
Abstract
Background
Early innovations are often disruptive but gain traction when the benefits become evident. EXtended Reality (XR) has recently gained momentum for surgical training. XR involves a head-mounted display (HMD) blending physical and digital worlds for enhanced visualization, communication, and understanding. To understand its potential impact, the receptiveness of plastic surgeons was assessed for its usefulness and usability.
Methods
Plastic surgeons watched XR interventions and completed a survey assessing applications for remote consultation, intra-operative education, and pre-operative planning. Responses were analyzed using descriptive statistics and categorical inferential testing, with group differences assessed using Fisher’s exact test on dichotomized Likert responses.
Results
Eleven attending and ten resident physicians (21/44, 48%) responded to the survey. Attendings perceived greater usefulness of XR for virtual consultation than residents (91% vs 50%), with a near-significant trend (P = 0.056) and higher reported mean usefulness and usability scores. Residents more often anticipated need for technical support during virtual consultation (60% vs 27%). Both groups strongly endorsed XR for intra-operative education. Willingness to use and optimism were high among both groups. For pre-operative planning, both groups perceived XR as useful, though usability concerns were prominent, including moderate perceived complexity and anticipated need for technical support particularly among residents (89% vs 70%).
Conclusion
Attendings were more receptive than residents to integrating XR in plastic surgery training with residents reporting greater cognitive load. Residents valued improved intra-operative visibility and noted the Hawthorne effect. Selecting high-value, usable XR applications while minimizing trainee role stress is essential for advancing residency education.
Introduction
The promise of eXtended Reality (XR) applications in surgery has abounded over the last 20 years, covering many applications from simulation/training to intra-operative decision-making to predicting operative outcomes. 1 Optimistic results have touted these technologies as transformative, including significantly reduced patient pre-operative anxiety, improved surgical efficiency, and better surgical outcomes.2-4 Current literature has recognized barriers to adoption, like increasing costs, security and privacy concerns, and latency challenges.5-7 This leaves Academic plastic surgeons with pros and cons to consider when evaluating these new interventions.
To prove its utility, new technology must sufficiently address a tangible need, offering improvements over the current practice model. These improvements include time saved, increased confidence and competence, better clinical outcomes, richer data capture/transmission to a decision-maker, enhanced communication and collaboration, better patient experience, and cost-effectiveness. New interventions must also meet the user’s needs in terms of usability to ensure its viability. Usability can be defined as the extent of friction a user must adapt to extract the promised value of the intervention over the status quo. Academic plastic surgeons must balance usefulness and usability when deciding if and what XR interventions are worth pursuing. However, this answer alone is insufficient to predict adoption in academic medicine.
This work aims to identify 3 activities within an academic plastic surgery program where resident training could be improved. We seek to answer the usefulness vs. usability inquiry based on the well-established Technology Acceptance Model (TAM) that has been described as one of the most influential models of technology acceptance, especially applied to newer healthcare adoption categories of telemedicine and mobile applications.8,9 Further, this study aims to elucidate why even favorable XR interventions may (and often do) fail to achieve widespread adoption. We hypothesize that the adoption potential of new technologies, defined by a combination of its usefulness and usability, will differ meaningfully between attending and resident physicians.
Methods
This study was approved by the University of Michigan Medical School Institutional Review Board (HUM00213488). Three interventions were chosen in a single section of plastic surgery throughout April 2022 and all were conducted prospectively. The first aimed to enhance consult training and resident evaluation via a teleconsult model. A resident physician wore an Iristick head-mounted device (HMD) into an emergency department room to evaluate a new facial fracture (Figure 1). The interaction was recorded and live-streamed to a craniofacial fellow in another part of the hospital, who assessed and offered guidance on the resident’s history-taking and physical exam. The case was staffed with the attending craniofacial surgeon, who later reviewed the recorded Iristick teleconsult and provided feedback and advice to the resident and fellow physicians for future consults. The recording was also saved as educational preparation material for future resident physicians to utilize before joining that service. Remote clinical teaching using the Iristick HMD. A resident’s streamed point-of-view during an Emergency Department consult allows supervising faculty to observe the physical exam in real time and provide immediate educational feedback, even when off-site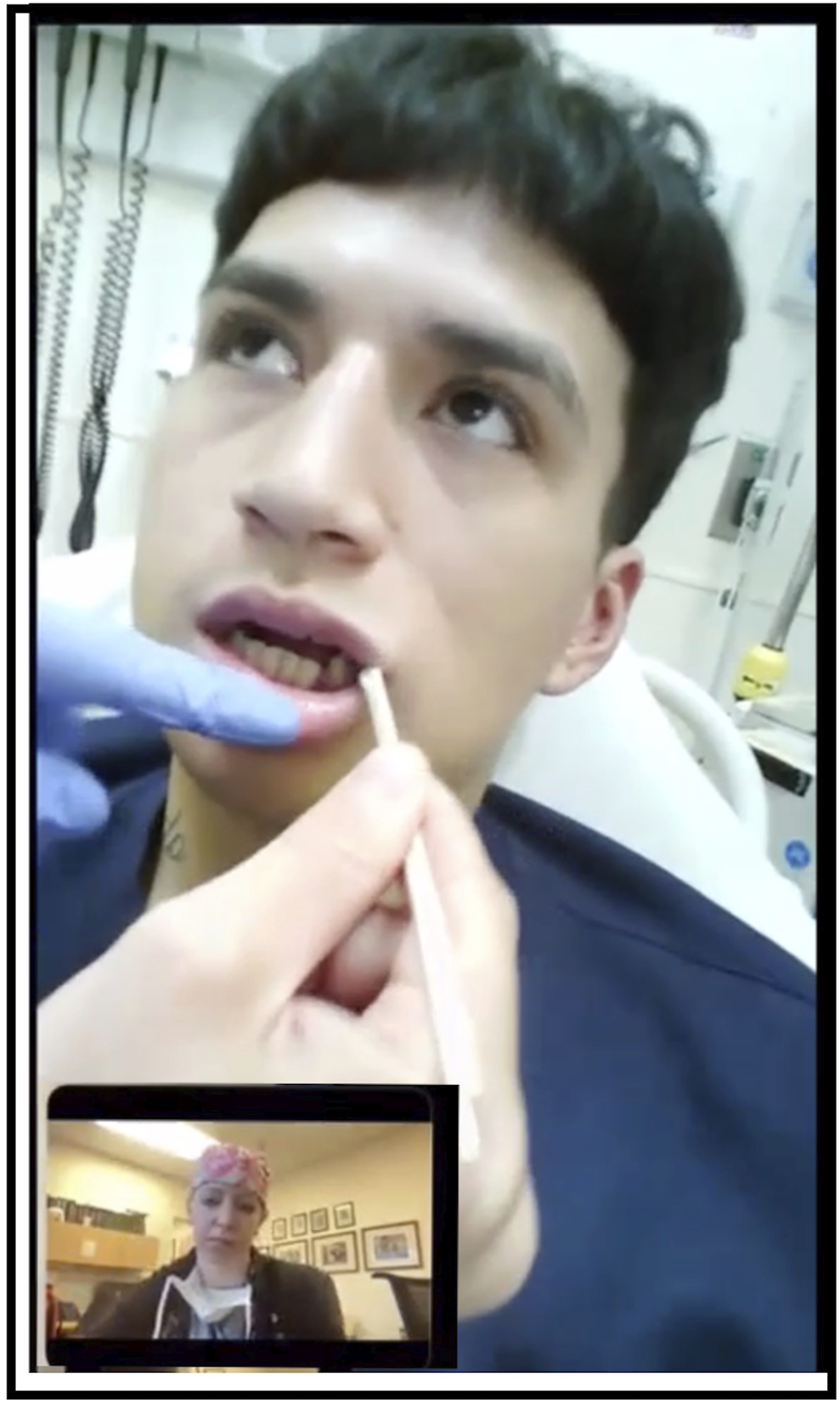
The second intervention aimed to enhance intra-operative learning; the attending craniofacial surgeon wore an Iristick HMD during a cleft lip repair, with residents and medical students assisting in person. The surgeon’s view was projected onto all displays in the operating room so all in-person attendees could see through his first-person view (Figure 2) and was live-streamed to remote medical students who could observe and ask questions. The live stream was recorded for asynchronous access and learning by other trainees in the future. Educational applications of the Iristick HMD. Left: A physician wearing the device during a teaching encounter. Right: The corresponding streamed view, demonstrating how learners and remote supervisors can share the physician’s visual field to facilitate procedural advising and decision-making education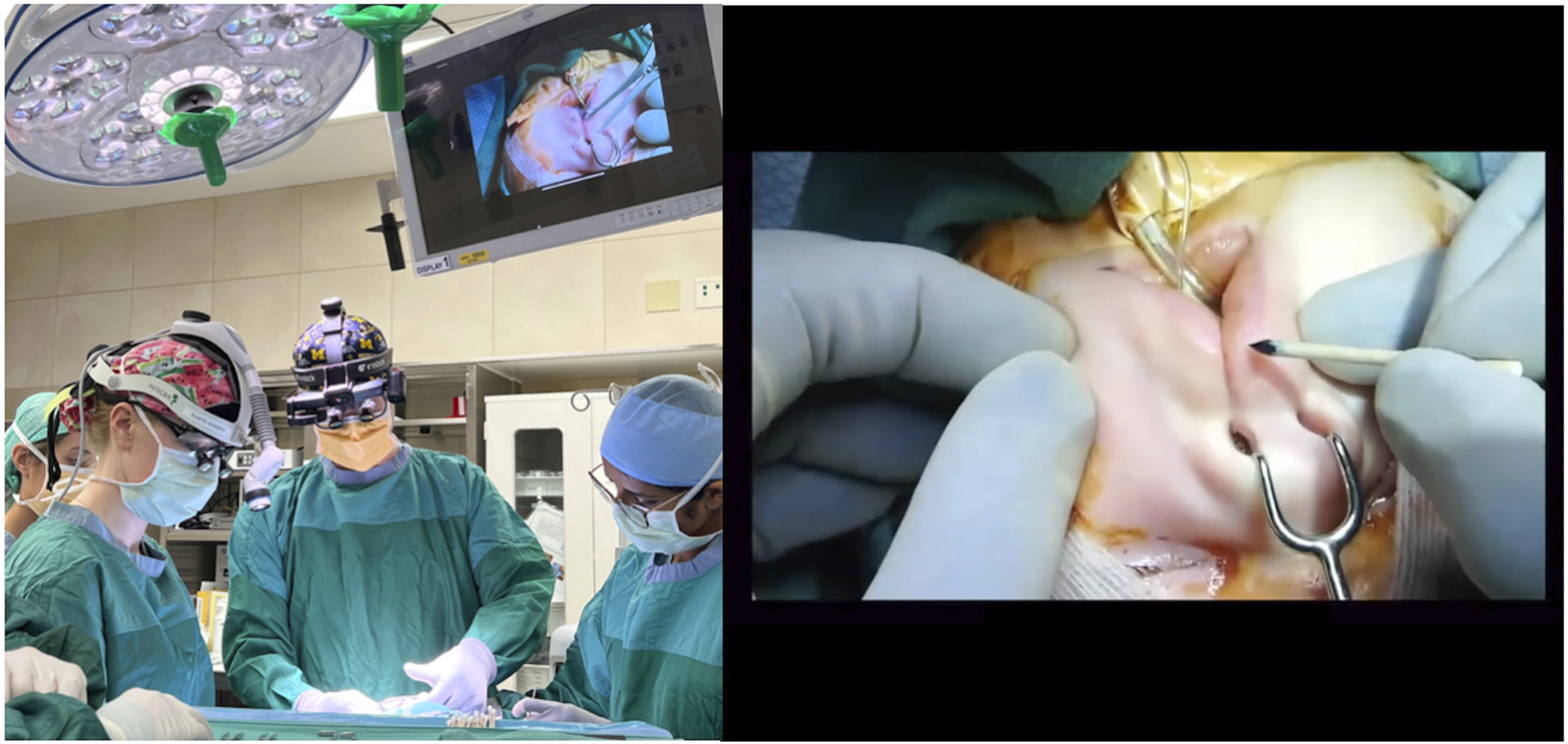
The third intervention focused on pre-operative planning and education; the attending craniofacial surgeon wore a Hololens HMD connected to the display monitors in a team room for his view to be projected to residents and fellows. The surgeon opened a 3D XR digital file of the upcoming patient’s facial scans to plan the finishing osteotomies of a Le Fort I after prior distraction osteogenesis (Figure 3). The 3D object was generated by converting the raw CT scan DICOM files into an STL file using Blender software. Once the STL file was loaded onto the Hololens HMD, the surgeon could open the file through the Apoqlar application on the device. Once the file was open and floating virtually in space in front of the surgeon, he could manipulate the virtual object by changing its size and rotation, measuring segments, and drawing/annotating on the image using hand gestures. These manipulations allowed him to explore, teach, consider, and communicate his surgical plan by seeing the anatomy in a new way broadcast to learners who could view his first-person perspective on room display monitors or through teleconferencing software virtually. The planning session was recorded for asynchronous access and learning by other trainees in the future. Augmented reality-enhanced surgical education with the HoloLens2. Left: A physician wearing the device. Right: The streamed 3D anatomy overlay, illustrating how XR platforms can support anatomy teaching, preoperative planning, and immersive resident learning
Intervention 1 - Virtual Consultation
Intervention 2 - Intra-operative Education
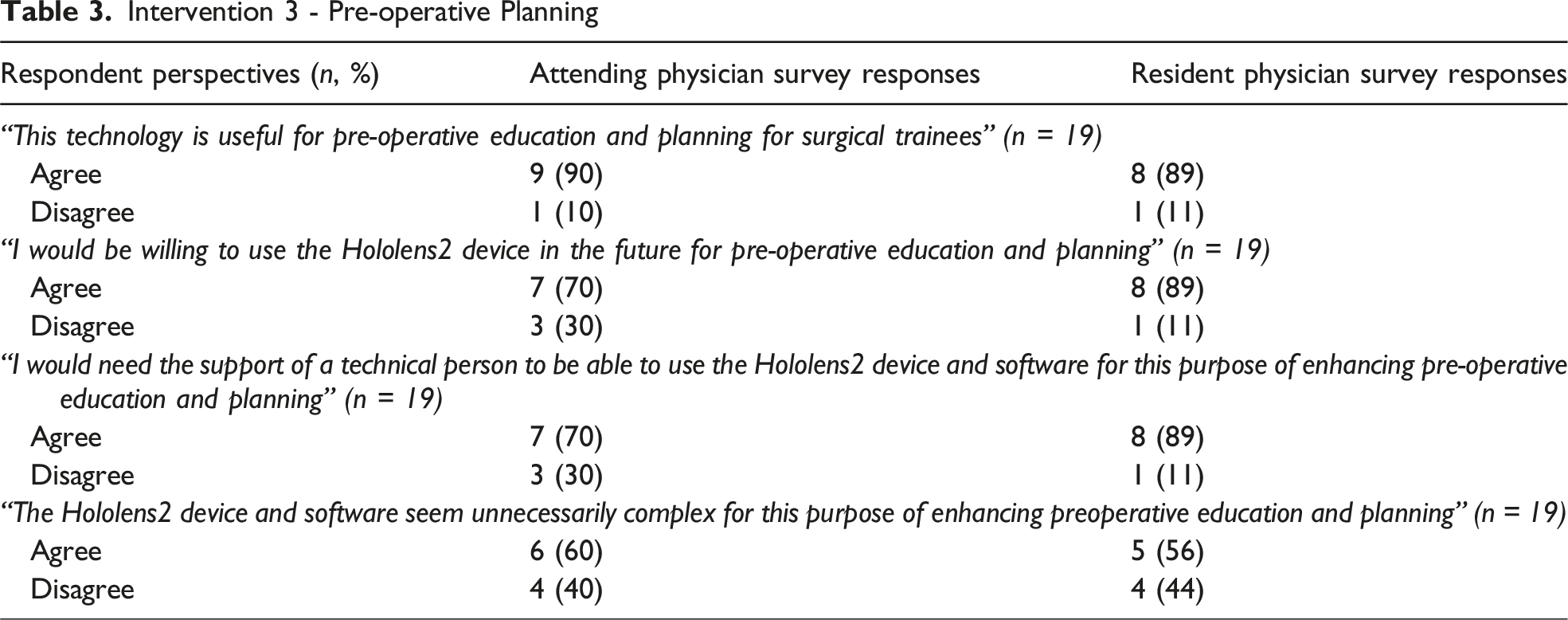
Intervention 3 - Pre-operative Planning
Responses were analyzed based on ratings of usability and usefulness for each intervention and further broken out by training level (resident vs attending responses) using both descriptive statistics (means ± standard deviations) and categorical inferential testing. Group-level differences between residents and attending physicians were assessed using Fisher’s exact test due to small sample sizes with Likert-scale responses collected on a four-point scale and dichotomized as disagree (scores 1-2) vs agree (scores 3-4).
Results
Eleven attending and ten resident physicians (21/44, 48%) responded to the survey.
Virtual Consultation
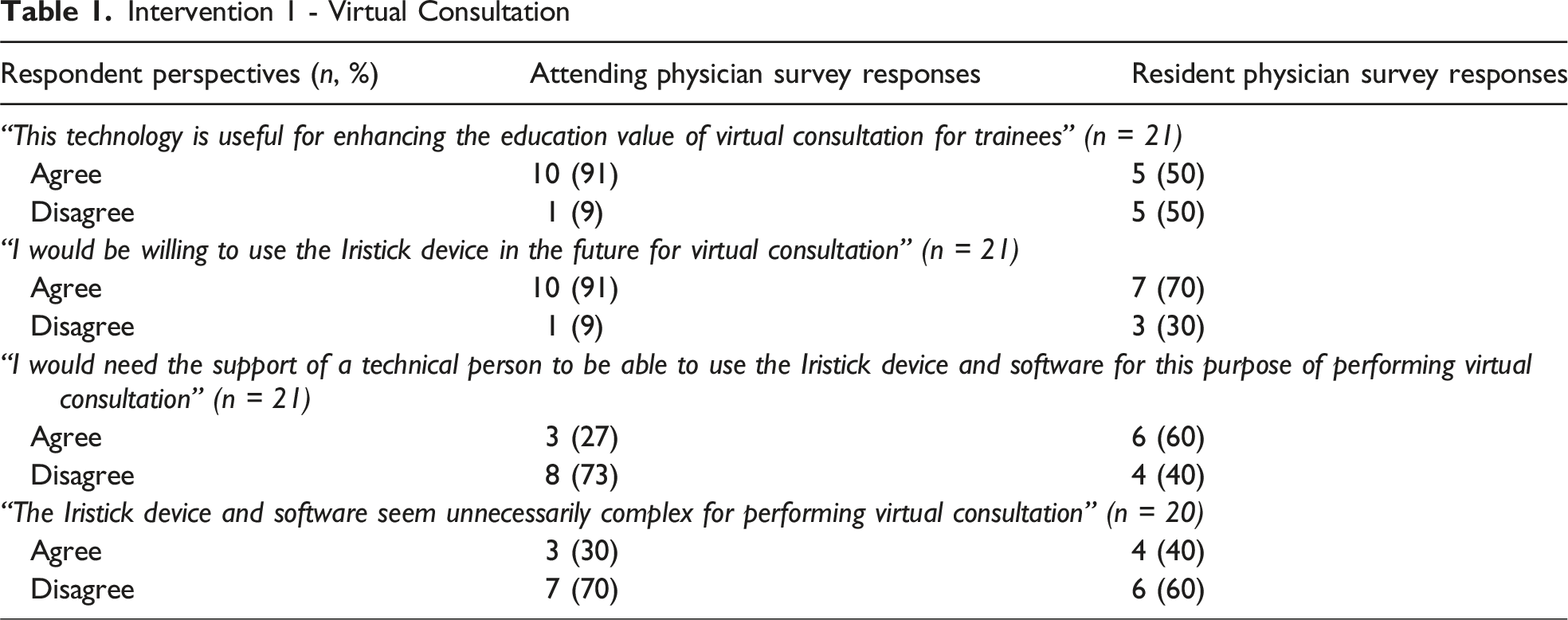
Across all interventions, attending physicians expressed the greatest willingness to use and optimism toward virtual consultation. “Optimistic” refers to positive answers to questions like, “This technology is useful for [the intended intervention].” Attendings more frequently agreed that virtual consultations were useful compared to residents (91% vs 50%), demonstrating a near-significant trend on Fisher’s exact testing (P = 0.056). Consistent with this finding, attendings reported higher mean perceived usefulness scores than residents (3.3 ± 0.9 vs 2.4 ± 1.2). Mean usability scores were also higher among attendings (3.3 ± 0.7) compared to residents (2.9 ± 1.0). Attending physicians were more confident in their ability to use the Iristick HMD for remote consultation, with only 27% agreeing they would need technical support vs. 60% of residents noting they would need technical support, though this difference was not statistically significant. Scores for perceived complexity of the Iristick HMD for remote consultation were low in both groups (residents: 2.2 ± 0.8; attendings: 1.9 ± 0.8), with no significant group differences. All virtual consultation results are illustrated in Figure 4. Comparison of attending and resident survey responses for the virtual consultation intervention. Stacked bar charts display the proportion of respondents who agreed vs. disagreed with each statement related to usefulness, willingness to use, need for technical support, and perceived complexity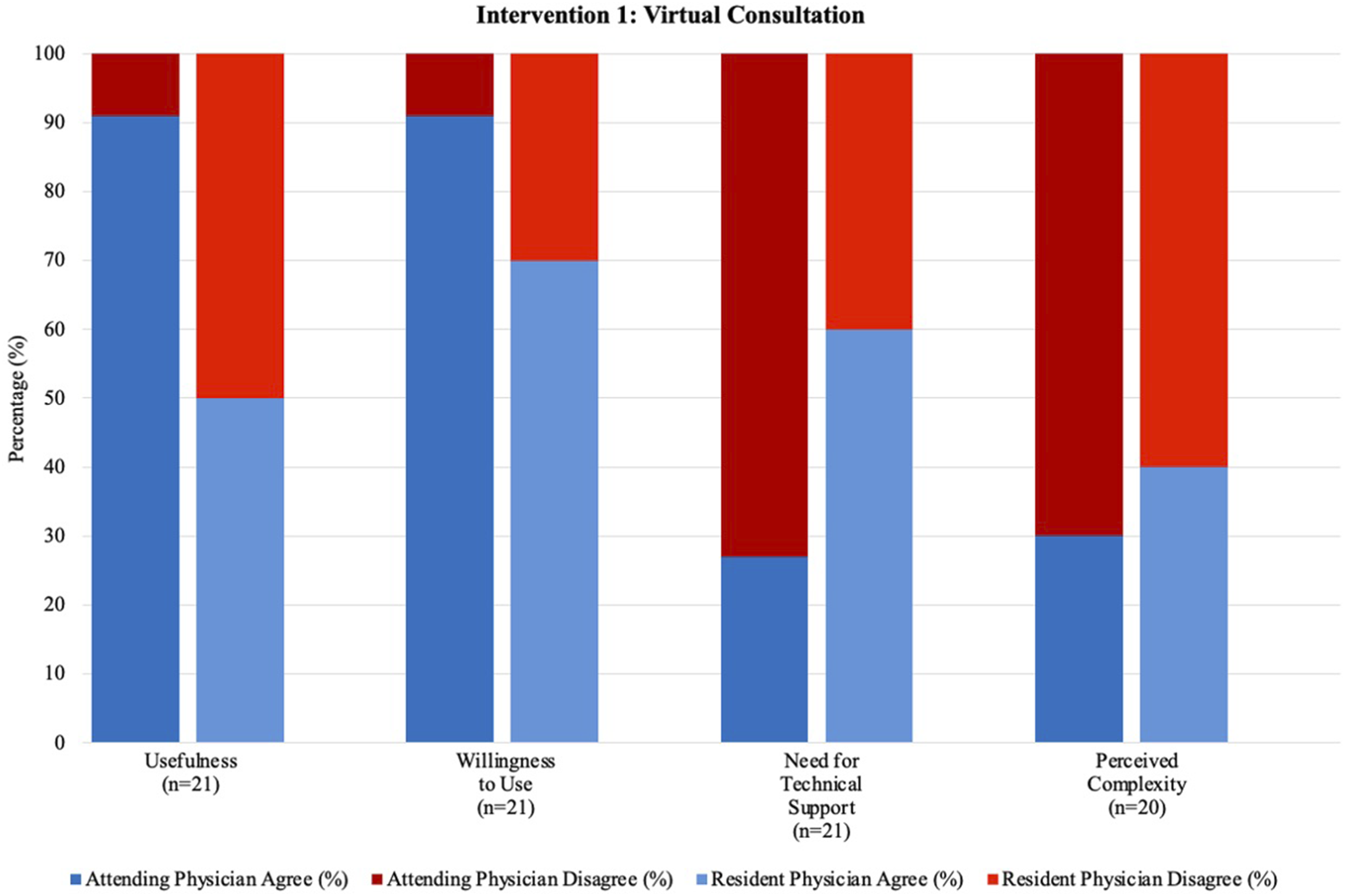
Intra-operative Education
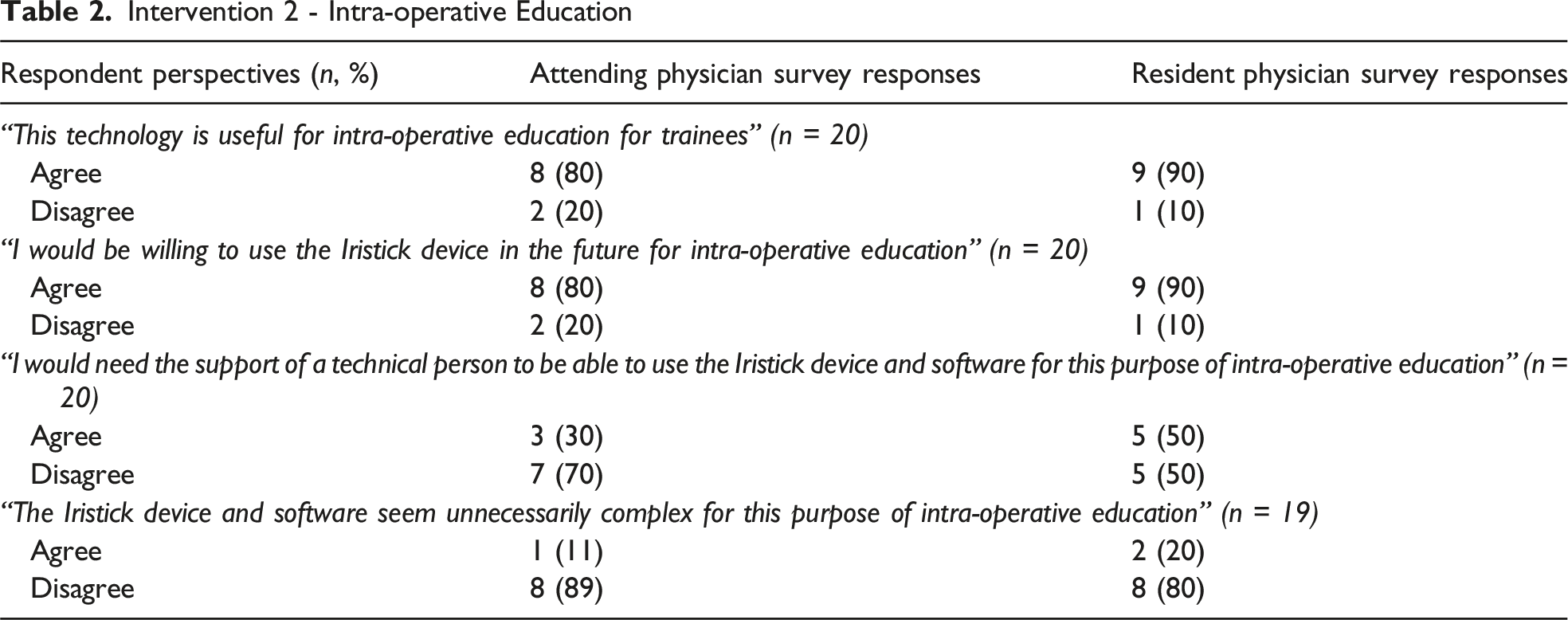
Both residents and attending physicians demonstrated high levels of agreement regarding the usefulness and usability of XR for intra-operative education. Residents reported slightly higher mean usefulness and usability scores than attendings (usefulness: 3.6 ± 0.7 vs. 3.2 ± 1.0; usability: 3.5 ± 0.7 vs. 3.1 ± 1.2), though categorical analyses showed no statistically significant differences between groups (Fisher’s exact P = 1.00 for both). Consistent with these findings, residents were most willing to use and optimistic about intra-operative education using the Iristick device (90% for both), while attending physicians expressed similarly high willingness and optimism (80% for both). Attending physicians were more confident in their ability to use the Iristick HMD for intra-operative education, with only 30% agreeing they would need technical support vs. 50% of residents noting they would need technical support (residents: 2.3 ± 0.8; attendings: 2.2 ± 0.9). Perceived complexity remained low for both residents and attendings (1.9 ± 0.7 and 1.9 ± 0.9, respectively), with no significant group differences. All intra-operative education results are illustrated in Figure 5. Comparison of attending and resident survey responses for the intra-operative education intervention. Stacked bar charts display the proportion of respondents who agreed vs. disagreed with each statement related to usefulness, willingness to use, need for technical support, and perceived complexity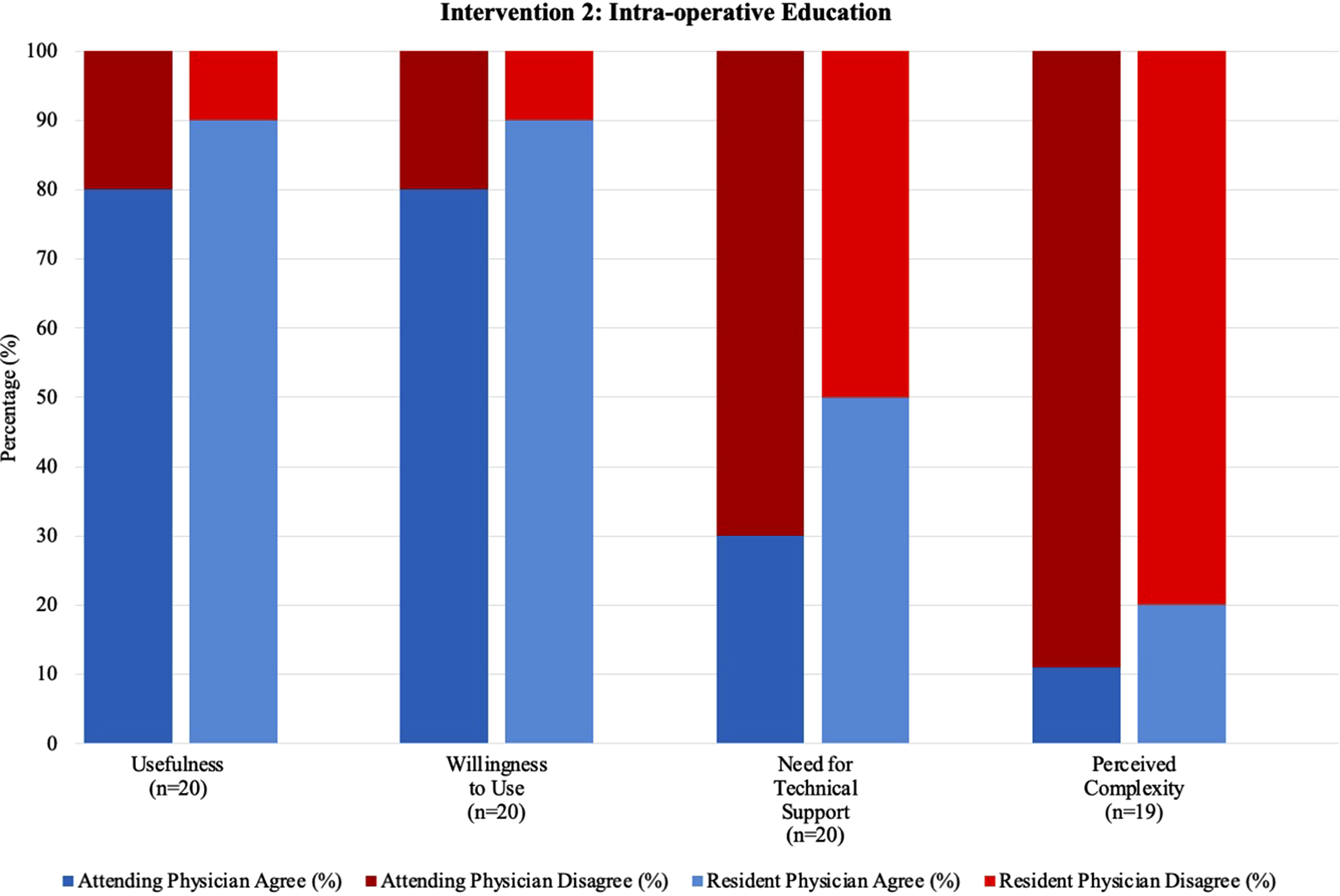
Pre-operative Planning
For pre-operative planning using the HoloLens2, both attendings and residents largely agreed that the technology was useful (90% vs. 89%, Fisher’s exact P = 1.00). Attendings reported slightly higher mean usefulness scores than residents (3.4 ± 0.7 vs. 3.0 ± 0.5), while mean usability scores were similar between groups (attendings: 3.0 ± 1.1; residents: 3.0 ± 0.5). From a usability perspective, attending and resident physicians considered the HoloLens2 unnecessarily complex (60% & 56%, respectively) with mean perceived complexity scores moderate and comparable between groups (residents: 2.4 ± 1.0; attendings: 2.6 ± 1.1), with no statistically significant differences on categorical analysis. Additionally, a majority of both attendings (70%) and residents (89%) reported that they would require technical support for pre-operative planning with the HoloLens2, with comparable mean scores for perceived need for technical support (residents: 3.1 ± 0.9; attendings: 2.9 ± 1.2). All pre-operative planning results are illustrated in Figure 6. Comparison of attending and resident survey responses for the pre-operative planning intervention. Stacked bar charts display the proportion of respondents who agreed vs. disagreed with each statement related to usefulness, willingness to use, need for technical support, and perceived complexity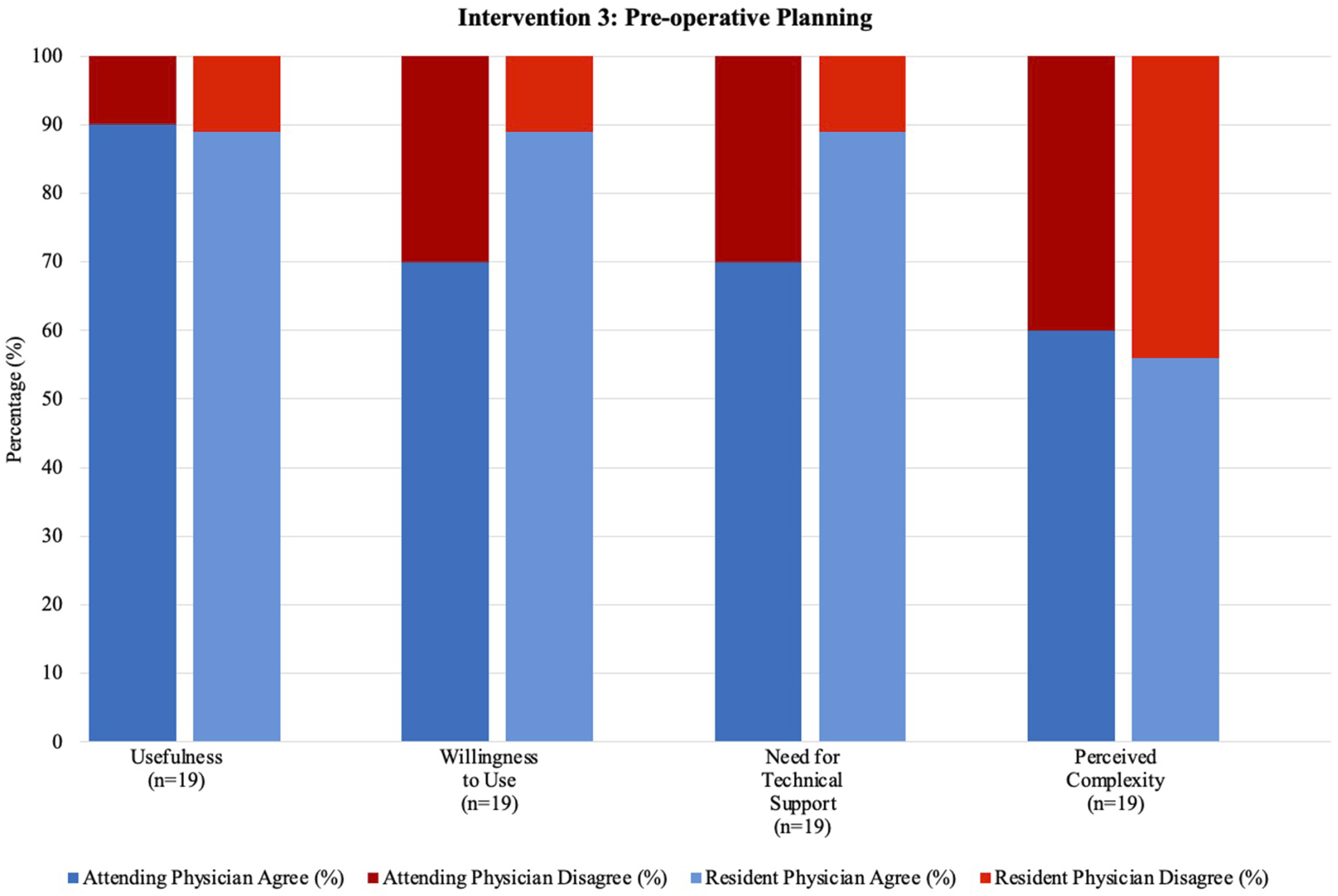
Summary of Group Differences
Mean (±SD) TAM Scores by Training Level and XR Modality With Group Comparisons
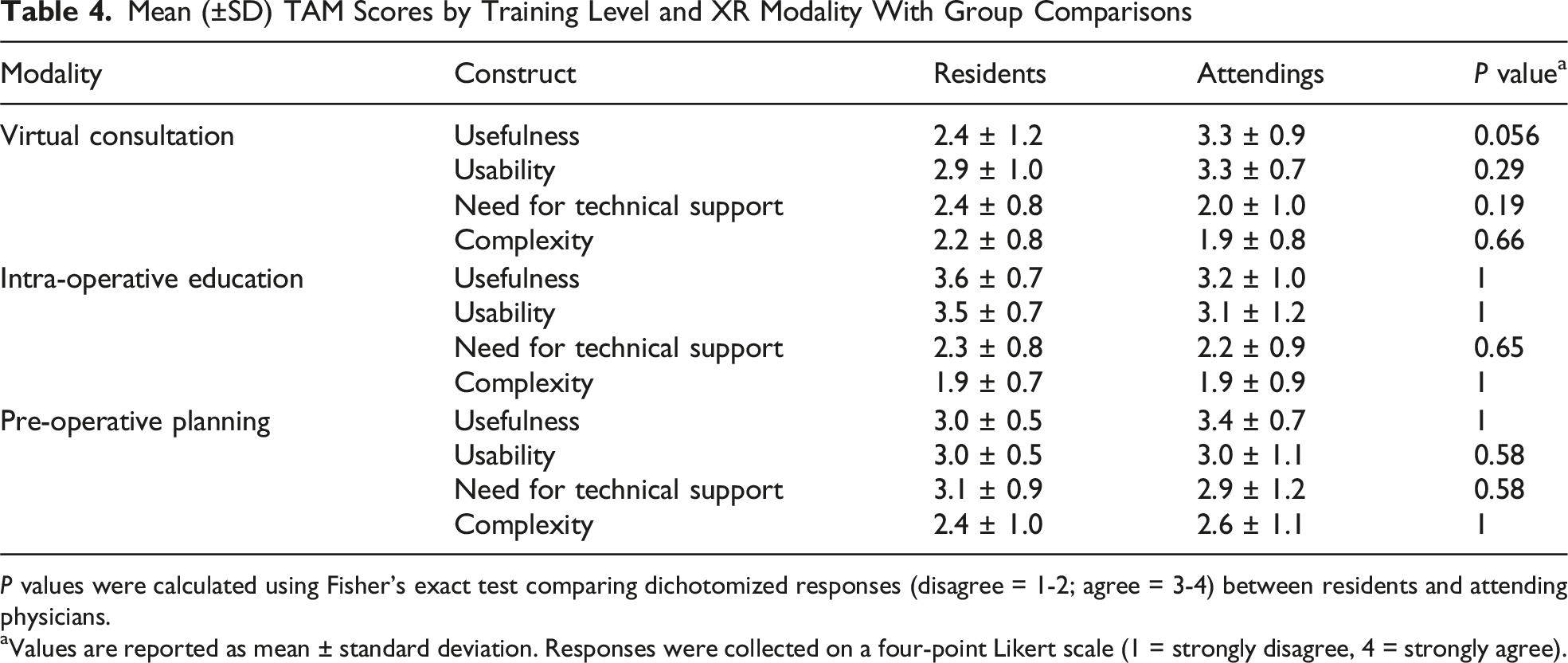
P values were calculated using Fisher’s exact test comparing dichotomized responses (disagree = 1-2; agree = 3-4) between residents and attending physicians.
aValues are reported as mean ± standard deviation. Responses were collected on a four-point Likert scale (1 = strongly disagree, 4 = strongly agree).
Discussion
Usefulness
The study found differences between attending physicians and residents in evaluating the perceived usefulness of XR-enriched consults, intra-operative education, and pre-operative planning in plastic surgery. Perceived usefulness refers to the belief that using technology will enhance performance and/or learning gains. 8 In this study, attending surgeons found all interventions useful in fostering residents’ readiness and skill development, whereas residents viewed intra-operative streaming as more useful due to its increased autonomy while offering real-time guidance during surgery. This finding parallels prior studies examining the pedagogical and technological affordances of XR approaches in surgical education. 11 One study examined a tele-mentoring system for minimally invasive surgery, allowing a mentor to demonstrate surgical instrument motions to a mentee remotely. 12 The trainee benefits from increased visualization and data with little deviation from their normal behavior of observing an attending physician. Qualitatively, attending physicians may believe that intra-operative viewing is already frictionless for trainees. In contrast, several resident physicians described difficulty visualizing the surgical area of focus when multiple people are scrubbed in. Additionally, residents from in-person intervention sessions noted that an attending physician wearing and streaming their view elicited a Hawthorne effect, whereby the wearer seemed to verbalize more of their tacit knowledge that might have otherwise gone unnoted in the absence of a recording device. Although often framed as a source of observational bias, this effect may also be pedagogically advantageous, prompting attending physicians to externalize their decision-making processes, highlight intra-operative cues, and provide constructive real-time instruction that enhances both live and asynchronous learning.
Usability
Residents demonstrated a higher reliance on technical support across all interventions, including virtual consults (Iristick), intra-operative education (Iristick), and pre-operative planning (Hololens). However, interventions utilizing simpler devices like the Iristick garnered more favorable usability ratings. To explain these findings, several factors warrant consideration, including variability in cognitive burden, device ergonomics, and the potential for “inattentional blindness.” Sweller’s study of novice and expert performance argues that novices and experts experience different levels of cognitive burden. 13 Novices, such as residents, bear a higher cognitive burden as they need to learn a task’s fundamental concepts and rules. In contrast, attendings are experts in their field and carry a lower cognitive load, as they have developed efficient mental models and automatic processing for surgical tasks.
The intervention that resident physicians rated least valuable was the only application where they were wearers of the HMD instead of observers. Qualitative responses suggest residents are under increased cognitive load, and novel processes may be perceived as stress-inducing if they are the intended wearer of the HMD. In this way, “usefulness” may be conflated with “usability.” When integrating XR technology into the surgical workflow, the increased cognitive burden on residents may impact their ability to adapt to the novel demands of XR interventions. New technology may add to the cognitive burden as residents try to manage a high cognitive load of new tasks and maintain a high level of visuospatial coordination, which leaves room for misinterpretation. Confusion, stress, and risk of error can be exacerbated when this uncertainty is coupled with the learning curve of operating new technology, such as adjusting the headpiece camera to ensure a clear and well-centered surgical visual field. Conversely, attendings may find integrating XR into their existing workflow easier, as they have established frameworks and automatic processing for the baseline surgical task.
A primary usability concern is the ergonomics of XR technologies during intra-operative procedures. Studies have reported that surgeons wearing the Microsoft HoloLens had to adjust their neck position throughout procedures, causing unwanted head and neck pain.14,15 Given the bulkier design and greater facial coverage of the HoloLens, improper head positioning can lead to adverse physical consequences for surgeons. The Iristick, however, resembles smart glasses and sports a lightweight, compact design that provides greater comfort and ease of wear for extended periods. Usability in this setting hinges on the residents’ receptiveness to the physical device design and their willingness to embrace the new format of information visualization during surgical cases. Both attending and resident physicians considered the Hololens2 unnecessarily complex (60% & 56%, respectively), while simpler devices such as the Iristick were rated more favorably for usability. Persistently, in all Iristick interventions, attendings were more confident than residents in their ability to use the devices without technical support.
There is also the potential challenge of “inattentional blindness,” a phenomenon that describes surgeons becoming so absorbed in the XR overlay that they may overlook important events in the periphery. 16 This poses a risk of technology-mediated user error. However, this risk can be mitigated by optimizing the XR rendering to streamline visual information. Compared to other interventions that use XR and overlay images onto the surgical field, such as the Hololens, the Iristick does not incorporate holographic manipulation but offers a unique training opportunity that is not bound by the physical presence of attending physicians. The Iristick facilitates enhanced communication between residents and attending physicians, enabling remote training and simulation while increasing resident autonomy through verbal instructions and first-person point-of-view observation.
Barriers to Adoption
Our study utilized the well-established Technology Acceptance Model, which revealed high scores for “usability” and “usefulness” of the technology applications we examined. While these results could suggest that the next logical step is to design follow-up studies exploring additional benefits like time savings, improved clinical outcomes, enhanced communication and collaboration, better patient experience, and cost-effectiveness, the lack of proliferation of these advanced technologies in academic medicine programs indicates there are barriers for adoption that must be addressed first. We propose several factors impacting the adoption of XR. Barriers directly reflected in our data include evolving evidence regarding efficacy/safety, integration into the clinical workflows, compounding effects of existing infrastructure, faculty and learner professional development, accessibility, technical challenges/limitations, and user acceptance of the new technology. Additional factors such as cost, a dense regulatory environment, and limited content and applications are discussed as contextual considerations that, while not directly measured in this study, remain relevant to real-world implementation and future scalability. Our study findings are consistent with prior studies which point to these “hidden barriers” that have emerged and must be overcome before the benefits of these technologies can be fully realized in practice. 17
An Evolving Landscape of Clinical Efficacy
While growing evidence supports the benefits of XR in medicine, the field is still relatively new, and robust clinical studies validating its efficacy are limited. 18 Most studies of XR applications come from single-institution prospective or retrospective trials as opposed to multi-institutional randomized control trials. The lack of evidence can deter healthcare providers and institutions from investing in XR without clear proof of effectiveness. 19 However, there are many institutions and current grant-funding opportunities that aim to produce such research to help enhance the adoption of XR technologies across the medical landscape.
Integration with Existing Infrastructure
XR is a high-tech innovation requiring high-quality hardware, reliable tracking systems, interaction and input mechanisms, networking and connectivity, performance optimization, and adherence to security and data privacy protocols.
Integrating these systems into established clinical workflows often necessitates additional training and technical expertise, posing challenges for already resource-limited healthcare environments.
Technical Limitations
XR technologies are still evolving and technical limitations exist. Common issues include potential latency issues, bulkiness and limited battery life, and concerns related to cyber motion sickness or discomfort experienced by some users.7,20,21 In high-stakes clinical settings, even minor disruptions to workflow or performance may impede adoption, underscoring the need for highly reliable, user-friendly, comfortable systems.
Resistance to Change
Resistance to new technologies is a common barrier in healthcare. Ultrasound can be used as a primary example, first denounced by healthcare professionals as a technology with limited use and now seen as a standard of care. 22 Reluctance to embrace XR technology may be due to a lack of familiarity, concerns about disrupted workflows, feeling that current technology is “good enough,” and not understanding the potential impact of an evolving technology. Addressing these concerns through education, demonstrations, and evidence-based research is essential in overcoming resistance to change.
Cost
XR technologies require investment in hardware, software, infrastructure, training/education, maintenance and support, content development, and regulatory compliance. In the current healthcare landscape, characterized by reimbursement challenges and increasing administrative costs, these upfront and ongoing expenses can be prohibitive. To adopt XR technologies in the healthcare setting, an initial sunk cost lies in acquiring the hardware needed to provide such a service. Devices such as the Microsoft HoloLens2 and Apple Vision Pro, each priced at approximately $3500 per unit, represent substantial investments especially when intended clinical use cases are limited. 23
Regulatory and Legal Challenges
XR implementation in healthcare raises unresolved regulatory and legal concerns, including patient safety, data privacy, and medical liability. Health authorities have yet to establish clear clinical guidelines and regulations for using XR, leaving institutions to independently define implementation standards. 24 Until a clear set of standards has been defined, this will continue to be a barrier to adoption for many organizations.
Limited Content and Applications
The market capitalization of XR technology is growing significantly; its use in healthcare, training, and education follows only behind its growth in the gaming industry. 25 XR content and applications tailored for medical use may be limited currently but with high-growth expectations longer-term. Developing high-quality, medically relevant XR content requires close collaboration between XR developers and healthcare experts to ensure accurate workflows and use-case-specific implementation, which may pose a barrier to widespread adoption. The availability of open-source standardized, no-code XR content libraries and platforms may help mitigate this barrier.
Recommendations for Breaking the Barriers
Start with low-hanging fruit by implementing quick proof-of-concept interventions that provide immediate benefits. By showcasing successful outcomes and addressing concerns in these limited settings, support for broader adoption can be garnered. Identify and address barriers for broader stakeholders, such as IT departments, hospitals, safety committees, and patient privacy advocates. Engage these groups early to ensure their support, encourage involvement, and show commitment to addressing ongoing concerns.
Future Directions
Future work may include multicenter studies with standardized protocols to expand on usability and educational impact across settings. Incorporating objective, competency-based assessments such as skill checklists or procedure-specific metrics can help determine whether perceived usefulness translates into measurable learning outcomes. Linking XR applications to simulation outcomes may clarify their effect on skill acquisition and readiness for autonomy. As technological platforms mature, integrating XR within competency-based curricula with structured feedback systems and longitudinal evaluation will be essential for sustainable, evidence-driven adoption in surgical education.
Limitations
This study has several limitations. Interventions were conducted at a single institution and employed a heterogeneous mix of XR technologies (Iristick vs Hololens2) for different use cases, which reduces standardization of results across the technology genre as a whole. The study relied primarily on subjective perceptions without objective outcome measures such as skill acquisition and knowledge retention metrics. In addition, assessments were short-term without longitudinal or behavioral follow-up and the 48% response rate introduces potential response bias, as respondents may differ systematically from non-respondents in their perceptions of XR technologies. Future studies with larger samples and anonymized demographic stratification are needed to evaluate adoption patterns across training levels and subspecialties. Finally, responses may have been influenced by novelty bias, with participant rating new technologies more favorably due to their innovative nature.
Conclusion
The study demonstrated that the adoption potential of new technologies differed in a meaningful way between attending physicians and resident physicians in terms of usefulness vs usability. Attendings were overall more receptive than residents to the integration of XR in plastic surgery training, likely due to greater familiarity and prowess within the baseline operative/medical workflow. Residents, however, valued the technology interventions that provided better visibility in the operating room and pre-operative decision-making. Comprehensively, XR is a powerful educational tool that could transform the resident/attending training dynamic if it is implemented in a way that builds trust, insight, and value without undue burden. Therefore, selecting the best value use cases and executing them with the most user-friendly technology in a process mindful of role stress is paramount to advancing residency education efforts.
Footnotes
Ethical Considerations
The studies involving humans were approved by University of Michigan Medical School Institutional Review Board (HUM00213488). The studies were conducted in accordance with the local legislation and institutional requirements.
Consent to Participate
The participants provided their written informed consent to participate in this study.
Consent for Publication
Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
Author Contributions
Established the study design: MDB, DAI, CJV
Execution of the study: MDB, DAI, CJV, TK
Data collection: MDB
Data analysis: MDB, DAI, HX, VP, TK, CJV
Preparation of the manuscript: MDB, DAI, NAA, NM, HX, VP, TK, CJV
Revision of the manuscript: MDB, DAI, NAA, NM, HX, VP, TK, CJV
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.