
Abstract
Background
Laparoscopy represented one of the most innovative surgical techniques approached in the surgery field. Dexmedetomidine association with general anesthesia promotes the response control to trauma by altering the neuroinflammatory reflex, provides better clinical outcomes in the postoperative period and reduces the excessive use of drugs with risk for addiction. This trial aims to evaluate the potential drug treatment of dexmedetomidine on organic function, with the targets in neuroinflammation, perioperative pain control and blood pressure measurements in a medium-sized surgical model.
Methods
Fifty-two patients were randomized in two groups: Sevoflurane and Dexmedetomidine – A (dexmedetomidine infusion [1 μg/kg loading, .2-.5 μg/kg/h thereafter]) vs Sevoflurane and Saline .9% - B. Three blood samples were collected at three times: before surgery, 4 to 6 hours after surgery and 24 hours postoperatively. The primary outcome was inflammatory and endocrine mediators dosage analisys. Finally, we evaluated pain and opioid use as secondary outcomes, also the hemodynamic values.
Results
In Dexmedetomidine group A, a reduction of Interleukin 6 was found during 4-6 hours after surgery. A reduction of IL-10 was noted in the measurement of its values 24 hours after the procedure, with statistical significance. Also, systolic and diastolic blood pressure, as well heart rate were attenuated, and there was a lower incidence of pain and opioid consumption in the first postoperative hour (P < .0001) in the anesthetic recovery room.
Conclusions
Dexmedetomidine provided anti-inflammatory activity, sympatholytic effect and analgesia with cardiovascular safety. It reinforces the therapeutic nature of highly selective α2-adrenergic agonists when combined within anesthetic interventions.
Keywords
Background
Videolaparoscopic cholecystectomy provided a change in the line of perioperative care and represented one of the most innovative surgical techniques approached in the surgery field. 1 Accurate communication with the surgical team is essential at the beginning of the pneumoperitoneum inflation, with special attention to the intraperitoneal pressure that generates ischemia and reperfusion after its deflation. Its prolonged inflation not only causes changes in regional blood flow, but also triggers a sympathetic adrenergic response with an increase in afterload, obstruction and reduction of venous return and consequently of preload which may result in a decrease in stroke volume and cardiac output. 2
Surgical stress is characterized by an acute response to compromised bodily barrier functions by sterile injury, pathogen invasion (intestinal bacterial translocation or postoperative wound infection) and anesthesia. In aseptic trauma, the response starts with an increase in sympathetic discharge which, if unchecked, has multiple effects on homeostasis, inflammation, altering coagulation, modifying immune competence and T cell mobilization through a process mediated by β2-adrenergic receptors, increasing susceptibility to infection and reducing tissue oxygenation. The understanding that different drugs can act on receptors with specific mechanisms of action, modulating these reactions, drives the anesthesiologist to achieve better alternatives and favorable postoperative outcomes for the patient.3,4 Therefore, enhanced recovery protocols in surgery with strategic drugs and regional blocks are essential for the anesthesiologist, making the treatment with dexmedetomidine as a standalone sedative drug or as adjunct to general and regional anesthesia an attractive option for postoperative pain control. 5
Dexmedetomidine is a selective and potent α2-adrenergic receptor agonist. It acts on the activation of supraspinal pre- and postsynaptic receptors, in the locus coeruleus and dorsal horn of the spinal cord, and may influence endogenous sleep-promoting pathways by acting on the gamma-aminobutyric acid (GABA) system. 6 It’s believed that its association with general anesthesia may promote control of the trauma response by altering the neuroinflammatory reflex, the antinociception, the immunomodulation and the cholinergic anti-inflammatory pathway.7-9 However, the perspective shift on treatment of the lesion by surgical injury, previously treated as painful, now possibly with an immunomodulatory eye and its correlation with clinical outcomes in medium-sized surgical models, needs to be increasingly awakened. By attenuating the excessive release of noradrenaline during ischemia-reperfusion, with decreased potential to form reactive species of oxygen, some authors have reported a superior anti-inflammatory effect than other drugs: antiapoptotic activity, better modulation of macrophage function and reduction of pro-inflammatory mediators such as Interleukin 6 (IL-6) and tumor necrosis factor α (TNF-α).10,11 Study, in addition, demonstrated an increase in the ratio of Th17/Treg lymphocytes, wich means a decrease in the production of IL-4 and IL-10, that are cytokines of Treg cells, and a shift in the balance towards Th17 attenuating the immune response induced by surgical stress. 12
The balance between supply and demand for blood oxygen in the myocardium and a reduction in the risk of cardiac complications including ischemia/reperfusion injury, arrhythmogenesis and left ventricular dysfunction have been described with dexmedetomidine. The cardioprotective effects occur due to the inhibition of NE release at the locus coeruleus, suppressing sympathetic excitation with a consequent reduction in blood catecholamine levels, cardiac work and myocardial oxygen consumption. In addition, action in alpha-2 adrenergic receptors may prolong diastolic perfusion time, increase left ventricular coronary blood flow, reduce myocardial lactic acid release and improve myocardial resistance to ischemia and hypoxia (preconditioning). It also acts by sequentially reducing apoptosis through mechanisms involving mitochondrial functions and exercises activation of the eNOS/NO cardioprotective signaling. Study showed that the application of dexmedetomidine can reduce the incidence of ventricular tachycardia in patients who have undergone cardiac surgery, with tolerable adverse events, without increase the incidence of hemodynamic complications.13,14
The results of experimental procedures can vary substantially if the infusion dose is not standardized and its titration must be individualized for the intended clinical objective. This research describes a model of aseptic trauma in order to evaluate the clinical benefits for the anesthetic-surgical practice of dexmedetomidine administration, analyzing the behavior of inflammatory and endocrine mediators of surgical stress and their implications on pain control and hemodynamic response.
Methods
Sample Selection
This study included patients scheduled for elective laparoscopic cholecystectomy, that belonged to both genders, aged between 18 and 70 years, physical status stratified by American Society of Anesthesiologists (ASA) between 1 and 2 and who agreed to participate in the study after signing the Informed Consent Form. We established as exclusion criteria procedures converted to open surgery, since they implied an increase in surgical trauma and absence of pneumoperitoneum ischemia-reperfusion syndrome, duration greater than 3 hours, patients using illicit drugs and drugs that induce the cytochrome complex P450, patients with renal and/or hepatic failure, chronic users of corticoids and/or non-steroidal anti-inflammatory drugs, body mass index (BMI) greater than or equal to 40, heart failure, valvular or ischemic heart disease and use of tricyclic antidepressants.
The recruitment was conducted after approval by the Ethics and Research Committee of the Gaffrée e Guinle University Hospital, Federal University of the State of Rio de Janeiro (UNIRIO), Rio de Janeiro, Brazil, in December 2021(CAAE nº 50311621.0.0000) and registered on the Brazilian Clinical Trial Registration Platform (REBEC, https://ensaiosclinicos.gov.br/, RBR-2rgxbdv, last accessed on 19 January 2023), on 28 March 2022. The patients received the intervention in the mentioned hospital’s surgical facilities. The Surgery and Anesthesiology Departments are recognized by the Federal Ministry of Education and the Brazilian Society of Anesthesiology. The beginning of the data collection of the participants occurred in April 2022 and ended in October 2022.
Consented study participants were randomized by using a list of random numbers in varying block sizes on a 1:1 ratio with no restrictions to any of the two study groups: Sevoflurane and Dexmedetomidine (Group A) vs Sevoflurane and Saline .9% (Group B) (Figure 1). Randomization was performed by the nursing team together with the pharmacy sector through a schedule provided by a statistics staff. Patient data were replaced by computer-generated numbers and these codes were inserted in sealed envelopes, drawn before the infusion of the solution by the surgeon. The medicine or placebo was prepared by the pharmacist, labeled with the study subject code and physically delivered by the pharmacy staff to the anesthesiologist (G.N.S) performing the infusion. The infusion management was blinded to the anesthesia and surgical teams, patients and clinical investigators. The nurse allocated each patient with the indicated envelope immediately upon your arrival in the operating room. After preparing the study drugs, the pharmacy staff and the nurse exposed to the allocation was not involved in any part of the conduct of the research. The evaluation of postoperative pain scores was performed by a anesthetist of the clinical staff who wasn´t part of the study. CONSORT flow diagram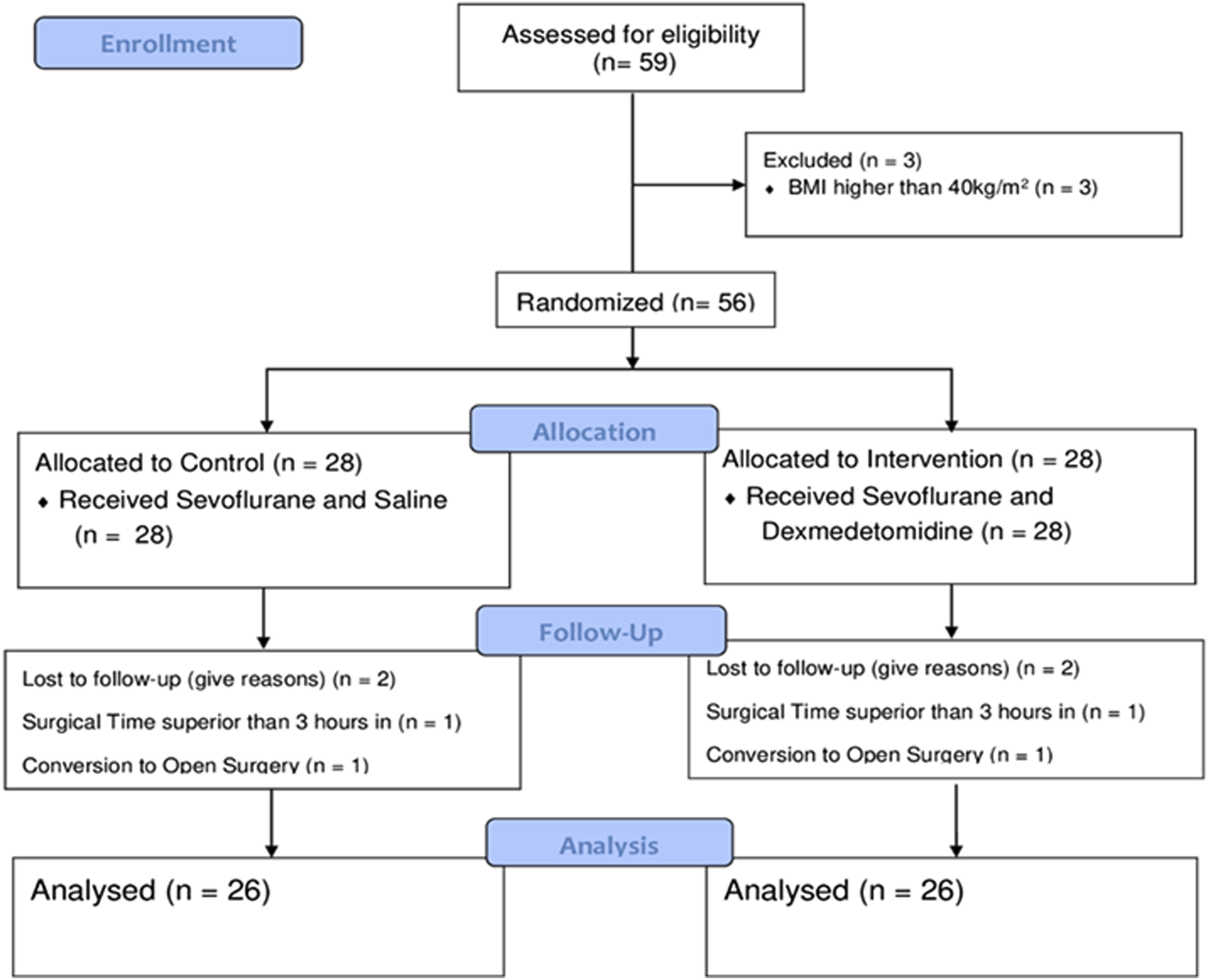
This manuscript adheres to the applicable CONSORT (Consolidated Standards of Reporting Trials) guidelines. 15
Anesthetic Technique Standardization
All patients upon admission to the operating room were monitored according to the recommendations of the ASA, guaranteed peripheral venous access with 20 or 18 gauge peripheral intravenous catheter. The anesthetic drugs and their dosages were standardized so that there were no differences between the groups. Induction of general anesthesia: fentanyl (5 mcg/kg), lidocaine (1.5 mg/kg), propofol (2.5 mg/kg) and cisatracurium (.15 mg/kg) intravenous. After an endotracheal tube was placed and position was confirmed, positive pressure ventilation was started with tidal volume 6-8 ml/kg and the respiratory rate was titrated to maintain the end-tidal CO2 between 35 and 45 mmHg. Intraoperative maintenance: sevoflurane 1 to 1.5 MAC with oxygen 30% and air 70%. Bispectral index was maintained between 40 and 60 during the operation. All patients received dipyrone at a dose of 30-50 mg.kg-1 and ketoprofen 100 mg intravenous at the end of surgery, in addition to infiltration of the surgical portals with ropivacaine .3%, volume of 15 mL. Additional doses of opioids were not given intraoperatively. In the immediate postoperative period, at the anesthetic recovery room, patients received intravenous opioid (morphine 0.05 - 0.1 mg/kg, intravenous) in moderate to severe pain (Visual Analogic Pain Scale). For prophylaxis of nausea and vomiting, ondansetron 8 mg intravenous was administered in the intraoperative period. The only difference was that in Group A, after venoclysis, the infusion of dexmedetomidine 1 mcg/kg for 20 minutes was started, followed by .2 - .5 mcg/kg/h until surgical closure. In Group B, a placebo solution with .9% saline similar to dexmedetomidine was infused.
Hemodynamic fluctuations between the two groups were compared through variations in heart rate (HR), systolic blood pressure (SBP) and diastolic blood pressure (DBP) before the procedure (time 0), during anesthetic induction (and subsequent 25 minutes), surgery and awakening.
Laboratory Assay
Three venous blood samples were collected at three times (T): T0h before surgery in the preoperative room, T4-6h after surgery and T24h postoperatively close to hospital discharge. We measured in all samples: interleukin-6 (IL-6), interleukin-10 (IL-10), cortisol, C-reactive protein and glycemia. They were centrifuged at 2000 rpm for 15 minutes and stored in the biorepository at - 80°C in cryotubes in the Immunology and AIDS Research Laboratory at the University Hospital. The measurement of results was performed at the laboratory of the Programa Nacional de Controle de Qualidade (PNCQ) in Rio de Janeiro after 6 months from the beginning of data collection. Serum concentration of IL-6 was determined by electrochemiluminescence immunoassay using the Roche Cobas e411® immunoassay analyzer. The quantification of IL-10 in plasma was determined applying the ELISA technique, using the “Human IL-10 ELISA Set” kit (BD, Pharmigen, San Diego, CA), following manufacturer’s instructions. Briefly, plates were sensitized with overnight anti-IL-10 capture antibody, to 4°C. The samples were added to each well, after washing and blocking nonspecific sites. Anti-IL-10 capture antibody was added to the wells. The reaction was revealed with streptavidin-horseradish peroxidase conjugate (SAv-HRP), using 3.3’,5.5’-tetramethylbenzidine and Hydrogen Peroxidase as a substrate. Recombinant human IL-10, at concentration of 500 pg/mL, was used to construct standard curves. Serum concentration of CRP was determined by a Roche® immunoturbidimetric assay using the Bioclin 3000 automated analyzer. Blood glucose values were determined by colorimetric enzymatic assay - GOD - PAP (Trinder) Roche®, using the automatic analyzer Bioclin 3000. Serum concentration of cortisol was determined by chemiluminescence immunoassay (CLIA) Roche®, using the Abbott Architect i1000 immunoassay analyzer.
Outcomes
The primary outcomes included the behavior of Interleukin 6(IL-6), Interleukin 10 (IL-10), Cortisol, C-reactive protein (CRP) and Glycemia in the perioperative period of this surgical modality, elucidating the treatment and protective mechanism of dexmedetomidine in the inflammatory response to trauma.
The secondary outcomes were the pain management, opioid use and hemodynamic variables behavior between the groups. The quality of analgesia was evaluated by two factors: the amount of opioid (morphine) used 1 h, 6 h and 24 h after awakening and the gradation of pain measured by the visual analogic pain scale at these times after extubation. The recorded values were divided into the following pain categories: No pain - 0; Slight - 1 to 3; Moderate - 4 to 6; Severe - 7 to 10.
Statistics
This study was designed to detect a difference in perioperative plasma level of endocrine and inflammatory mediators between the groups, aiming to reach a satisfactory Cohen effect size for the variables. The sample size was estimated to compare medians and proportions, with a statistical power of 80% for all variables (except IL-6 and blood glucose in some ranges) and a significance level of 5% (α = .05). Considering the patient’s eligible criteria and the desired power, we reached a minimum sample size of 52 patients (26 patients per group), similar to study with approximate design. 12
For the variables that follow a Normal distribution for the control and intervention groups by the Shapiro-Wilk test, the t-test was chosen. For comparison of medians and quantitative variables the non-parametric Mann-Whitney test was used. Considering the qualitative or categorical variables, the non-parametric Chi-square test was chosen. Some study variables were presented strongly correlated, having been the ones that had a correlation above 70%, showing linear dependence: IL-6 and CRP. The results were postulated as median (1st and 3rd quartiles) for each variable used. All analyses were performed using R software version 4.0.3 (R Project for Statistical Computing, Vienna, Austria).
Results
Fifty-nine patients were selected for the study, but seven were excluded: two patients due to surgery lasting longer than 3 hours, two due to conversion to open surgery and three due to BMI greater than 40. In the end, 52 patients were eligible, divided into two groups: Sevoflurane and Dexmedetomidine - Group A (n = 26) vs Sevoflurane and Saline .9% - Group B (n = 26), assuming equal sizes for the two groups of interest. The CONSORT flow diagram is shown in Figure 1.
Demographics and Clinical Data.
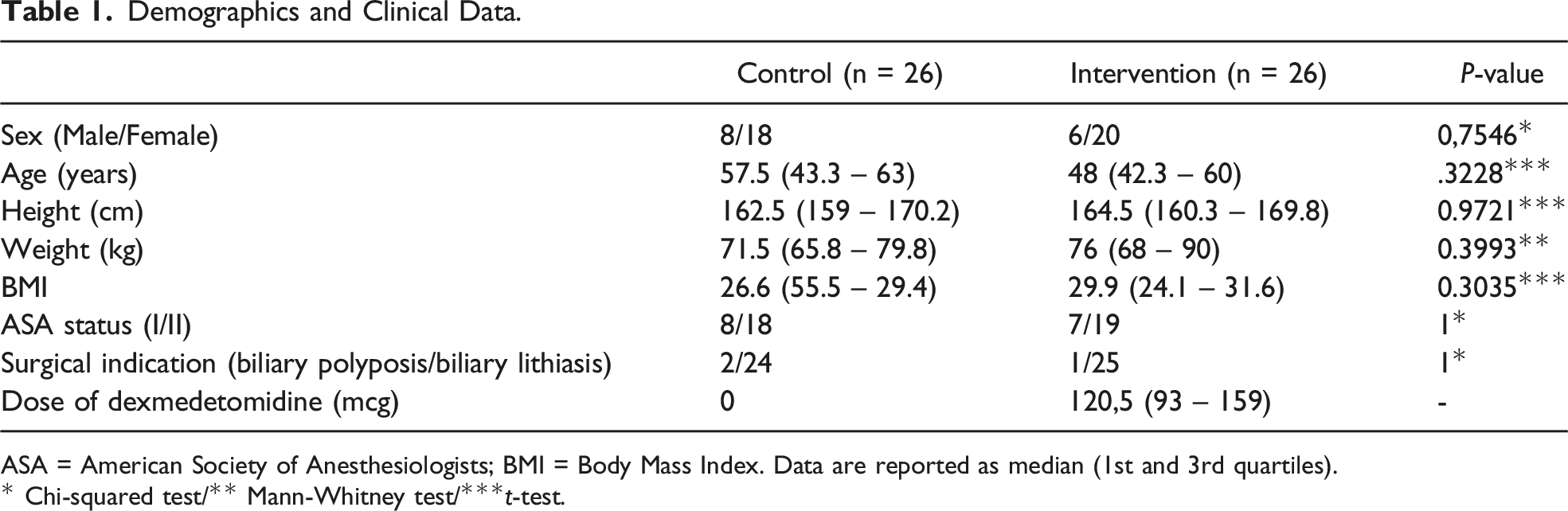
ASA = American Society of Anesthesiologists; BMI = Body Mass Index. Data are reported as median (1st and 3rd quartiles).
* Chi-squared test/** Mann-Whitney test/***t-test.
Results From Hypothesis Tests for the Non-demographic Variables of the Study.
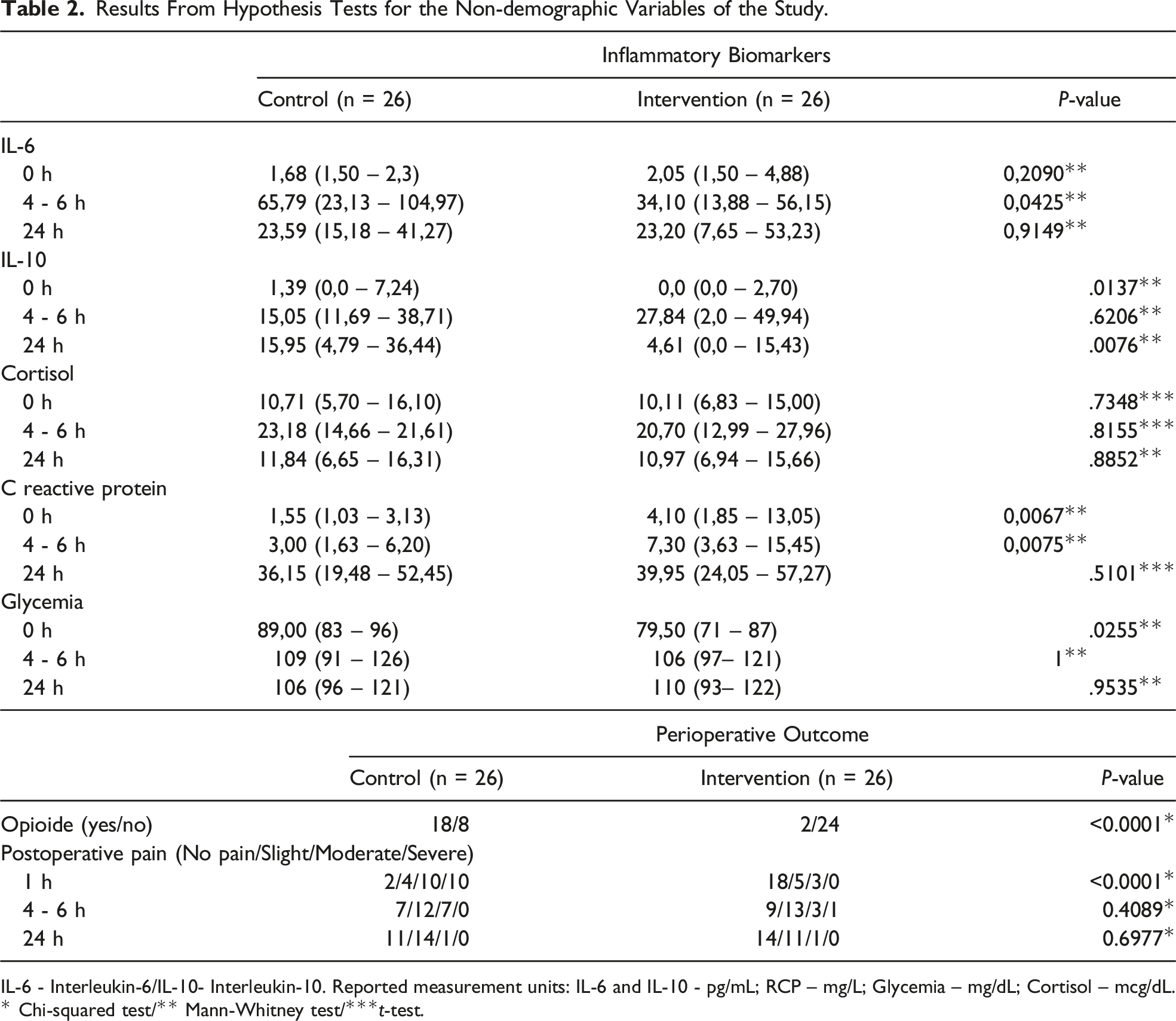
IL-6 - Interleukin-6/IL-10- Interleukin-10. Reported measurement units: IL-6 and IL-10 - pg/mL; RCP – mg/L; Glycemia – mg/dL; Cortisol – mcg/dL.
* Chi-squared test/** Mann-Whitney test/***t-test.
Surgical time was similar between groups, lasting less than 3 hours. The occurrence of pain and opioid use was higher in the first hour after surgery in the control group. None of the patients developed bradycardia or significant hemodynamic instability requiring suspension of medication infusion in the intraoperative period. A buffering for IL-6 at 4-6vhours after surgery was found in the intervention group, demonstrating biological effect of alpha-2 blockade on immune response with statistical significance Group B [65.79 (IQR 23.13 - 104.97)] vs Group A [34.10 (IQR 13.88 - 56.15)] P = .0425 (Figure 2). Boxplots & Graphs from the variable IL-6. Note that the median, represented by the central line of each of the boxplots, at 4-6 hours after surgery, showed more distant values between the control and intervention groups than for the other periods recorded. At the 5% significance level, there was a statistical difference between the groups. Graphs: values observed by patient for IL-6 for each measurement time between groups.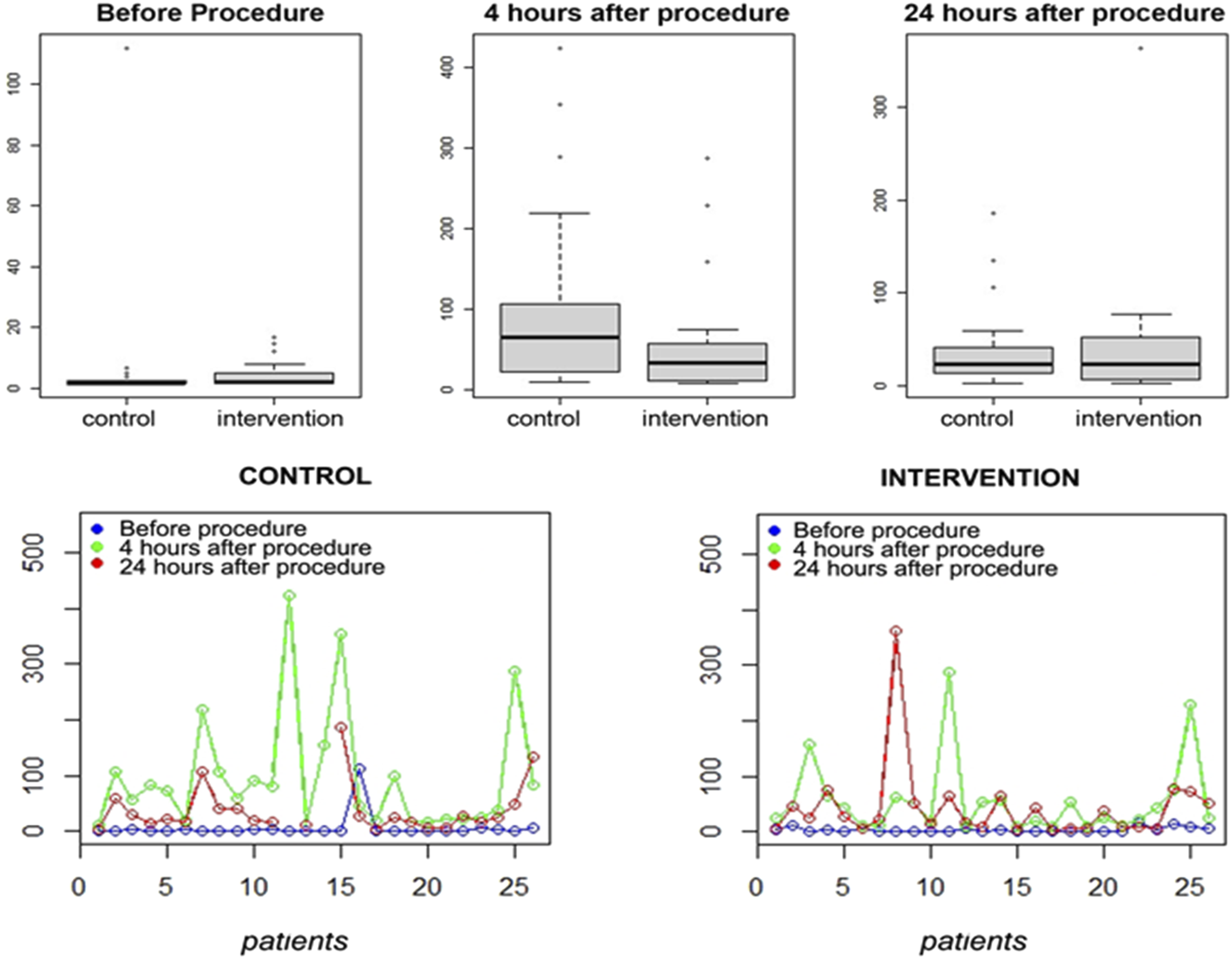
In addition, there was an increase in IL-10 values 4-6 hours in the intervention group and a subsequent reduction in the measurement of its values 24 hours after the procedure, with statistical significance B [15,95 (IQR 4.79 – 36.44)] vs A [4.61 (IQR 0.0 – 15.43)] P = .076 (Figure 3). Boxplots & Graphs from the variable IL-10. Note that the median, represented by the central line of each of the boxplots, at 24 hours after surgery, showed more distant values between the groups than for the other periods recorded. At the 5% significance level, there was a statistical difference in A group. Graphs: values observed by patient for IL-10 for each measurement time between groups, demonstrating, after treatment, an attenuation of values close to hospital dis-charge.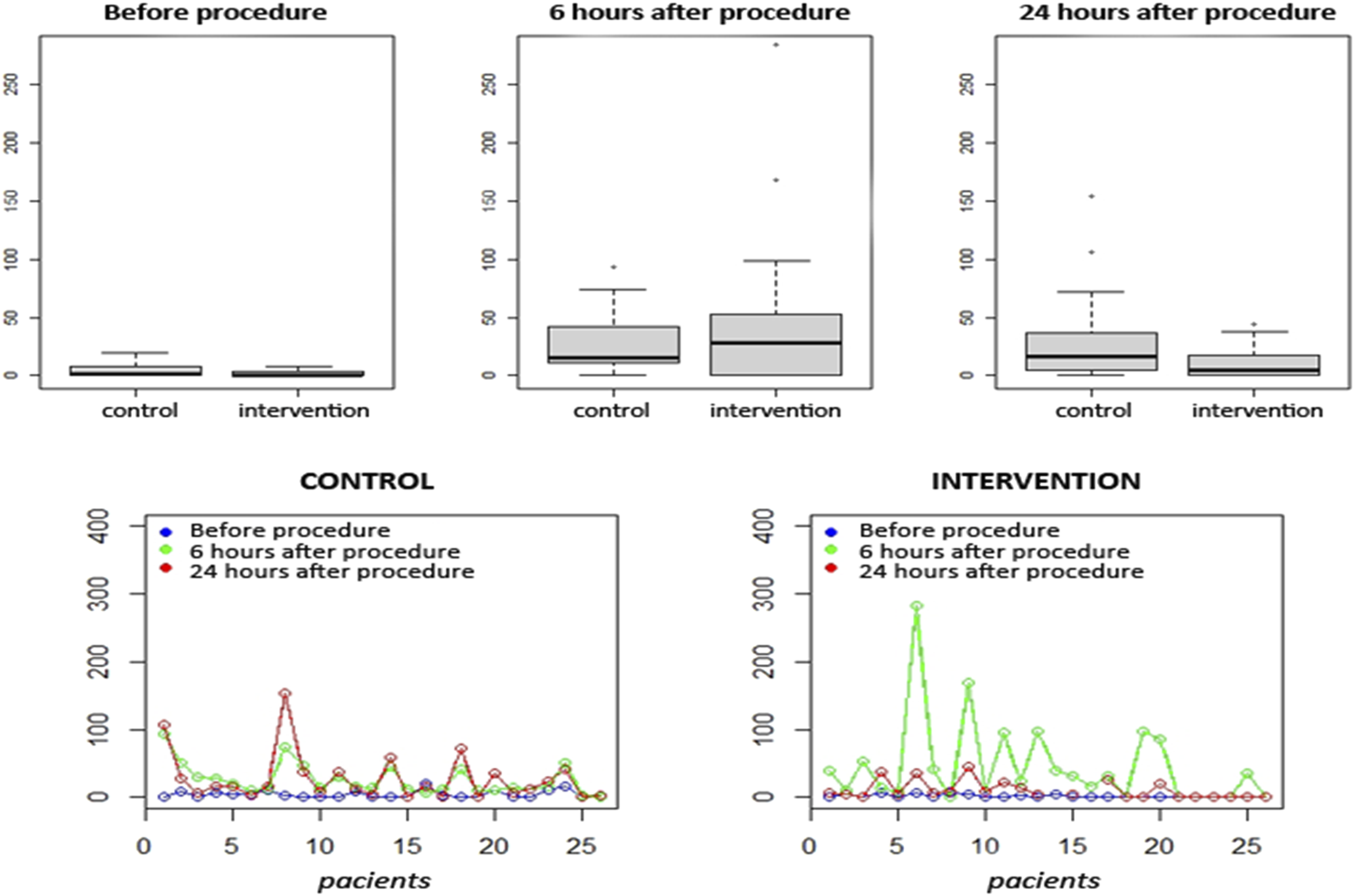
It was noticed that the elevation of CRP remained postoperatively in both groups and results indicated that the intervention with dexmedetomidine alone was not enough to change the endocrine response to surgical trauma. There was no difference between the groups when serum cortisol and blood glucose levels were compared postoperatively (Table 2).
Results From Hypothesis Tests for the Hemodynamic Variables of the Study.
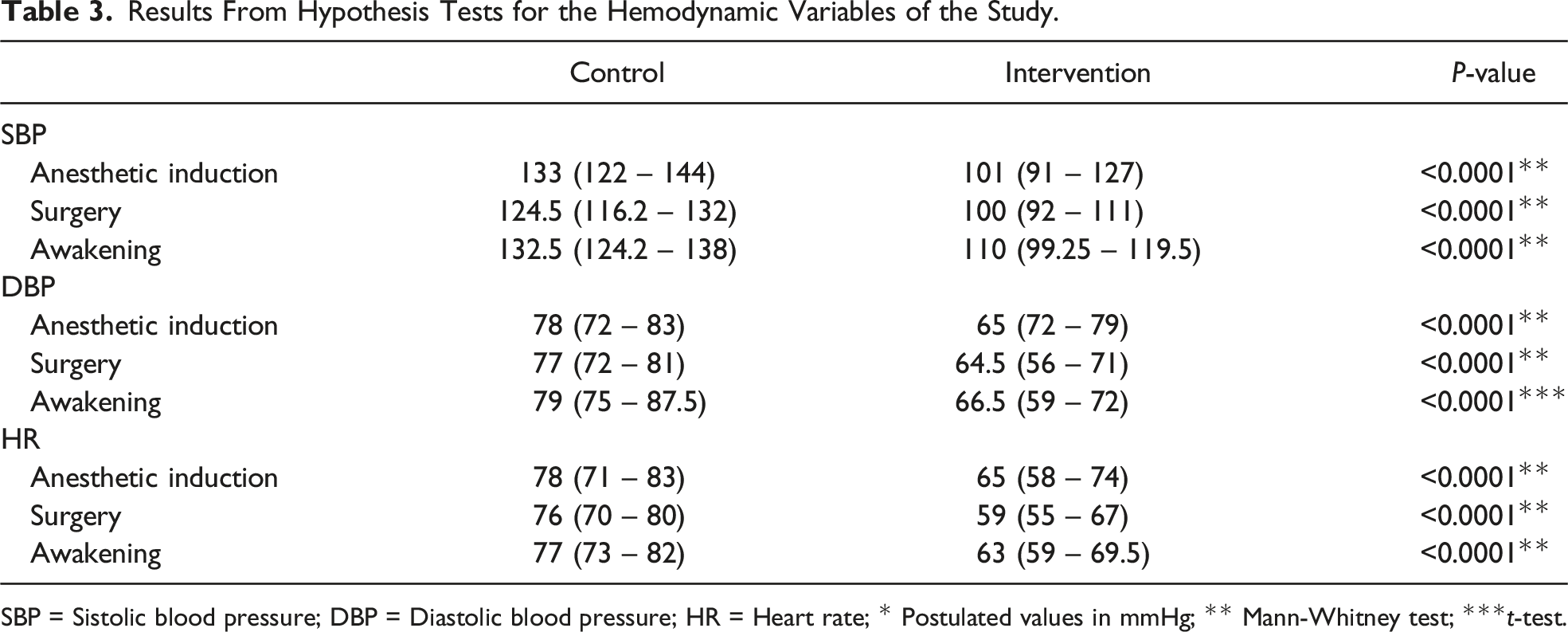
SBP = Sistolic blood pressure; DBP = Diastolic blood pressure; HR = Heart rate; * Postulated values in mmHg; ** Mann-Whitney test; ***t-test.
The P-values calculated using the Chi-square test for operative outcome variables were significant for opioid necessity and category of postoperative pain 1 hour after the procedure performed. For the 1 h time, the groups showed a statistical difference in opioid consumption (P < .0001) and pain score (P < .0001) with lower opioid use and pain scores in A group. For the 4 h and 24 h times, there was no difference between the groups.
Discussion
The immunotherapeutic properties of dexmedetomidine are being widely studied. Three hypotheses can explain these treatment mechanisms: regulation of cytokine production by immune system cells, antinociception and alteration of the cholinergic anti-inflammatory pathway by central sympatholytic effect.6,8,16-18 Innate immunity cells are capable of expressing alpha-2 adrenoreceptors on their cell membrane. Blocking adrenergic tone on effector tissues can contribute to modulation of cytokine production by lymphocytes, macrophages and monocytes during the stress response and reductions in serum levels of pro-inflammatory cytokines such as IL-6, IL-8 and TNF-α over a period of up to 24 hours after surgery. The control of immune and inflammatory reactions, with fine tuning between pro- and anti-inflammatory cytokines, are essential to minimize major pathological damage in various settings such as trauma, sepsis and cancer.7,19,20
IL-6 is a marker of inflammatory response to surgical trauma that induces synthesis of acute phase reactants by the liver, stimulates neutrophil production in the bone marrow and promotes differentiation of T helper cells producers of IL-17. It is produced by macrophages, dendritic cells, endothelial cells, fibroblasts and other cells in response to Pathogen-associated molecular patterns (PAMPS) and also to IL-1 and TNF. The innate lymphoid cells of group 2 are activated in response to the epithelial cell-derived cytokines, IL-33 and IL-25. These cells release mediators associated with a Th2 response, such as IL-6. Its serum increase directly reflects the magnitude of stress, as in sepsis, resulting in mitochondrial dysfunction, glycocalyx disruption and endothelial dysfunction implying increased morbidity and mortality.21,22 We found a buffering in the graph for IL-6, 4-6 hours after surgery in the intervention group, demonstrating biological effect of alpha-2 blockade on immune response with statistical significance B [65.79 (IQR 23.13 - 104.97)] vs A [34.10 (IQR 13.88 - 56.15)]; P = .0425 when compared to control group.
IL-10-producing regulatory Natural Killer cells act as innate inflammatory effectors during the early stages of infections (represented by IFN-g production) and acquire immunoregulatory and anti-inflammatory capacity posteriorly during the injury. This interleukin favors the maintenance of epithelial and endothelial barrier integrity by blocking IL 6 and IL-8. It was noticed that IL-10 is essential for the spontaneous expansion and apoptosis modulation of mast cells. In addition, it has dual effects in its activation: acceleration and suppression. Although rapid activation is required for immediate immune responses, including protection against infections, the excessive and/or unnecessary activation of these cells can lead to the development of allergic diseases. Therefore, the role of IL-10 in the cell activation control is essential for a rapid immune response providing tissue homeostasis.23-25 In our study, we noticed, in the perioperative period, an initial increase in IL-10 and subsequent immunoregulation with a statistical reduction in its values with treatment, 24 hours after surgery: B [15.95 (IQR 4.79 – 36.44)] vs A [4.61(IQR 0.0 – 15.43)]; P = .076 when compared to control group. This fact signalizes an improvement in the inflammatory response.
Studies have shown that dexmedetomidine did not provide adequate protective effect on stress hormones (epinephrine, cortisol). 26 This may be due to its main mechanism of action being via hyperpolarization of noradrenergic neurons of the locus ceruleus, unlike other drugs. 27 However, when combined with other adjuvants, such as propofol in continuous infusion, it can effectively alleviate the stress response of patients undergoing laparoscopic cholecystectomy and potentiate the stabilization of perioperative hemodynamics. 28 Our results also indicated that the treatment with dexmedetomidine, as a single agent, was not sufficient to alter the endocrine response. There was no difference between groups when cortisol and glycemia serum dosages were compared in the postoperative period.
The anti-inflammatory cholinergic pathway activation is a survival mechanism to attenuate sympathetic effects during surgical trauma. The reflex, via the vagus nerve, by which its afferent fibers detect inflammatory mediators and transmit these signals to the dorsal motor nucleus, generates an efferent signal and release of ACh on α-7 nicotinic receptors on the surface of macrophages and cells of innate immunity. This vagal pathway suppresses local and systemic inflammation by inhibiting the release of pro-inflammatory mediators, including IL-1β, IL-18 and TNF-α.29,30 Treatment with dexmedetomidine has been shown pre- and post-conditioning capacity with cardioprotective effects by reducing cell necrosis and apoptosis, and attenuation of mitochondrial dysfunction. In this context, the sympatholytic effect and anti-inflammatory signaling pathways activation, that confer protection against hypoxia-ischemia injury may provide therapeutic activity after ischemia and reperfusion during pneumoperitoneum in video laparoscopic surgeries.13,14 In our study, SBP, DBP and HR values were significantly lower in Group A, that is, greater stability of blood pressure variables.
Abusive use of opioids has become a worldwide public health crisis. Between 2001 and 2006, the number of opioid-related deaths in the United States increased by 345%. Therefore, its controlled use in the postoperative period is of paramount importance. 31 Several studies have demonstrated the efficacy of dexmedetomidine in controlling postoperative pain. It is associated with improved quality of postoperative recovery and reduced opioid consumption in the immediate postoperative period. These factors not only make dexmedetomidine an attractive agent for enhanced recovery in surgery (ERAS) protocols, as well as for patients with acute and chronic pain.32,33 For the 1 h time, the groups showed a statistical difference in opioid consumption (P < .0001) and pain score (P < .0001) with less opioid use and lower pain scores in the intervention group (Table 2). It is further considered in pain management as a strategy to decrease opioid use/abuse and as adjuvant with other drugs, in regional and neuroaxis blocks in order to increase duration and analgesic quality.34-36
The study had some limitations. First, it failed to evaluate dose-dependent changes in the protection of specific organs by means of markers of protection such the antiapoptotic regulatory pathways of postoperative cognitive dysfunction. Second, the effects of different doses of dexmedetomidine on the anesthetics and analgesics consumption during surgery were not analyzed in this study. Third, the sample size may have prevented achieving statistical difference and power of 80% for other variables analyzed, although the reduced volume of elective surgeries during the COVID-19 pandemic and the low availability of supplies indirectly affected the sampling.
Conclusions
The inflammatory response to trauma is influenced by numerous factors and the neuroinflammatory eye is considered of paramount importance and often neglected. In this trial, we can say that the association of dexmedetomidine with general anesthesia for laparoscopic cholecystectomy damped the inflammatory response by decreasing the release of IL-6, the main pro-inflammatory mediator, in the immediate postoperative period. In addition, we noticed a reduction in IL-10 close to hospital discharge, also demonstrating an immunotherapeutic effect on immune response to trauma. This experiment demonstrated the benefits of using alpha-2 agonists in the perioperative period due to their analgesic and sympatholytic effects, with cardiovascular safety. There was better control of decisive clinical parameters in the management of aseptic trauma, and it can be considered and indicated in video laparoscopic surgeries. Its use is linked to less opioid consumption in the immediate postoperative period in overuse times, becoming an assertive option for the anesthesiologist to pain management.
Supplemental Material
Supplemental Material - Immunotherapeutic Properties of Dexmedetomidine on Pain Management and Cardiovascular Function in Videolaparoscopic Cholecystectomies: A Randomized, Two-Arm, Double-Blinded, Placebo-Controlled Trial
Supplemental Material for Immunotherapeutic Properties of Dexmedetomidine on Pain Management and Cardiovascular Function in Videolaparoscopic Cholecystectomies: A Randomized, Two-Arm, Double-Blinded, Placebo-Controlled Trial by Gustavo Nascimento Silva, Virna Guedes Brandão, Marcelo Vaz Perez, Sandoval Lage Sobrinho, João Gabriel de Cerqueira Campos Villardi, Priscilla Mendonça do Sacramento, Luiz Claudio Pereira Ribeiro, and Rossano Kepler Alvim Fiorelli
Footnotes
Acknowledgements
The authors would like to thank Cleonice Bento (biomedical researcher, Department of Biomedicine, Federal University of Rio de Janeiro) for her professionalism and critical review; Luiz Cláudio (head of the Laboratory of Research on Immunology and AIDS at GGUH) for storing the samples in appropriate conditions; and the staffs of the Surgery/Anesthesia Division of Universitary Hospital, for their support in the logistics of surgical routines and careful patient selection.
Author Contributions
Conceptualization, G.N.S., V.G.B., and M.V.P.; methodology, S.L.S., J.G.C.C., and R.K.A.F.; software, J.G.C.C.; validation, G.N.S., L.C.P.R. and S.L.S.; formal analysis, R.K.A.F. and S.L.S.; investigation, J.G.C.C.; resources, G.N.S., V.G.B., P.M.S., and L.C.P.R.; data curation, P.M.S.; writing—original draft preparation, R.K.A.F.; writing—review and editing, G.N.S., V.G.B., and M.V.P.; visualization, V.G.B., P.M.S., S.L.S., and L.C.P.R.; supervision, R.K.A.F.; project administration, G.N.S., V.G.B., M.V.P.; funding acquisition, G.N.S., V.G.B. and R.K.A.F. All authors have read and agreed to the published version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the authors. The physical structure and supplies used were provided by Gaffrée e Guinle Universitary Hospital, Federal University of the State of Rio de Janeiro (UNIRIO), Rio de Janeiro, Brazil.
Ethical Statement
Informed Consent
All patients/participants or their relatives provided their written informed consent to participate in this study.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.