different age groups showed that the overall and systemic complication rates presented an increased trend along with age. This indicated that increased age would be a leading risk factor for systemic complication than for local complication. The reason for this may be that elderly patients always have reduced functional reserve and increased comorbidities.27-29 In the current study, comorbidity was also identified as an independent risk factor for systemic complication. Therefore, for elderly patients, we should pay more attention in preoperative assessment and postoperative management.
There are several limitations to this study. First, all surgeons included in this study had experience with LG prior to initiation of RG, which limited the generalizability of these findings to surgeons with less LG experience. Second, this study is limited in generalizability since BMI of majority of patients was lower than 25 kg/m2, which may be lower than what most surgeons would encounter in Western countries. Last, patients who underwent neoadjuvant therapy were excluded from the study. This may limit the generalizability of the study results.
In conclusion, the current study suggests that RTG is a safe and feasible surgical procedure for the treatment of GC with acceptable morbidity and mortality. More complications were observed for RTG, indicating that RTG is more invasive than RDG. We suggest that surgeons should be more careful and choose patients in good conditions in the learning stage of RG.
Supplemental Material
sj-pdf-1-sri-10.1177_15533506211047011 – Supplemental Material for Comparison of the Postoperative Complications Between Robotic Total and Distal Gastrectomies for Gastric Cancer Using Clavien–Dindo Classification: A Propensity Score-matched Retrospective Cohort Study of 726 Patients
Supplemental Material, sj-pdf-1-sri-10.1177_15533506211047011 for Comparison of the Postoperative Complications Between Robotic Total and Distal Gastrectomies for Gastric Cancer Using Clavien–Dindo Classification: A Propensity Score-matched Retrospective Cohort Study of 726 Patients by Zheng-yan Li, Yong-liang Zhao, Feng Qian, Bo Tang, Zi-yan Luo, Yan Wen, Yan Shi and Pei-wu Yu in Surgical Innovation
Footnotes
Acknowledgments
The authors thank Yan Wen for data collection and management.
Author Contribution
Li Zheng-yan, Shi Yan, and Yu Pei-wu designed the study. Qian Feng, Luo Zi-yan, and Wen Yan were responsible for data acquisition. Zhao Yong-liang and Shi Yan were responsible for quality control of data and algorithms. Li Zheng-yan and Tang Bo analyzed and interpreted the data. Li Zheng-yan wrote the article. All authors have seen and approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Chongqing Postdoctoral Science Special Foundation.
Ethical Approval
This study was approved by the Ethics Committee of the Southwest Hospital, Third Military Medical University. This article does not contain any studies with animals performed by any of the authors.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.