
Abstract
Background
The high-definition 3D exoscope is an innovative and promising tool that was recently introduced in the clinical practice. It may be used during open surgical procedures to enhance the ability to perform precise dissection of fine structures. We describe our preliminary experience with the 3D exoscope in thyroid surgery, discussing potential advantages of this system.
Methods
A high-definition 3D exoscope (3D VITOM®) mounted on the VERSACRANETM holding system (Karl Storz, Tuttlingen, Germany) was used to perform open thyroid surgery.
Results
The 3D exoscope was used in three patients without significant intra-operative delay or complications. Both thyroidectomy and central compartment dissection were performed. The 3D exoscope allows to perform precise dissection in the identification and preservation of the recurrent laryngeal nerve and the parathyroid glands.
Conclusions
3D exoscope-assisted thyroid surgery seems to be feasible and safe. Further studies should be encouraged to analyze potential clinical benefit in the post-operative period.
Keywords
Introduction
Several exoscopic devices have been developed during the last decade such as the VITOM® 3D (Karl Storz, Tuttlingen, Germany), Orbeye® (Olympus, Tokyo, Japan) and Modus VTM (Synaptive Medical). In particular, Karl Storz’s video telescope operating monitor (VITOM®) was released in 2011 as a two-dimensional (2D) high definition exoscope. The telescope was characterized by a 10 mm outer diameter and a shaft length of 14 cm, allowing for mean focal distance is 200 mm with the depth of field of 12 mm. It was connected to a high-definition (HD) digitized camera with an optical zoom and focus features, providing high-resolution image with minimal spherical aberrations or chromatic distortions, and a wide viewing angle comparable to the operating microscope. However, the main limitation was the lack of stereopsis compared to the operating microscope, resulting in a reduced image depth on the screen. The introduction of three-dimensional systems (VITOM® 3D operating exoscope) aimed to improve the depth perception during surgery allowing for planning, targeting and controlling fine hand movements. 1
The high-definition (HD) VITOM® 3D operating exoscope is an innovative and promising tool that was recently introduced in the otorhinolaryngologist – head and neck surgeon’s clinical practice. The exoscope was developed to substitute the operating microscope in performing microsurgical procedures such as microvascular anastomoses, laryngeal and lateral skull base surgery.2-4 Nevertheless, the possibility to employ this new technology during other surgeries should be further investigated.
Technological advancements have been introduced in thyroid surgery with the purpose of better cosmetics results and less postoperative pain. However, the primary aim during a thyroidectomy is to completely remove the thyroid gland preserving recurrent laryngeal nerves (RLNs) and parathyroid glands (PGs). After a preliminary dissection, the RLN should be adequately identified to reduce the risk of iatrogenic damage. Although various medical devices have been developed over the past two decades for intraoperative use to simplify the RLN preservation, the visual nerve identification still represents the gold standard.5,6 Loupes are widely used to enhance the surgical field magnification, improving the ability to perform tissue dissection in the area of the RLNs and PGs, consequently reducing the risk of nerve tearing and PGs devascularization. However, the magnification is restricted to the surgeon unless the loupes are coupled to a microcamera. Moreover, a three-dimensional endoscopic-assisted thyroidectomy was already introduced in the clinical practice. 7 In this context, the introduction of the 3D exoscope as a new visualization and magnification tool represents an innovative way to improve the identification and preservation of the RLNs and the PGs during conventional open thyroidectomy. This system projects the surgical image onto a large 32 inch monitor which can be easily seen by all the operators and other surgical staff. The 3D image of the exoscope allows the surgeon to have a better view of the surgical field associated to depth perception thanks to a 4K screen. Moreover, image magnification could be adjusted to the specific procedure, and it could be modulated during surgery to focus anatomical structures of interest. Thanks to these features, the 3D exoscope could be used during open surgical procedures to enhance the ability to perform precise dissection of fine structures.8,9 Finally, the possibility to easily record images of the surgical field showing intact RLN and PGs could have an impact also from a medicolegal perspective.
The aim of this paper is to describe our preliminary experience with the 3D exoscope in thyroid surgery, discussing potential advantages of this system.
Methods
The Institutional Ethic Committee of Humanitas Clinical and Research Center approved the study (Prot. Ne. CE Humanitas 478/19 06/2019). Informed consent was obtained from patients.
Exoscope Configuration
A high-definition 3D exoscope (3D VITOM®, Karl Storz, Tuttlingen, Germany) was used. A telescopic 3D camera, with a magnification power of 8-30 X and a depth of field of 7-44 mm, was connected to a 4 K resolution screen through IMAGE 1 S platform. Visualization in 3D requires the viewer to wear 3D glasses, that allow the surgeon to have a better view of the surgical field improving their depth perception. The system’s light source is from a table-top lighting system (Power LED 300), feeding light to the surgical field via a fibre optic cable that fixes to the camera.
The operating camera system is controlled by an intuitive joystick (IMAGE1 PILOT). The IMAGE1 PILOT is able to zoom in and out on the surgical field by pulling or pushing in the joystick. The focus of the camera could be modified by rotation of the joystick, while the image projected on the screen could be adjusted by moving up, down, left and right on the joystick on the vertical axis.
Both the 3D camera and the IMAGE1 PILOT could be sterilely covered to allow the surgeon to control them during the dissection. The exoscope was mounted on the VERSACRANETM holding system (Karl Storz, Tuttlingen, Germany), which can be manually adjusted by the operator to place the camera in the preferred position, allowing for a focal distance from 20 cm to 50 cm. The main advantage of this system is the smaller size and the greater maneuverability if compared to some of the larger operating microscopes.
Operating Room Setting
During thyroid surgery, we placed the 3D camera above the surgical field at a distance of approximately 40 cm. The VITOM® projects the surgical image onto a 32 inch 4K resolution screen which is located in front of the main surgeon, on the other side of the operating table. Moreover, an additional screen is placed in front of the assistant surgeon to allow for adequate visualization and magnification of the surgical field. The screens must be placed precisely in front of the intended user(s) to allow for a precise 3D visualization of the surgical field. The IMAGE1 PILOT is fixed to the surgical table and positioned towards the feet of the patient, between the surgeon and scrub nurse. The VERSACRANETM holding system is placed between the surgeon and assistant surgeon standing at the head of the patient, when three surgeons are performing the procedure.
An example of the operating room (OR) setting is shown in Figure 1. Real operating room setting using the 3D exoscope.
3D Exoscope-Assisted Thyroid Surgery
The first part of the dissection was carried out without the direct use of the exoscope. However, it was mounted over the surgical field to record the procedure, and to share surgical steps to the entire staff. A midline neck incision was performed as in open conventional thyroidectomy. The dissection proceeded until the thyroid lobe was mobilized from the deep tissues and the superior thyroid artery was ligated. Once surgical landmarks (eg trachea) were adequately exposed, the surgeons wore 3D glasses and started using the exoscope. The surgical table was rotated away from the main surgeon for about 20° to better focus the area of interest (tracheoesophageal groove) in the surgical field. A precise dissection of tissue could be conducted, and small vessels could be easily recognized and ligated to preserve the parathyroid glands. Once identified, the RLN was traced cephalad until it entered the cricothyroid membrane (Figure 2). After this step, the lobectomy was completed with the aid of the exoscope. Then, central compartment neck dissection was performed using the exoscope. PGs could be easily recognized and differentiated from the contiguous lymph nodes, so the vascularization to the PGs was preserved. At the end of the lobectomy and homolateral central compartment dissection, the orientation of the image was rotated without moving the camera, and the same procedure was performed on the contralateral side. At the end of the procedure, haemostasis could be precisely performed under exoscopic vision to avoid nerve injury with bipolar cautery. The anatomic integrity of the RLNs was verified before drainage placement and wound closure. An explanatory video is provided in 2D vision (Video S1). High-definition vision with the 3D exoscope after the identification of the right RLN (black arrow), the inferior (black arrowhead), and superior (white star) parathyroid glands. Note the difference with lymph nodes suspected for disease (black asterisks).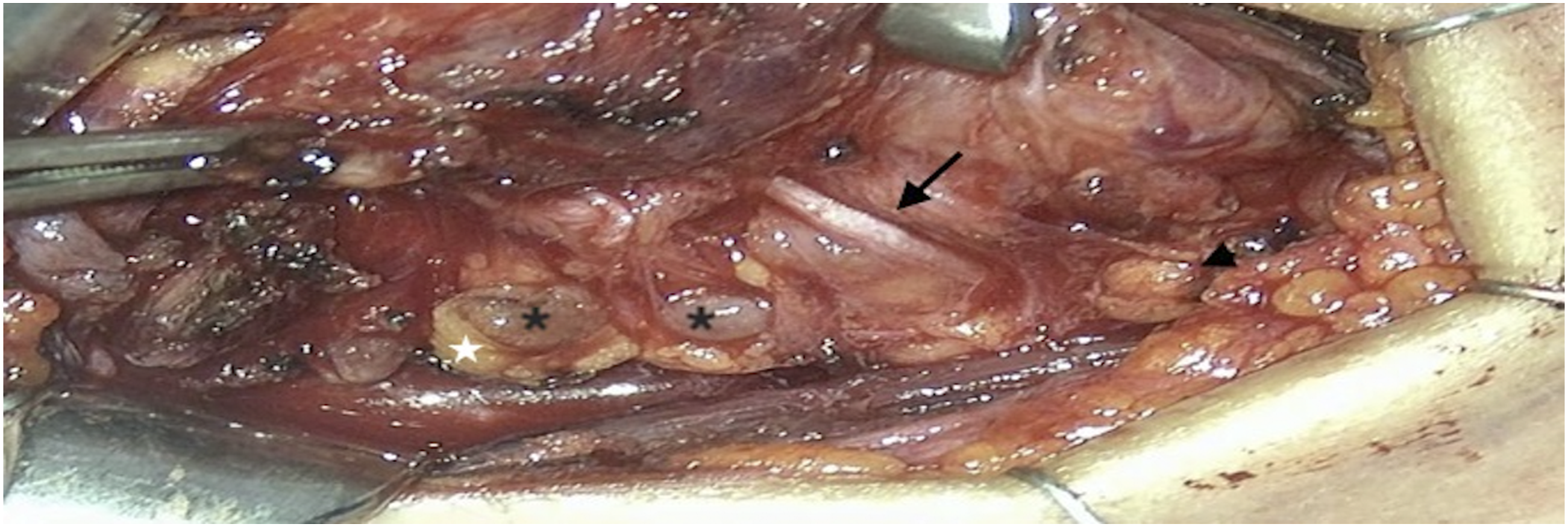
Data Collection and Analysis
A customized questionnaire (Exoscope Quality Assessment Tool) was used in order to analyze the main features of a surgical visualization and magnification tool, as reported in a previous paper. 10 After each procedure, main and assistant surgeons and scrub nurses were asked to fill out a questionnaire on a three-point Likert scale (1—not acceptable, 2—acceptable, 3—good). Data were collected and stored in a Microsoft Excel® spreadsheet. Dichotomous variables were reported as counts and percentage, while continuous variables as median and IQR (interquartile range). The Fisher exact test was used for the comparison of the Exoscope Quality Assessment Tool among the surgeons and the nurses groups. Our criterion for statistical significance was set at P-value of less than .05 (two-tailed).
Results
Three (females: 2; mean age: 47.0, range 42-56) total thyroidectomies with or without central compartment neck dissection were performed. The 3D exoscope was used without significant intra-operative delay or complications compared to the standard procedure without the exoscope. The exoscope set-up time was approximately 5 min in all the procedures. Mean operative time was 96 min (range 81-119).
Exoscope Quality Assessment Tool results. Data are Reported as Counts and Percentage for Each Item.

Discussion
In this paper we showed the feasibility of 3D exoscope-assisted thyroid surgery. The implementation of lighting and magnification of the surgical field determined by the exoscope could improve the ability to perform precise dissection of fine structures. In particular, this technology allowed the identification of the RLNs and the preservation of the PGs without complications.
Although the exoscope was developed to substitute the operating microscope in microsurgical procedures, several papers have been recently published demonstrating the usefulness of exoscope-assisted open surgery. In particular, the exoscope was used for parotid surgery 8 and upper airway stimulation 9 during the identification and dissection of the facial and hypoglossal nerves, respectively.
The Exoscope Quality Assessment Tool was used to better define advantages and disadvantages of this system in open thyroid surgery, as already performed in other clinical and pre-clinical contexts. In particular, the questionnaire was proposed to both main and assistant surgeons, and scrub nurses to identify any differences during exoscope-assisted thyroid surgery.
One of the main advantage of this system is surely the possibility to share the same vision of the main surgeon during the procedure.10,11 As shown in Video 1, the first part of the thyroidectomy was not performed under exoscopic vision, but the exoscope was only used to share the surgical vision and to record the surgical steps for educational purposes. The optimal ergonomics of the small 3D camera, associated to the slim holding system, allowed the exoscope to be placed above the surgical field without interfering with surgical maneuvers. In addition, both the 3D camera and the IMAGE1 PILOT could be equipped with sterile covers. In fact, both items “range of motion of the holding system” and “surgical working space” were judges “very good” by almost all participants. Once the macroscopic dissection was carried out as conventional open thyroidectomy, the main surgeon and the assistant could wear the 3D glasses and switched to exoscopic vision. Also, the scrub nurse could benefit from the 3D vision on the HD screen to better understand surgical steps, and to anticipate the surgeon’s next choice of instrument. From this perspective, we should mention that an additional screen should be placed in front of the assistant and the scrub nurse (Fig. 1), given that the optimal 3D vision could be achieved only with the gaze perpendicular to the screen.
The “image quality” and especially the “luminance” are the exoscope’s features that need an improvement according to both surgeons and nurses responses. Even if the 3D vision enhance the perception of objects volume and the depth of structures for planning, targeting and controlling fine movements, the use of 3D glasses probably reduce the luminance of the surgical field compared to conventional shadowless operating lamps. Moreover, the scrub nurses reported a not negligible eye strain due to the 3D glasses.
Even if the image quality is expected to improve thanks to technological advancements, the “magnification rate” was considered adequate by all participants to improve the definition of fine structures during the identification and preservation of the RLNs and the PGs. Another aspect that should be mentioned was the possibility to modulate the image magnification dynamically during the procedure. The joystick was easy to use, allowing movement of the camera and magnification of the area of interest during the procedure, and assisting the surgeon during fine dissection. This could represent an advantage compared to surgical loupes given their fixed magnification. Moreover, the image orientation could be changed without moving the camera, and there was no loss of time in the transition to the contralateral side during total thyroidectomy. In general, the exoscope set-up was rated “very good” by all participants, as demonstrated by the fast set-up time of approximately 5 min. Some differences in terms of OR set-up are encountered depending on the surgical procedure, but the system is surely intuitive and easy to prepare for thyroid surgery with no intra-operative delay.
A central compartment neck dissection was performed in one patient after thyroidectomy. Exoscopic assistance was useful during the first part of the dissection when the RLN should be separated from the lymph nodes along its course. Then, the exoscope was not strictly necessary and the dissection could be completed on a direct vision. In our opinion, if only crucial surgical steps are performed with the aid of the exoscope, the operative time could be comparable to a conventional thyroidectomy. However, a learning curve may be expected in first-time users.
Some concerns should be raised from the economic perspective. Given the widespread of surgical procedures performed in the otolaryngology field (eg microvascular anastomoses, laryngeal and lateral skull base surgery), the possibility to use the exoscope also for thyroid surgery will may be encouraged in the future. On the other hand, exoscope-assisted thyroid surgery seems to present an unfavorable cost-benefit ratio in other settings, such as general surgery, where the exoscopic system has not been introduced at this time.
Conclusion
3D Exoscope-assisted thyroid surgery seems to be feasible and safe. The high-definition 3D exoscope could be used to perform precise dissection in the identification and preservation of the RLNs and the PGs. Further studies should be encouraged to analyze potential clinical benefit in the post-operative period.
Footnotes
Authors' Contributions
GM: Study design, data analysis, manuscript development, review of final manuscript. AC: Study design, data collection and analysis, manuscript development, review of final manuscript. ADV: Study design, review of final manuscript. FF: Data collection, review of final manuscript. GS: Study design, manuscript development, review of final manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.