
Abstract
Background. There have been few advances in technique since vascular anastomosis was performed with silk suture on a curved needle in 1902. This technique results in disruption of the endothelium with exposed intraluminal suture, both of which may lead to thrombocyte aggregation, intimal hyperplasia, and vascular stenosis. A variety of alternative techniques have been explored, with limited success. Photochemical tissue bonding (PTB) is a light-activated methodology of rapidly cross-linking tissue interfaces at the molecular level. Herein, we describe a new technique for anastomosis of venous interposition graft in an ovine model of femoral artery bypass utilizing PTB. Methods. Polypay specific pathogen free sheep (n = 5; 40-45 kg) underwent femoral artery bypass utilizing saphenous vein. The femoral artery was transected and reversed saphenous vein was implanted as an interposition graft. The proximal anastomosis was created as a vein-over-artery cuff utilizing PTB, and the distal anastomosis was created with standard interrupted 8-0 polypropylene suture. Four weeks post-index operation, femoral angiogram was performed to evaluate patency, tortuosity, and luminal diameter. All bypass grafts were harvested and longitudinal and transverse histological sections from the proximal anastomosis were analyzed. Results. The PTB anastomoses (n = 5) were immediately watertight and patent. All animals survived the 28-day study duration. Angiography revealed patent grafts with no aneurysm or stenosis (n = 5). Histologic examination revealed integration of the venous endothelium with the arterial adventitia. Conclusion. Photochemical tissue bonding creates an immediate strong, watertight vascular anastomosis that can withstand physiologic arterial pressure and remains patent at 28 days without the need for intraluminal suture.
Introduction
After performing the first successful vascular anastomosis in 1902, Alexis Carrel formulated the tenets of vascular repair: avoid luminal narrowing, avoid folds and/or a rough inner surface of the vessel, appose the intimal edges, and avoid contact between suture material and blood. 1 While the first three guidelines are routinely followed more than a century later, vascular anastomosis with suture remains the clinical standard to this day, and there have been few advances of significance since the first vascular anastomosis with fine silk on a curved needle. 2 While practical, there are numerous disadvantages of the needle and suture technique. The initial penetration of the vessel wall by the needle results in a defect approximately twice the diameter of the needle. 3 The traditional hand-sewn vascular anastomosis can be time consuming (sometimes >30 minutes), increasing the risk of thrombosis. 4 Resultant disruption of the endothelium may initiate a repair response involving platelet aggregation, smooth muscle proliferation, and endothelial thickening.3,5 The intraluminal suture in a conventional sutured anastomosis may lead to a foreign body reaction resulting in thrombocyte aggregation, intimal hyperplasia, and vascular stenosis.6-8 Despite these significant drawbacks of needle and suture for vascular anastomosis, this technique is performed in many common surgical interventions including large vessel and microvascular anastomoses.
Recognizing these issues, a variety of alternative techniques attempting to eliminate the intraluminal suture have been attempted with limited success. In the past 50 years sutureless techniques utilizing rings/couplers,9-15 clips,8,16-18 stents,19-22 and adhesives23-27 have been described. While achieving patency rates similar to suture anastomosis, these techniques have been associated with increased inflammation due to foreign body response, friction with erosion into adjacent tissue, tissue toxicity resulting in vessel wall necrosis, and aneurysm formation. Vascular anastomosis using thermal laser energy for tissue welding has also been described,28-31 but this technique leads to protein denaturation resulting in a weak vessel wall that is also prone to aneurysm formation.32,33
Photochemical tissue bonding (PTB) is a light-activated methodology of rapidly cross-linking tissue interfaces at the molecular level that relies on chemical, rather than thermal, reactions. A photoactive dye is applied to tissue surfaces that are brought into contact and then illuminated; the dye absorbs the light energy forming reactive intermediates that generate covalent protein-protein bonds (crosslinks), and an immediate watertight seal. 34 This study utilized Rose Bengal (4,5,6,7-tetrachloro-2′,4′,5′,7′-tetraiodofluorescein), a red halogenated xanthene dye currently FDA approved as a diagnostic agent in ocular exams to assess for conjunctival or corneal tissue change, a diagnostic for human brucellosis, and was used historically as a diagnostic agent in liver function studies.35-37 It is also currently in clinical trials to treat cancer of the liver and metastatic melanoma.38-40 Rose Bengal is a photoinitiator that facilitates crosslinking through electron transfer or energy transfer mechanisms, in the absence and presence of oxygen. 35 PTB has demonstrated the ability to seal a variety of tissues in animal models 35 including successful microvascular anastomosis in rats.41,42 Because PTB occurs at much lower power than laser welding and does not involve heating of tissues, PTB provides sealing without the adverse effects of thermal tissue damage.
Our approach to vascular anastomosis using PTB involves a small artery-in-vein cuff to increase the surface area of the bond and results in an immediate water-tight seal without intraluminal suture when performed for vascular anastomosis. A technical challenge has been the requirement for intraluminal support to correctly approximate the two tissue surfaces in the vascular cuff undergoing PTB. A proof-of-principle study of microvascular anastomosis using PTB technology utilized hollow polymer stents that facilitated water-tight sealing but resulted in increased rates of thrombosis due to increased flow resistance and the presence of a persistent foreign body, 41 thus eradicating the benefit of no intraluminal suture at the anastomosis. Herein, we describe a new technique for fixation of venous interposition graft in an ovine model of femoral artery bypass utilizing PTB at the proximal anastomosis that results in patent vascular anastomosis at 4 weeks after bypass.
Animals and Operative Procedure
Four to eight-month-old Polypay specific pathogen free sheep (n = 5; 40-45 kg) were purchased from New England Ovis (Rollinsford, NH) and acclimatized for 3 days prior to surgery in standard animal facilities at the Massachusetts General Hospital (Boston, MA). All experiments and animal care conformed to the National Institutes of Health Guide for the Care and Use of Laboratory Animals and were approved by the Massachusetts General Hospital Institutional Animal Care and Use Committee (IACUC) and the Animal Care and Use Review Office (ACURO) of the U.S. Army Medical Research and Development Command.
Prior to surgery, animals were fasted for 12 hours and hay was withheld for 36 hours. Anesthesia was induced with telazol (3 mg/kg, IM) (Patterson Veterinary, Devens, MA), xylazine (.05 mg/kg, IM) (Patterson Veterinary), and propofol (2-4 mg/kg IV) (Patterson Veterinary), and maintained with isoflurane (1-5% titrated to effect, IH) (Patterson Veterinary) and propofol (.5 mg/kg/min, IV) (Patterson Veterinary). Animals were intubated and received preoperative doses of cefazolin (40 mg/kg, IV) (Patterson Veterinary) and buprenorphine (.007 mg/kg, IM) (Buprenex, Reckitt Benckiser, Slough, UK). The bilateral hindlimbs, bilateral groins, and lower abdomen were prepped and draped in sterile fashion.
The procedure was initiated with an 8 cm transverse incision in the inguinal crease. A combination of blunt dissection and electrocautery was utilized to access the femoral vessels. The femoral artery was dissected from the deep femoral artery proximally to approximately 10 cm distal, where multiple large branches originate. Once dissection was complete, attention was shifted to harvesting the lateral saphenous vein through a 10 cm longitudinal incision on the lateral aspect of the hindlimb. The vein was dissected free and branches were suture ligated with 6-0 Prolene (RB-2 needle) (Ethicon, Inc. Somerville, NJ). After ligating the vein proximally and distally with 0 silk suture (Ethicon, Inc) and harvesting by sharp excision, the vein was flushed with heparinized saline. The lateral hindlimb incision was closed in layered fashion with 2-0 Monocryl suture (Ethicon, Inc.) and 3-0 Monocryl (Ethicon, Inc.) with topical 3M™ Vetbond™ Tissue Adhesive (3M, Maplewood, MN) applied to the skin. Systemic heparin (100 units/kg, IV) (Meitheal Pharmaceuticals, Chicago, IL) was administered after closure of the lateral hindlimb incision and 10 minutes prior to clamping of the femoral artery. The femoral artery was then clamped proximally and distally and sharply transected. A sterile solution of .1% (w/v) Rose Bengal (RB), prepared prior to surgery by dissolving solid RB (Sigma-Aldrich) in sterile phosphate-buffered saline (Sigma-Aldrich) and then passing the solution through a .22 μm filter (EMD Millipore, Burlington, MA), was then painted circumferentially on the adventitial surface of the femoral artery using a sterile cotton tip applicator. The dye was allowed to saturate for 1 minute, after which residual dye was removed with dry gauze. An atraumatic hydrophilic .018 inch straight vascular wire (Boston Scientific Corp., Marlborough, MA) was inserted through the harvested saphenous vein in antegrade fashion to avoid trauma to valves, and a Sterling™ over-the-wire balloon dilatation catheter (4 mm x 30 mm x 80 cm) (Boston Scientific) was placed over the wire in retrograde fashion and the wire removed. The balloon was inserted into the open proximal end of the transected femoral artery and the saphenous vein approximated with the transected femoral artery (Figure 1A). Four 8-0 Prolene (Ethicon, Inc) stay sutures were placed into the adventitial layer of the artery 90° apart and approximately 5 mm from the severed end of the artery. These sutures were then placed through the full thickness of the vein wall and the sutures were used to draw the saphenous vein graft into place over the transected femoral artery to form a 5 mm overlapping vein cuff (Figure 1B). It was imperative that the stay sutures remained extra-luminal on the artery to avoid any intraluminal foreign body material. A) Illustration demonstrating transected femoral artery (right) and vein graft (left) with balloon dilatation catheter inserted into femoral artery. B) Stay suture placement through arterial adventitia and full thickness of vein graft wall. C) Inflation of balloon dilatation catheter resulting in complete interface between outer vein graft and inner artery. D) Photobonding performed. E) Photobleaching of the Rose Bengal dye demonstrating photobonding has been performed successfully.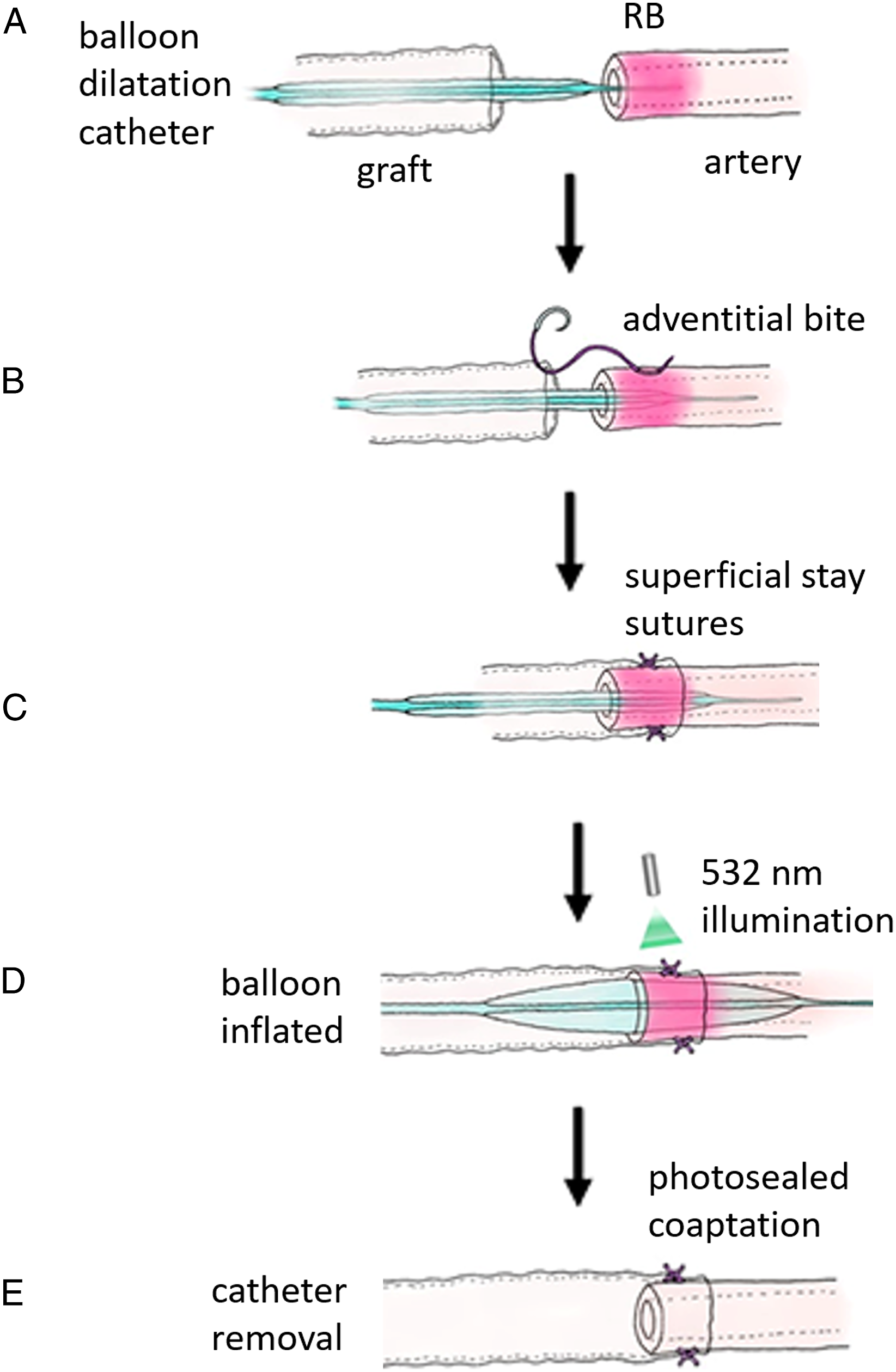
The angioplasty balloon was then inflated, resulting in a complete and intimate interface between the femoral artery and the overlying vein graft (Figure 1C). The balloon was left inflated and the anastomotic cuff was then photobonded by illumination at 532 nm from a continuous wave KTP laser (Laserscope Aura-i, San Jose, CA irradiance of .5 W/cm2) in three increments of 120o around the anastomotic circumference for 120 seconds each (Figure 1D). The angioplasty balloon was then deflated and removed (Figure 1E). The distal anastomosis was then formed with standard interrupted 8-0 Prolene™ sutures (Ethicon, Inc) 2 mm apart and arterial clamps removed. Acute patency was confirmed with doppler ultrasound. Deep and subcutaneous tissues were closed with 2-0 Monocryl suture on an SH taper needle (Ethicon, Inc.) and skin was closed with subcuticular 3-0 Monocryl suture (SH taper needle) (Ethicon, Inc.) with Vetbond™ Tissue Adhesive (3M)applied over the wound. Buprenorphine (.007 mg/kg, IM) (Buprenex) was administered every 8 to 12 hours for 72 hours, and aspirin (81 mg, PO) (Bayer Healthcare LLC, Whippany, NJ) was initiated once per day on post-operative day (POD) 1. All animals were housed in the standard animal housing facilities at the Massachusetts General Hospital and received standard grain ovine diet and water ad libitum.
Graft Harvest
On POD 28 the animals returned to the operating room, where anesthesia was induced as previously described. A combination of blunt dissection and electrocautery was utilized to access the vascular graft. Angiograms (BV Pulsera, Phillips, Amsterdam, Netherlands) were performed to confirm patency, evaluate intraluminal diameter, and assess for aneurysm formation. The graft was then sharply excised and the animal euthanized with a weight-based dose of pentobarbital sodium and phenytoin sodium (Euthasol®, Virbac, Carros, France).
Histology
Longitudinal and transverse segments of excised proximal anastomotic cuff were removed for histological examination and fixed in 10% formalin buffered phosphate (Fisher Scientific, Waltham, MA) and embedded in paraffin. From all paraffin blocks 5 μm sections were cut and staining was performed with hematoxylin and eosin (H&E) and Verhoeff stains. A board-certified pathologist unaffiliated with the study evaluated histologic specimens.
Results
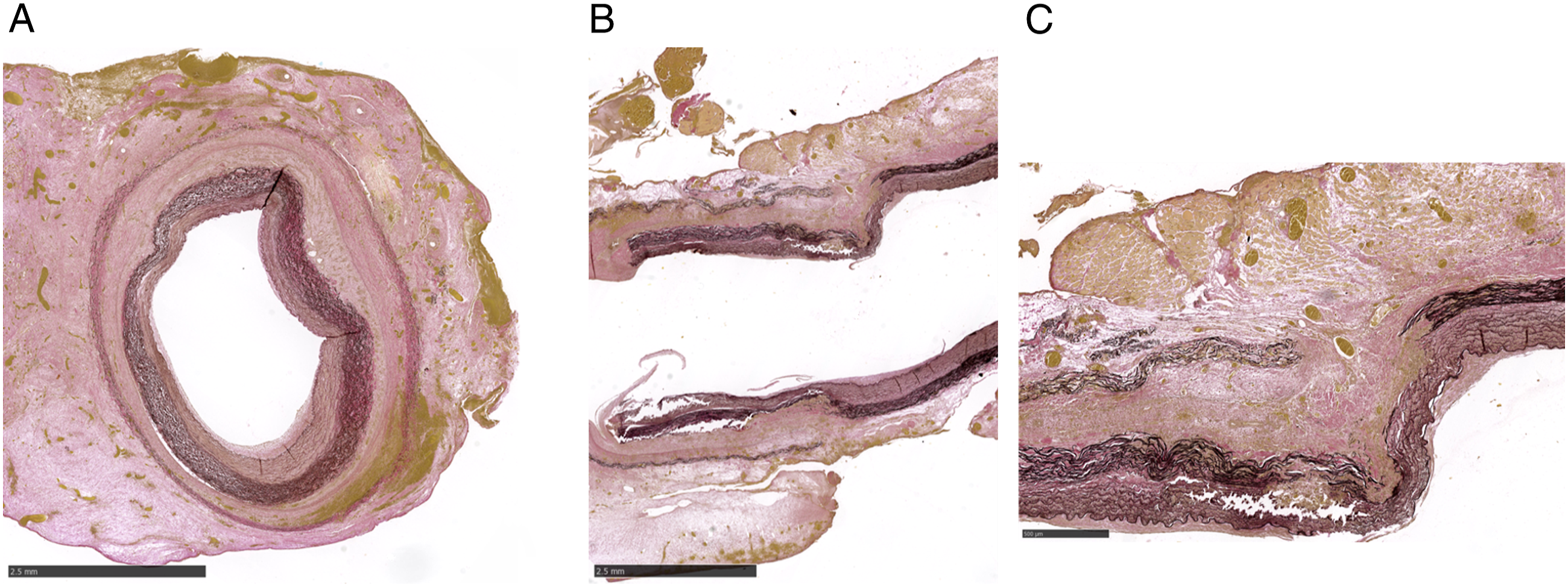
The initial PTB anastomosis was watertight and patent upon completion in all animals (n = 5). All animals survived the 28-day study duration without complication. Upon return to the operating room on POD 28, all grafts were found to be patent by Doppler ultrasound. Angiography confirmed patent grafts without formation of aneurysm. (Figure 2) Histologic examination of the excised PTB anastomosis revealed an intact venous elastic lamina and media in the outer cuff, with the venous endothelium indistinguishable from the arterial adventitia demonstrating merger of the vein with artery. (Figures 3A and B) This inconspicuous junction of the vein and artery included granulation tissue with fibroblasts at the proximal aspect of the cuff, characteristic of early remodeling of the extracellular matrix. (Figure 3B and C) The arterial media and intima were well visualized and intact, without evidence of thrombi and minimal intimal hyperplasia. Femoral angiography demonstrating patent venous bypass grafts without aneurysm. Transverse section of photochemical tissue bonding (PTB) anastomosis demonstrating fusion of the venous endothelium with the arterial adventitia. (Scale bar 2.5 mm) B: Longitudinal section of PTB anastomosis (right: proximal, left: distal) demonstrating intact venous elastic lamina over the intact arterial media, with the inconspicuous junction of vein and artery. (Scale bar 2.5 mm) C: Increased magnification of longitudinal section, better demonstrating merger of vein with artery, with fibroblasts at the proximal aspect of the cuff. (Scale bar 500 μm).
Discussion
Photochemical tissue bonding is a light-activated nonthermal tissue repair technique that has proven to consistently create a strong, immediately watertight vascular anastomosis without intraluminal suture or other persistent foreign body that remains patent in a large animal model at 28 days. We demonstrate that PTB can be safe and effective, can withstand physiologic arterial pressure (demonstrated by the absence of leak, hematoma, aneurysm, or rupture in any animal) and warrants clinical consideration.
Photochemical tissue bonding follows Carrel’s four principles of vascular anastomosis: the intimal edges are apposed, the balloon dilatation catheter ensures folds and luminal narrowing are avoided, and there is no intraluminal suture material in contact with blood. Photochemical tissue bonding also avoids needle trauma and disruption of the endothelium, potentially averting the adverse sequelae such as platelet aggregation, endothelial thickening, and intimal hyperplasia. Furthermore, following release of vascular clamps after performing an anastomosis with PTB the anastomosis was completely watertight, as described in preliminary studies. 42 This is an advantage over suture repair as anastomotic bleeding can require additional operative time for hemostasis and activation of the clotting cascade can lead to pathologic thrombosis. 43 Histologic evaluation of the PTB anastomoses reveals an anastomotic cuff with fusion of the venous endothelium with the arterial adventitia, as a result of the covalent protein-protein crosslinks. This photochemical reaction results in an immediate strong and watertight seal. Additionally, while four extraluminal stay sutures were utilized to bring the vein graft over the femoral artery in order to create the anastomotic cuff, there was no evidence of foreign body reaction in the PTB anastomosis specimens. These extraluminal sutures, placed to ensure the vein graft remained in place during photoillumination, may not be necessary and further study of this technique without extraluminal stay sutures is warranted and planned.
A limitation of the technique described herein is the requirement of intraluminal support to ensure an intimate interface between artery and vein to create the anastomotic cuff. Previous descriptions of microvascular anastomosis utilizing PTB included the use of angiocatheters 42 and hydrogel intraluminal stents 41 to provide the support required for tissue interface. By utilizing balloon dilatation catheters in this technique, we provide the ability to choose catheters of multiple diameters to fit any anatomical variation. If the dilation is too large endothelial stretch damage may occur, potentially resulting in intimal hyperplasia and stenosis. 44 On the other hand, if inadequate intraluminal support is inadequate (eg, a balloon dilatation catheter with too small a diameter) the intimate interface between artery and vein required for photobonding may not occur, resulting in an incomplete seal and anastomotic failure. This scenario can also occur with too great a size mismatch between artery and vein. In our cohort of five animals, we recorded the extraluminal diameter of the femoral artery and saphenous vein in situ prior to excision. All vessels were matched in size to within 1 mm.
The clear walled angioplasty balloon utilized for intraluminal support does potentially allow for light delivery from within the lumen (as opposed to extraluminal light delivery as described in this technique), thus eliminating one extra step in the procedure. However, light delivery to the graft interface would be less efficient due to light needing to traverse the thicker arterial wall to reach the photosensitizing dye within the vein-artery interface. The penetration of green light through tissues is thickness dependent, due to the scattering nature of tissue. 35 However, the possibility of intraluminal light delivery is intriguing and would increase the simplicity of the technique, and warrants further study.
In this study, we chose to only utilize PTB at the proximal anastomosis and perform a standard suture anastomosis distally. The vein-over-artery PTB technique at the proximal anastomosis results in continued laminar flow due to a smooth transition from artery to vein graft. Prior studies using saphenous vein grafts have indicated higher failure rates at the proximal anastomosis when compared to the distal anastomosis,45,46 likely due to the response of the vein to the arterial circulatory system as changes in hemodynamic parameters can lead to vascular smooth muscle cell proliferation, migration and vessel wall remodeling. 47 Such effects would be more pronounced at the proximal anastomosis where the pressure gradient is highest.
In summary, we have demonstrated evidence in a large animal model that PTB results in a clinically feasible, watertight and atraumatic vascular anastomosis. Our next step is to evaluate the potential benefits of PTB when compared to standard suture anastomosis, as the elimination of endothelial trauma may result in decreased intimal hyperplasia. The PTB technique is promising as an option for surgeons to create a quick and effective vascular anastomosis without endothelial damage and intraluminal foreign body and may result in an improvement in long-term vascular patency.
Conclusions
Photochemical tissue bonding can create a strong, immediately watertight vascular anastomosis that can withstand physiologic arterial pressure and remain patent at 28 days without intraluminal suture. The absence of endothelial injury and intraluminal foreign body may result in decreased smooth muscle cell proliferation, intimal hyperplasia, and vessel stenosis.
Footnotes
Acknowledgments
The authors would like to acknowledge the Knight Surgical Research Lab for veterinary tech and anesthesia assistance during cases, Joshua Tam, PhD for his contributions towards the artistic figures, Dr Jie (Jenny) Zhao, MD, PhD and the Wellman Center Photopathology core for preparation of histology and Dr Ivy Rosales, MD for interpretation of histology.
Author Contributions
Designed the study: M.A.R. and R.W.R.
Performed the operative procedures: B.B.S., M.A.R., and F.P.S.G.
Post-operative animal care, data collection and data analysis: B.B.S., F.P.S.G., and R.C.W.
Wrote the manuscript with input from all authors: B.B.S.
Overall supervision of the project: R.W.R. and M.A.R.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Henry M Jackson Foundation for the Advancement of Military Medicine, Inc. (#2018A010755)