
Abstract
Background
Robotic-assisted surgery (RAS) is widely adopted, and understanding the learning curve (LC) is crucial for surgeons self-assessment and credentialling. We characterised the transition from laparoscopy to robotic approach for three experienced surgeons based on analysis of colectomies performed for malignancy.
Methods
We analysed retrospectively all consecutive robotic colon cancer surgeries performed between February 2020 and April 2025. We excluded rectal cancer resections, palliative, multivisceral and beyond TME cases. The cumulative summation (CUSUM) methodology was utilised to graphically represent the colectomy LC based on total operative time.
Results
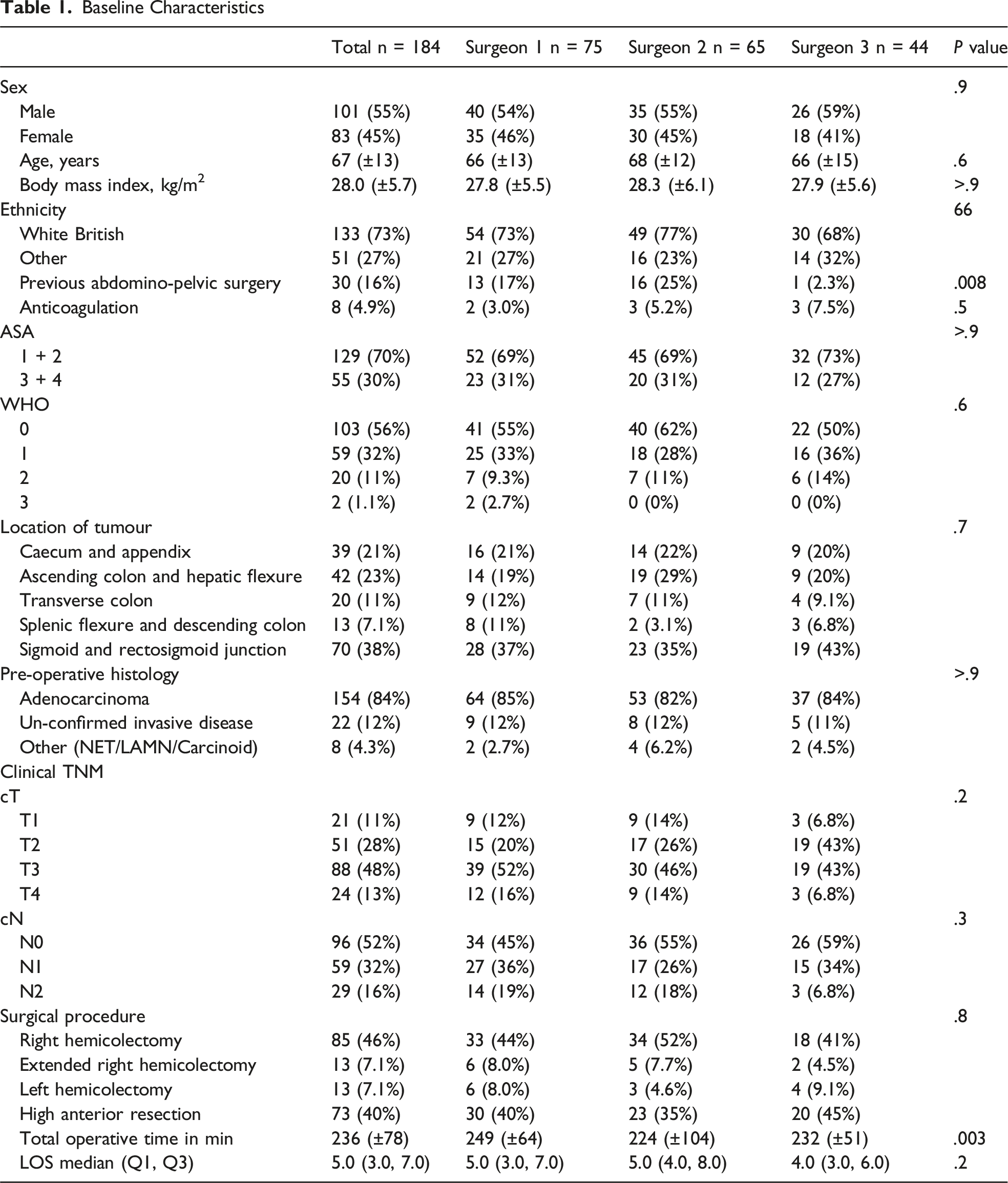
Our analysis included 184 colectomies: 75 performed by surgeon 1, 65 by surgeon 2, and 44 by surgeon 3. Demographics data and tumour characteristics were comparable between surgeons, exempt from operative time and previous abdomino-pelvic surgery (P < .05). The CUSUM curve revealed a three-phase pattern: a learning phase (cases 1–16), a competence phase (cases 17–29), and a proficiency phase (beyond case 30). The median total operative time trended downward from the learning phase (240 min) to the proficiency phase (218 min), though this was not statistically significant (P = .13). We also observed a trend towards reduced estimated blood loss (109 mL to 86 mL, P = .066) and a decrease in 30-day re-admission rates from 14% to 4% (P = .11) in the proficiency phase.
Conclusion
We present our department LC with the DaVinci Xi Robot for surgical treatment of colonic cancer. Based on our calculations, it is necessary for a surgeon to perform 30 robotic cases to reach the proficiency part of the LC of RAS for colonic resections.
Background
One of the latest GLOBOCAN report states that colorectal cancer (CRC) is the most prevalent gastrointestinal (GI) malignancy worldwide, with an incidence of 1.9 million (9.6%) among all GI cancers and the highest mortality of 904 019 (9.3%).1,2 Current literature suggests that nearly 75% of newly diagnosed CRC cases present with stage I, II, and III disease; therefore, radical resection is the optimal approach.2,3 Due to inherent advantages such as less surgical trauma, faster return to normal activities, and decreased postsurgical morbidity, minimally invasive surgical (MIS) techniques such as laparoscopy have gained popularity, gradually replacing conventional open surgery and representing the current standard of care worldwide.4-6
A promising platform for the surgical treatment of CRC in XXI century is the surgical robot.7,8 Robot-assisted surgery (RAS) has gained popularity, especially in developed countries, as it overcomes many of the limitations of laparoscopy, such as decreased dexterity and operator tremor, while offering high-resolution three-dimensional visualization. 9 Compared with the laparoscopic approach, RAS offers stability and enhanced dexterity because of the presence of articulated instruments that mimic the movement of the surgeon’s hands. These factors increase the precision of dissection and reduce surgeons’ fatigue, eventually enhancing the quality of surgery and patient outcomes. 10 The effectiveness, feasibility, and safety of robotic platforms have facilitated the wide adoption of RAS in the Western population, particularly in limited spaces such as pelvic surgery. 7
The debate regarding the superiority of RAS over traditional laparoscopy continues, despite its increasing use in medical practice worldwide. A limited number of randomized controlled trials have yielded conflicting evidence regarding the efficacy of RAS.11,12 A previous retrospective study from our centre supplements this literature, reporting that the robotic approach is equally effective (non-inferior) to laparoscopy in surgical treatment of CRC. Despite the fact that the reported cohort included initial learning curve (LC) procedures, there was a statistically higher lymph node yield and, although not statistically significant, a shorter hospital stay than the laparoscopic approach. 13
Despite the presence of various articles reporting the outcomes of RAS for CRC treatment, there is a significant lack of data regarding the rate at which surgeons achieve proficiency within a certain robotic platform in a non-selected real-world setup. Based on the experience of surgeons worldwide when they began laparoscopy, the adoption of RAS as a novel surgical technology requires a LC. Similar to laparoscopy RAS LC is defined as the accession and improvement of a competence while operating on a certain robotic platform over a certain period.14,15 Certain surgery-related variables were measured and recorded over time, serving as a proxy for assessing performance in a series of cases. Based on these parameters, the LC can be graphically displayed using a minimum of four data points. 16
Surgical literature often uses Cumulative Sum control chart method or CUSUM analysis of the total operative time (TOT) for consecutive robotic operations in order to graphically depict the learning phases of surgeons. 17 The CUSUM methods is multidimensional and visually identifies changes in a surgeon’s performance.14,18 Analysing this LC and its application in developing proficiency in RAS for CRC offers essential insights to gain essential data to structure training. Also this guided surgeons efficiently as they convert from laparoscopy to RAS. 18 Therefore, it is crucial to understand this to optimise patient outcomes and ensure the safety and effectiveness of the technology.
Surgical LC analysis is often complicated by many factors one of the main being the varied nature of cases. Particularly within colorectal speciality, where both case complexity and patient anatomy can differ significantly. While both complete mesocolic excision (CME) for colon cancer and total mesorectal excision (TME) for rectal cancer are standardised procedures, the inherent anatomical differences and distinct pathological challenges make their LCs distinct and incomparable.
The LC for rectal cancer surgery, for instance, is usually steeper and longer.19,20 This is largely due to the challenges of pelvic dissection and the frequent use of preoperative neoadjuvant therapy, which can obscure tissue planes. Combining rectal cancer cases with colectomy cases would introduce a significant confounding variable, potentially leading to a misleading assessment of a surgeon’s true learning progression.
Similarly, the variable nature of inflammatory bowel disease (IBD) or diverticular disease surgery, characterised by dense scar tissue and inflammation, makes a standardized LC analysis for these procedures difficult. Unlike cancer surgery, which follows distinct fascial planes, IBD surgery requires a different skill set to navigate a pathologically altered environment.
To ensure a more accurate and representative characterization of the LC for a new surgical platform, our study focused exclusively on robotic colectomies for malignancy. This approach minimised confounding variables and allowed for a clearer, more precise illustration of skill acquisition in a specific, repeatable procedure. This paper aims to outline and describe our group’s LC for robotic colectomy within our Trust by focusing on three surgeons transitioning to the new platform.
Using CUSUM analysis, we delineated the LC and identified metrics and indicators to evaluate and establish the number of cases required to reach proficiency. Moreover, by analysing our curve, we identified factors that affected our LC trajectory, such as previous laparoscopic experience, patient selection, complexity of surgery, and training of senior registrars and fellow surgeons. The results of this audit of practice could potentially aid in the refinement and improvement of current robotic training programs, and in establishing criteria for patient selection and perioperative care. In addition, insights into the learning process for RAS within our trust can optimize surgical outcomes to ensure that patients receive high-quality care.
Methods and Materials
Design
We performed an audit of all colorectal robotic procedures performed within our NHS high volume Trust between February 2020 and April 2025. In our analysis, we included cases operated on using the robotic Davinci Xi platform for confirmed colon cancer or highly suspicious growths without conclusive histopathological invasion showing radiological evidence of malignancy. Rectal cancer procedures, palliative, multi-organ, and exenterative cases as well as cases performed for benign indications were excluded. Our study adhered to the Strengthening the Reporting of Cohort Studies in Surgery (STROCSS) criteria. 21
Variables
Data on demographics, including age, sex, body mass index (BMI), ethnicity, American Society of Anesthesiologists (ASA) classification, and World Health Organization (WHO) performance status, were collected from charts and electronic medical records. Tumour characteristics and intraoperative parameters were recorded, including tumour location, TNM staging, clinical stage, surgical procedure, TOT, and conversion rate or changes in the surgical approach.
Perioperative outcomes were assessed, and procedural morbidity were recorded. This was classified according to the Clavien-Dindo classification. Anastomotic leaks were identified based on the clinical or radiological evidence of anastomotic dehiscence. Prolonged ileus was defined as the absence of bowel function after surgical procedures lasting longer than 4 days. Length of inpatient stay (LOS), 90-day surgical readmission rate, mortality, and specimen characteristics. In particular, we recorded the resection status and number of lymph nodes.
Outcomes
The primary outcome was to construct colon cancer LC for three experienced colorectal surgeons who passed the LC using a robotic platform utilising CUSUM analysis.
The secondary outcomes included a comparison of short-term patient outcomes across the surgical performance phases based on CUSUM graph analysis.
CUSUM Analysis
CUSUM method is a sequential statistical method used to identify changes in the process mean values. 14 Many medical professionals commonly use this technique to estimate LCs through sequential calculations of total deviations between individual data points and mean values. 22 Upward and downward trends in the CUSUM graph indicate significant changes and can signal consistent patterns across data points. Conversely, a lack of consistent change is characterized by sporadic fluctuations around the zero line, with no pronounced deviations. CUSUM charts were constructed based on the TOT. 18
Statistical Analysis
The statistical analyses were performed using the IBM SPSS Statistics for Windows version 23 software (SPSS, IBM, Chicago, IL, USA) and MS Excel (Microsoft Corporation). The chi-square test was used to examine the associations between categorical variables. If the restrictions of the chi-square test were not met (when the expected frequencies in any of the contingency table cells were less than five), the conclusions were confirmed using Fisher’s Exact Test. Analysis of Variance (ANOVA) was used to compare means. The non-parametric Kruskal–Wallis test was used when the assumptions of normality were not met. The threshold for statistical significance was set at P < .05. Regression analysis was used to identify the slopes of different learning phases.
Ethical Statements
This study was conducted in compliance with the principles of the Declaration of Helsinki. The institutional ethics committee review did not require ethical approval for this study. This study is a service-delivery evaluation of the use of robotics in the treatment of CRC within the department. No consent was obtained from the patients.
Local Setup
Our Trust comprises two large district general hospitals in England that serve diverse populations from a wide range of social and ethnic backgrounds across Northeast London. All elective cases are operated within Surgical Elective Hub which is recognized as one of the first eight institutions in the country to be accredited by the Getting It Right First Time (GIRFT) national scheme. 23
The department is supported by seven dedicated colorectal consultants who collectively perform over 260 colorectal resection procedures annually, with a minimally invasive approach offered as the primary surgical option in all amenable cases.
Driven by the colorectal department’s commitment to adopting RAS as a standard of care, our trust initiated its robotic program within the Surgical Elective Hub in February 2020. Following a comprehensive training program endorsed by Intuitive Surgery and proctored competency assessments, three out of six colorectal surgeons achieved proficiency in RAS on the Xi platform. The comprehensive program incorporated several key elements, commencing with e-learning modules, to establish foundational knowledge. Subsequently, surgeons engaged in extensive virtual simulation, accumulating over 30 h of practice on robotic surgical simulators. Practical skills were further developed through participation in specialized workshops, specifically TR200 and TR300 courses. To gain real-world experience, surgeons undertook observational visits at established high-volume centers, namely, the Champalimaud Foundation and St Mark’s Hospital. The initial surgical experience was supported by proctorship in the first seven to eight cases, ensuring expert guidance during the critical early phase of the LC. Continuous assessment of surgical performance was performed through ongoing proctor support and rigorous data collection and analysis, which are integral to routine clinical practice. Our centre has adopted the Xi platform as its primary system with no prior RAS experience.
Results
Between February 2020 and April 2025, 363 colorectal procedures were performed by the surgical team within the Trust (Figure 1). One hundred eighty-four cases were included in final analysis. The study period encompassed UK COVID-19 lockdowns, which reduced the overall surgical volume. Flow Chart of Colorectal Procedures Performed Between 1.2.2020 and 30.04.2025 Using the Robotic Platform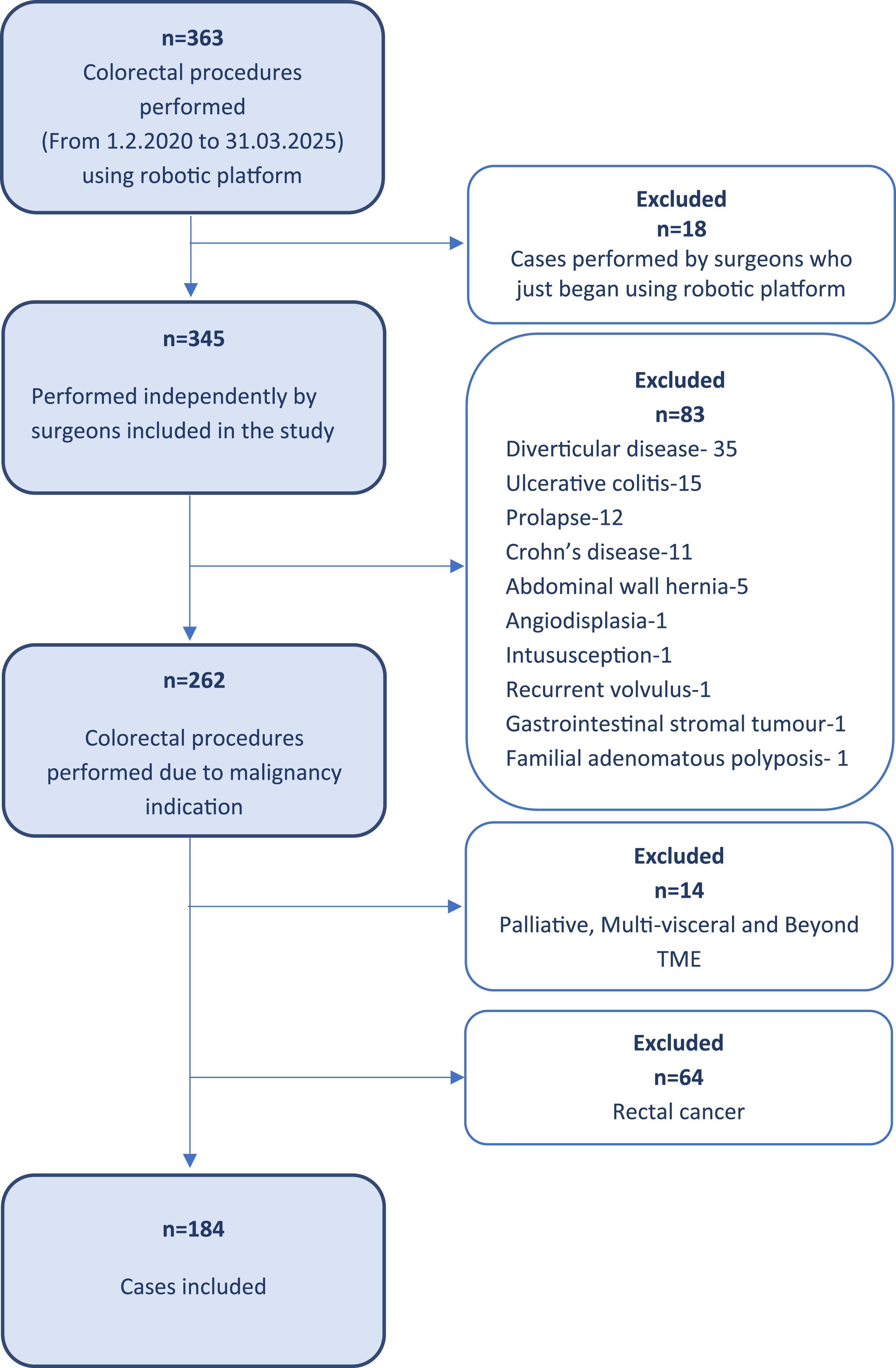
Baseline Characteristics
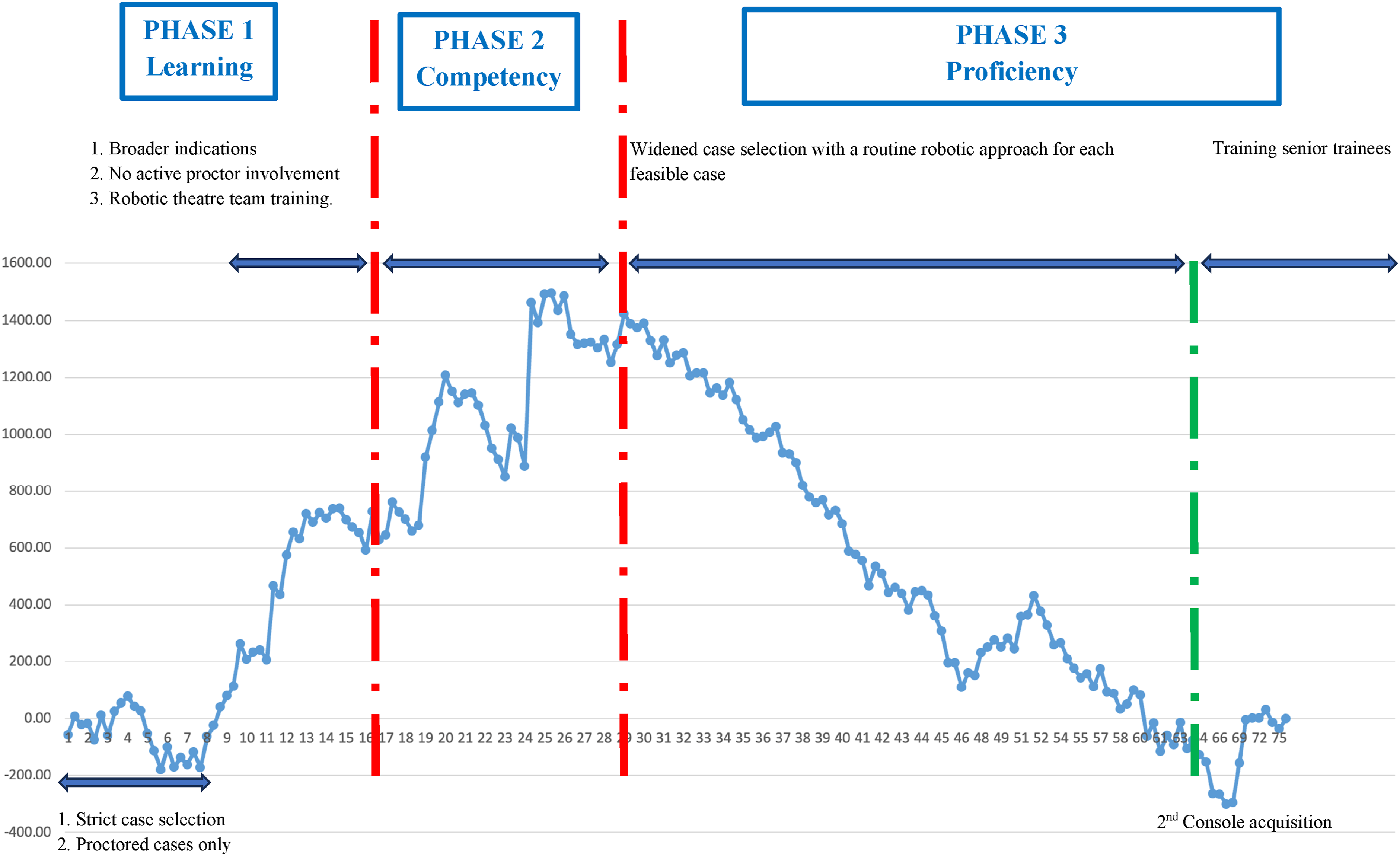
To graphically represent our LC, a CUSUM chart was produced using the total operative time and CUSUM analysis formula (Figures 2 and 3). Cumulative Sum (CUSM) Calculation Formula Graphical Representation as Graph of Cumulative Sum (CUSUM) Analysis Studying Total Operative Time
All three surgeons’ cases (Surgeon 1, n = 75; Surgeon 2, n = 65; and Surgeon 3, n = 44) were arranged chronologically. The first case of total operative time for Surgeon 1 was matched with that of Surgeons Two and Three, which were performed chronologically in all cases. Surgeon Three completed only nine instances in the third-proficiency phase.
The cumulative sum (CUSUM) graph of the total operative time was calculated using the following formula (Figure 2):
Visual inspection of the CUSUM curve allowed us to identify the transition points between these three phases. The CUSUM graph trend slope was positive in cases 1–16 (βst = 0.79, P < .001), with positive and negative oscillations from cases to 17–29 (βst = −0.51, P < .001), and transitioned to a steeper negative slope in cases beyond 30 (βst = −0.70, P < .001). Although after visual analysis of the curve we see oscillations, overall visualization represents three phases that correspond to the learning, competency, and proficiency phases described in the literature.14,18,24
Operative Characteristics and Short-Term Outcomes Characteristics. Cohorts are Divided Based on the CUSUM Curve
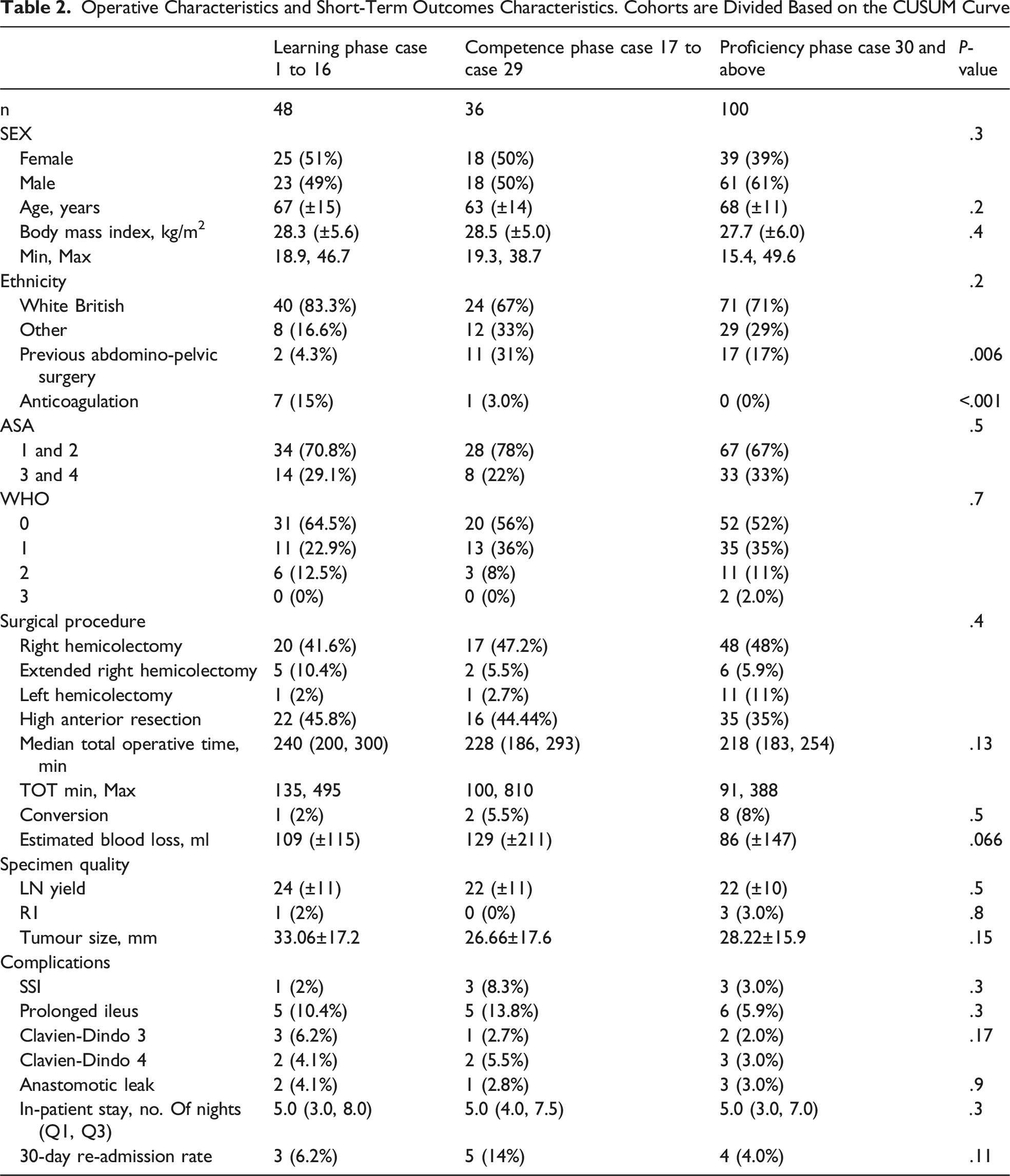
A trend towards a higher proportion of patients with ASA 3 and 4 was observed during the proficiency phase than during the competence and learning phases. However, this difference was not statistically significant. In addition, a decreasing trend in the mean total operative time was observed across the phases, which was not statistically significant.
Thirteen patients experienced Clavien-Dindo grade 3-4 complications, including six anastomotic leaks, all of which required surgery with defunctioning. Although this difference did not reach statistical significance, it may be attributed to the increased complexity of the cases included in individual phase.
In our cohort, we reported two cases of Clavien-Dindo grade 5, both of which were related to COVID-19 infection.
Eleven procedures were converted: two to laparoscopy early in the LC for splenic flexure mobilisation and nine to open surgery, primarily in the later stages of the LC when patient selection bias was minimal. The indications for conversion included advanced disease requiring multiorgan resection (five cases), intraoperative bleeding necessitating open haemostasis (two cases), and physiological intolerance to pneumoperitoneum (two cases). For the entire cohort, the mean operative time was 236 min. The median length of hospital stay (LOS) was 5 days. Twelve (6.5%) patients were readmitted within 30 days.
Discussion
With three surgeons now offering the robotic approach as the primary option for elective practice, evaluating their LCs provides valuable insights for our unit. Using the CUSUM statistical method, we aimed to analyse the LC for RAS in the surgical treatment of colon cancer at our centre, focusing on TOT as an indicator of operative competency, displayed graphically across identified phases, and correlated with the process components of our learning. Understanding the relationship between robotic surgical proficiency and the number of consecutive robotic procedures performed can inform other centres seeking to replicate a successful transition to robotic colorectal surgery.
The challenge in defining the LC for robotic colectomy performed for cancer stems from wide heterogeneity in reported study design, surgical experience prior to embarking on RAS and case selections together with patient factors.24,25 Certain systematic reviews suggest a surgeon needs between 20 and 70 RAS resectional procedures with a mean of 45 to see of the CUSUM graphs statistically significant reduction within TOT and postoperative complication rate.24,25 This broad range is influenced by factors such as the surgeon’s prior MIS experience, the complexity of cases, the structure of institutional training as well as available support. 26 One strategy to accelerate this skill acquisition is to start with simpler procedures, such as hernia, cholecystectomies or colectomy surgery. In right sided colectomies for instance some studies report that after 16 cases performed you will be able to see drop in the TOT compared to 25 for laparoscopic approach. 27 However, this benefit disappears for more complex procedures, which show similar learning thresholds (42 or 45 cases) for both modalities. 28 Implementation of enhanced recovery protocols may also influence the LC as some studies report faster patient recovery and shorter LOS with robotic colectomies even during the early phase of adoption.29,30
By visualizing our colectomy CUSUM curve, we identified three distinct phases: learning, competence, and proficiency. These phases aligned with the model described by Nasseri et al. 18 Our CUSUM graphs revealed slope changes in cases 16 and 29, delineating three distinct phases of the LC. The primary learning period focused on developing technical skills with the da Vinci Si system, including docking, instrument handling and three-dimensional visualisation. This period involved strict case selection for the first eight cases, gradually broadening thereafter, without active proctor involvement after case 8–10. It also encompasses the proactive development of non-technical skills for operating surgeons and familiarization of robotic team members and their roles in the robotic theatre list. In Case 17, based on the CUSUM graph, the surgeons transitioned to the competence phase, marked by a plateau-type oscillating slope, indicating stabilized performance. A steeper downward trend in operative time in cases beyond 29 suggested a gradual improvement as surgeons gained experience and entered the proficiency phase, which subsequently returned to baseline performance levels when all three surgeons began teaching surgical trainees and obtained their second console. Teaching duties may have influenced the operative times in this phase, potentially increasing them.
Overall, the statistical analysis of the cohort divided by CUSUM graph slope changes revealed no significant differences. Operative time showed a downward trend with a non-statistically significant level of postoperative complications, confirming an efficiency comparable to that of published data.
Among the existing studies on robotic LCs, only Bokhari et al 24 examined a broader spectrum of colorectal cases performed by a single experienced laparoscopic surgeon, including rectopexy, abdominoperineal resection, anterior resection, and low anterior resection. Nasseri et al also described their LC.18,24 Parisi et al 31 reported a three-stage LC for robotic colorectal surgery based on 108 cases, with the initial stage encompassing the first 44 cases. Raimondi et al 32 study of 23 consecutive cases identified two stages via CUSUM analysis, with the initial stage requiring 13 cases. The current literature indicates heterogeneity in RAS LCs for CRC, potentially due to variations in case numbers and prior minimally invasive surgical experience as well as inclusion of both colonic and rectal resections within the same cohort. Despite this, studies consistently noted a downward trend in operative time and blood loss, alongside increase in specimen quality, suggesting continuously growing RAS efficiency and surgeon expertise. Within our group, a downward trend in operative times, albeit not statistically significant, was observed, along with a comparable level of postoperative complications to published data, confirming the efficiency of the surgical approach.
The LC of RAS is dependent on the technical skills of the operating surgeon and the experience of the robotic theatre team, which differs from that of traditional laparoscopy. As the team progresses along the LC, key metrics such as docking time, console time, and overall operative time tend to decrease . TOT is the most widely used variable in the literature to assess the LC, serving as a reflection of the technique’s adaptability and competitiveness. This underscores the critical role of team experience and case complexity as factors that influence mastery of robotic surgical systems. The LC in RAS can be significantly shortened through consistent self-auditing by the surgeon and the surgical team after each procedure. The team can improve the efficiency and results by thoroughly examining the surgical procedures to detect improvement opportunities and technique refinement. Robotic systems provide specific benefits for mid-to-low rectal cancer surgeries because their iterative process decreases operative bleeding and enhances specimen quality. As the learning process evolves and the robotic team gains experience, coupled with a better understanding of the RAS principles, this leads to shorter operative times with better precision, which establishes the ability to evolve and engage in more complex cases. 33
Our study contributes to expanding the literature on robotic surgical learning. Upgrade to a dual console system after the proficiency phase improved training practices without compromising patient outcomes. This retrospective study of three experienced colorectal surgeons transitioning from laparoscopy to a robotic approach had several advantages. From what we can gather, our series for robotic colectomy LC is the largest reported from a district general hospital in England which is providing a realistic representation of the LC for surgeons with prior extensive MIS experience.
The authors acknowledge the several limitations of this study. A primary limitation is the retrospective design of the data analysis, while a self-explanatory flowchart was used to address the issue of selection bias, the study retrospective nature still presents inherent challenges. Additionally the impact of operating room staff involvement such as robot docking and instrument exchange could not be fully considered as within our database the docking time represent an incomplete dataset. We look to include these parameters within our further studies. We intend to submit further work in the future with a larger dataset focusing solely on rectal resection to allow for independent LC assessment as well as to refine our understanding of this long-term LC.
In conclusion, our CUSUM graph presents our centre’s experience of transitioning from a laparoscopic to a robotic platform for colon cancer treatment. Based on our calculations, it is necessary for a surgeon to perform 30 robotic colectomy cases to transition to the proficiency phase of the RAS.
Footnotes
Ethical Considerations
The study was conducted in accordance with the Declaration of Helsinki and presented and approved as an audit of colorectal robotic practice by the governance meeting of the department. This is a service delivery evaluation of the use of robotic platform within treatment of colorectal cancer in our Trust. Institutional ethics committee review did not require ethical approval for this study as this was not considered research by the NHS Health Research Authority Checklist.
Author Contributions
Conceptualization: VB, AM, NR. Data curation: VB, JH, OP, AM, SK, JH, RB, NR, Formal analysis: VB, AM, SK. Funding acquisition: N/A. Investigation: All authors. Methodology: VB, AM, SK, JH, RB, NR, Project administration: VB, AM, SK, JH, RB, NR, Visualization: VB, AM, SK, JH, RB, NR, Writing–original draft: VB, AM, SK, JH, RB, NR, Writing–review & editing: VB, AM, SK, JH, RB, NR. All authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Fully anonymised datasets used and analysed during the current study are available from the corresponding author upon reasonable request.